




Crossref Citations
This article has been cited by the following publications. This list is generated based on data provided by Crossref.
Tjørnhøj-Thomsen, Tine
and
Hansen, Helle Ploug
2011.
Knowledge in health technology assessment: Who, what, how?.
International Journal of Technology Assessment in Health Care,
Vol. 27,
Issue. 4,
p.
324.
Brooker, Ann-Sylvia
Carcone, Steven
Witteman, William
and
Krahn, Murray
2013.
QUANTITATIVE PATIENT PREFERENCE EVIDENCE FOR HEALTH TECHNOLOGY ASSESSMENT: A CASE STUDY.
International Journal of Technology Assessment in Health Care,
Vol. 29,
Issue. 3,
p.
290.
Kleme, Jenni
Pohjanoksa-Mäntylä, Marika
Airaksinen, Marja
Enlund, Hannes
Kastarinen, Helena
Peura, Piia
and
Hämeen-Anttila, Katri
2014.
PATIENT PERSPECTIVE IN HEALTH TECHNOLOGY ASSESSMENT OF PHARMACEUTICALS IN FINLAND.
International Journal of Technology Assessment in Health Care,
Vol. 30,
Issue. 3,
p.
306.
Hoeck, Bente
Ledderer, Loni
and
Hansen, Helle Ploug
2015.
Involvement of Patients with Lung and Gynecological Cancer and Their Relatives in Psychosocial Cancer Rehabilitation: A Narrative Review.
The Patient - Patient-Centered Outcomes Research,
Vol. 8,
Issue. 2,
p.
127.
Dipankui, Mylène Tantchou
Gagnon, Marie-Pierre
Desmartis, Marie
Légaré, France
Piron, Florence
Gagnon, Johanne
Rhiands, Marc
and
Coulombe, Martin
2015.
EVALUATION OF PATIENT INVOLVEMENT IN A HEALTH TECHNOLOGY ASSESSMENT.
International Journal of Technology Assessment in Health Care,
Vol. 31,
Issue. 3,
p.
166.
Weeks, Laura
MacPhail, Elaine
Berglas, Sarah
and
Mujoomdar, Michelle
2017.
Patient Involvement in Health Technology Assessment.
p.
247.
Gagnon, Marie-Pierre
Dipankui, Mylène Tantchou
and
DeJean, Deirdre
2017.
Patient Involvement in Health Technology Assessment.
p.
201.
Nielsen, Camilla Palmhøj
and
Væggemose, Ulla
2017.
Patient Involvement in Health Technology Assessment.
p.
265.
Single, Ann N.V.
Facey, Karen M.
Livingstone, Heidi
and
Silva, Aline Silveira
2019.
Stories of Patient Involvement Impact in Health Technology Assessments: A Discussion Paper.
International Journal of Technology Assessment in Health Care,
Vol. 35,
Issue. 4,
p.
266.
Mason, Robert J.
Searle, Karlee M.
Bombard, Yvonne
Rahmadian, Amanda
Chambers, Alexandra
Mai, Helen
Morrison, Marjorie
Chan, Kelvin K. W.
and
Jerzak, Katarzyna J.
2020.
Evaluation of the impact of patient involvement in health technology assessments: A scoping review.
International Journal of Technology Assessment in Health Care,
Vol. 36,
Issue. 3,
p.
217.
Georgieva, C.
and
Yanakieva, A.
2021.
Role of the Patient‘s Viewpoint in Health Technologies Assessment in Bulgaria.
Acta Medica Bulgarica,
Vol. 48,
Issue. 3,
p.
5.
Puebla, Marcos
Korrodi-Gregório, Luis
Trentin, Luca
De Maria, Annabel
and
Blanqué, Nerea
2025.
A comparative analysis of patient participation in health technology assessment systems worldwide: trends and practices.
Frontiers in Public Health,
Vol. 13,
Issue. ,
There is an increasing focus on designing health services as “patient focused,” including involvement of patients in their own care, as well as patients and citizens in decisions about healthcare services and delivery. This general and increasing attention is reflected in a growing focus on patient aspects and patient involvement in health technology assessment (HTA), and how this focus might be strengthened (Reference Facey, Boivin and Gracia1).
A review on the inclusion of patient and/or organizational aspects in HTA reports published by INATHA members 2000–05 showed a great variation; in relation to explicit inclusion of the aspects to be assessed as well as in how the aspects were addressed. This has the effect of leaving the reader uncertain as to whether or not the relevant issues were included, and if they were assessed using a relevant methodology (Reference Lee, Skött and Hansen4;5). Based on the results from this review, an interest emerged for reviewing the Danish HTAs in relation to how these reports have addressed patient aspects.
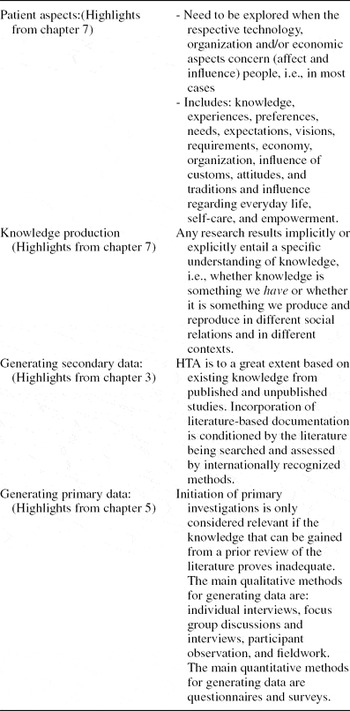
In Denmark, there is a long tradition for conducting HTAs within a framework of four key elements: (i) technology, (ii) patient, (iii) organization, and (iv) economy. In the recently updated Danish Handbook of HTA (Reference Kristensen and Sigmund3), it is stated that the patient element must focus on patient aspects, such as patient perspectives, needs, experiences, preferences, and/or acceptance of a given technology. In Table 1, an overview of recommendations for patient assessments in the Danish Handbook is presented.
Danish Recommendations for Assessment of Patient Aspects (3)
The objective of this study is to describe the management, presentation, and significance of the assessment of patient aspects in Danish HTA reports and thereby contribute to the ongoing national and international debates about patient aspects in HTAs.
METHODS
A review of the sixty-two Danish HTA reports published between January 1999 and February 2010 either as National HTA reports or as reports funded by a DACHETA grant was conducted (Reference Randwijk and Hansen9) (Supplementary Table 1, which is available at www.journals.cambridge.org/thc2011024). The inclusion criteria being assessment of patient aspects meant that four reports were excluded: Two focused exclusively on economic evaluation (Reference Olsen, Bjerregaard, Ibfelt and Laurberg8;Reference Rasmussen, Kilsmark, Hvenegaard, Thomsen, Engberg, Lauritzen and Søgaard10) and two reports had no specific focus on patient aspects (6;7). Four questions guided our reading of the fifty-eight reports included in the review: (i) How are patient aspects addressed in the reports? (ii) What kind of data is included and how are they generated? (iii) Are the results about patient aspects integrated in the concluding parts of the report? (iv) Are there any changes in how patient aspects have been investigated and presented in HTA-reports over the years?
RESULTS
How Are Patient Aspects Addressed in the Reports?
Objectives and/or research questions were specifically stated concerning the patient aspects in fifty-four of the fifty-eight reports. Four reports did not include a specific objective and were published before 2006. In fifty-one of the fifty-eight HTA reports there was a separate chapter about patient aspects. Of the remaining seven reports, two stood out. Here, the authors argued that because of their theoretical approach, patients aspects must be incorporated in other elements of the report. In one of these, theories of knowledge and knowledge production were used to illustrate the ward round at a hospital as a production of knowledge, aimed at managing the diagnostic and therapeutic work (number 25 in table 2). Here, patient aspects were integrated with the organizational element. In the other report, actor-network theories (ANT) were used to understand certain aspects of poly-pharmacologic treatment of type 2 diabetes (number 37 in Table 2). Here, patient aspects were integrated in the elements of technology and organization. The remaining five reports did not specify reasons for not having a separate chapter for patient aspects.
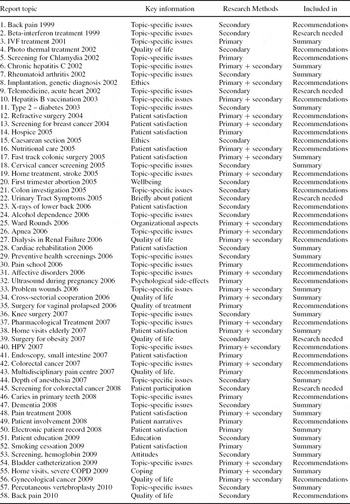
The Fifty-eight Danish Reports
What Kind of Data Is Included and How Are They Generated?
The fifty-eight reports are presented in Table 2. All of the fifty-eight reports included literature in a systematic or unsystematic way and 34 (59 percent) of the reports included primary data to answer the HTA questions (Table 2).
Secondary Research
While all the reports included some kind of literature search, there was a considerable variation in relation to if and how the authors presented and discussed their choice of search, regarding the purpose and perspectives of the study. In twelve reports (21 percent), a systematic literature search was included specifically for the patient aspects. In one report, a systematic literature search was included but the databases used were not presented. In twenty-nine reports (50 percent), a collective systematic literature search was included for all the (four) aspects of the report. In sixteen reports (28 percent), the literature search followed a more experience based process, where the authors' browsed the literature. The most frequently used databases were medical, such as Medline, Pubmed, Embase, Cinahl, and HTA databases. A few reports included sociological or anthropological databases, such as Sociological Abstracts.
Primary Research
In thirty-four (59 percent) of the reports, primary data were generated. Sixteen of these reports (47 percent) used quantitative methods, thirteen (38 percent) used qualitative methods, and five reports (15 percent) used both kinds of methods. Of the twenty-four reports that did not produce primary data, twenty-two (92 percent) relied on literature reviews. The remaining two reports relied on data generated in other reports or studies, and engaged with literature related to those, without making systematic literature reviews.
Are the Results About Patient Aspects Integrated in the Concluding Parts of the Report?
All fifty-eight reports addressed patient aspects either in their conclusion, syntheses and/or recommendations. The inclusion of patient aspects might be categorized as; included in the recommendations of the report or included in the summary of the report. Thirty-four reports (59 percent) included patient aspects in the recommendations of the report. Twenty-six of these included recommendations for future clinical practice based on patient aspects. One example on future clinical practice was a recommendation about how to organize a specific form of treatment. It was argued that this specific form of treatment must be kept within the primary healthcare sector to avoid unnecessary pathologization of the patient (number 1 in Table 2). Another example was a recommendation about a greater flexibility in the understanding of the patient as an active agent (number 49 in Table 2).
Eight reports recommended an improvement in patient information. One example was a recommendation to increase the information to social groups with different ethnic and cultural backgrounds (number 5 in Table 2). Another example was reflections on how information, regarding side effects in relation to a specific treatment, can be handled most effectively (number 40 in Table 2). None of the recommendations were based on, or referred to, theories of communication and information.
In the remaining twenty-four reports (41 percent), the patient aspects were included in the concluding part of the report. The text focused either on how patient aspects had been investigated (in nineteen reports) or stated that the knowledge we have today about patient aspects have limitations (in five reports). One example was a report in which it was concluded that there was no knowledge available about the patients' physical, psychological, and social challenges in relation to the specific disease and its treatment (number 39 in Table 2). No conclusions or recommendations concerning patient aspects were drawn in these reports.
Of the twenty-six reports including patient aspects in the recommendations for future clinical practice, twenty (77 percent) had generated new empirical data. This is a significantly higher proportion than that of all reports generating new empirical data (59 percent). Eleven of the twenty reports (55 percent) used qualitative methods for the assessment and the rest used quantitative methods.
Are There Any Changes in How Patient Aspects Have Been Investigated and Presented in HTA Reports Over the Years?
By combining the distribution of reports in the years 1999–2010 and the above results, we were able to identify some chronological trends in relation to how the literature search was conducted, and which methods were used for generating primary data. There was a tendency for an increase in the systematic literature search on patient aspects. Whereas this was the case for up to 17 percent of the reports published in the period 1999–2005, the proportion had risen from 17 to 33 percent for the reports published between 2006 and 2009.
Also, the proportion of reports generating primary data changed across the years investigated. Although 53 percent of the reports published in the years 1999–2005 included primary data, the percentage for 2006–09 had risen to 65 percent. The two reports published in 2010 were different in that they neither included a specific literature search on patient aspects nor generated primary data for the assessment.
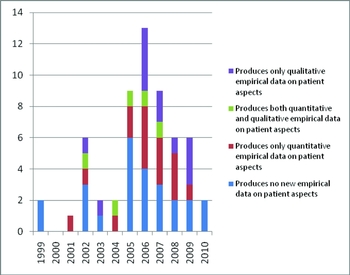
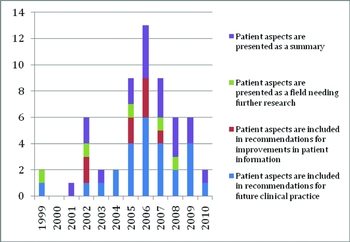
When looking at methods more specifically in the reports, the use of quantitative methods was published in reports from 2001, and the use of qualitative methods in the reports from 2002. In 2002, reports using both quantitative and qualitative methods were published (Fig. 1). There was no difference in relation to patient aspects included in the recommendations or in the summary of the reports during 1999–2010 (Fig. 2).
Inclusion of empirical data and methods used.
Patient aspects included in the concluding part of the reports.
DISCUSSION
The present review finds that patient aspects were included in fifty-eight of sixty-two Danish HTA reports published between 1999 and 2010, and that fifty-four of the fifty-eight reports included objectives and/or research questions for patient aspects. This shows that Danish HTA reports, to a greater extent than most, include these aspects (Reference Lee, Skött and Hansen4;5) and does it in a considered manner.
Although all the Danish reports included some literature for the assessment of patient aspects, only a minority included a systematic literature search specific for the aspects. More than half of the reports generated empirical data, using qualitative as well as quantitative methods. Assessing a period over 10 years showed an increase in the specific literature search on patient aspects and in inclusion of primary data. The first assessment using qualitative methods was published in 2002 and the first using quantitative methods was published in 2001. While all fifty-eight reports included the patient assessment in the summary, more than half included patient aspects in the recommendations of the report, showing some significance of the patient assessment in the final conclusions of the reports. The reports including patient aspects in the recommendations were significantly more frequently based on primary data, than the total group of reports assessed. This indicates that enhancing the assessments with primary research might be best practice for reaching conclusions relevant for decision making. From the review of the fifty-eight Danish HTA reports and from an article by Tjørnhøj-Thomsen and Hansen in this volume, a strong recommendation is that researchers base their decisions about methodology used in the assessments of patient aspects on clear and explicit reasoning (Reference Tjørnhøj-Thomsen and Hansen11).
The new HTA handbook, published in 2007 (Reference Kristensen and Sigmund3), developed chapters about patient aspects and qualitative methods from the former HTA handbook (Reference Kristensen, Hørder and Poulsen2), emphasizing theoretical considerations in relation to production of knowledge. Whereas some time trends were identified in the present review, it is as yet too early to assess how the new handbook might have influenced the methodology for assessment of patient aspects. Fourteen HTA reports were published after 2007, and because the research presented in the reports might have been ongoing for several years, it can be discussed if the status of patient aspects in HTA reports should be drawn from the year the research was initiated, rather than from the year it was published. Just the two reports published in 2010 (57;58) may have been influenced by the handbook published in 2007. They both included a systematic literature search specific for the assessed patient aspects and an evaluation of the literature (relevance and internal validity) and included findings in the recommendations for the technology. It should be noted that this was the case in some of the previously published reports as well.
The distinct inclusion of patient aspects in Danish HTA's could be the result of the tradition of including four elements, one of these being patient aspects. Presenting patient aspects in a separate chapter in the HTA allows a more direct and explicit focus on the patient's problems, needs, experiences and preferences etc. in relation to a given technology. On the other hand, an integration of the aspects to be assessed, including that of the patient, and as found in two Danish HTA reports framed by a theoretical approach, might lead to a more holistic approach to HTA, opening up for an investigation into how patients and technology affect, and is affected by, each other.
The generating of HTA questions, and the theories and methodologies used to answer them, are informed by theoretical and methodological movements in the field of health policy research and HTA, as well as a result of the composition of the project group with respect to academic background and schooling. It is, however, crucial that the necessary choices in relation to aspects and methodology are transparent, if production and reporting of HTA is to adhere to scientific standards. Although the role of members of the project group was not investigated in the present review, the authors' experience is this, that researchers with competences within social aspects increasingly are involved in the production of Danish HTA's.
If health policy and decision making is to be patient-focused, it is important that HTAs in the future integrate patient aspects in recommendations of HTA. Although both inclusion and management of patient aspects are distinct and improving in the Danish HTA reports, there is room for improvement in relation to methodology and inclusion of theory, as well as in the scientific managing, reporting, and production of clear recommendations.
SUPPLEMENTARY MATERIAL
Supplementary Table 1
www.journals.cambridge.org/thc2011024
CONTACT INFORMATION
Helle Ploug Hansen, PhD, mag.scient. (extended MA), (hphansen@health.sdu.dk), Professor in Humanistic Rehabilitation Research, Institute of Public Health Research Unit; Health, Man and Society & National Research Centre for Cancer Rehabilitation, Anne Lee, MSc (Health), RN (ale@cast.sdu.dk), Senior Consultant, Centre for Applied Health Services Research and Technology Assessment, Christian Balslev van Randwijk, MA, PhD-student (crandwijk@health.sdu.dk), Institute of Public Health, Research Unit: Health, Man and Society, University of Southern Denmark, J.B. Winsløws Vej 9, DK-5000 Odense C, Denmark
CONFLICT OF INTEREST
All authors report they have no potential conflicts of interest.