


Introduction
Self-rated health (SRH) is a widely recognised and reliable indicator of overall health and well-being. It serves as an integrative measure of cumulative life experiences, reflecting how individuals evaluate their health in light of chronic conditions, functional capacity, and psychosocial adaptation (Cullati et al., Reference Cullati, Rousseaux, Gabadinho, Courvoisier and Burton-Jeangros2014). While conventional studies often assess SRH cross-sectionally – focusing on health perceptions at a single point in later life – a life course perspective provides a deeper understanding of how subjective health changes across different stages of life (Wang and Lu, Reference Wang and Lu2024). The World Health Organization (WHO) life course framework conceptualises health in later life as the cumulative product of exposures and experiences encountered across childhood, adulthood, and older age (WHO, 2025). Childhood represents a critical formative phase during which foundational health capital is built through early-life health, nutrition, education, and labour force participation (Muhammad and Joy, Reference Muhammad and Joy2022). Adulthood serves as a period of socioeconomic development and mobility, where occupation, income, and lifestyle behaviours either reinforce or mitigate early-life disadvantages. In older adulthood, accumulated experiences interact with health behaviours, multimorbidity, mental well-being, and functional limitations to predict overall health outcomes (Foster and Walker, Reference Foster and Walker2021). Understanding SRH from a life course perspective, therefore, allows a more comprehensive interpretation of subjective health trajectories than cross-sectional assessments alone (Halfon and Hochstein, Reference Halfon and Hochstein2002; Wang and Lu, Reference Wang and Lu2024; WHO, 2025).
Considering the ongoing demographic transition in India, where the ageing population is rapidly expanding (James and Goli, Reference James and Goli2021), the life course approach could be instrumental in understanding subjective health trajectories among older adults. India is currently in the third stage of its demographic transition, marked by declining mortality and fertility rates. By 2050, the country’s elderly population is projected to reach 340 million (International Institute for Population Sciences [IIPS] & United Nations Population Fund [UNFPA], 2023). This growing demographic group represents not only a national challenge but also a global concern for ensuring a healthy and productive ageing population. Recognising this national and international priority, translating India’s demographic transformation into healthy ageing outcomes is an urgent policy goal (IIPS & UNFPA, 2023). Therefore, applying a life course approach to examine subjective health trajectories across different life stages offers a more contextually relevant framework for addressing the health and policy needs of India’s ageing population.
Globally, empirical evidence has demonstrated that life course subjective health assessment is more predictive in understanding later-life health status (Cullati et al., Reference Cullati, Rousseaux, Gabadinho, Courvoisier and Burton-Jeangros2014; Eliason et al., Reference Eliason, Mortimer and Vuolo2015; Wheatley and Buglass, Reference Wheatley and Buglass2019; Foster and Walker, Reference Foster and Walker2021; Wagner et al., Reference Wagner, Carmeli, Jackisch, Kivimäki, van der Linden, Cullati and Chiolero2024). However, subjective health research remains predominantly cross-sectional, emphasising current health status and its correlates in India (Hossain et al., Reference Hossain, Yadav, Nagargoje and Vinod Joseph2021; Saha et al., Reference Saha, Rahaman, Mandal, Biswas and Govil2022; Roy et al., Reference Roy, Saha, Rahaman, Kapasia and Chouhan2024). These studies consistently report that women, rural residents, and socioeconomically disadvantaged groups are more likely to report poor SRH, whereas engagement in social, physical, and religious activities is associated with better SRH. Nonetheless, such studies capture only static perceptions, offering limited insight into how health trajectories unfold across the life span. A few recent works have incorporated retrospective indicators, including childhood health and social mobility in India (Selvamani and Arokiasamy, Reference Selvamani and Arokiasamy2021; Muhammad and Joy, Reference Muhammad and Joy2022; Ko et al., Reference Ko, Oh, Subramanian and Kim2025), but systematic evidence on subjective health transitions remains limited.
Addressing this critical gap, the present study employs a life course measure of SRH to examine subjective health transitions from childhood to older adulthood using nationally representative data from the Longitudinal Ageing Study in India (LASI). The data provides a unique opportunity to construct such a measure by including both retrospective childhood SRH and current SRH among older adults (IIPS, 2020). By intersecting these two dimensions, this study operationalises a composite life course SRH indicator, enabling analysis of the predictors and trajectories of perceived health over time (Cullati et al., Reference Cullati, Rousseaux, Gabadinho, Courvoisier and Burton-Jeangros2014; Wheatley and Buglass, Reference Wheatley and Buglass2019; Wang and Lu, Reference Wang and Lu2024). This approach moves beyond conventional late-life assessments to capture the dynamic and cumulative nature of health across the life span. The study contributes novel empirical evidence to India’s ageing research and enriches gerontological theory by linking early-life and adult experiences to subjective well-being in later life. The findings are expected to inform life course–oriented health and social policies that promote equitable and healthy ageing for India’s growing elderly population.
Methods
Data
The present study used secondary data from the first wave of Longitudinal Aging Study in India (2017–2018). The survey design offers nationally representative estimation of the health, economic, and social well-being of older adults (aged 45 and above) (International Institute for Population Sciences (IIPS), 2020). The survey used a multistage stratified cluster sample design across Indian states and union territories (UTs). Three-stage and four-stage sampling frames were adopted for rural and urban areas, respectively. The survey was conducted from April, 2017 to December, 2018. A total of 72,250 individuals aged 45 and above and their spouses, irrespective of age, were covered in the survey (IIPS, 2020). The present study analysed a total sample of 70,595 individuals aged 45 and above after cleaning the missing data.
Outcome Variable
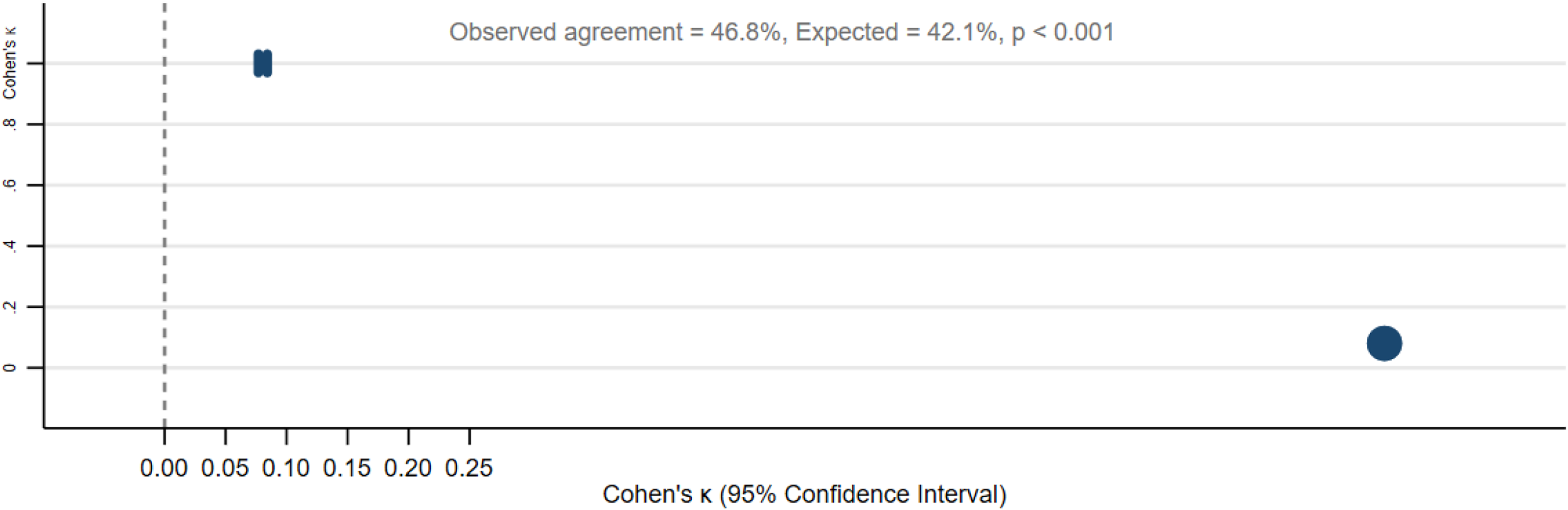
The primary outcome was the life course adverse SRH trajectory among older adults, constructed by combining retrospective childhood and current SRH, following established approaches (Feenstra et al., Reference Feenstra, Van Munster, MacNeil Vroomen, De Rooij and Smidt2020; Clouston and Link, Reference Clouston and Link2021). Childhood health was retrospectively assessed by asking participants to rate their overall health up to age 16, while current health was evaluated through a similar question on their present general health. The two measures were cross-classified into four categories: constant good SRH, adverse SRH trajectory (good→poor), improving SRH (poor→good), and constant poor SRH. Reliability analysis showed low agreement between childhood and current SRH (Cohen’s κ = 0.084, p < 0.001), indicating distinct but related constructs (Figure 1). For analytical purposes, the outcome variable was dichotomised, with adverse SRH trajectory coded as 1 and all others as 0.
Agreement between retrospective childhood and current self-rated health (SRH) among older adults, India, LASI Wave 1 (2017–2018).

Explanatory variables
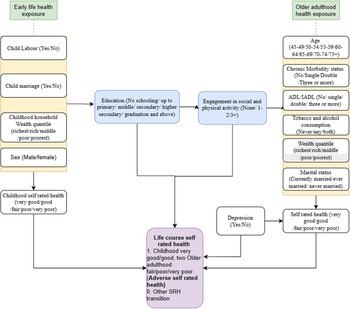
In line with existing empirical and theoretical evidence (Cullati et al., Reference Cullati, Rousseaux, Gabadinho, Courvoisier and Burton-Jeangros2014; Foster and Walker, Reference Foster and Walker2021; Wang and Lu, Reference Wang and Lu2024), the conceptual framework of the present study illustrates how early-life exposures (child labour, child marriage, and childhood household wealth status) and biological identity (sex) are linked with adult and later-life factors (education, socio-physical activity, multimorbidity, limitations in activities of daily living [ADL] and instrumental activities of daily living [IADL], health behaviours, depression, and current household wealth status) to shape subjective health in older age (Figure 2). These cumulative exposures influence transitions in SRH from childhood to older adulthood, where education and participation in socio-physical activities may mediate the long-term effects of early health disadvantage on SRH trajectory.
Conceptual framework of factors of adverse self-rated health trajectory.

Guided by this conceptual framework and prior literature (Cullati et al., Reference Cullati, Rousseaux, Gabadinho, Courvoisier and Burton-Jeangros2014; Feenstra et al., Reference Feenstra, Van Munster, MacNeil Vroomen, De Rooij and Smidt2020; Wang and Lu, Reference Wang and Lu2024), a range of demographic, socioeconomic, behavioural, and health-related variables were included as explanatory factors: age (45–49, 50–54, 55–59, 60–64, 65–69, 70–74, 75+), sex (male, female), marital status (currently married, ever married, never married), education level (no schooling, up to primary, middle, secondary, higher secondary, graduation & above), child labour history (never worked, child labour, non-child labour), child marriage (no, yes), life course household economic mobility (constant well-off, poor to well-off, well-off to poor, constant poor, others/mixed), tobacco and alcohol consumption (never, any, both), chronic multimorbidity (no, single, double, three or more), ADL/IADL limitations (no, single, double, three or more), depression (no, yes), participation in socio-physical activities (none, up to two activities, three or more activities), and place of residence (rural, urban).
In line with existing literature (Saha et al., Reference Saha, Rahaman, Mandal, Biswas and Govil2022), currently married indicates those who are married and currently living with their spouse, whereas ever married includes those who were married but are currently widowed, separated, or divorced. Never worked refers to individuals who were never engaged in any form of waged labour. Child labour denotes those who engaged in waged labour during childhood, while ‘non–child labor’ refers to individuals who engaged in waged labour only after childhood. Life course household economic mobility refers to changes in household wealth status from childhood to older adulthood (Ko et al., Reference Ko, Oh, Subramanian and Kim2025). Chronic morbidity includes self-reported hypertension, diabetes, cancer, lung and heart diseases, stroke, and arthritis. ADL and IADL include dressing, bathing, walking, eating, bedding, using the toilet, preparing a hot meal, shopping, telephoning, taking medicine, managing money, and getting around or finding an address in an unfamiliar place (Roy et al., Reference Roy, Saha, Rahaman, Kapasia and Chouhan2024). Socio-physical activities include visiting restaurants, parks, or relatives’ houses; engaging in indoor or outdoor games; and attending religious, political, or cultural functions (IIPS, 2020).
Statistical analysis
Univariate, bivariate, and multivariable binary logistic regression analyses were employed. Bivariate analyses were conducted to estimate the prevalence of adverse SRH across socio-demographic groups. The Pearson chi-square test was applied to assess statistical significance. The equation for the Pearson chi-square test is as follows:
 ${\chi ^{2\;}} = \sum {{{{{(O - E)}^2}} \over E}},$
${\chi ^{2\;}} = \sum {{{{{(O - E)}^2}} \over E}},$
where O refers to observed frequency in each cell, and E indicates expected frequency under the assumption that age and adverse health are independent. Multivariable binary logistic regression models were performed to predict the adjusted likelihood of adverse SRH. The likelihoods are presented in odds ratios (OR) with 95% confidence intervals (CI). Four separate models were performed to estimate socio-demographic, economic and behavioural/health-level predictors of adverse SRH. The equation of the multivariable binary logistic model is as follows:
 $\log \left( {{p \over {1 - p}}} \right) = {\beta _0} + {\beta _1}{X_1} + {\beta _2}{X_2} + \ldots {\beta _k}{X_k},$
$\log \left( {{p \over {1 - p}}} \right) = {\beta _0} + {\beta _1}{X_1} + {\beta _2}{X_2} + \ldots {\beta _k}{X_k},$
where p means probability of the adverse SRH, β0 indicates the intercept (log-odds when all predictors are at the reference level), X 1,X 2,…,X k represent predictors, β1,β2,…,β k indicate coefficients (log odds ratios) for predictors.
Exponentiating both sides:
 ${p \over {1 - p}} = {e^{{\beta _{0 + \beta 1X1 + \ldots .. + \beta kXk}}}}$
.
${p \over {1 - p}} = {e^{{\beta _{0 + \beta 1X1 + \ldots .. + \beta kXk}}}}$
.
Multivariable logistic regression model fit is assessed using the area under the ROC curve (AUC) and correct classification rate estimations in the supplementary (Figure 3).
 $\mathop \smallint \nolimits \int_0^1 TPR\left( {FPR} \right)dFPR$
$\mathop \smallint \nolimits \int_0^1 TPR\left( {FPR} \right)dFPR$
Distribution and transition of self-rated health (SRH) from childhood to later life among older adults, India, LASI Wave 1 (2017–2018).

where TPR refers to sensitivity, and FPR indicates false positive rate.
A multicollinearity test was performed using the variance in factors (VIF) before performing the regression model. All analyses were performed using Stata 17.0 and R 3.6.0 software.
Results
Description of the study participants
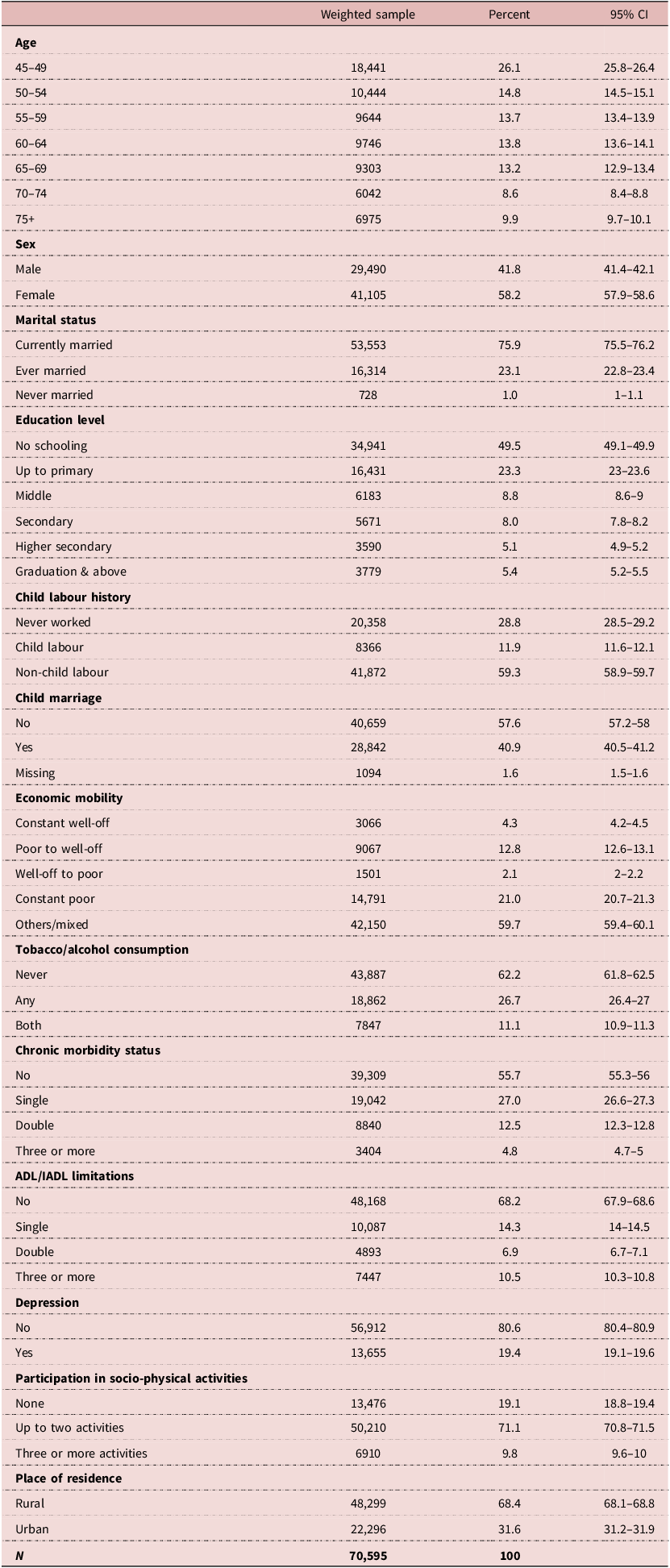
About one-fourth were aged 45–49 years (26%), followed by 50–54 years (15%) and 55–59 years (14%). More than half were females (58%) and were currently married (76%). Nearly half (49%) had no formal education, and about 10% reported having worked as labourers during childhood. One-fifth of the participants belonged to consistently poor households, while 13% had transitioned from poor to being well-off over their life course. Regarding health behaviours, 27% reported consuming either tobacco or alcohol, and 11% reported consuming both. About 27% had a single chronic morbidity, while 10% experienced multiple functional limitations. Nearly one-fifth (19%) were inactive in social and physical activities (Table 1).
Descriptive statistics of study sampled population, India LASI 2017–2018

Table 1 Long description
The table presents descriptive statistics of a study sampled population in India. It includes data on age, sex, marital status, education level, child labor history, child marriage, economic mobility, tobacco/alcohol consumption, chronic morbidity status, ADL/IADL limitations, depression, participation in socio-physical activities, and place of residence. The table has 19 rows and 5 columns. Column headers are Age, Sex, Marital status, Education level, and Child labour history. Row labels include age groups, sex categories, marital statuses, education levels, and child labor history statuses. The table provides the weighted sample, percent, and 95% confidence interval for each category. Notable trends include a higher percentage of females (58.2 percent) and currently married individuals (75.9 percent). Nearly half (49.5 percent) had no formal education, and about 10 percent reported having worked as laborers during childhood. One-fifth of the participants belonged to consistently poor households, while 12.8 percent had transitioned from poor to being well-off over their life course. Regarding health behaviors, 26.7 percent reported consuming either tobacco or alcohol, and 11.1 percent reported consuming both. About 27.0 percent had a single chronic morbidity, while 10.5 percent experienced multiple functional limitations. Nearly one-fifth (19.1 percent) were inactive in social and physical activities.
Note: Column based percentage distribution; CI Confidence Interval.
Life course SRH status
Figure 3 depicts the distribution and transition of SRH from childhood to older adulthood among adults aged 45 years and above. Panel A shows that 88.8% of respondents reported good health in childhood, 9.7% reported fair, and only 1.5% reported poor health. Panel B indicates a substantial deterioration in perceived health in later life, with only 42.7% rating their current health as good, 41.1% as fair, and 16.2% as poor. A clear rightward shift in the SRH distribution from childhood to adulthood, confirming a general decline in self-perceived health status over time (Panel C). Over half of the respondents (51.4%) transitioned from good to poor or fair health, reflecting an adverse health trajectory. About 36.2% maintained consistently good health, 7.0% remained constantly fair, 0.7% remained constantly poor, and only 0.4% improved from poor to good health (Panel D).
Levels and patterns of adverse SRH trajectory
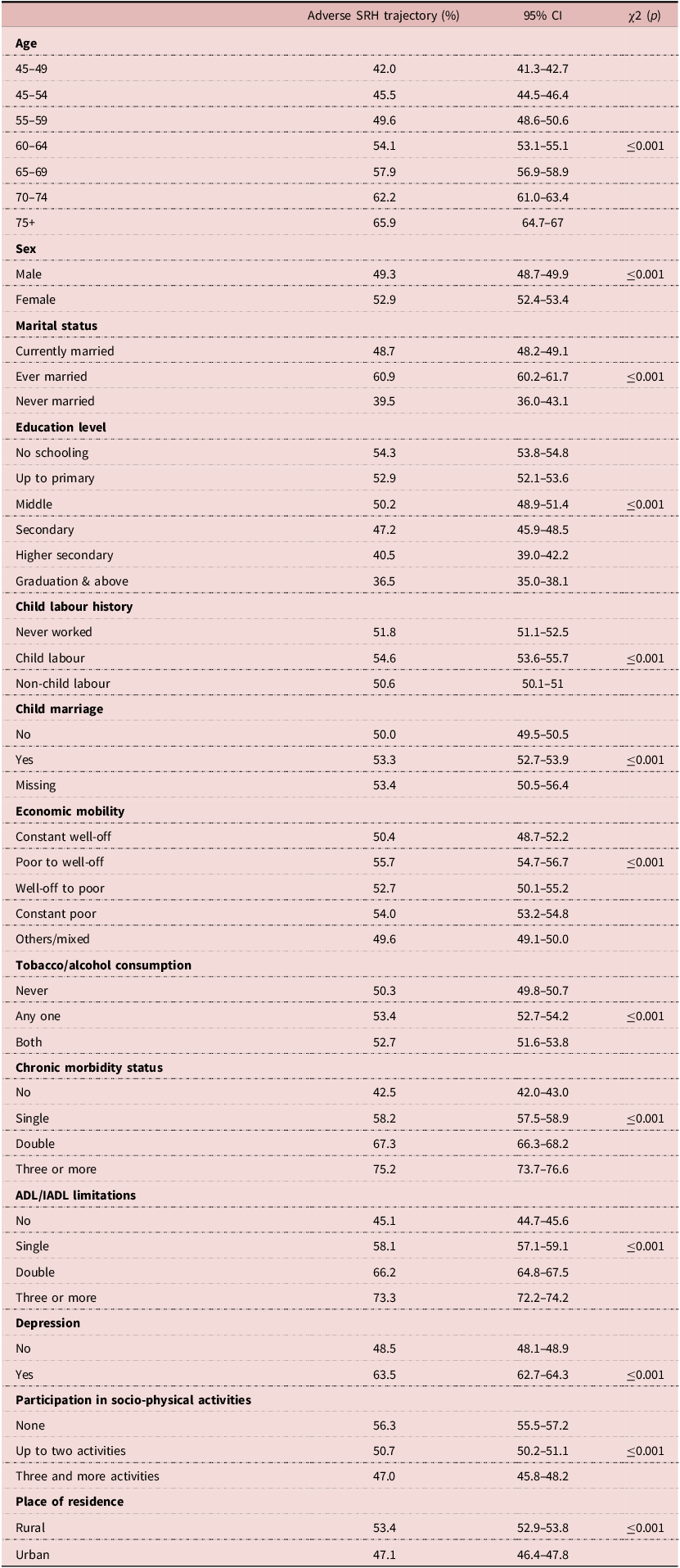
The prevalence of adverse SRH increased steadily with age, from 42% among adults aged 45-49 years to 65.9% among those aged 75 years and above (Table 2). Ever-married individuals (60.9%) showed a higher prevalence than those currently married (48.7%). Adverse SRH was more prevalent among those with child labour (54.6%), child marriage (53.3%), multimorbidity (≥75.2%), depression (63.5%), and three or more ADL/IADL limitations (73.3%) (p < 0.001). In contrast, graduate education (36.5%), participation with three or more socio-physical activities (47%), and urban residence (47.1%) were associated with lower prevalence.
Levels and patterns of prevalence adverse SRH among older adults, India LASI 2017–2018

Table 2 Long description
A table comparing the prevalence of adverse SRH among older adults in India based on various factors. The table has 20 rows and 5 columns. Column headers are Age, Adverse SRH trajectory (percent), 95% CI, and χ2 (p). Row labels include Age, Sex, Marital status, Education level, Child labour history, Child marriage, Economic mobility, Tobacco/alcohol consumption, Chronic morbidity status, ADL/IADL limitations, Depression, Participation in socio-physical activities, and Place of residence. Each row lists the percentage of adverse SRH trajectory, 95% confidence interval, and chi-square value with p-value. Notable trends include increasing prevalence with age, higher prevalence among ever-married individuals, those with child labour and child marriage, and those with chronic morbidity and depression. Lower prevalence is noted among graduates, those participating in socio-physical activities, and urban residents.
Note: Life Course Adverse SRH trajectory presented in row percentage; CI Confidence Interval.
A considerable state-level variation in the prevalence of adverse SRH among older adults was observed across India (Figure 4). The highest prevalence was reported in Tamil Nadu (78%), followed by Puducherry (73%), Punjab (67%), Kerala (65%), and West Bengal (64%). In contrast, the lowest prevalence of adverse SRH was found in Arunachal Pradesh (18%), followed by Meghalaya (18%), Andaman & Nicobar Islands (28%), Nagaland (31%), and Mizoram (34%).
State-level distribution of adverse self-rated health (SRH) trajectory among older adults, India, LASI Wave 1 (2017–2018).

Adjusted odds ratio of adverse SRH trajectory
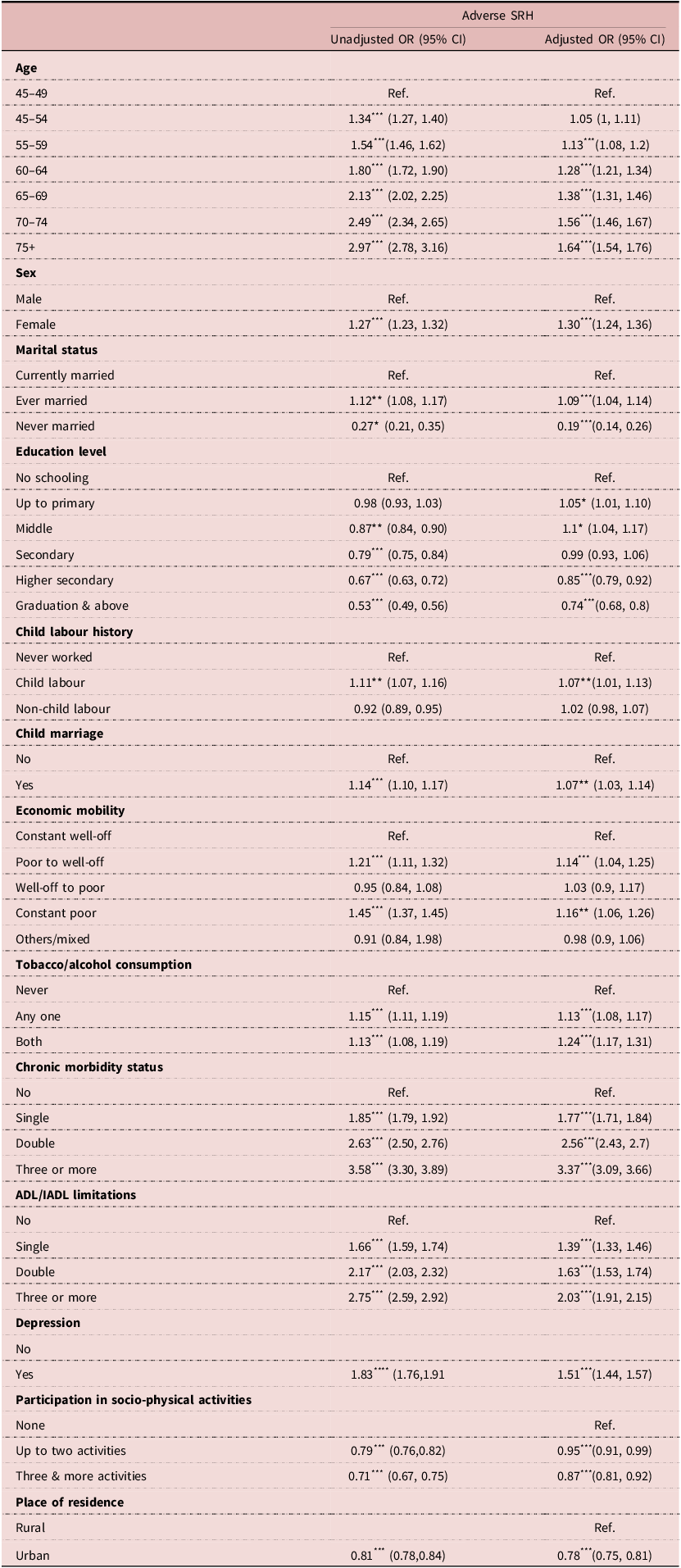
The adjusted likelihood of reporting an adverse SRH trajectory increased significantly with advancing age (Figure 5). Compared with adults aged 45–49 years, those aged 75 years and above had 1.64 (95% CI: 1.54–1.76) times higher odds of adverse SRH trajectory (Table 3). Women (AOR: 1.30; 95% CI: 1.24–1.36) and ever-married individuals (AOR: 1.09; 95% CI: 1.04–1.14) were more likely to report an adverse SRH, whereas those never married were less likely (AOR: 0.19; 95% CI: 0.14–0.26) to report an adverse SRH trajectory. Compared to those without formal schooling, individuals with higher secondary (AOR: 0.85; 95% CI: 0.79–0.92) and graduate-level education (AOR: 0.74; 95% CI: 0.68–0.80) were less likely to report poor SRH. Early-life disadvantages increased risk – those with child labour history (AOR: 1.07; 95% CI: 1.01–1.13), child marriage (AOR: 1.07; 95% CI: 1.03–1.14), or constant household poverty (AOR: 1.16; 95% CI: 1.06–1.26) had higher odds of adverse SRH. Those consuming tobacco or alcohol (AOR: 1.13; 95% CI: 1.08–1.17) and both substances (AOR: 1.24; 95% CI: 1.17–1.31) were more likely to report adverse SRH trajectory. Multimorbidity, functional limitations, and depression emerged as the strongest predictors, with three or more chronic conditions (AOR: 3.37; 95% CI: 3.09–3.66) and severe limitations (AOR: 2.03; 95% CI: 1.91–2.15) showing higher odds of adverse SRH trajectory than their reference groups. Conversely, social-physical activity (AOR: 0.87; 95% CI: 0.81–0.92) and urban residence (AOR: 0.78; 95% CI: 0.75–0.81) were protective factors.
Adjusted odds ratios (AOR) and 95% confidence intervals for predictors of adverse self-rated health (SRH) among older adults, India, LASI Wave 1 (2017–2018).

Unadjusted and adjusted odds ratios (AOR) for adverse SRH among older adults, India LASI 2017–2018

Table 3 Long description
A table comparing unadjusted and adjusted odds ratios (OR) for adverse self-rated health (SRH) among older adults in India, based on data from the Longitudinal Aging Study in India (LASI) 2017-2018. The table has 18 rows and 4 columns. Column headers are Age, Sex, Marital status, Education level, Child labour history, Child marriage, Economic mobility, Tobacco/alcohol consumption, Chronic morbidity status, ADL/IADL limitations, Depression, Participation in socio-physical activities, and Place of residence. Row labels include different categories within each column header. Values are presented as unadjusted OR (95% CI) and adjusted OR (95% CI). Notable trends include increasing odds ratios with advancing age, higher odds for females and ever-married individuals, and lower odds for those with higher education levels. Early-life disadvantages, tobacco/alcohol consumption, multimorbidity, and functional limitations increase the risk of adverse SRH, while social-physical activity and urban residence are protective factors.
Note: OR Odds Ratio; CI Confidence Intervals; Ref. Reference; ***p ≤ 0.001; **p ≤ 0.010; *p ≤ 0.050.
Discussion
India’s demographic and epidemiological transition – marked by an expanding ageing population and the growing burden of chronic diseases – necessitates a deeper understanding of life course subjective health trajectories. This study contributes to that discourse by contextualising adverse SRH trajectory among older adults through a life course approach, linking biological ageing, early-life adversity, and social inequality to perceived well-being.
The observed increase in adverse SRH with age is consistent with the cumulative risk framework (Feenstra et al., Reference Feenstra, Van Munster, MacNeil Vroomen, De Rooij and Smidt2020), reflecting the aggregation of biological wear, social disadvantage, and behavioural exposures over time. However, the substantial proportion of middle-aged adults (45–49 years) reporting adverse SRH trajectory suggests that health deterioration begins earlier in India, pointing to the need for midlife interventions to delay functional limitations and chronic disease onset. In line with earlier studies (Perianayagam, Reference Perianayagam2024), the gender gap in adverse SRH trajectory was evident, with women reporting worse SRH than men. Despite lower participation in risky behaviours, women experience compounded disadvantages through reproductive health burdens, nutritional deficits, unpaid caregiving, and restricted healthcare autonomy in India (Mbulo et al., Reference Mbulo, Murty, Zhao, Smith and Palipudi2021; Saha et al., Reference Saha, Rahaman, Mandal, Biswas and Govil2022). These findings align with gendered ageing theories, which emphasise that cumulative structural inequities – not biological vulnerability alone – drive women’s poorer self-perceived health in later life.
Aligning with the disablement process model (Verbrugge and Jette, Reference Verbrugge and Jette1994), multimorbidity and functional limitations remain key predictors of adverse SRH trajectory. Chronic conditions and functional impairments interact to diminish daily functioning and emotional well-being, reinforcing perceptions of ill health (Hossain et al., Reference Hossain, Yadav, Nagargoje and Vinod Joseph2021). Depression emerged as a significant predictor of adverse SRH, underscoring the interplay between psychological distress and perceived health. Consistent with previous studies (Roy et al., Reference Roy, Saha, Rahaman, Kapasia and Chouhan2024), depressive symptoms may amplify somatic complaints, reduce motivation for self-care, and heighten negative health appraisal. Therefore, integrating routine mental-health screening within geriatric and primary-care services is essential. Substance use also contributed to the adverse SRH trajectory, supporting prior Indian findings (Dolui et al., Reference Dolui, Sarkar, Hossain and Manna2023). Early-life adversity – such as child labour, child marriage, and persistent household poverty – was strongly associated with adverse SRH trajectory, illustrating the views of cumulative disadvantage theory. These findings are consistent with previous studies (Muhammad and Joy, Reference Muhammad and Joy2022; Ko et al., Reference Ko, Oh, Subramanian and Kim2025), which emphasise that childhood deprivation imposes long-term penalties on education, nutrition, and health capital. Although upward socioeconomic mobility in adulthood offers partial compensation, early physiological and psychosocial stress may have irreversible effects on ageing trajectories.
Conversely, education and socio-physical engagement were observed as significant resilience factors. Generally, education enhances health literacy, decision-making power, and access to healthcare (Elovainio et al., Reference Elovainio, Rosenström, Hakulinen, Pulkki-Råback, Mullola, Jokela, Josefsson, Raitakari and Keltikangas-Järvinen2016). Similarly, participation in social and physical activities was observed as a protective factor against adverse SRH, as such engagement fosters emotional and physical well-being (Wheatley and Buglass, Reference Wheatley and Buglass2019). However, with only one-fourth of India’s older population engaging in regular activity (IIPS, 2020), there is a missed opportunity to leverage Ayushman Arogya Mandir wellness interventions for active ageing. Marriage also appeared to serve a protective role against adverse SRH in this study. Social support theory suggests that a spouse can support emotional well-being, facilitate care-seeking, and safeguard against psychosocial stressors. Spouses often serve as companions in old age, especially as adult children become occupied with their own lives (Saha et al., Reference Saha, Rahaman, Mandal, Biswas and Govil2022).
A substantial state-level variation in the trajectory of adverse SRH among older adults in India is another important concern. Southern states – such as Kerala, Tamil Nadu, and Andhra Pradesh – recorded higher levels of adverse SRH compared with northern and northeastern regions. Higher prevalence of adverse SRH in the South may paradoxically signal more realistic health assessment, whereas lower prevalence in the Northeast may reflect health perception bias rather than superior health status. Finally, the persistent rural–urban divide underscores the structural dimension of ageing. Urban residents reported better SRH, likely due to improved healthcare access, infrastructure, and social networks. Bridging spatial variation through target-based healthcare delivery, geriatric outreach, and community-based wellness interventions is critical to ensuring healthy ageing across India’s diverse geographies (Adhikary et al., Reference Adhikary, Goyal and Akhtar2025).
Policy implications
Findings emphasise the need to strengthen India’s life course approach under the National Programme for Health Care of the Elderly (NPHCE) and the National Programme for Prevention and Control of Non-Communicable Diseases (NP-NCD). Early-life adversities such as child marriage and child labour require stronger enforcement of the Prohibition of Child Marriage Act (2006) and Child Labor (Prohibition and Regulation) Act (2016), complemented by awareness and education initiatives through Beti Bachao Beti Padhao and PM-Poshan. In later life, Ayushman Arogya Mandir wellness centres can promote social and physical activity, chronic disease screening, and geriatric care. Integrating these interventions can reduce the life course adverse health trajectory.
Limitations and strengths
This study has certain limitations. First, the primary outcome – adverse SRH trajectory – is based on subjective perception and may be influenced by individual cognitive and cultural interpretations of health. Second, the retrospective reporting of childhood SRH and early-life adversities is susceptible to recall and social desirability biases, potentially affecting temporal precision. Third, while the model’s predictive accuracy was acceptable (AUC: 0.718), the exclusion of other variables such as psychosocial stress and neighbourhood context may have constrained explanatory scope. The cross-sectional design of LASI Wave 1 further limits causal inference, underscoring the need for longitudinal follow-up.
Nonetheless, the study’s strengths are considerable. It employs a nationally representative dataset and an integrative life course framework, enabling a multidimensional assessment of biological, behavioural, and social determinants of ageing. By linking early-life adversity, adult health behaviours, and later-life outcomes, the study enriches theoretical understanding of cumulative disadvantage and provides empirically grounded evidence to inform equitable and context-sensitive ageing policy in India.
Conclusion
This study concludes that ageing in India is a socially patterned process, shaped by cumulative exposures across the life course rather than by biological decline alone. Early-life deprivation, multimorbidity, and functional impairments exacerbate vulnerability, while education, social participation, and supportive environments enhance resilience. By integrating a life course perspective, the study situates subjective health within broader structural and behavioural determinants. It underscores the need to embed equity-oriented, preventive, and participatory approaches within national ageing and NP-NCD programmes to transform longevity into a more inclusive, health-enabling, and socially sustainable experience of ageing in India.
Data availability statement
The present study uses secondary data, which is available from the International Institute for Population Sciences (IIPS), Mumbai, upon request for research purposes.
Acknowledgements
The Principal Investigator gratefully acknowledges the support of the Indian Council of Medical Research for providing human resource support under the project titled “Evaluating the Effect of the ICMR-NCTB Mudra Toolbox and Cognitive Harmony Program on Cognitive Health at Ayushman Arogya Mandir: A Multi-Centric, Mixed-Method Pragmatic Quasi-Experimental Trial” (Project ID: IIRPIG/DL-MH/2024-00208), which facilitated the development of this article.
Author contributions
Conceptualisation: UV, MR.
Data curation: UV, MR.
Formal analysis: UV, MR.
Investigation: UV, AG, OPB.
Methodology: UV, MR.
Project administration: UV.
Resources: AG, UV.
Software: UV, MR.
Supervision: UV, OPB, AG.
Validation: UV, AG, OPB, MR.
Visualisation: UV, MR.
Writing – original draft: UV, MR, AG, OPB.
Writing – review and editing: UV, MR, OPB, AG.
Funding statement
None.
Competing interests
We have no conflicts of interest to declare.
Ethics standard
An ethical waiver was obtained from the Institutional Human Ethics Committee (IHEC) of the All India Institute of Medical Sciences (AIIMS), Gorakhpur (AIIMS/GKP/IHEC/BMR/592).




 Open access
Open access