


Burnout, or a psychological response to chronic work-related stress characterized by feelings of emotional exhaustion, depersonalization, and diminished personal accomplishment (Maslach et al., Reference Maslach, Jackson and Leiter1997), is a serious occupational hazard associated with far-reaching health and societal consequences (Bridgeman et al., Reference Bridgeman, Bridgeman and Barone2018; Han et al., Reference Han, Shanafelt, Sinsky, Awad, Dyrbye, Fiscus, Trockel and Goh2019). Health care providers (HCPs) are at particular risk of burnout (West et al., Reference West, Dyrbye and Shanafelt2018) given the emotional intensity and demanding nature of their work (Agency for Healthcare Research and Quality, 2023), the evolving landscape of care provision due to technological innovation (i.e., electronic health records, new delivery approaches, physician order entry) (Shanafelt et al., Reference Shanafelt, Mungo, Schmitgen, Storz, Reeves, Hayes, Sloan, Swensen and Buskirk2016; Dyrbye et al., Reference Dyrbye, Shanafelt, Sinsky, Cipriano, Bhatt, Ommaya, West and Meyers2017), and the increased likelihood of burnout associated with long hours and shift work (Wisetborisut et al., Reference Wisetborisut, Angkurawaranon, Jiraporncharoen, Uaphanthasath and Wiwatanadate2014; Robertson et al., Reference Robertson, Elliott, Burton, Iversen, Murchie, Porteous and Matheson2016). Since the COVID-19 pandemic, HCP burnout rates have reached ‘crisis’ levels (Nigam et al., Reference Nigam, Barker, Cunningham, Swanson and Chosewood2023), with one in every two providers experiencing burnout often (Yellowlees et al., Reference Yellowlees, Coate, Misquitta, Wetzel and Parish2021). HCPs at safety-net hospitals, broadly defined as publicly funded hospitals that provide care regardless of a patient’s insurance status or ability to pay (Popescu et al., Reference Popescu, Fingar, Cutler, Guo and Jiang2019), may be at even greater burnout risk since they face unique challenges associated with caring for underserved communities: they see high acuity patients with multiple comorbidities and barriers to care (Figueroa and Jha, Reference Figueroa and Jha2018). High levels of HCP burnout are concerning in that they threaten healthcare quality (Khullar, Reference Khullar2023) and safety (Dewa et al., Reference Dewa, Loong, Bonato, Thanh and Jacobs2014); specifically, burnout is associated with increased medical errors (Tawfik et al., Reference Tawfik, Profit, Morgenthaler, Satele, Sinsky, Dyrbye, Tutty, West and Shanafelt2018; Owoe et al., Reference Owoc, Mańczak, Jabłońska, Tombarkiewicz and Olszewski2022; Li et al., Reference Li, Shah, Harness, Goldberg and Nash2023), reduced patient satisfaction (Anagnostopoulos et al., Reference Anagnostopoulos, Liolios, Persefonis, Slater, Kafetsios and Niakas2012), and poorer clinical outcomes (Mangory et al., Reference Mangory, Ali, Rø and Tyssen2021). Patients seeking care from safety-net hospitals have limited care options, therefore understanding factors that increase or mitigate the risk of burnout among HCPs in public healthcare systems is critical.
Research has consistently demonstrated a link between adverse childhood experiences (ACEs), defined as experiences of abuse, neglect, or household dysfunction before the age of 18 (Felitti et al., Reference Felitti, Anda, Nordenberg, Williamson, Spitz, Edwards, Koss and Marks1998), and burnout among physicians (Yellowlees et al., Reference Yellowlees, Coate, Misquitta, Wetzel and Parish2021) and other healthcare professionals (Clemens et al., Reference Clemens, Beschoner, Jarczok, Weimer, Kempf, Morawa, Geiser, Albus, Steudte-Schmiedgen, Gündel and Fegert2021; Williams et al., Reference Williams, Welindt, Hafferty, Stumps, Flanders and Williams2021; Williamson et al., Reference Williamson, Daniel, Carter, Ridenhour, Pulgar, Gay and Debinski2025). On average, half of HCPs report experiencing one or more ACEs (Stork et al., Reference Stork, Akselberg, Qin and Miller2020; Mercer et al., Reference Mercer, Cookson, Simpson-Adkins and van Vuuren2023). Notably, HCPs with higher childhood adversity scores report greater levels of compassion fatigue (Renkiewwicz and Hubble, Reference Renkiewicz and Hubble2021) and miss more days of work (Maunder et al., Reference Maunder, Lancee, Mae, Vincent, Peladeau, Beduz, Hunter and Leszcz2010). In addition, a recent study found that emergency medical service (EMS) professionals with personal histories of ACEs were at increased risk of vicarious traumatization (i.e., trauma symptoms resulting from exposure to traumatic experiences of patients; Renkiewicz and Hubble, Reference Renkiewicz and Hubble2023), opportunities for which are abundant in the medical profession. Considering the negative impacts of ACEs and burnout on HCPs’ personal and professional well-being, identifying strategies to minimize their effects and promote patient-centred, trauma-informed care is of utmost importance.
One factor that may buffer against ACEs’ impact on HCP burnout is resilience. While ongoing debate exists regarding its definition (Southwick et al., Reference Southwick, Bonanno, Masten, Panter-Brick and Yehuda2014), there is consensus that resilience involves the ability to successfully adapt or ‘bounce back’ from adversity (Connor and Davidson, Reference Connor and Davidson2003). Resilience has been found to buffer against burnout in Portuguese nurses and doctors (Ferreira et al., Reference Ferreira, Marques and Gomes2021), Australian general practitioner trainees (Cooke et al., Reference Cooke, Doust and Steele2013), and medical staff within a National Health Service Trust in the United Kingdom (McCain et al., Reference McCain, McKinley, Dempster, Campbell and Kirk2018). However, no studies have examined resilience’s potential protective role against burnout in the context of ACEs among HCPs. Thus, the current study (i) examines the association between ACEs and burnout in a sample of HCPs at a public healthcare system and (ii) explores whether this association is moderated by resilience. We hypothesize (H1) there will be a positive association between ACEs and burnout, and (H2) ACEs and resilience will interact to predict burnout, such that the association between ACEs and burnout will be attenuated by resilience.
Method
Participants and procedure
As part of a primary care-wide trauma-informed care initiative, HCPs at a public teaching hospital in a large city in the southeastern United States were recruited via electronic and paper flyers to complete an online survey assessing their trauma history and professional well-being. See Lathan et al. (Reference Lathan, Haynes, Langhinrichsen-Rohling, Sonu and Powers2023) and Powers et al. (Reference Powers, Langhinrichsen-Rohling, Sonu, Haynes and Lathan2024) for more information. For inclusion, participants must have provided direct patient care (i.e., physician/resident, nurse, medical assistant) within a primary care clinic at Grady Memorial Hospital at the time of the study, been able to read, speak, and understand English and been willing and able to participate in a research study and provide informed consent.
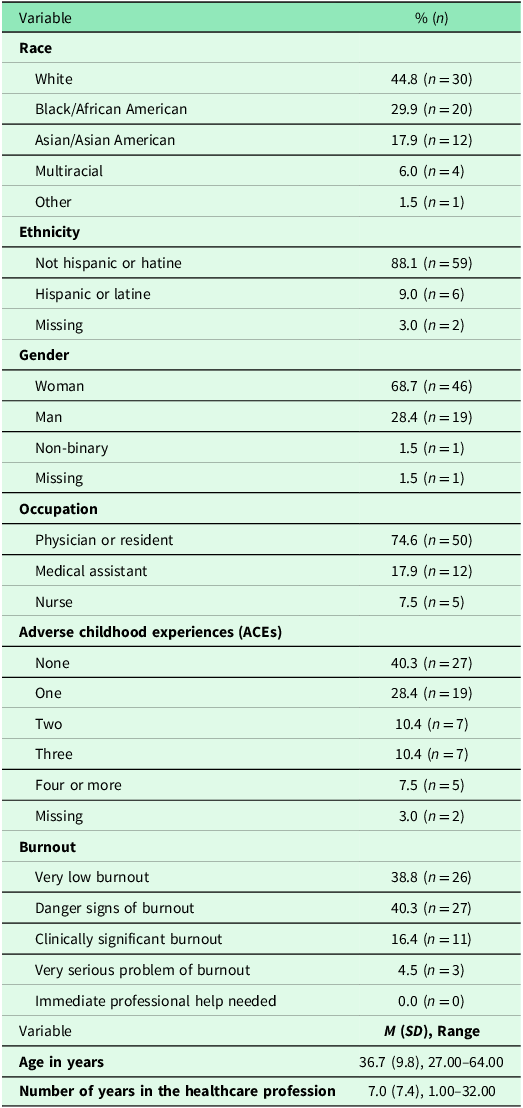
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional guidelines on human experimentation (i.e., Emory University Institutional Review Board and the Grady Research Oversight Committee) and with the Helsinki Declaration of 1975, as revised in 2008. After following the survey link/QR code in the recruitment advertisement, the study’s purpose was presented via a REDCap page. Electronic consent was required before proceeding to the survey items. Participants could opt out of answering any item. At the end of the survey, participants were debriefed, compensated $25, and offered a list of community resources. Sixty-seven HCPs completed the survey between May 2022 and August 2022 (68.7% women; 44.8% White; M age = 36.7 years, SD age = 9.8; Table 1).
Sample characteristics

Measures
Demographics
HCPs were asked to provide various demographic characteristics, including race, ethnicity, gender, occupation, and age. We also assessed healthcare-related experience via the following item: ‘How many years have you been working in the healthcare profession?’
ACEs
ACEs were assessed using the ACE Questionnaire (Felitti et al., Reference Felitti, Anda, Nordenberg, Williamson, Spitz, Edwards, Koss and Marks1998), a 10-item self-report measure assessing exposure to various forms of abuse, neglect, and household dysfunction before the age of 18. Each item is rated on a binary scale (0 = No, 1 = Yes) and items are summed to generate a total score, with higher scores indicating greater ACE exposure.
Resilience
The Connor-Davidson Resilience Scale-2 (CD-RISC-2; Vaishnavi et al., Reference Vaishnavi, Connor and Davidson2007), a 2-item self-report instrument developed as a brief version of the CD-RISC, was used to measure providers’ resilience (i.e., their ability to adapt and bounce back after stress). Responses are rated on a 0 (Not true at all) to 4 (True nearly all the time). Items were summed to generate a total score with a range of 0 to 8. Greater scores suggest higher levels of resilience. Cronbach’s alpha indicated good internal consistency (α = .86).
Burnout
Burnout was measured via the Burnout Measure, Short Version (BMS; Malach-Pines, Reference Malach-Pines2005), a unidimensional 10-item assessment of physical, emotional, and mental exhaustion. Participants were asked, ‘When you think about your work overall, how often do you feel the following?’ in relation to a range of burnout symptoms (e.g., trapped, ‘I’ve had it’). Responses are rated on a 1 (Never) to 7 (Always) scale. The BMS, an abbreviated version of the 21-item Burnout Measure (Pines and Aronson, Reference Pines and Aronson1988), has demonstrated validity and reliability among nurses (Malach-Pines, Reference Malach-Pines2005) and physicians (Alrawashdeh et al., Reference Alrawashdeh, Al-Tammemi, Alzawahreh, Al-Tamimi, Elkholy, Al Sarireh, Abusamak, Elehamer, Malkawi, Al-Dolat, Abu-Ismail, Al-Far and Ghoul2021). Mean scores are reported. Mean scores can indicate very low burnout (<2.4), danger signs of burnout (2.5–3.4), burnout (3.5–4.4), very serious problem of burnout (4.5–5.4), and immediate professional help needed (>5.5). Internal consistency was excellent (α = .90).
Data analyses
There were no missing burnout data. Two participants (3.0%) failed to respond to any ACEs items; these participants were removed from further analyses. Three participants (4.4%) had one ACE item missing; available data were summed to create a total score. Roughly 11.9% (n = 8) of resilience scores were missing. Skewness (.45–1.73) and kurtosis (.31–3.47) fell within normal ranges.
Descriptive statistics were conducted to identify rates of ACEs and burnout among the HCPs. A one-way analysis of variance was conducted with post-hoc LSD tests to examine mean differences in ACEs, burnout, resilience, and years of experience by occupation (physician/resident vs. medical assistant vs. nurse). A correlation matrix was generated to examine the bivariate relations among HCPs’ ACEs, resilience, burnout, and years of experience scores. Pairwise deletion was used, so sample sizes differ across analyses. Moderation models were then conducted using Hayes’ PROCESS Macro to assess for interaction effects of ACEs and resilience on burnout. ACEs was entered as the independent variable, burnout as the dependent variable, resilience as the moderator, and number of years in the healthcare field was entered as a covariate, given its potential association with burnout (Meredith et al., Reference Meredith, Bouskill, Chang, Larkin, Motala and Hempel2022). All variables were mean-centred. Listwise deletion was used for the moderation analysis. Statistical significance was defined as p < .05.
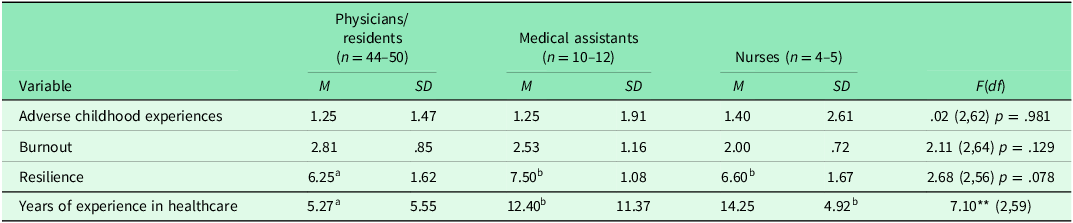
Results
On average, participants reported exposure to 1.26 ACEs (SD = 1.62). Fifty-seven percent of participants endorsed exposure to one or more ACEs (n = 38); 7.5% (n = 5) indicated exposure to four or more ACEs (Table 1). The mean burnout score was 2.70 (SD = .92). One in every five participants (20.9%; n = 14) reported significant levels of burnout, and 40.3% (n = 27) reported levels consistent with burnout ‘danger signs’. Roughly 38.8% (n = 26) of participants reported very low burnout. The mean resilience score was 6.49 (SD = 1.59). Number of ACEs, F(2,62) = .02, p = .98, burnout, F(2,64) = 2.11, p = .98, and resilience, F(2,56) = 2.68, p = .078, did not differ by occupation (see Table 3). Years working in the healthcare profession differed by occupation, F(2,59)=7.10, p = .002; specifically, medical assistants, M = 12.40, SD = 11.37, p = .004, and nurses, M = 14.25, SD = 4.92, p = .013, reported working more years in healthcare than physicians/residents, M = 5.27, SD = 5.55.
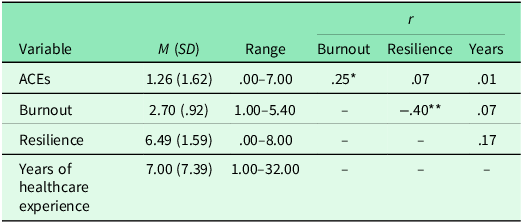
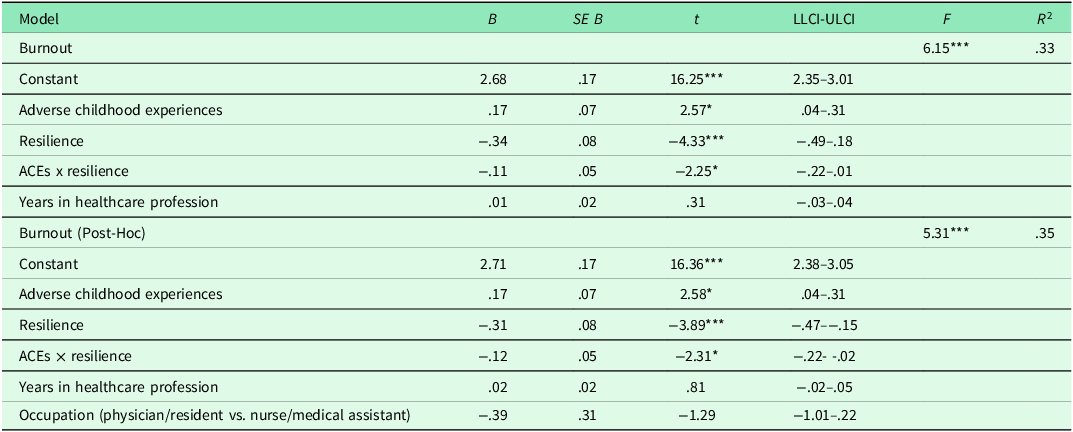
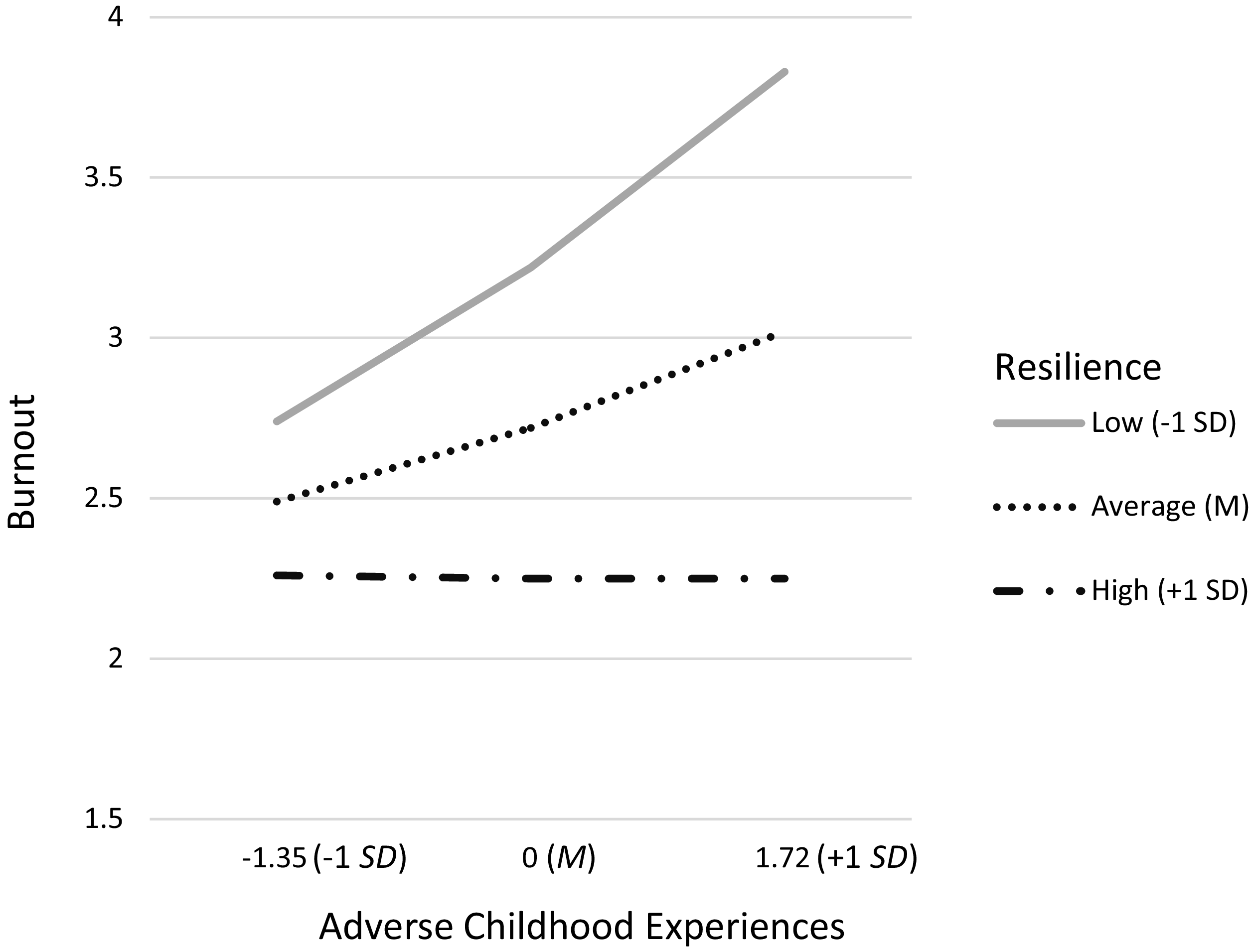
At the bivariate level, ACE scores were positively associated with burnout (H1; r = .25, p = .048), and resilience was negatively associated with burnout (r = −.40, p = .002; Table 2). The moderation analysis revealed main effects of ACEs, B = .17, SE = .07, p = .013, and resilience, B = −.34, SE=.08, p = .000, on burnout, when controlling for number of years in the healthcare profession, B = .01, SE = .02, p = .72 (Table 4). There was a significant interaction of ACEs and resilience on burnout, n = 55, B = −.11, SE = .05, p = .029 (Figure 1). A positive relation was found between ACEs and burnout for participants who reported low, t = 3.21, p = .002, and average, t = 2.57, p = .013, levels of resilience. The association between ACEs and burnout was nonsignificant at high levels of resilience, t = .01, p = .99. A post-hoc moderation analysis including occupation as a covariate was also conducted; given lack of mean differences across variables, nurses and medical assistant were collapsed into one group [nurses/medical assistants = 1] and compared to physicians/residents [physicians/residents = 0]). Moderation findings did not meaningfully differ when occupation was included as a covariate in the model. See Table 4.
Descriptive statistics and bivariate correlations

Note: ACEs = Adverse Childhood Experiences; n = 59–67; *p < .05, **p <.01, ***p<.001.
Group means and standard deviations by occupation

Note: means of groups with different subscripts are statistically different from one another; *p < .05, **p < .01, ***p <.001.
Summary of moderation analysis for ACEs predicting burnout by resilience level

n = 55; *p < .05, **p < .01, ***p < .001.
Interaction of adverse childhood experiences and resilience on health care provider burnout controlling for years in healthcare profession and occupation.
Note: Low resilience, β = .36, SE = .11, t = 3.26, p = .002. Average resilience, β = .17, SE = .07, t = 2.58, p = .013. High resilience, β = −.003, SE = .10, t = −.03, p = .975.

Discussion
The current study assessed the relations among ACEs, resilience, and burnout among HCPs in primary care clinics at a safety-net hospital. While previous research has demonstrated that HCP burnout is positively associated with ACEs (Robertson et al., Reference Robertson, Elliott, Burton, Iversen, Murchie, Porteous and Matheson2016; West et al., Reference West, Dyrbye, Sinsky, Trockel, Tutty, Nedelec, Carlasare and Shanafelt2020; Clemens et al., Reference Clemens, Beschoner, Jarczok, Weimer, Kempf, Morawa, Geiser, Albus, Steudte-Schmiedgen, Gündel and Fegert2021; Yellowlees et al., Reference Yellowlees, Coate, Misquitta, Wetzel and Parish2021; Williamson et al., Reference Williamson, Daniel, Carter, Ridenhour, Pulgar, Gay and Debinski2025), but negatively associated with resilience (Cooke et al., Reference Cooke, Doust and Steele2013; McCain et al., Reference McCain, McKinley, Dempster, Campbell and Kirk2018; Ferreira et al., Reference Ferreira, Marques and Gomes2021), this study is the first to examine resilience as a potential protective factor in the association between ACEs and burnout among HCPs in primary care.
In support of H1 and consistent with previously mentioned studies, HCPs who endorsed more ACEs reported higher levels of burnout. In addition, this association was moderated by resilience, even when controlling for the number of years in the healthcare profession (H2). More specifically, experiencing more ACEs correlated with experiencing greater burnout among HCPs with low-to-average resilience. For HCPs with higher levels of resilience, however, the association between ACEs and burnout was no longer significant. Overall, current findings suggest that the presence of resilience traits may help mitigate, or even prevent, burnout among all HCPs; however, it seems to be particularly beneficial for those with ACE histories.
Thus, it is imperative that hospital and clinic administrators emphasize the importance of building resilience among HCPs that provide care within the larger healthcare system (Shanafelt, Reference Shanafelt2021). Given few disclose psychological distress to their workplace (Zamir et al., Reference Zamir, Tickle and Sabin-Farrell2022), healthcare organizations may benefit from following universal precaution as a trauma-informed approach (Substance Abuse and Mental Health Services Administration, 2014) by understanding the impact of ACEs on HCP well-being, identifying the signs and symptoms of trauma and burnout, and offering hospital-wide opportunities to enhance resilience. Perhaps, a viable path to decreased burnout and enhanced resilience involves routine, system-wide exposure to trauma-informed professional development or self-care opportunities (Sood et al., Reference Sood, Prasad, Schroeder and Varkey2011). A specific intervention that has demonstrated particular effectiveness among HCPs is Mindfulness in Motion, an 8-week modified mindfulness-based intervention designed for nurses in chronically high-stress environments and to be delivered on-site, during work hours and in a group setting (Klatt et al., Reference Klatt, Steinberg and Duchemin2015). Notably, the effects of the intervention were sustained for 12 months (Klatt et al., Reference Klatt, Westrick, Bawa, Gabram, Blake and Emerson2022), suggesting adequate dosage could be achieved through annual participation. Even further, intentionally incorporating information on the link that exists between psychosocial experiences and overall health – in both patients and HCPs – may increase the trauma-informed nature of existing interventions, which is key for HCPs regularly interfacing with trauma-exposed populations. Notably, HCPs with ACE histories have more favourable attitudes towards trauma-informed care (Selwyn et al., Reference Selwyn, Lathan, Platt and Minchew2023), highlighting the importance of attracting and retaining HCPs with lived experiences, especially in organizations dedicated to building a resilient workforce.
When considering findings, certain limitations must be taken into account. For example, this study used a cross-sectional design, which prohibits causal conclusions regarding the directionality of the association between ACEs and burnout. Also, this study only measured ACEs among HCPs; however, many other types of traumatic events can influence provider burnout, such as workplace violence (Mento et al., Reference Mento, Silvestri, Bruno, Muscatello, Cedro, Pandolfo and Zoccali2020) and secondary trauma (Leung et al., Reference Leung, Schmidt and Mushquash2023). Other limitations concern the small sample sizes, especially in relation to medical assistant and nurse participants, as well as the need to collapse physicians/residents into one group due to a subset of current residents selecting ‘physician’ as their occupation. Replication in larger samples with more sizable and distinct groups of residents, physicians, nurses, and medical assistants is needed.
Conclusions
While the precise definition of resilience is still debated and biomedical research on resilience is in its nascent phase, these findings indicate that resilience is particularly important for HCP well-being, increasing capacities to bounce back amidst the rigours of highly intense, demanding, and emotionally challenging work. Such implications are especially important for HCPs working in safety-net or resource-limited settings as well as those with higher cumulative ACEs. As research continues to elucidate risk factors associated with burnout – such as stressful work environments and ACEs – promoting resilience will be of increasing importance both individually and institutionally (Figueroa and Jha, Reference Figueroa and Jha2018). Consequently, further research is needed to understand how resilience can be cultivated and supported. Finally, it is important to note that an imbalanced overemphasis of resilience without interrogating and understanding the external conditions that demand its presence can be highly problematic and inadvertently deflect attention from necessary system-level reform. In healthcare, therefore, promoting resilience should not replace institutional efforts to mitigate burnout nor be used to justify or maintain unsafe cultures and policies.
Disclosures
The authors have no conflicts of interest to disclose.
Funding statement
This work was supported by the Emory Medical Care Foundation (grant awarded to TH, AP, SC, and ECL).
All authors have read the manuscript and agree to it being submitted for publication. All individuals listed as authors meet the appropriate authorship criteria. This work has not been previously published and is not under consideration elsewhere. This study followed ethical guidelines and was approved by Emory University Institutional Review Board and the Grady Hospital Oversight Committee. We have no conflicts of interest to disclose

 Open access
Open access