


Introduction
Breastfeeding is a critical component of infant nutrition and development, recognized globally for its numerous health benefits. 1–Reference Koray, Wanjiru and Kerkula4 The World Health Organization (WHO) recommends initiating breastfeeding within 1 hour of birth, exclusive breastfeeding (EBF) during the first 6 months of life, and continued breastfeeding up to 2 years of age or beyond. 5 However, achieving optimal breastfeeding practices remains a significant challenge worldwide, Reference Zong, Wu, Zhao, Magnussen and Xi6 and fewer than half of infants in low- and middle-income countries (LMICs) are breastfed optimally to these standards. Reference North, Gao, Allen and Lee7 In sub-Saharan Africa recent data across 25 countries indicate a pooled prevalence of EBF of 49%, Reference Koray, Wanjiru and Kerkula4 however, EBF rates are declining and point to only four African countries being likely to meet the WHO’s 2030 EBF target. 5,Reference Mohammed, Calvert and Webb8
Suboptimal rates of breastfeeding are associated with 45% of child deaths globally, Reference Black, Allen and Bhutta9 and contribute to malnutrition. Reference Kinshella, Prasad and Hiwa10 In the context of the developmental origins of health and disease (DOHaD), breastfed infants are less likely to become sub-optimally nourished, and both stunting and obesity in infancy are associated with an increased risk of developing non-communicable diseases (NCDs) in adult life, including type 2 diabetes. Reference Hanson, Gluckman, Ma, Matzen and Biesma11–Reference Horta, Loret de Mola and Victora13 Data collected between 2017 and 2022 from 24 LMICs estimated that 149 million children under the age of five were stunted, while 38.9 million were overweight or obese. Reference Birhanu, Yitbarek, Bobo, Atlantis and Woldie14 Stunting in infancy is strongly associated with chronic diseases such as high blood pressure, heart disease, and stroke in later life, Reference Soliman, De Sanctis and Alaaraj15 and infants who gain excessive weight are at a higher risk of becoming obese and developing type 2 diabetes as adults. Reference Horta, Loret de Mola and Victora13
In Africa, the situation is particularly concerning; sub-Saharan Africa bears a disproportionate burden of under-five child mortality. Reference Black, Allen and Bhutta9,Reference Kinshella, Prasad and Hiwa10 Appropriate breastfeeding practices are central to reducing both mortality and malnutrition and also to achieving other short- and long-term health benefits. Reference Binns, Lee and Low3,Reference Pretorius, Asare, Genuneit, Kruger and Ricci16 Importantly, in the context of burgeoning health care costs, future benefits would likely include a reduction in the economic losses resulting from NCDs acquired in adult life. Reference Rollins, Bhandari and Hajeebhoy17
While women have been the principal targets for DOHaD-related interventions, including the promotion of breastfeeding and other parental roles able to optimize fetal and newborn health through the first 1000 days of life, this paradigm can inappropriately focus responsibility for infant health outcomes on mothers and inadvertently deflect attention from other windows for intervention. Reference Pentecost, Macnab, Mayekiso and Ross18 Clearly it is relevant for both genders to learn the immediate and longer-term benefits of optimal maternal and infant health and nutrition, Reference Macnab and Mukisa19 and the promotion of successful breastfeeding is not the sole responsibility of a woman. Reference Rollins, Bhandari and Hajeebhoy17 Importantly, fathers who understand the benefits of breastfeeding can significantly support mothers who want to breastfeed to succeed. Reference Ogbo, Akombi and Ahmed20 In this context, engagement with adolescents through school-based health promotion offers a unique opportunity to engage with both boys and girls at a key age point in the DOHaD trajectory by educating the parents of tomorrow, Reference Tohi, Tu’akoi and Vickers21 and it is known that knowledge and behaviors learned in adolescence can impact self-efficacy and translate into positive lifestyle choices evident in adult life. Reference Viner, Ozer and Denny22,Reference Macnab23
In school-based health promotion related to DOHaD, prior research has identified that some facts and issues resonate more with adolescents than others. Reference Macnab and Mukisa19 For this reason, more effective engagement in breastfeeding education could be promoted by pre-intervention inquiry to identify where interest exists and what outcomes are perceived as relevant. More effective engagement could then lead to greater acquisition of knowledge with greater potential to influence future behavior. Studies also provide some evidence of gender- and culturally related differences in adolescents’ comprehension of DOHaD concepts in addition to indicating low levels of understanding. Reference Tohi, Tu’akoi and Vickers21 Hence, it has been suggested that a prime target for study is the potential benefit of incorporating gender-specific educational messages based on what girls and boys, respectively, perceive as most relevant. Reference Davies, Macnab and Byass24
Dialog with an adolescent audience may also help to determine if they have preconceived perception or bias that could present unique barriers or offer unique opportunities. Despite strong cultural support for breastfeeding, the reality is that African mothers who want to breastfeed face numerous challenges. Reference Apanga25,Reference Zegeye, Gebrehana and Bezabih26 In Nigeria, poor access to breastfeeding counseling services and inadequate healthcare infrastructure hinder optimal breastfeeding. Reference Zegeye, Gebrehana and Bezabih26 Zambia faces similar issues, with additional challenges related to maternal education and community support. Reference Jacobs, Michelo and Chola27 In South Africa, the prevalence of EBF is low, partly due to socioeconomic disparities and the high prevalence of HIV, which complicates breastfeeding practices. Reference Goon, Ajayi and Adeniyi28 And, Ghana, while showing some progress, still struggles with cultural beliefs and practices that discourage EBF. Reference Tampah-Naah, Kumi-Kyereme and Amo-Adjei29
Our hypothesis was that in the context of school-based health education to promote breastfeeding, inquiry can identify those elements most likely to interest and engage girls and boys in the target population. The objective was to use questionnaire-based responses to evaluate the impact on pupils of an in-class session summarizing the core benefits of breastfeeding promoted by WHO, 1 and principles of early nurturing care related to DOHaD. Reference Pietrobelli and Agosti30–Reference Britto, Lye and Proulx32 The purpose of these data was to identify if the teaching session provided knowledge and insights that altered the pupils’ perceptions about breastfeeding and discover from their ranking of the benefits of breastfeeding explained in the session what elements girls and boys, respectively, found to be of most and least interest.
Methods
This observational study involved senior year classes of pupils in secondary schools in 5 African countries: Ghana, Malawi, Nigeria, South Africa and Zambia. In each country, university ethics board approval was obtained. Schools were contacted to obtain permission to conduct an in-class health education session on the benefits of breastfeeding. In each country, the local members of the research team used the same format and content for the education session and evaluated the pupils’ preferences using the same printed questionnaires. All students in the class were eligible to participate, and every student assented or consented to take part dependent on their age before participation. All contributions were anonymous; the responses each student provided were not identified by either name or number.
The investigator introduced the session by explaining to the class that pupils would have the opportunity to enter their responses to a series of written questions related to the content of the presentation. Specifically pupils were asked to (1) identify how what they had heard impacted what they already knew, and (2) rank their level of interest in different elements of the topic. To ensure understanding of what was being asked, as the printed questionnaires were written in English, each question was read out by the investigator and shown on flip charts written in the local language.
Two questionnaires were developed for this project (see appendix). Development involved consultation with each of the researchers; consideration was given to possible differences in social focus or cultural perception in each country, with the aim of avoiding issues related to the use of the same questionnaire in different countries. An iterative process was followed; no formal trial of these materials was conducted, but age-appropriate comprehension was confirmed by asking a 14-year-old high school pupil in Uganda to paraphrase the meaning of each question. The final versions used were approved by the ethics review boards in each country.
Both questionnaires were administered prior to the education session to obtain baseline data from each pupil and then repeated after the intervention to evaluate the effect of the information presented. Questionnaire 1 assessed knowledge and awareness related to parenthood and nurturing care concepts through 10 questions answered by Yes/No responses. Questionnaire 2 evaluated the relevance to each pupil of DOHaD concepts related to breastfeeding. To do this, girls and boys ranked their level of interest in three facts about feeding a baby, choosing either most interesting, interesting, or least interesting in four categories: (1) benefits to the baby, (2) benefits to the mother, (3) benefits to the father, and (4) benefits to the community and society.
The education session was given as a PowerPoint presentation to explain to the class the importance of the first 1000 days of life, the place of nurturing care by parents, and the benefits of breastfeeding; this was based on content from position statements on breastfeeding by the WHO 1 and principles of early-life nurturing care related to DOHaD. Reference Pietrobelli and Agosti30–Reference Britto, Lye and Proulx32 The content expanded on the knowledge and concepts summarized in Questionnaires 1 and 2. Open dialog followed completion of the post-intervention questionnaires; pupils were able to ask clarity-seeking questions and relate relevant examples from their own experience.
Statistical analysis
To determine the top-ranked items (response rate (%) and the aspects of breastfeeding ranked most and least interesting, the pupils’ pre- and post-questionnaire data and rankings were combined with content coding. Kendall’s coefficient of concordance, Chi-square, and McNemar test were used in the statistical analysis; p values were considered significant when they were less than 0.05.
Results
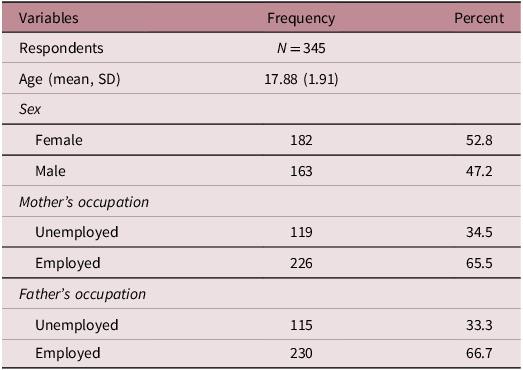
Seven schools, 2 in Ghana, 2 in South Africa, and 1 in Malawi, Nigeria, and Zambia hosted the educational sessions, and 345 pupils participated. Table 1 presents the respondents’ demographic information; their average age was 17.88 years (SD 1.91). The sample was closely split by gender (52.8% female and 47.2% male); 65.5% of pupils’ mothers and 66.7% of fathers were employed.
Demographic information of respondents

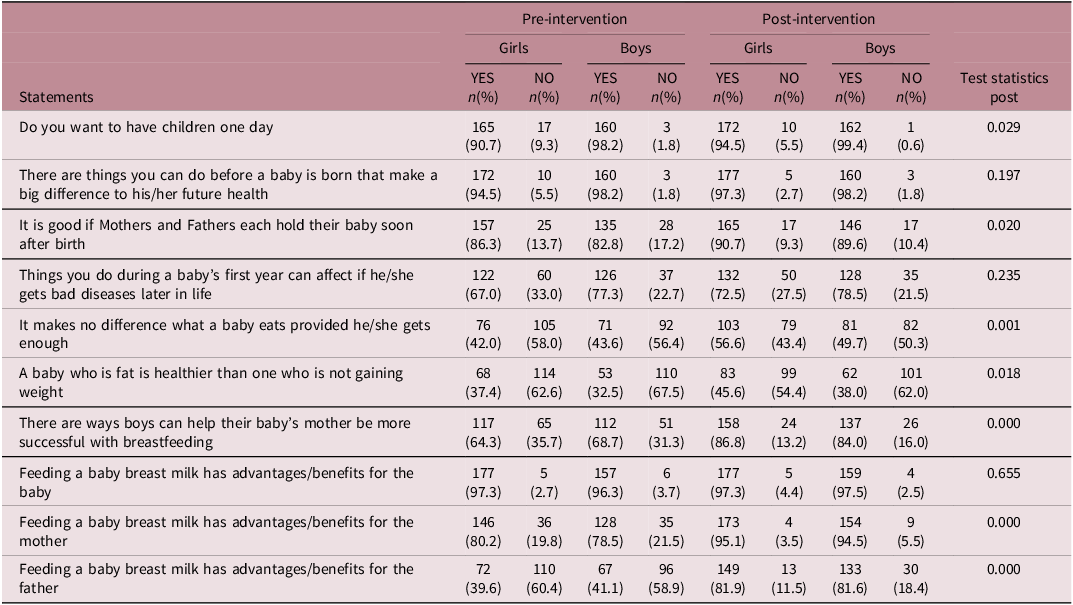
Table 2 shows the pupils’ initial responses to concepts about being parents and the contribution of breastfeeding as documented on questionnaire 1, and also how their perceptions changed following the educational intervention when questionnaire 1 was readministered. The majority of both genders indicated they “wanted to have children one day” (boys 98.2% and girls 90.7%); girls intent increased post-intervention (94.%); boys remained unchanged. Comparing statements 2–10, post-intervention the number of girls who gave the correct answer to each statement increased, except for one which remained unchanged: “Feeding a baby breast milk has advantages/benefits for the baby” had the highest number of correct answers (97.3%) pre- and post-intervention. Similarly, the number of boys answering correctly also increased except for 1 unchanged statement: “There are things you can do before a baby is born that make a big difference to his/her future health” had the highest number of correct answers pre- and post-intervention (98.2%) Overall, 98.7% of respondents gave correct answers following the education session compared to 92.4% before; the McNemar test (p-value > 0.001) confirms that this change is statistically significant.
Questionnaire data: pre- and post-intervention responses divided by gender

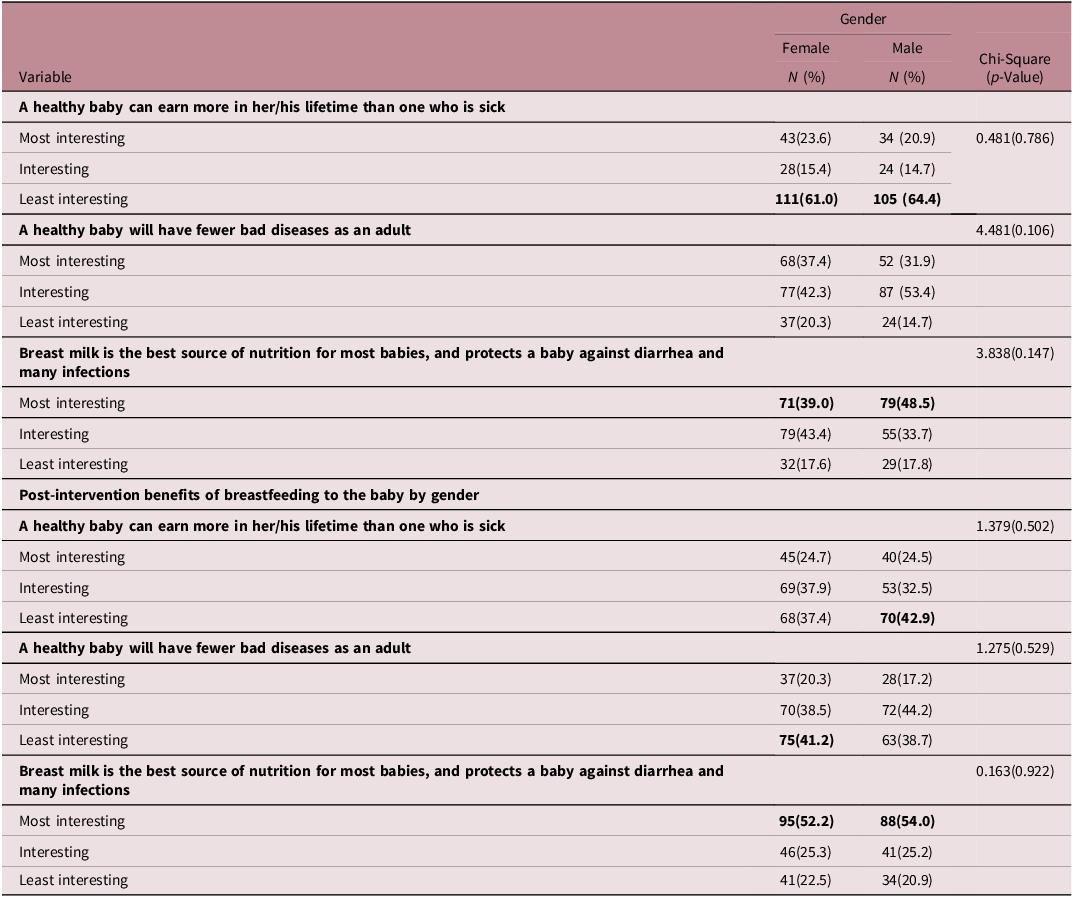
Tables 3–6 show Questionnaire 2 data separated by gender for pupils’ pre- and post-intervention rankings of their interest in known benefits of breastfeeding to the baby, the mother, the father, and the community, respectively. The impact of the education session is reflected by changes made by both girls and boys in their ranking for many of the concepts. A significant gender-based difference was evident in how boys and girls ranked their interest regarding a specific benefit to the father.
Pre-intervention benefits of breastfeeding to the baby by gender

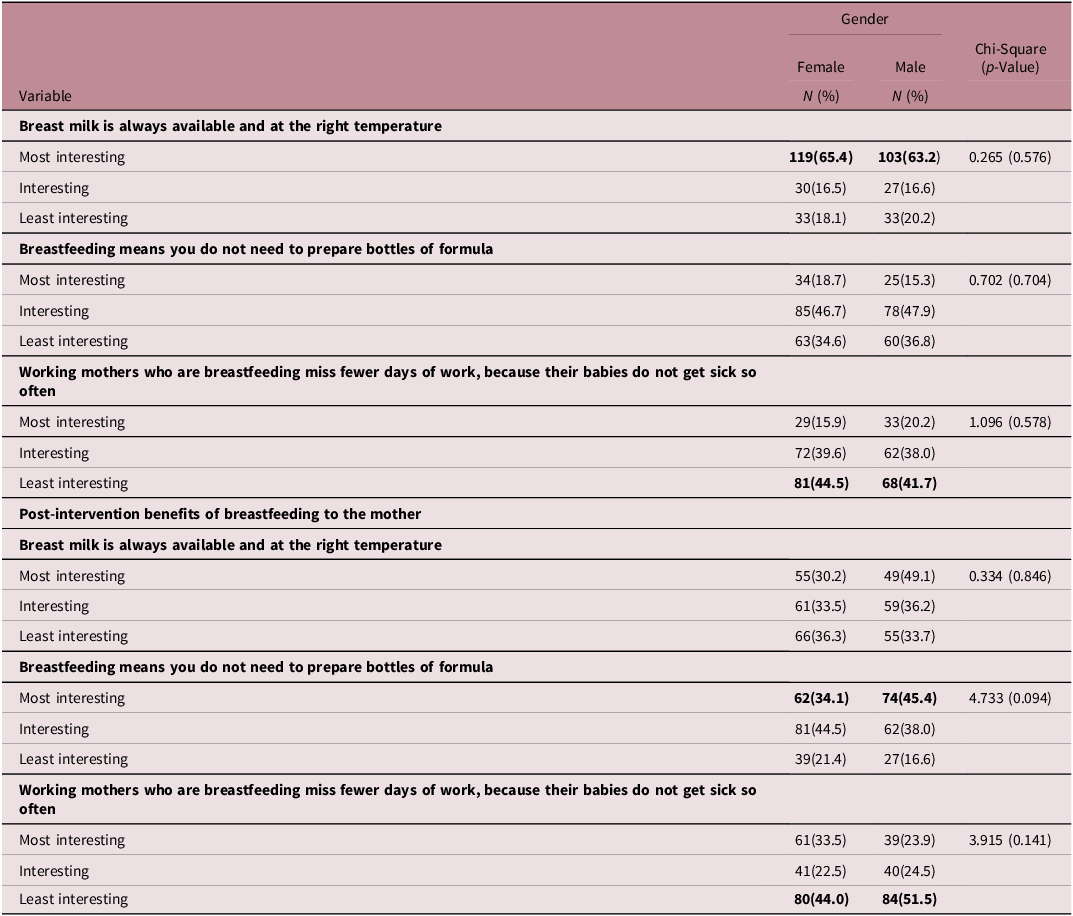
Pre-intervention benefits of breastfeeding to the mother

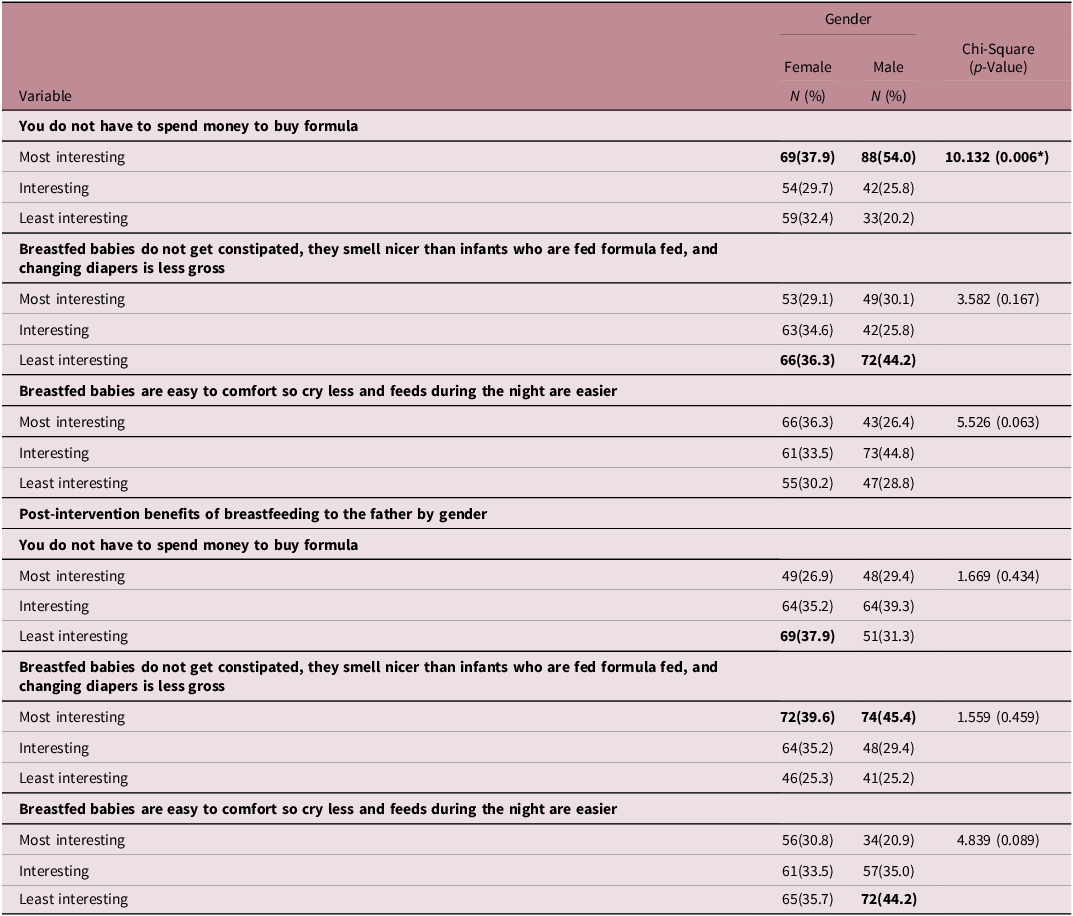
Pre-intervention benefits of breastfeeding to the father by gender

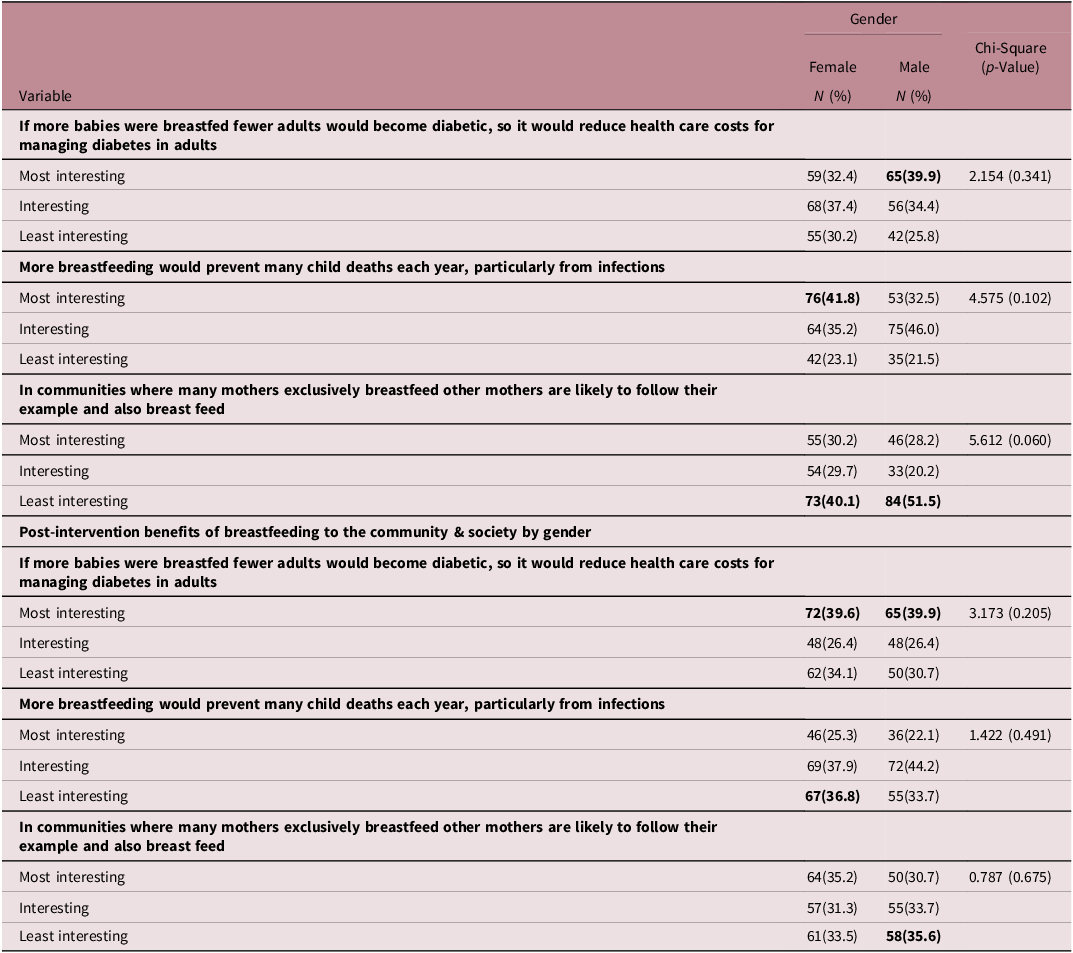
Pre-intervention benefits of breastfeeding to the community and society by gender

On benefits to the baby (Table 3), pre-intervention “Breast milk is the best source of nutrition for most babies and protects a baby against diarrhea and many infections” was ranked as the most interesting fact, by 39% of girls, and 61% ranked “A healthy baby can earn more in her/his lifetime than one who is sick” as least interesting. Boys’ rankings were similar (48.5% and 64.4%, respectively).
Post-intervention 52.2% of girls now ranked “Breast milk is the best source of nutrition for most babies and protects a baby against diarrhea and many infections” as most interesting, and “A healthy baby will have fewer bad diseases as an adult” as least interesting (41.2%). Boys most interesting fact continued to be the beneficial effect of breast milk on infections, with the number increasing to 54%. Boys’ least interesting fact remained “A healthy baby can earn more in her/his lifetime than one who is sick,” but the number choosing this fell (42.9%).
On benefits to the mother (Table 4), pre-intervention both girls and boys ranked “Breast milk is always available and at the right temperature” as most interesting (65.4% and 63.2%, respectively); there was also agreement that the least interesting fact was that “Working mothers miss fewer days of work because their babies do not get sick so often,” (44.5% and 41.7%).
Post-intervention most girls and boys now ranked “Breastfeeding means you do not need to prepare bottles of formula” as most interesting (34.1% and 45.4%). Both girls and boys continued to rank “working mothers who breastfeed miss fewer days of work” as least interesting (girls 44% and boys 51.5%).
On benefits to the father (Table 5), pre-intervention boys and girls agreed that “You do not have to spend money on formula” was most interesting, but the number of boys that selected this fact was significantly greater – 54% of boys versus 37.9% of girls (p = 0.006). Boys and girls also agreed on what was least interesting; 44.2% and 36.3%, respectively, chose “Breastfed babies don’t get constipated, they smell nicer than infants who are fed formula, and changing diapers is less gross.”
Post-intervention there was again agreement between the genders, but the fact ranked most interesting had now changed to “Breastfed babies don’t get constipated, they smell nicer than infants who are fed formula, and changing diapers is less gross” (boys 45.4% and girls 39.6%). Both genders’ least interesting ranking had also changed, with boys now choosing “Breastfed babies are easy to comfort so cry less, and feeds during the night are easier” (44.2%), while girls selected “You do not have to spend money on formula” (37.9%).
On benefits to the community (Table 6), pre-intervention girls ranked “More breastfeeding would prevent many child deaths each year, particularly from infections” as most interesting (41.8%), while boys chose “If more babies were breast fed fewer adults would become diabetic, so it would reduce health care costs for managing diabetes in adults” (39.9%). Girls and boys both ranked the fact that “In communities where many mothers exclusively breastfeed other mothers are likely to follow their example and also breast feed” as least interesting (40.1% and 51.5%, respectively).
Post-intervention boys’ most interesting ranking remained the same, and girls now also ranked the potential for breastfeeding to reduce healthcare costs for managing diabetes in adults as most interesting (39.6%). Girls also changed their most interesting ranking pre-intervention (prevention of deaths from infection) to least interesting (36.8%). And more boys now found it either most interesting or interesting that in communities where many mothers exclusively breastfeed, other mothers are likely to follow their example (64.4% versus 48.4% pre-intervention).
Discussion
This study confirmed the feasibility of delivering school-based education on DOHaD-related concepts about parenthood and nurturing care and the benefits of breastfeeding, that adolescents can be engaged to learn about these topics, and that facts shared impact the knowledge and attitudes of the target audience.
Pre- and post-intervention assessment by questionnaire indicated that participating adolescents acquired knowledge that altered their perceptions, and also that girls’ and boys’ level of interest in several key facts about the benefits of breastfeeding changed after the education session. In this way we identified that the intervention was effective in achieving an impact, at least in the short term, but it remains unknown if the impact from the education session will translate into improved breastfeeding rates in the future.
We came to understand which aspects of the DOHaD-themed education shared with the pupils were most likely to make them want to learn more about how to help make breastfeeding happen when they become parents. We also identified those aspects which the adolescents ranked as least interesting. We suggest that a similar inquiry to obtain such data will enable educators to deliver better-focused health promotion. Identifying where there is a lack of interest allows special attention to be given where teachers revisit the topic to underscore messages from the initial education session, or where educators from outside the school return for further in-class sessions. In addition, important elements of DOHaD science, key knowledge, or formative parenting skills that the adolescents’ responses indicate were not of interest and may in fact not have been understood or viewed as relevant can also be revisited.
In a prior study, pupils were asked during the initial in-class session to indicate which aspects of DOHaD science interested them most by a show of hands in response to questions written in the local language on a flipchart. Reference Macnab and Mukisa19 If pupils’ responses are obtained in this way in “real time,” their feedback can be used to guide the current in-class discussion, so that key knowledge that is not fully appreciated can be explained and put in context. Awareness of differences in girls’ and boys’ rankings of relevance also enables educational content to be targeted to attract and inform both genders. In this regard, a statistically significant difference in the level of interest in the cost-benefit of breastfeeding was evident between boys and girls.
DOHaD-related school-based education is relevant as studies highlight a generally low understanding of the importance of the first 1000 days of life in adolescents, Reference Tohi, Tu’akoi and Vickers21,Reference Tohi, Tu’akoi and Vickers33 and as they are the next generation of parents, this demographic is a key age group to educate on the benefits of breastfeeding. However, to date, adolescents have attracted limited attention as a target audience, even though positive attitudes and behaviors exhibited by adults can originate from learning and experiences gained in adolescence, Reference Tohi, Tu’akoi and Vickers21–Reference Macnab23 and there is evidence that health interventions based on the WHO “Health Promoting School” model can improve pupils’ health literacy in ways that have a continuing impact on their lives. Reference Macnab, Gagnon and Stewart34–Reference Macnab and Mukisa37 School-based interventions on obesity prove most effective when this age group is engaged directly, Reference Weihrauch-Blüher, Kromeyer-Hauschild and Graf38 and comprehensive community-based health education programs that focus on adolescents have been identified as an avenue for prevention of overweight, obesity, and associated comorbidities. Reference Msollo and Majaliwa39 As Tohi et al state, “Investment in today’s adolescents has the potential to act as an NCD “circuit breaker” and thus will yield significant dividends for future generations.” Reference Tohi, Tu’akoi and Vickers21
The benefits of breastfeeding are well established, and there is a growing literature on the protective effects on chronic NCDs in adulthood from being breastfed as an infant. Reference Victora, Bahl and Barros2,Reference Binns, Lee and Low3,Reference Kelishadi and Farajian12,Reference Horta, Loret de Mola and Victora13,Reference Cerf40–Reference Capra, Aliverti and Bellani43 But while breastfeeding practices in LMICs have continued to improve in the past decade, parental success in initiating and sustaining the practice still lags behind the recommendations promoted by the WHO, Reference Zong, Wu, Zhao, Magnussen and Xi6 and few countries in sub-Saharan Africa are expected to be able to reach the goals for EBF set by the WHO for 2030. 1,Reference Mohammed, Calvert and Webb8
Achieving optimal breastfeeding practices could save over 820,000 children’s lives annually among those under five years old, as well as contribute to improved IQ, better school attendance, and higher income in adult life. Reference North, Gao, Allen and Lee7 Currently, NCDs are occurring at younger ages and more aggressively in LMICs, and the resulting economic, societal, and personal costs are crippling; government promotion of breastfeeding practices could reduce stunting and obesity, and if a reduction in the incidence of NCDs resulted, government costs for NCD-related healthcare would likely fall. Reference Norris, Macnab, Daar and Pauw44,Reference Atun, Davies and Gale45 As Hanson et al have stated, “Preparing a mother, her partner and her future child for ‘the first 1000 would break the cycle of risk and demonstrate benefit in the shortest possible time.” Reference Hanson, Gluckman, Ma, Matzen and Biesma11
Empowering Africa’s mothers, fathers, and families to be agents for change in this way requires broad societal engagement, and integrating DOHaD-informed knowledge and health practices into school curricula and other youth-oriented arenas is only one approach. By using clear and uncomplicated messaging and innovative means of delivery, tomorrow’s parents can be given knowledge and skills able to help them set up healthier trajectories for their children. But, while such knowledge contributes to parents being able to do this and to modify their own NCD trajectories, Reference Norris, Daar and Balasubramanian46 individual education is only one component of a necessarily multipronged approach to NCD prevention. Society-level factors that influence expectations regarding breastfeeding and its acceptability also need to be addressed; these can be explained during school-based health promotion, including myths and misconceptions in the local community, the negative impact of ineffective support for mothers, and positive roles that fathers can contribute.”
Childcare and nutrition are still traditionally viewed socially and culturally as the responsibility of women. Reference Kimani-Murage, Wekesah, Wanjohi, Macnab, Daar and Pauw47 While mothers’ knowledge and positive attitudes certainly play key roles in EBF, Reference Dukuzumuremyi, Acheampong, Abesig and Luo48 success in initiating and sustaining the practice is a collective societal responsibility, Reference Rollins, Bhandari and Hajeebhoy17,Reference Pentecost, Macnab, Mayekiso and Ross18 and community engagement needs to focus on other “reproductive actors” including male adolescents. Reference Majombozi, Mutendi, Pentecost, Kearney, Moll and Penkler49 School-based programs should help future parents to understand that successful breastfeeding involves both mothers and fathers; in this context, inviting new parents from the community as “peer educators” and in-class role play are effective ways to engage adolescents as they prefer learning about health-related concerns from their peers rather than adults. Reference Macnab and Mukisa19,Reference Dodd, Widnall and Russell50 Fathers educated to understand the benefits of breastfeeding can play a significant role in a mother’s decision to initiate, continue, or stop breastfeeding. In a systematic review, Ogbo et al evaluated the impact of specific types of male partner support; new mothers receiving verbal encouragement breastfed longer and more exclusively; sensitivity to the needs of the nursing mother positively improved breastfeeding practices, as did awareness of how to help prevent and manage breastfeeding difficulties, and practical help with household chores. Reference Ogbo, Akombi and Ahmed20 Boys can be made aware that there are effective support measures that fathers can provide. Boys in our cohort gained awareness of how the example of mothers who breastfeed in a community can positively influence others, and African boys participating in school-based DOHaD education have called for an equal role in parenting responsibilities saying, “Don’t make it all sound for girls.” Reference Macnab and Mukisa19
Prior literature has identified that cultural norms that favor men and boys foster and perpetuate gender inequity that undermines the rights of women and girls, Reference Macnab, Besigye and Tusubira51–Reference Bosire, Pentecost, Mendenhall, Pentecost, Kearney, Moll and Penkler53 and shown evidence of the likelihood that boys and girls attach different degrees of relevance to particular health-related facts. Reference Tohi, Tu’akoi and Vickers21,Reference Davies, Macnab and Byass24 Because of this, gender-based variations in the interest and perceived relevance of concepts shared within the target audience likely impact how health education is received. In this context, a statistically significant difference found in our evaluation is likely relevant; far more boys than girls attached importance to the cost-benefit of breastfeeding, with 88% ranking a father not having to provide money to buy formula as most interesting. In contrast to boys, girls saw more relevance for fathers that breastfed babies are “easy to comfort, so cry less and feeds during the night are easier,” and that “changing diapers is less gross.” A gender-based difference was also evident in the importance of health care costs for managing diabetes in adults potentially being influenced by breastfeeding; boys consistently ranked this as most interesting pre- and post-intervention, and the impact of financial considerations on adolescents’ interest in DOHaD-related education has been identified previously. Reference Macnab and Mukisa19 As strong gender stereotypes exist that influence what roles and aspirations boys and girls view as appropriate, Reference Fabes, Hayford, Pahlke, Schoon and Eccles52 educators need to be mindful of gender-based factors influencing the interests of girls and boys in their target audience in order to engage and inform both groups effectively.
Health education is central to the transfer of scientific knowledge to inform and potentially influence positive behavior. This applies to the promotion of breastfeeding, where effective educational strategies are important to improve and correct knowledge, attitudes, beliefs, and sociocultural norms. In the context of DOHaD, the need has been highlighted for socially tailored approaches to promote breastfeeding, Reference Koray, Wanjiru and Kerkula4 and integrated and inclusive interventions that encompass broader social framings, adopt life-course approaches, and engage adolescents are called for. Reference Pentecost, Macnab, Mayekiso and Ross18 Because of the critical time window that adolescence represents school-based programs are now recognized to afford unique opportunities to engage and inform the next generation of parents. Reference Tohi, Tu’akoi and Vickers21 And empowering such knowledge in adolescents is seen as important for future health as it promotes independence, responsibility, and risk avoidance, which in turn encourages them to care for their own health and help safeguard the next generation.” Reference Tohi, Tu’akoi and Vickers33
Strengths and limitations
Strengths of this study include that it describes a novel yet simple approach that enables educators to identify where adolescents are likely to find interest and relevance in breastfeeding education, and also as it indicates that girls and boys can acquire knowledge pertinent to their future decision-making as parents regarding breastfeeding practices. The in-class questionnaires provided information able to guide follow-up education sessions, but if pupil input is garnered in real time by a show of hands in response to questions presented via PowerPoint or flipchart, this feedback can be used within the same session to guide discussion that can correct misconceptions and emphasize and explain key facts.
We recognize limitations in what we report. While there is a statistical significance of gender differences in interest regarding the cost-benefit of breastfeeding for the cohort as a whole, as the sample size for each individual country is small this finding cannot be assumed to apply equally to all countries. While the same presentation and evaluation tools were used in each of the schools, the session was delivered by different investigators, so some variations in style and emphasis are inevitable. The questionnaires were developed for this study and not based on validated tools. While significantly more participants gave correct responses post-presentation to the questions on concepts of parenthood and nurture, we cannot know if what was learned will be retained or if these changes will persist over time. The purpose of the study was to identify gender-based differences with the potential to impact breastfeeding education, and no information on other important demographic and social factors was obtained. We also recognize that adolescent education to promote awareness of the benefits of breastfeeding needs to be part of multifaceted society-wide interventions, that interacting components will influence outcomes, effects will vary with local conditions, and how important it is to avoid repeating gendered stereotypes. Ideally, DOHaD-related parenting will be part of a life skills curriculum in the future where equity in gender roles and responsibilities, and the importance of respectful relationships will be emphasized alongside health.
Conclusions
DOHaD-related health promotion delivered through school-based programs has the potential to reach large numbers of young Africans who will soon become parents. However, prior research indicates that adolescents in school programs have varying levels of interest in key elements of the health messages delivered. As this presumably impacts what they perceive as relevant and thereby influences which facts they are likely to retain, it behooves educators to design education focused around aspects of the topic that are seen as interesting and relevant by both genders in order to engage this target audience effectively.
Our study indicates that school-based education on nurturing parental care and the benefits of breastfeeding is feasible, can engage participating adolescents, and can lead to the acquisition of knowledge that alters their perception and attitudes at least in the short term. Also, data ranking the level of interest among girls and boys about key messages related to the importance of the first 1000 days of life can be obtained from appropriate inquiry during an in-class health promotion session. As differences were evident in what girls and boys indicated they saw as most and least interesting, we suggest that in future similar inquiry should be included where school-based health education is undertaken. Awareness of gender-based differences in pupils’ perceptions of relevance will enable educational content to be targeted to attract and inform both genders. In this way adolescents participating in school-based health education are more likely to hear the knowledge shared, understand how they can benefit from the skills described, and ultimately retain key elements with the potential to influence their attitudes and future behaviors.
Acknowledgments
We thank the Stellenbosch Institute for Advanced Study (STIAS) for convening the Summer School to build a network of young scientists in sub-Saharan Africa; this led to the formation of the STIAS African Scholars Network, whose aim is to increase research capacity in the Developmental Origins of Health and Disease on the continent. We are also grateful for the collaboration of the schools that participated in this study and to the teachers and pupils for their contributions.
Financial support
This work was supported by funding from the Hillman Medical Education Fund administered by Rose Charities Canada and the Stellenbosch Institute for Advanced Study, South Africa. Mukoma Gudani is supported by the University Capacity Development Grant (UCDP) at the University of Venda.
Competing interests
The authors have no conflict of interest to report.
Appendix Questionnaires
QUESTIONAIRE 1

QUESTIONAIRE 2
We want to know which of the following facts about feeding a baby you think are most interesting and would make you want to learn more about how boys and girls can help make breastfeeding happen. And which facts interest you the least
BENEFITS TO THE BABY
Choose which of the following three facts is MOST INTERESTING to you and write the number as your answer
-
1. A healthy baby can earn more in her/his lifetime than one who is sick
-
2. A healthy baby will have fewer bad diseases as an adult
-
3. Breast milk is the best source of nutrition for most babies, and protects
a baby against diarrhea and many infections.
ANSWER (write a 1, 2 or 3) -------
Choose which of the following facts is the LEAST INTERESTING to you and write the number as your answer
-
1. A healthy baby can earn more in her/his lifetime than one who is sick
-
2. A healthy baby will have fewer bad diseases as an adult
-
3. Breast milk is the best source of nutrition for most babies, and protects
a baby against diarrhea and many infections.
ANSWER (write a 1, 2 or 3) -------
BENEFITS TO THE MOTHER
Choose which of the following three facts is MOST INTERSTING and write the number as your answer
-
1. Breast milk is always available and at the right temperature. Mothers can breastfeed anytime and anywhere
-
2. Breastfeeding means you do not need to prepare bottles of formula
-
3. Working mothers who are breastfeeding miss fewer days of work,
because their babies don’t get sick so often
ANSWER (write a 1, 2 or 3) -------
Choose which of the following facts is the LEAST INTERESTING and write the number as your answer
-
1. Breast milk is always available and at the right temperature. Mothers can breastfeed anytime and anywhere
-
2. Breastfeeding means you do not need to prepare bottles of formula
-
3. Working mothers who are breastfeeding miss fewer days of work, because their babies don’t get sick so often
ANSWER (write a 1, 2 or 3) -------
BENEFITS TO THE FATHER
Choose which of the following three facts is MOST INTERSTING and write the number as your answer
-
1. You do not have to spend money to buy formula if a mother breastfeeds infants who are fed formula, and changing diapers is less gross
-
2. Breastfed babies don’t get constipated, they smell nicer than
-
3. Breastfed babies are easy to comfort so cry less and feeds during the night are easier
ANSWER (write a 1, 2 or 3) -------
Choose which of the following facts is the LEAST INTERESTING and write the number as your answer
-
1. You do not have to spend money to buy formula
-
2. Breastfed babies don’t get constipated, they smell nicer than infants who are fed formula fed, and changing diapers is less gross
-
3. Breastfed babies are easy to comfort so cry less and feeds during the night are easier
ANSWER (write a 1, 2 or 3) -------
BENEFITS TO YOUR COMMUNITY and SOCIETY
Choose which of the following three facts is MOST INTERSTING and write the number as your answer
-
1. If more babies were breastfed fewer adults would become diabetic, so it would reduce health care costs for managing diabetes in adults,
-
2. More breastfeeding would prevent many child deaths each year, particularly from infections
-
3. In communities where many mothers exclusively breastfeed other mothers are likely to follow their example and also breastfeed
ANSWER (write a 1, 2 or 3) -------
Choose which of the following facts is the LEAST INTERESTING and write the number as your answer
-
1. If more babies were breastfed fewer adults would become diabetic, so it would reduce health care costs for managing diabetes in adults.
-
2. If more babies were breastfed this would prevent many child deaths each year, particularly from infections
-
3. If more babies were breastfed other mothers in the community would be likely to follow this example and also breastfeed
ANSWER (write a 1, 2 or 3) -------

 Open access
Open access