


Introduction
Conceptual clarity is essential for high-quality palliative and supportive care practice and research, particularly in ethically complex areas such as end-of-life decision-making. Debates about euthanasia are often clouded by conceptual ambiguity. Nowhere is this more evident than in India, where the term “passive euthanasia” is widely used to describe the withdrawal or withholding of life-sustaining treatment. This is illustrated by the landmark case of Aruna Shanbaug (Brassington Reference Brassington2021; Agarwal Reference Agarwal2023). Aruna Shanbaug had been in a persistent vegetative state since a sexual assault on November 27, 1973. During the assault, the attacker had put a dog chain around her neck, due to which the supply of oxygen to her brain was interrupted. On March 7, 2011, the Indian Supreme Court reviewed a petition to terminate her life support. Beginning with the Supreme Court’s judgment in this case and further clarified in subsequent rulings, Indian law now permits forgoing of life-sustaining treatment under defined procedural safeguards, while the intentional administration of lethal drugs to a patient remains legally prohibited (Agarwal Reference Agarwal2023). Though, interesting from a definitional perspective is that the court that ruled on the Aruna case, along with a subsequent 2018 ruling, used the term “euthanasia” to describe the withdrawal of treatment, reflecting common usage in India (India SCo 2011; Brassington Reference Brassington2021; Agarwal Reference Agarwal2023). Similarly, studies on attitudes toward euthanasia in India often adopt a broader interpretation of the term, encompassing both the withdrawal of treatment and the administration of lethal drugs to a patient (Kamath et al. Reference Kamath, Bhate and Mathew2011; Poreddi et al. Reference Poreddi, N and Pashapu2022). Within this broad interpretation of euthanasia, distinctions are frequently made between active and passive euthanasia, as well as direct and indirect euthanasia (Garrard and Wilkinson Reference Garrard and Wilkinson2005; Clemens et al. Reference Clemens, Klein and Jaspers2008; Brassington Reference Brassington2020).
This usage diverges sharply from many international definitions, according to which euthanasia refers exclusively to the administration of lethal drugs with the explicit intention of ending life. For instance, Bert Broeckaert has critiqued the broad interpretation of euthanasia in numerous publications, proposing his own conceptual framework instead (Broeckaert Reference Broeckaert, Payne, Seymour and Ingleton2008, Reference Broeckaert2009). His framework for “treatment decisions in advanced disease” categorizes end-of-life decisions into 3 main areas: (1) “(forgoing) curative and/or life-sustaining treatment”, (2) “pain and symptom control”, and (3) “euthanasia and assisted suicide”. The latter refers specifically to interventions aimed at hastening death through the administration of lethal drugs.
Broeckaert defines euthanasia as “the intentional administration of lethal drugs to painlessly end the life of a patient suffering from an incurable condition deemed unbearable by the patient.” When the administration is performed at the patient’s request, Broeckaert terms the act voluntary euthanasia. Conversely, if the patient is unable to consent, Broeckaert classifies the act as nonvoluntary euthanasia. Assisted suicide, according to Broeckaert, occurs when someone is “intentionally assisting a patient, at this patient’s request, to terminate his or her life” (Broeckaert Reference Broeckaert, Payne, Seymour and Ingleton2008, Reference Broeckaert2009). Due to its conceptual clarity, Broeckaert’s typology is applied in this article, which will use “euthanasia” to refer collectively to both voluntary and nonvoluntary euthanasia.
As indicated above, research and public debate in India have not widely adopted such more restrictive and narrow definition of euthanasia, which has led to terminological confusion. This confusion may misguide policy debates and obscure the ethical distinctions that clinicians and families must navigate at the end of life. Although this confusion arises in the Indian context, its implications extend far beyond national borders. Comparative studies of attitudes toward euthanasia risk false equivalence if the same term is used to describe fundamentally different practices. For global ethical discourse, palliative care, and health policy, definitional clarity is not a semantic luxury but a prerequisite for meaningful dialogue. India thus provides a critical case study of how conceptual slippage may undermine both research validity and ethical deliberation.
This systematic review and meta-analysis aims to examine Indian physicians’ and nurses’ attitudes toward euthanasia as defined by Broeckaert. By pooling available data, this study attempts to estimate the proportion of healthcare professionals who support euthanasia. More importantly, this study aims to evaluate whether and how the use of the concept “passive euthanasia” inflates or distorts these estimates. Such finding would highlight both the urgent need for rigorous, conceptually precise research in India and the broader lesson for global scholarship.
Materials and methods
Search strategy
This systematic review and meta-analysis adhered to the updated 2020 PRISMA guidelines (Page et al. Reference Page, McKenzie and Bossuyt2021a; Page et al. Reference Page, Moher and Bossuyt2021b). On January 19, 2026, the investigators conducted searches across 4 academic databases: PubMed, EMBASE, PsycINFO, and CINAHL. For PubMed, PsycINFO, and CINAHL, a broad search string was applied: ((euthanasia) OR (assisted suicide) OR (assisted death) OR (assisted dying) OR (mercy killing)) AND (India). The investigators opted not to add search terms focusing on physicians and nurses, because they had originally planned to study attitudes across different healthcare professions. Adding a potentially incomplete list of healthcare professionals to the search string would have increased the risk of inadvertently excluding relevant reports.
In EMBASE, however, this search string yielded a disproportionately high number of seemingly irrelevant results. To refine the outcomes, the investigators employed single quotation marks for specific phrases, such as “assisted suicide,” “assisted death,” “assisted dying,” and “mercy killing,” ensuring the results contained exact matches. For all databases, the search was limited to studies published from 2010 onward. Following the study selection, the investigators reviewed reference lists from the selected studies to ensure no relevant data were overlooked.
Study selection
After duplicates were removed, the unique records were imported into Covidence (Covidence 2025). Two investigators (KK and JG) independently screened the titles and abstracts to assess alignment with the inclusion and exclusion criteria. Upon completion of this initial screening, the investigators convened to resolve any discrepancies in the selected records.
Next, the full-text versions of the remaining records were gathered and incorporated into the Covidence results. The investigators then reviewed these full texts to confirm whether they adhered to the inclusion and exclusion criteria. Discrepancies during this stage were again resolved by consensus through discussion.
All included reports had to meet the inclusion criteria. Included reports were required to provide quantitative insights into Indian healthcare professionals’ attitudes toward euthanasia or physician-assisted suicide, as defined by Broeckaert. The investigators excluded studies if they involved people with a healthcare background who were not currently practicing (e.g., students, retirees, volunteers), focused on medical practice instead of attitudes, only studied forgoing treatment, were qualitative studies or conference abstracts, or did not provide Indian data. Since the focus was on India and English is the dominant language of health science communication in the country, the investigators assumed that all retrieved studies would be in English. Consequently, setting English as an inclusion criterion or establishing a translation process for non-English reports was deemed unnecessary.
Data extraction, risk of bias assessment, and analysis
Once the study selection process was complete, the 2 investigators independently extracted data from the selected reports and evaluated the risk of bias in each study. Following this, they convened to resolve any discrepancies and reach a consensus.
While all selected studies were included in the systematic review, the meta-analysis was limited to studies that clearly reported how many healthcare professionals in the sample approved of euthanasia, as defined by Broeckaert. Consequently, studies that merged approval data for euthanasia with forgoing treatment under a broader interpretation of “euthanasia” were excluded from the meta-analysis. For studies that only reported percentages of approval, these percentages were converted into numerical values based on the stated sample size. If a study only provided figures for disagreement with euthanasia and did not include a neutral response category, the remaining participants in the sample were assumed to approve of euthanasia, enabling the calculation of approval rates. The investigators used the Mixed Methods Appraisal Tool (MMAT), version 2018, developed by Hong et al. (Reference Hong, Pluye and Fàbregues2018), to assess the risk of bias in the studies.
For the meta-analysis, the investigators utilized Jamovi 2.3.28 (Jamovi Reference Jamovi2025). Within Jamovi, the proportions option in the MAJOR module was employed to assess the pooled prevalence of pro-euthanasia attitudes. MAJOR serves as a Jamovi interface for the R package Metafor, which generates heterogeneity statistics and a Forest Plot. However, the publication bias assessment and Funnel Plot generated by Metafor were not included, as these tools are not recommended for proportional meta-analysis (Hunter et al. Reference Hunter, Saratzis and Sutton2014; Barker et al. Reference Barker, Migliavaca and Stein2021).
The investigators developed a review protocol prior to conducting the study, though it was not registered. This protocol, along with data extraction forms and risk of bias assessment templates, is available from the corresponding author upon request. All extracted data from the included studies are presented within this article. As this systematic review and meta-analysis relied solely on aggregate data and published statistics, it does not qualify as human-subjects research and did not require approval from an Institutional Review Board or Ethics Committee.
Results
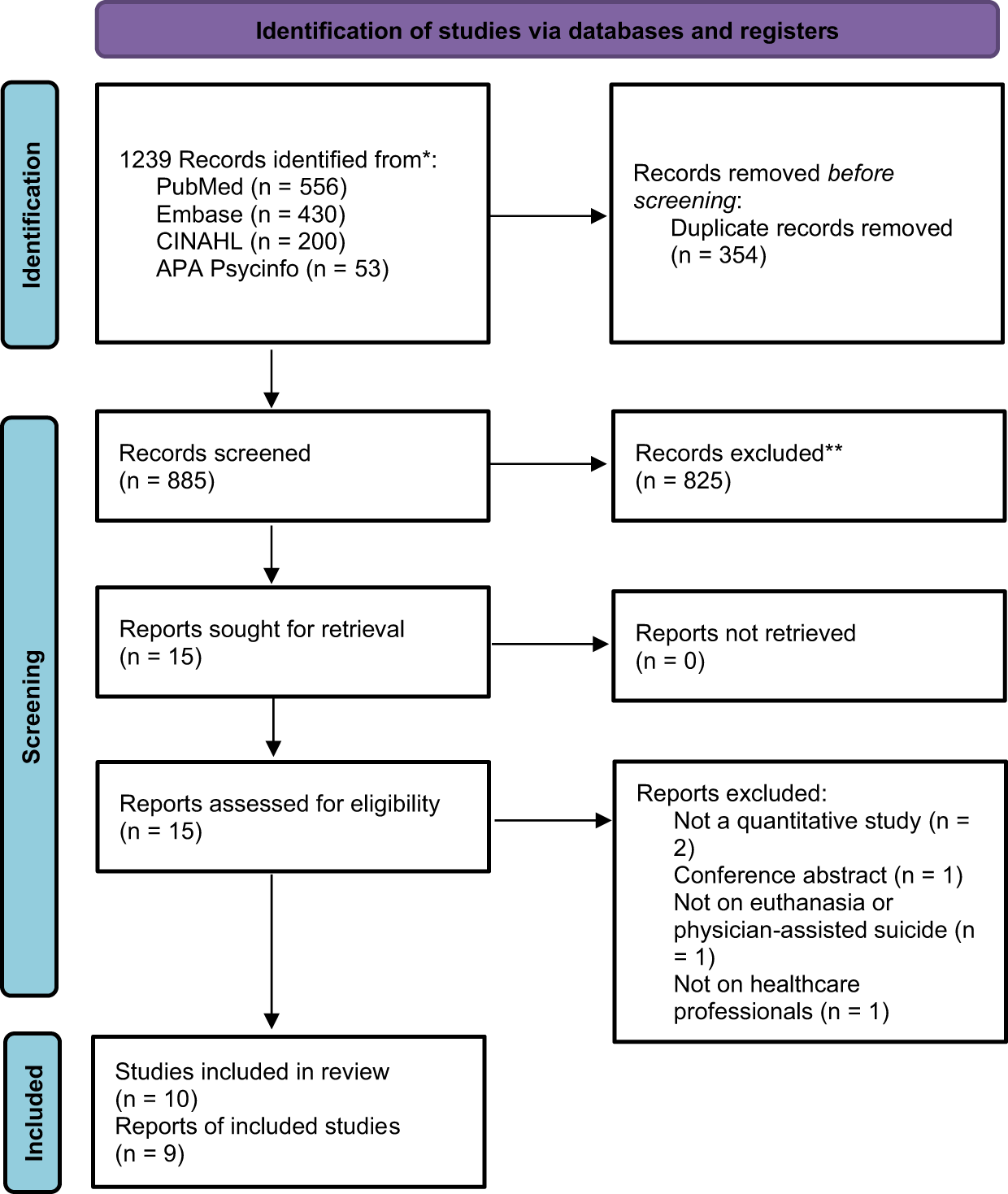
Figure 1 summarizes the results of the search and selection process. Out of the 885 unique records that were identified from the 4 searched databases, 10 reports presenting findings of 9 studies were included in the data extraction and risk of bias assessment. A review of the reference lists of the included studies did not lead to any additional relevant studies.
PRISMA flowchart (Page et al. Reference Page, McKenzie and Bossuyt2021a).

Description of the included studies
The characteristics of the included studies are detailed in Table 1. Six studies focused on the attitudes of nurses toward euthanasia (Poreddi et al. Reference Poreddi, Nagarajaiah and Bada Math2013; Goel et al. Reference Goel, Chhabra and Weijma2014; Maria Therese et al. Reference Maria Therese, Rukumani and Mano2014; Singh et al. Reference Singh, Gupta and Singh2016; Kalal et al. Reference Kalal, Kumar and Choudhary V2020; Nair Reference Nair2025). Six explored the perspectives of physicians (Kamath et al. Reference Kamath, Bhate and Mathew2011; Maria Therese et al. Reference Maria Therese, Rukumani and Mano2014; Singh et al. Reference Singh, Gupta and Singh2016; Subba et al. Reference Subba, Khullar and Latafat2016; Shekhawat et al. Reference Shekhawat, Kanchan and Saraf2023; Nair Reference Nair2025). One included other healthcare professionals (“pharmacists, physiotherapists, and nursing assistants”) (Nair Reference Nair2025), and 1 examined the views of individuals in the healthcare “teaching profession” (Maria Therese et al. Reference Maria Therese, Rukumani and Mano2014). These studies represent findings from 5 Indian states: Delhi (Goel et al. Reference Goel, Chhabra and Weijma2014; Singh et al. Reference Singh, Gupta and Singh2016), Karnataka (Poreddi et al. Reference Poreddi, Nagarajaiah and Bada Math2013; Subba et al. Reference Subba, Khullar and Latafat2016), Rajasthan (Kalal et al. Reference Kalal, Kumar and Choudhary V2020; Shekhawat et al. Reference Shekhawat, Kanchan and Saraf2023), Kerala (Nair Reference Nair2025), and Tamil Nadu (Maria Therese et al. Reference Maria Therese, Rukumani and Mano2014).
Characteristics and risk of bias of the included studies

a The description of the sample only includes healthcare professionals from India. If the survey included respondents from other countries or non-healthcare professionals (e.g. students), they were not included.
b 1. “Is the sampling strategy relevant to address the research question?”, 2. “Is the sample representative of the target population?”, 3. “Are the measurements appropriate?”, 4. “Is the risk of nonresponse bias low?”, 5. “Is the statistical analysis appropriate to answer the research question?” Answers: +: “Yes,” −: “No,” ?: “Can’t tell.”
The risk of bias assessment, summarized in Table 1, indicated that all included studies either presented a substantial risk of bias or lacked sufficient information in their manuscripts to accurately assess the risk of bias.
Euthanasia definition and attitudes
Table 2 outlines the various broad definitions of euthanasia employed across the included studies. In some cases, euthanasia was not explicitly defined, requiring the authors’ interpretation to be inferred from the manuscript. Consistent with these broad definitions, the studies examined attitudes toward a range of end-of-life treatment decisions, including the withdrawal of treatment, pain and symptom management, as well as euthanasia as defined by Broeckaert.
Definition, operationalization, and approval of euthanasia in the included studies

N/A: Broeckaert’s categories could not be applied because the survey did not make clear distinctions between the various treatment decisions; or the authors did not report data on individual items on euthanasia attitudes; or there was no question on legalization in the survey.
a Only attitude items have been listed. Items that enquired after knowledge about current legal status were not included.
b Survey sample with discernible data on euthanasia approval.
To gather these data, 5 studies developed their own survey items on euthanasia (Kamath et al. Reference Kamath, Bhate and Mathew2011; Goel et al. Reference Goel, Chhabra and Weijma2014; Subba et al. Reference Subba, Khullar and Latafat2016; Shekhawat et al. Reference Shekhawat, Kanchan and Saraf2023; Nair Reference Nair2025) while another 4 utilized tools previously designed by other researchers to assess these attitudes (Poreddi et al. Reference Poreddi, Nagarajaiah and Bada Math2013; Maria Therese et al. Reference Maria Therese, Rukumani and Mano2014; Singh et al. Reference Singh, Gupta and Singh2016; Kalal et al. Reference Kalal, Kumar and Choudhary V2020). Despite the ambiguity introduced by the broad interpretation of euthanasia, 5 studies clearly included survey items that corresponded with Broeckaert’s definition of euthanasia. Additionally, 5 surveys explored attitudes regarding the legalization of euthanasia; however, the specific treatment decisions assessed by these items remained unclear. Consequently, survey items on legalization were excluded from further analysis. Notably, none of the studies investigated attitudes toward assisted suicide.
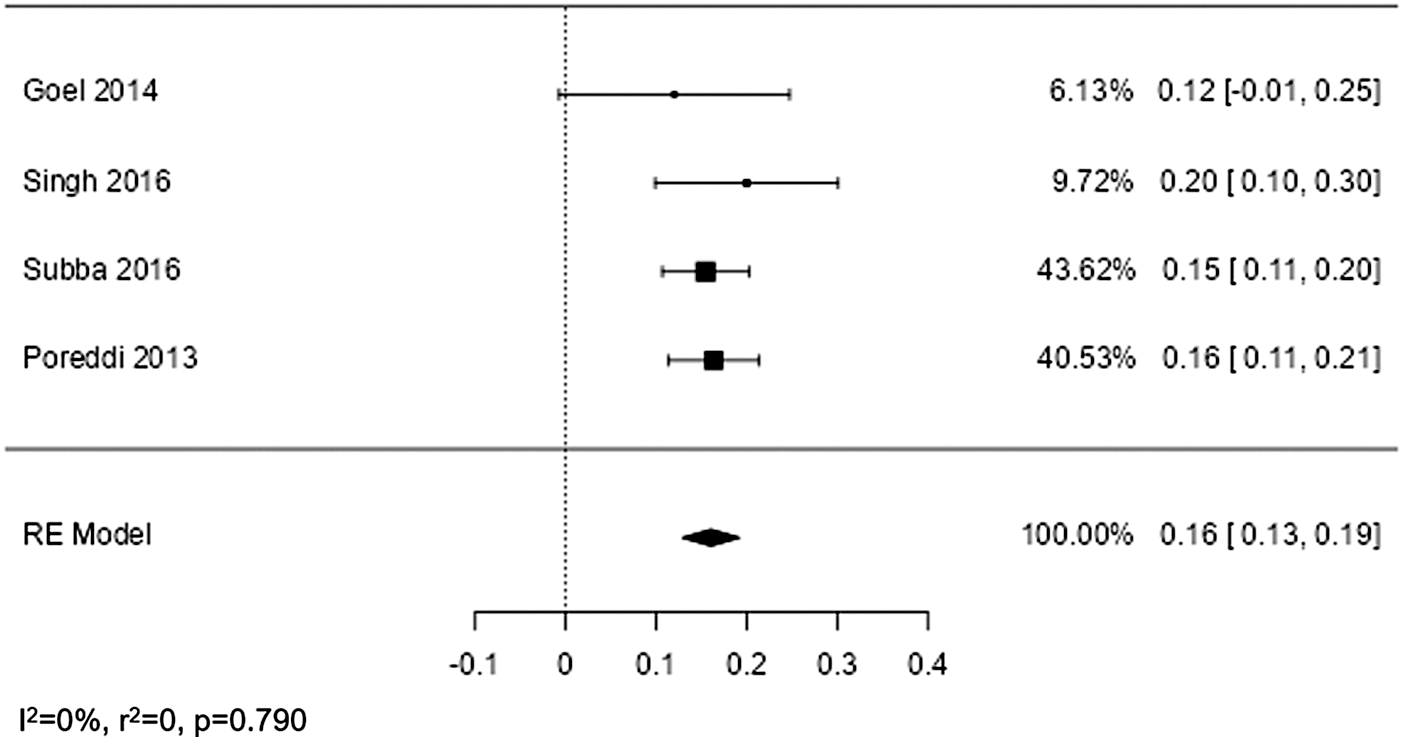
Among the 5 studies with a survey item on euthanasia attitudes consistent with Broeckaert’s definition, 1 study (Maria Therese et al. Reference Maria Therese, Rukumani and Mano2014) did not report specific results for the relevant survey item. Instead, it provided a composite score that combined attitudes toward various treatment decisions. Consequently, data from 4 studies were included in the meta-analysis (Poreddi et al. Reference Poreddi, Nagarajaiah and Bada Math2013; Goel et al. Reference Goel, Chhabra and Weijma2014; Singh et al. Reference Singh, Gupta and Singh2016; Subba et al. Reference Subba, Khullar and Latafat2016). As summarized in Table 2 and Figure 2, the meta-analysis comprised 239 nurses and 280 physicians, totaling 519 healthcare professionals. The forest plot in Figure 2 indicates that approval of euthanasia as defined by Broeckaert ranged between 12% and 20%, with a pooled approval rate of 16% in the random-effects model. Notably, the evaluation of heterogeneity demonstrated a high degree of homogeneity.
Forest plot.

Discussion
The meta-analysis uncovered 2 notable findings: first, the approval of euthanasia among healthcare professionals was only 16%, and second, this approval rate was consistent across the 4 included studies, ranging from 12% to 20%. These findings appear to contradict the descriptions and analyses provided in the reviewed studies themselves. The results and discussions in those reports suggested both higher and more widely varied rates of approval for what the authors termed “euthanasia.” For example, Kalal et al. (Reference Kalal, Kumar and Choudhary V2020) reported that 47.77% of Indian nurses supported “euthanasia,” while Subba et al. (Reference Subba, Khullar and Latafat2016) found that 46.8% of doctors approved of “euthanasia.” In contrast, the pooled prevalence of euthanasia approval in this meta-analysis was much lower, at 16%. However, the meaning of “euthanasia” in the cited studies was inconsistently defined or not defined at all making it unclear whether participants were endorsing the active administration of lethal drugs following Broeckaert’s definition of euthanasia, or something else, such as forgoing treatment. The approval of euthanasia was often assessed through survey items without a consistent definition of euthanasia and, therefore, required participants to interpret the concepts on their own. This likely led participants to interpret the survey items in various ways. These inconsistencies highlight the difficulty of interpreting prevalence data when terminology is vague or contradictory, and they reinforce the need for conceptual clarity in future research. What may appear to be a discrepancy in approval rates is more accurately a reflection of the underlying incoherence in how euthanasia is defined and measured across studies. In many cases, the lack of precise definitions means that comparisons between studies are not just difficult but potentially meaningless.
The meta-analysis adhered to Broeckaert’s narrow definition, which limits euthanasia to the intentional administration of lethal drugs to patients with “incurable” and “unbearable” conditions. As a result, for the meta-analysis, the investigators looked at individual items in the surveys and only included those items that clearly enquired about the participants’ attitudes to euthanasia as Broeckaert defined it. This meant that the majority of survey items in the selected studies were excluded from the meta-analysis because the included studies frequently adopted broader definitions of euthanasia, encompassing attitudes toward various forms of treatment withdrawal and withholding.
For instance, Kalal et al. (Reference Kalal, Kumar and Choudhary V2020) employed a modified version of Tordella and Neutens’ Euthanasia Attitudes Scale, which used the term “euthanasia” throughout without defining it (Tordella and Neutens Reference Tordella and Neutens1979). Although, in the introduction to their article, Kalal et al. defined euthanasia as “the termination of a very sick person’s life in order to relieve them of their suffering,” they did not include this definition in their revised version of the Euthanasia Attitudes Scale that they administered to the survey participants, so that the ambiguity of the original scale remained unresolved. Moreover, the euthanasia definition they used remains broad and fails to distinguish between forgoing treatment and the active administration of lethal drugs, a distinction that is central to Broeckaert’s typology and to the aims of this review. This ambiguity leaves it unclear whether Kalal et al.’s participants approved of euthanasia as per Broeckaert’s narrow definition, forgoing of treatment, or even another treatment decision. Similarly, Subba et al. (Reference Subba, Khullar and Latafat2016) described euthanasia as either active or passive, in the article, but did not offer a definition of the term itself. The absence of a precise definition leaves it unclear whether participants were endorsing the administration of lethal drugs, the withdrawal of treatment, or both. This ambiguity limits the interpretability of the study’s findings.
The importance of clear conceptual distinction is also underscored by the findings of Shekhawat et al. (Reference Shekhawat, Kanchan and Saraf2023). They reported that 40.5% of Indian healthcare professionals, including dentists, approved of “passive euthanasia” (i.e., various kinds of forgoing treatment), while only 8.5% supported “active euthanasia,” which aligns more closely with Broeckaert’s definition. A further 33.5% approved of both active and passive forms. Thus, 42% of participants in this study found “active euthanasia” morally acceptable, a figure significantly higher than the meta-analysis’ 16% approval rate. This discrepancy highlights the potential for confusion among respondents when terms like “active” and “passive euthanasia” are used without clear definitions as in the study of Shekhawat et al. When only items consistent with Broeckaert’s definition are analyzed, approval rates are substantially lower and remarkably consistent across studies.
This demonstrates that definitional ambiguity materially alters the empirical picture. For researchers, this means that comparisons across studies or across countries more broadly may be unreliable unless the underlying definitions are clearly articulated in the survey tools and in the publications that report on the collected data. For palliative care scholarship, this observation underscores the importance of conceptual precision when studying attitudes toward ethically sensitive practices.
Even when euthanasia is clearly defined, significant variations in approval rates can exist across studies. A review comparing European physicians’ attitudes revealed approval rates ranging from 3% to 78% (Gielen et al. Reference Gielen, S and Broeckaert2008). These differences are partly influenced by the countries in which the studies were conducted, with higher approval rates in places like Belgium and the Netherlands, where euthanasia is legal (Emanuel et al. Reference Emanuel, Onwuteaka-Philipsen and Urwin2016). In India, where euthanasia remains illegal, it is unsurprising that only a small minority of healthcare professionals support it, as reflected in this meta-analysis. This general disapproval of euthanasia may reflect not only the legal restrictions but also broader cultural norms and institutional policies that discourage open endorsement to avoid any misuse of lethal drugs in India. In contexts where a medical act is both legally prohibited and socially sensitive, professionals may internalize these boundaries or at least be reluctant to express approval even in research settings.
In addition to these findings, this systematic review also highlights gaps in existing research. Notably, no data were found on attitudes toward assisted suicide, which may seem surprising given that more countries, regions, and states worldwide have legalized assisted suicide than euthanasia (Mroz et al. Reference Mroz, Dierickx and Deliens2021). This lack of attention to assisted suicide in Indian studies likely stems from the dominance of the term “euthanasia” in legal and public discourse most notably in the Aruna Shanbaug case. Although the case focused on the withdrawal of life-sustaining treatment, the Supreme Court judgment used the term “euthanasia” broadly and also took the opportunity to explicitly reject the legalization of assisted suicide, despite it not being under review. This judicial framing has helped shape how euthanasia and not assisted suicide is discussed in both medical and legal conversations in India (India SCo 2011; Brassington Reference Brassington2021).
Another limitation is the restricted scope of the available data. While this review aimed to assess the attitudes of healthcare professionals broadly, substantial data were only found for nurses and physicians. Although some studies address the attitudes of medical and nursing students (Mazumder and Mazumder Reference Mazumder and Mazumder2019; Shruthi and Sudaakar Reference Shruthi and Sudaakar2021; Poreddi et al. Reference Poreddi, N and Pashapu2022), who are not yet healthcare professionals, research on other professional groups in Indian healthcare remains a critical gap.
This systematic review and meta-analysis faces 3 key limitations, primarily due to the limited data available and methodological constraints of the included studies. First, while risk of bias was identified for some studies, insufficient information prevented bias assessment for others. Despite this, the meta-analysis showed homogeneity across the included data, suggesting that the pooled prevalence of euthanasia approval may be representative beyond the sampled populations.
Second, the geographic coverage of the included studies was extremely limited. Observations came from only 5 Indian states out of a total of 28 states and 8 union territories. Furthermore, the meta-analysis included data from just 2 states: Delhi (Goel et al. Reference Goel, Chhabra and Weijma2014; Singh et al. Reference Singh, Gupta and Singh2016) and Karnataka (Poreddi et al. Reference Poreddi, Nagarajaiah and Bada Math2013; Subba et al. Reference Subba, Khullar and Latafat2016).
Third, the meta-analysis did not include recent data. The analyzed studies were published in 2013 (Poreddi et al. Reference Poreddi, Nagarajaiah and Bada Math2013), 2014 (Goel et al. Reference Goel, Chhabra and Weijma2014), and 2016 (Singh et al. Reference Singh, Gupta and Singh2016; Subba et al. Reference Subba, Khullar and Latafat2016), with potentially older underlying data. Only 1 of these studies (Subba et al. Reference Subba, Khullar and Latafat2016) mentioned the year in which data were collected, leaving the timeliness of the findings uncertain.
Conclusion
This systematic review and meta-analysis shows that Indian quantitative studies on attitudes toward euthanasia employ inconsistent and often overly broad definitions of the term. When euthanasia is defined narrowly as the intentional administration of lethal drugs, approval among healthcare professionals is low, ranging from 12% to 20%, with a pooled estimate of 16%. These findings contrast with higher approval rates reported in the studies, which use broader definitions. This finding highlights how conceptual ambiguity can distort empirical results.
The findings have methodological significance for palliative care scholarship. Clear and consistent definitions are essential for interpreting research on end-of-life attitudes and for ensuring that empirical data meaningfully inform ethical analysis and policy discussions. Strengthening definitional clarity in future studies will improve the quality and comparability of research in this area in India but elsewhere in the world as well.
Acknowledgments
During the preparation of this work, the authors used Microsoft Copilot to check the writing and readability of the manuscript. After using this tool, the authors reviewed and edited the content as needed and take full responsibility for the content of the publication.
Funding
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Competing interests
The authors declare none.



 Open access
Open access