


Introduction and purpose
Mental illnesses are health conditions that involve changes in emotion, thinking, or behaviour that are associated with distress or problems functioning in social, work, or family activities (APA, 2018). While the World Health Organization (WHO) has prioritized mental health promotion as a key to global development, mental illnesses continue to impact overall well-being worldwide and are significantly related to years of life lost due to illness (WHO, 2019). Unfortunately, in addition to the illnesses themselves, much of this negative impact is due to mental illness stigma (Livingston, Reference Livingston2013; Stuart, Reference Stuart2017). Therefore, it is important to find practical ways to reduce mental illness stigma through policy, programs, and best practices.
This study investigates the lived experiences of individuals with a diagnosis of mental illness in terms of stigma from family members and how they deal with potential familial mental illness stigma. The researchers also look at the forms of familial stigma within the family system and how these impact individuals. Familial mental illness stigma herein denotes ‘stigma experienced by individuals from within the family or close relatives due to their mental instability or ailment: that is, families as perpetrators of stigma against their relatives with mental illnesses and not as those being stigmatized’ (Adu et al., Reference Adu, Oudshoorn, Anderson, Marshall, Stuart and Stanley2021, p. 3).
Overview of mental illness stigma
Stigma has been described as a mark of shame or disapproval that results in an individual being rejected, discriminated against, and/or prohibited from participating in several different aspects of society (Goffman, Reference Goffman1963; WHO, 2001). Link and Phelan (Reference Link and Phelan2006) have conceptualized stigma as the co-occurrence of five interrelated components (i.e., labelling, stereotyping, separation, status loss, and discrimination) in the context of social power. Stigma can involve labelling ─ a process whereby individuals are defined by a trait deemed socially undesirable, such as certain health conditions (e.g., HIV/AIDS, some cancers, mental illness, leprosy, and tuberculosisLabelling produces a social distance with a deliberate or implicit effort to prevent people from social interactions within their environment (Lucas and Phelan, Reference Lucas and Phelan2012; Adu et al., Reference Adu, Oudshoorn, Anderson, Marshall and Stuart2022; Reference Adu, Oudshoorn, Anderson, Marshall, Stuart and Owusu2025a, Reference Adu, Wong, Boakye, Owusu, Etowa and Gyamfi2025b). Mental illness stigma is a priority concept in the extant mental health literature due to its harmful impact on individuals and society at large (Lucas and Phelan, Reference Lucas and Phelan2012; Mittal et al., Reference Mittal, Sullivan, Chekuri, Allee and Corrigan2012; Corrigan et al., Reference Corrigan, Mittal, Reaves, Haynes, Han, Morris and Sullivan2014; Follmer and Jones, Reference Follmer and Jones2018).
The stigma of mental illness has been characterized as a complex problem, owing to its hindrance to the global fight for mental wellness including in relation to economic development (Abbey et al., Reference Abbey, Charbonneau, Tranulis, Moss, Baici, Dabby, Gautam and Pare2011; Knaak et al., Reference Knaak, Mantler and Szeto2017; WHO, 2019). Mental illness stigma often functions as a medium through which society exploits, rejects, isolates, and prevents persons with mental illnesses from enjoying their social and economic rights (Abbey et al., Reference Abbey, Charbonneau, Tranulis, Moss, Baici, Dabby, Gautam and Pare2011; Stuart, Reference Stuart2017; WHO, 2019). This, in effect, tends to separate persons with a diagnosis of mental illness from those without such diagnoses and further excludes them from participating fully in activities within their communities (Knaak et al., Reference Knaak, Mantler and Szeto2017; WHO, 2019). It is also reported that the attitudes of the public towards persons with mental illnesses may prevent help-seeking from health and social supports, which can contribute to social and health problems such as unemployment, substance use, and homelessness (Corrigan et al., Reference Corrigan, Mittal, Reaves, Haynes, Han, Morris and Sullivan2014; Government of Canada, 2020; WHO, 2019). Ongoing discrimination towards individuals with mental illnesses could result in status loss with negative impacts on self-esteem and self-efficacy, creating barriers to a positive recovery journey.
Despite the known negative impacts of stigma on persons with mental illnesses globally, mental illness stigma continues to occur at every level of society, including institutions of public services (social, health, legal, prison, education, and other community services) and within families (Livingston, Reference Livingston2013; Stuart, Reference Stuart2017; Adu et al., Reference Adu, Oudshoorn, Anderson, Marshall and Stuart2022; Nyblade et al., Reference Nyblade, Stockton, Giger, Bond, Ekstrand, Mc Lean, Mitchell, La Ron, Sapag, Siraprapasiri and Turan2019). People with a suspected or diagnosed mental illness may conceal their condition to avoid social harassment that perpetuates psychological distress (Public Health Agency of Canada, 2006; van der Sanden et al., Reference van der Sanden, Pryor, Stutterheim, Kok and Bos2016). Therefore, changes need to be made to prevent stigma and associated social exclusion experienced by persons living with mental illnesses to stop the cycle of impeded social interactions and aggravated health conditions. These changes are essential, particularly within the family system, where mental illness stigma may operate more subtly. Literature to date has identified family mental illness stigma as a reality in many families (Östman and Kjellin, Reference Östman and Kjellin2002; Aldersey and Whitley, Reference Aldersey and Whitley2015; Paul and Nadkarni, Reference Paul and Nadkarni2017; O’Reilly et al., Reference O’Reilly, Paul, McCahon, Shankar, Rosen and Ramzy2019; Adu et al., Reference Adu, Oudshoorn, Anderson, Marshall, Stuart and Stanley2021); however, these studies are comparatively scarce compared to other forms of stigma such as stigma by association, public or social stigma, and self-stigma. In a recent meta-synthesis of the empirical literature on familial mental illness stigma in high-income countries in the last two decades (2000–2020), the research team found 28 articles, with only 4 situated in Canada (Adu et al., Reference Adu, Oudshoorn, Anderson, Marshall and Stuart2022).
In Canada, mental illnesses have been found to contribute significantly to disability, affecting 1 in every 5 people (Centre for Addiction and Mental Health, 2019; Public Health Agency of Canada, 2019). In addition, it is documented that about 11 million (38%) Canadians aged 15 years and above have at least one immediate or extended family member who lives with a mental health concern, diagnosed or otherwise (MHCC, 2015; Pearson et al., Reference Pearson, Janz and Ali2013; Pearson, Reference Pearson2015). Further, of Canadian families with a loved one living with a mental health concern, nearly 71% of them felt that their livelihoods were impeded by their relatives’ illness (MHCC, 2015; Pearson et al., Reference Pearson, Janz and Ali2013; Pearson, Reference Pearson2015). This current study, therefore, sheds light on the lived experiences of familial mental illness stigma and how it is confronted among persons with a diagnosis of mental illnesses in Ontario, Canada, and thus, adds to the extant literature on mental illness stigma, particularly stigma enacted by family members towards their loved ones. The overall objective of this work is to create knowledge to be used in better addressing and reducing familial mental illness stigma.
Methods
Design
An interpretive phenomenology design was adopted to understand the lived experiences of familial stigma among persons with mental illnesses, how it impacts familial relationships, and how individuals living with mental illness cope with this stigma. Martin Heidegger held the view that phenomenological investigation is interpretative, which allows researchers to analyse the experiences of others and connect them to their own interpretations and other forms of knowledge (Heidegger, Reference Heidegger1962 [Reference Heidegger1927]). Interpretive phenomenology is deeply connected with hermeneutics, or how the researchers interpret communications, texts, or even pre-understandings. Hermeneutics has been explained as a process and method capable of revealing concealed human experiences and relations as well as delving deeper into a given phenomenon than a mere description of core concepts and essences to look for actual meanings rooted in normal life practices (Spielgelberg, Reference Spielgelberg1976; Lopez and Willis, Reference Lopez and Willis2004). This is appropriate in the study context where there might be hesitation to discuss mental illness stigma occurring within one’s own family. Ultimately, there is an overlap between what is termed interpretive phenomenology and hermeneutic phenomenology, and herein, the term interpretive phenomenology is used. The focal point of interpretive research is on what human beings experience rather than what they consciously identify with, which are often connected to sociocultural and political settings (Lopez and Willis, Reference Lopez and Willis2004). In this study, the phenomenon of familial mental illness stigma is explored with an analysis of the social practices that construct, perpetuate, or prevent this phenomenon.
Interpretive phenomenology as a research methodology is suitable for describing and interpreting the lived experiences of familial mental illness stigma among persons with mental health problems. This study adopts van Manen’s (Reference van Manen1997) six practical interactive approaches for interpretive phenomenological inquiry to understand the phenomenon of familial mental illness stigma. The approaches consist of: ‘(1) orientating oneself to the phenomenon of interest and explicating assumptions and pre-understandings; (2) investigating experiences as lived through conversational interviews rather than as researchers conceptualize them; (3) reflecting upon and conducting thematic analysis which characterizes the phenomenon and interpretations through conversations; (4) describing the phenomenon through the art of writing and re-writing (rethinking, reflecting, and recognizing), which aims at creating in-depth writing; (5) maintaining a strong and oriented relation to the fundamental question about the phenomenon, and (6) balancing the research context by considering parts and wholes’ (van Manen, Reference van Manen1997, p. 30). In keeping with van Manen’s (Reference van Manen1997) practical interactive approaches, the researchers offered a description of the lived experiences of people with familial mental illness stigma in the context of their everyday life and contributions to the social construction of stigma.
Ethical approval for this study was obtained from the Western University’s Human Research Ethics Committee (#119602).
Study setting
The study was conducted in the province of Ontario, Canada. Participants resided in an urban area where acute and tertiary mental health services are organized by large hospital networks. Community mental health services are provided via primary care providers as well as specialized community mental health organizations, the largest of which is the Canadian Mental Health Association.
Recruitment
The researchers employed a criterion sampling technique to recruit participants for this interpretive phenomenology study. This allowed the research team to engage a subset of the adult population living with mental illness who were interested in discussing familial stigma. The distinct experiences presented across different ages of participants offered an interesting variety, with participants representing differing lengths of time since initial diagnosis and variable times for families to adapt (or not) to conditions. This allowed the researchers to understand the different dynamics of the familial stigma that may exist for individuals with a first onset versus long-term and recurrent illness. The target age for recruitment was 24 years or older, recognizing that the experiences of adults differ from those of youth and older adults. The age limit for this study was necessitated by the fact that familial mental illness stigma appears to be a sensitive issue, as the researchers sought to explore family members as stigmatizers of their loved ones with mental health problems. Hence, the investigators decided to speak to persons who are independent of their families and willing to share their lived experiences with the research team without fear or intimidation from family members. Recruitment was conducted with the assistance of key connections in the community such as family physician practice clinics, CMHA offices, and community health centers who work directly with the target population. The local organizations that support the target population posted the recruitment materials in their facilities.
The participants included 15 people living with mental illnesses in the province of Ontario, Canada. The sample size was informed by the use of interpretive phenomenology design. According to Creswell (Reference Creswell1998) and Morse (Reference Morse, Denizin and Lincoln1994), the ideal sample size for phenomenological studies should be between 5 and 25. Again, in interpretive phenomenology investigations, researchers intend to recruit a limited number of participants vis-à-vis a larger size to focus deeply on lived experiences to increase the likelihood of thick, rich, and unique stories relative to the phenomenon under study (Laverty, Reference Laverty2003). Inclusion criteria for participants for the in-depth interviews included: (1) being 24 years or older; (2) self-identifying as an individual living with mental illnesses; (3) speaks and understands English; (4) being a current resident of Ontario; and (5) being willing to participate in the study for 45–60 minutes. The exclusion criteria for participant recruitment included: (1) persons with mental illnesses who were not residents of Ontario; (2) persons with mental illnesses who were less than 24 years of age; (3) unable to communicate in and understand English; and (4) unwilling to participate in the study for 45–60 minutes.
Data collection
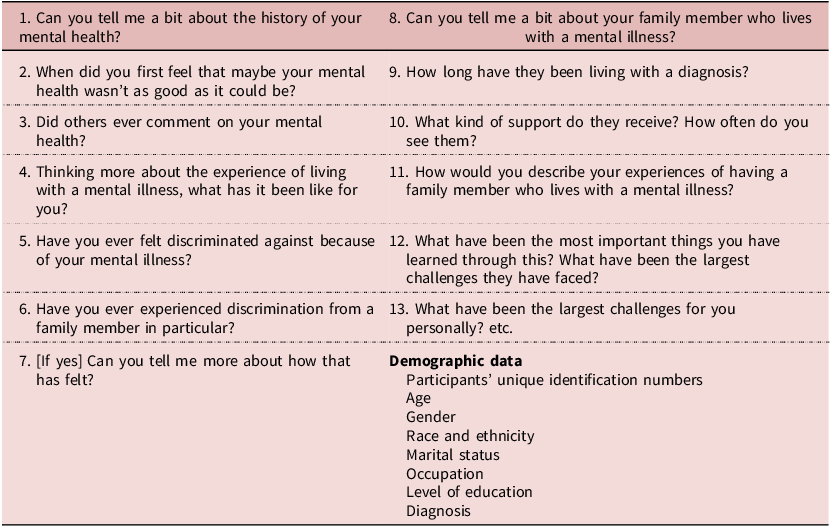
In-depth interviews were conducted with all participants between May and July 2022. In-depth interviews allow for both specificity and content flexibility (DeJonckheere and Vaughn, Reference DeJonckheere and Vaughn2019). This allowed the investigators to explore participant experiences to a degree of depth not afforded via other methods. The researcher’s appreciation of participants’ lived experiences of familial mental illness stigma was essential to create a space where participants could share in-depth about their experiences; the lead researcher, who conducted the interviews, used years of nursing and social service clinical experience to engage respectfully with participants. The researcher helped create a positive environment by opening with general questions to get to know participants, using active listening, and regularly thanking participants for their discussion. See Table 1 for the interview guide. With the permission of participants, all interviews were audio recorded and transcribed at the end of every session.
Interview Guide

Table 1 Long description
A table with two columns and thirteen rows of questions, plus a section for demographic data. The first column lists questions about personal mental health history, experiences, and discrimination. The second column lists questions about a family member with a mental illness, their support, and personal challenges. The demographic data section includes fields for unique identification numbers, age, gender, race and ethnicity, marital status, occupation, level of education, and diagnosis. Row 1: Can you tell me a bit about the history of your mental health? Row 2: When did you first feel that maybe your mental health wasn’t as good as it could be? Row 3: Did others ever comment on your mental health? Row 4: Thinking more about the experience of living with a mental illness, what has it been like for you? Row 5: Have you ever felt discriminated against because of your mental illness? Row 6: Have you ever experienced discrimination from a family member in particular? Row 7: If yes, Can you tell me more about how that has felt? Row 8: Can you tell me a bit about your family member who lives with a mental illness? Row 9: How long have they been living with a diagnosis? Row 10: What kind of support do they receive? How often do you see them? Row 11: How would you describe your experiences of having a family member who lives with a mental illness? Row 12: What have been the most important things you have learned through this? What have been the largest challenges they have faced? Row 13: What have been the largest challenges for you personally? etc.
All interviews were recorded on Zoom and transcribed. The confidentiality of participants was ensured, and all participants signed the informed consent form at the start of the meeting. Brief demographic information was collected from each participant, which was later anonymized using pseudonyms to conceal their identities. While conducting the in-depth interviews, observation notes were taken regarding nonverbal communication cues that were used to supplement the audio recordings of the verbal interactions.
Data analysis
Data analysis for this study was guided by Braun and Clarke’s (Reference Braun and Clarke2006) framework to produce textual accounts that reflect participants’ experiences of familial mental illness stigma. Braun and Clarke’s (Reference Braun and Clarke2006) framework provides the following stepwise process: (1) familiarizing oneself with the data; (2) generating initial codes; (3) searching for themes; (4) reviewing the themes; (5) defining and naming themes; and (6) producing the report. The purpose of this interpretive phenomenology analysis was to extract key aspects of the participants’ experiences that answer the research questions. The interpretative process unfolded by repeatedly engaging with the transcripts and observation notes to understand participants’ lived experiences, followed by detailed textual analysis. Detailed textual analysis implies in-depth exploration of the language in the text to form concepts and patterns that capture participants’ thoughts and lived experiences. The line-by-line analysis of transcripts of each participant allowed the researchers to capture the actual meaning embedded in the text or message. This was followed by a more in-depth analytical or theoretical ordering while looking for linkages among codes and preliminary categories to form clusters and themes. The various codes were organized into categories, from which initial themes were identified. Identification of themes was an iterative process of reviewing various sets of data with particular attention to how they pull together. To ensure intercoder reliability, the research team employed an open coding technique that allowed for the inclusion and repetition of important concepts and opinions identified and categorized as codes in all segments of the data relative to the study objectives. Two members of the research team read and coded all transcripts independently. The coding team met regularly to compare codes to maintain consistency in the coding process. Any inconsistency identified in the coding process was resolved through dialogue and consensus. Rigor was sought via discussion across the research team of codes, categories, and themes with associated illustrative quotes and continual revisions through analysis and writing. The research team had a post-analysis interaction as well as member checking with five selected participants who agreed to verify the final subthemes and themes to facilitate the trustworthiness and credibility of the findings. The ultimate review of themes was done by all members of the research team to confirm the study objectives. Themes and subthemes were supported by selected data excerpts as illustrated in the findings below.
Findings
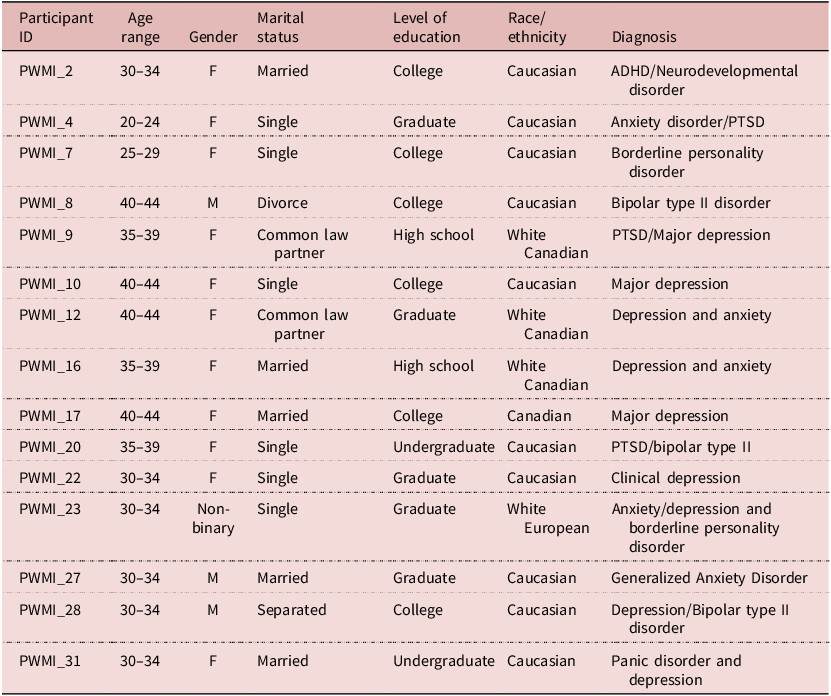
Eleven participants were female, three were male, and one person identified as nonbinary. The mean age of the participants was 36 years. All 15 participants were of Caucasian descent in a mid-sized city in Ontario, Canada. All participants had at least high school diplomas. Five had graduate degrees. See Table 2 for details on participants’ socio-demographic data.
Socio-demographic characteristics of study participants
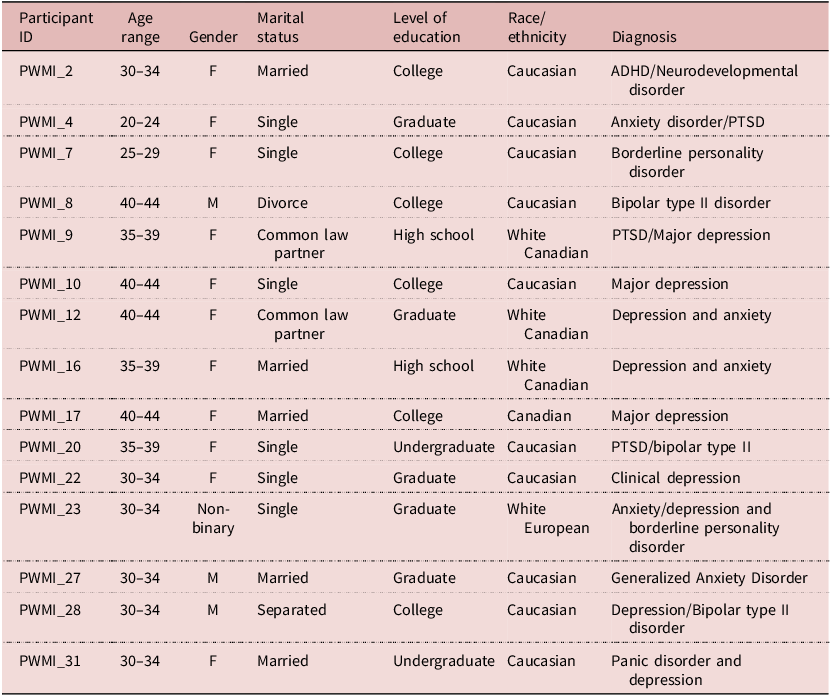
Table 2 Long description
A table with 15 rows and 6 columns detailing socio-demographic characteristics of study participants. The columns are labeled Participant ID, Age range, Gender, Marital status, Level of education, Race/ethnicity, and Diagnosis. Row 1: Participant ID, PWMI_2; Age range, 30-34; Gender, F; Marital status, Married; Level of education, College; Race/ethnicity, Caucasian; Diagnosis, ADHD/Neurodevelopmental disorder. Row 2: Participant ID, PWMI_4; Age range, 20-24; Gender, F; Marital status, Single; Level of education, Graduate; Race/ethnicity, Caucasian; Diagnosis, Anxiety disorder/PTSD. Row 3: Participant ID, PWMI_7; Age range, 25-29; Gender, F; Marital status, Single; Level of education, College; Race/ethnicity, Caucasian; Diagnosis, Borderline personality disorder. Row 4: Participant ID, PWMI_8; Age range, 40-44; Gender, M; Marital status, Divorce; Level of education, College; Race/ethnicity, Caucasian; Diagnosis, Bipolar type II disorder. Row 5: Participant ID, PWMI_9; Age range, 35-39; Gender, F; Marital status, Common law partner; Level of education, High school; Race/ethnicity, White Canadian; Diagnosis, PTSD/Major depression. Row 6: Participant ID, PWMI_10; Age range, 40-44; Gender, F; Marital status, Single; Level of education, College; Race/ethnicity, Caucasian; Diagnosis, Major depression. Row 7: Participant ID, PWMI_12; Age range, 40-44; Gender, F; Marital status, Common law partner; Level of education, Graduate; Race/ethnicity, White Canadian; Diagnosis, Depression and anxiety. Row 8: Participant ID, PWMI_16; Age range, 35-39; Gender, F; Marital status, Married; Level of education, High school; Race/ethnicity, White Canadian; Diagnosis, Depression and anxiety. Row 9: Participant ID, PWMI_17; Age range, 40-44; Gender, F; Marital status, Married; Level of education, College; Race/ethnicity, Canadian; Diagnosis, Major depression. Row 10: Participant ID, PWMI_20; Age range, 35-39; Gender, F; Marital status, Single; Level of education, Undergraduate; Race/ethnicity, Caucasian; Diagnosis, PTSD/bipolar type II. Row 11: Participant ID, PWMI_22; Age range, 30-34; Gender, F; Marital status, Single; Level of education, Graduate; Race/ethnicity, Caucasian; Diagnosis, Clinical depression. Row 12: Participant ID, PWMI_23; Age range, 30-34; Gender, Non-binary; Marital status, Single; Level of education, Graduate; Race/ethnicity, White European; Diagnosis, Anxiety/depression and borderline personality disorder. Row 13: Participant ID, PWMI_27; Age range, 30-34; Gender, M; Marital status, Married; Level of education, Graduate; Race/ethnicity, Caucasian; Diagnosis, Generalized Anxiety Disorder. Row 14: Participant ID, PWMI_28; Age range, 30-34; Gender, M; Marital status, Separated; Level of education, College; Race/ethnicity, Caucasian; Diagnosis, Depression/Bipolar type II disorder. Row 15: Participant ID, PWMI_31; Age range, 30-34; Gender, F; Marital status, Married; Level of education, Undergraduate; Race/ethnicity, Caucasian; Diagnosis, Panic disorder and depression.
Key: PWMI-Persons with mental illness.
Analysis of participants’ presentations of their lived experiences resulted in five major themes: (1) diagnosis as a ‘double-edged sword’; (2) potential familial isolation; (3) familial stigma as societal stigma localized; (4) stories of acceptance and support; and (5) confronting potential familial mental illness stigma.
Diagnosis as a ‘double-edged sword’
The combined narratives of the participants indicated both positive and negative effects after their formal diagnoses of mental illnesses. The researchers differentiated these experiences through two sub-themes: ‘a huge relief’ and ‘unfair treatment’.
A Huge relief : A diagnosis of a mental illness can be a relief, particularly if families are supportive and services are available. It can be a form of validation if the individual suspected what they were experiencing or was seeking a formal categorization of their experiences. Some participants felt liberated after their diagnoses, particularly if a diagnosis opened doors to treatment:
… I [participant] felt relieved and validated and understood myself a little more. I was able to prepare and implement tools in my life that will alleviate outbursts or hyper vigilance, and I’m able to understand and do some background research on my diagnoses and what the best course of action is to support them. And then be able to openly explain to people…. (Participant 2).
Comforted to know that there was a name for what I [participant] was having, there was a path to pursue that could help make it more manageable, and that it wasn’t something I just had to accept forever. Felt quite good after the diagnosis. It felt good to have a diagnosis and a plan (Participant 27).
These participants saw a confirmation of their diagnosis from experts as a sigh of relief as it offered them an opportunity to look at options necessary for treatment and possible recovery. Having struggled for many years with poor mental health problems, their diagnosis allowed them to have a plan to improve their mental status and better explain their condition to others.
Diagnoses could also be a relief where family members presented a degree of doubt about the validity of their experiences:
It [participant diagnosis] was like it was a huge relief for me because I think I had known it for many years, it was waiting for a doctor to finally confirm it. And then being able to kind of look at treatment options, which for borderline are extremely limited, but it gave a name to something, because it was more than anxiety, it was more than depression. So, for me, it was relief from some fear. … I think a lot more now is kind of having tried different things. It’s kind of a hopeless diagnosis, it feels like. But at that point, it was like, okay, thank God, someone said it. Who’s educated and knows what they’re talking about (Participant 7).
… I [participant] would say [that] before I was diagnosed with depression, one of my parents thought I was lazy. That was really hurtful and not understanding what I was going through. Luckily, when I was diagnosed, they were understanding. And then one of my siblings recently a few years ago, became very judgmental toward me, and he started saying things like, I was lazy and should work more and stuff like that. …, but he doesn’t know much about my mental health. So, if I talked to him about my mental health, I don’t know if he [a family member] would act differently, or he might. He thinks that I have like a victim mentality, so I don’t know what you would think if I told him I have complex PTSD (Participant 9).
This implies that the misconceptions associated with mental illnesses can lead some family members to question the personal traits of their loved ones with mental illnesses, as these families might doubt the capabilities of their relatives and liken them to being reckless. These stereotypes could damage the self-esteem and self-efficacy of affected individuals and prolong their recovery.
Unfair treatment : Conversely, some participants felt rejected by their families, particularly their parents, due to a diagnosis of mental illness. The insecurity experienced by these participants was not helpful for their mental health recovery due to the ongoing emotional conflicts within the immediate environment. Participants stated how they were treated differently by their parents compared to the rest of the family members:
… I [participant] would say it’s always been the same, that I have never really been included, it’s just been for different reasons. So, it used to be because I was the youngest one. And then after that, it was because I have [a] mental illness. And it’s almost as if, like I know my mom doesn’t involve me and things because she’s constantly saying well, I don’t know if you’re going to be alive, so what does it matter. Um, my dad doesn’t include me at all anymore since my parents split up (Participant 7).
This feeling of insecurity within the participant’s environment is not helpful to their mental health recovery due to associated emotional conflicts.
But I [participant] feel like he [Dad] just judges me a bunch more than my other siblings. …I guess he judges me differently [from] my sister. So, I feel like he kind of discriminates [against] me that way (Participant 10).
This suggests that persons with mental illnesses may experience stigma around their diagnosis in terms of differential treatment tied to perceptions of how personal character is linked to mental illness. Another participant shared:
… my older brother and I have both had mental health diagnoses. And we are both sort of seen [as] the black sheep of the family. I’m sort of like we’re considered less reliable and less trustworthy. … (Participant 16).
The participant’s view illustrates that persons with mental illnesses may be perceived as different from the rest of their family members. For instance, in this case, they were seen less reliable and mistrusted within their family due to their condition, which is demotivating for focusing on recovery.
Also, differential treatment experienced by some participants made them feel helpless within their households. The negative attitude exhibited by family members contributed to the distress that participants endured after their diagnoses of mental illnesses. A participant explained how they felt rejected by their family members due to a diagnosis:
…more secluded and more rejected and just kind of regretting them. Because I [participant] was being treated differently. … I think some of it is still the stigma around it [mental illness]. … (Participant 17).
This participant had a difficult time within their immediate environment just after a diagnosis, and they also talked about how they were kept out of information sharing within the family. The feeling of exclusion in family decision-making could negatively impact their already affected mental health.
Potential familial isolation
A common implicit form of stigma was isolation. Participants discussed the potential for isolation from family members under the following subthemes: breakdown of romantic relationships and isolation/loneliness.
Breakdown of romantic relationships : For some participants, their mental illness was perceived as a barrier to having romantic relationships:
It [mental illness] makes life unlivable. And I [participant] can’t work. I rarely go out, [and] romantic relationships are basically off the table. … (Participant 7).
These observations reflect that persons living with mental illnesses face many challenges due to the misconceptions connected to mental health problems at both the family and community levels. These challenges may include the breakdown of romantic relationships or difficulties in forming romantic relationships, which some participants, in turn, linked to low self-efficacy and personal empowerment as well as emotional suffering.
For others, it is the lack of understanding of their illness that leads to relationship breakdown:
Some days are really bad, there’s no real in between anymore. It is just that some days are terrible. …I’ve had relationships fall apart because my partners do not understand me (Participant 10).
One participant described their past relationships:
…they’re complicated because of the diagnosis. My [participant] emotions are zero to 100; they’re very unpredictable. There’s a lot of fear of abandonment. And there are issues with just trusting people, me reading other people’s behavior in a certain way that might not actually be the way it is. And so even if it was like a really positive relationship. For me [participant], it’s usually not a positive relationship with the other person. Because my symptoms are just there [and] they’re a lot to deal with (Participant 7).
The participant’s opinion indicates that the unpredictability of the symptoms associated with mental illness make it difficult for persons with mental health problems to keep romantic relationships at times.
Isolation/loneliness : Apart from preventing or undermining intimate relationships, mental illness stigma was also perceived as isolating participants from their family members, contributing to increased feelings of loneliness. Without family members’ openness to discussing their health conditions, some participants internalized their experiences. Participant’s perception of mental illnesses can negatively impact their self-esteem and their ability to maintain healthier relationships. The barriers they face to making friends and staying connected with people can result in the internalization of personal issues that, under normal circumstances, could be shared with their loved ones for support.
Another participant described their opinion on the turn of events within the family post-diagnosis, where they felt excluded within their family:
I [participant] feel like I’m not really included in a lot of stuff that happens in my family, I feel like I’m kind of an outsider. … it probably is if you compare before my diagnosis. I feel like before, they [family] were a little bit more open with asking me stuff. And now it’s like if they don’t want me to worry and stuff like that. Then they just keep me out of it, and they’ll just tell my sister … (Participant 10).
There seems to be an issue of trust versus mistrust among the participant and their family, which could exacerbate emotional distress that might negatively impact the participant’s mental health.
Several participants identified a lack of knowledge of specific mental illnesses by family members as a factor that accounted for various discriminations and stigma against persons with mental illnesses. A participant commented:
I [participant] think part of it is a lack of understanding, and I think even if they read everything that there was to know about borderline, until you live it and have lived experience. You don’t fully understand the person…, and I also think that the way I treat them sometimes, because of my disorder, people get fed up. I mean, no one wants to be treated poorly. … (Participant 7).
That is, some family members treat their loved ones with mental illnesses poorly at times. Good family relationships devoid of any partiality could result in social support for persons with mental illnesses. However, several of the study participants reported unfair treatment within the family, which negatively impacted their mental health. A participant commented:
Um, …My [participant] dad doesn’t include me anymore …. My brother is kind of based on his own life. He’s getting married in August, and I’ve met his fiancée once; he just keeps me out of his life … (Participant 7).
This participant also added:
…There’s a feeling in my family that mental illness doesn’t exist, except there’s so much mental illness that runs family. Um, … I don’t know how to go into it in detail because I know I’m answering this kind of generally within the family (Participant 20).
The complex interplay of familial relationships and mental illness stigma could be a reason for the discrimination experienced by these participants within their families, particularly the perceived lack of knowledge about mental health problems.
Familial stigma as societal stigma localized
In considering stigma experienced from their family members, or more generically speaking to their thoughts on familial stigma, participants noted that this form of stigma is inseparable from more general societal stigma around mental illness. That is, familial stigma is just one form by which more general mental illness stigma is enacted. Familial stigma as societal stigma localized is composed of four subthemes: ‘perceived dangerousness’; ‘exclusion from the circle of information within the family’; ‘loss of status or perceived incapability’; and ‘false narratives around mental illnesses.’
Perceived dangerousness : Participants noted that the general social narrative of people living with mental illness as ‘dangerous’ was taken up uncritically by family members and might be rooted in a lack of knowledge around mental illness:
I [participant] think it’s just that they [family members] find it kind of scary and unpredictable. I think that it’s something that they don’t understand. And unfortunately, haven’t done a lot of work to try and understand it. So, they put themselves in a kind of bubble, like they don’t understand mental illness, and they don’t make strides to try and understand it…. (Participant 16).
… It’s a challenge to support somebody when you don’t have tools, or you’re scared of it, or you’ve been brought up that you know, this is how people behave, and there’s no other way and if people are acting erratic or hearing things then, you know, they’re dangerous or they’re going to hurt you or your religion plays a piece in that and you’re cast out of your family and, or there’s just no resources and early diagnosis is not an option. … (Participant 2).
Participants noted fear and powerlessness among family members when it comes to relating with persons with severe mental illnesses, as they at times consider their loved ones as dangerous, depending upon the intensity of their symptoms.
Loss of status/ perceived incapability : Another social perception of mental illness is that of decreased capability. Mental illness is sometimes seen as a social disability by some families, which may result in loss of status:
…I [participant] think it’s just a bad family dynamic that I’ve been working to fix. They [family] may assess, fault-finding, or blame [you] with it. So, they may say that. and you did this, and this is the outcome of this. It may be just jockey[ing] for power…. (Participant 8).
One aspect of broader social stigma is the idea of mental illness as a shameful condition. One participant shared how this unfolded within their own family:
I [participant] think part of it is that they [family members] don’t understand what mental illnesses are, and like where my [participant] parents grew up. It wasn’t like we didn’t really talk about mental illness. You just kind of said, Oh, you know that person … has some sort of issue, or something like that, and I think it’s just the lack of understanding and lack of knowledge. I think it’s kind of the same, like a lack of understanding and lack of knowledge about it [mental illness]. …. So, they can’t understand that their loved one or significant other has some sort of mental illness (Participant 10).
This quote reflects the fact that some families fail to understand their loved ones with a mental illness diagnosis. The lack of in-depth understanding of mental illnesses continues to impact how their family responds to their loved one’s struggles. Again, the silence around mental illnesses has contributed to the family’s inability to fully grasp or accept that someone they love might be experiencing a mental health condition.
False narratives around mental illnesses : Most of the participants reported that misinformation and a lack of understanding of mental health issues at the family level continue to be the driving force behind the at times negative attitudes of family members towards their relatives with mental illnesses. A participant remarked:
I [participant] think there’s a lot of misunderstanding about mental illness. A lot of people think someone who’s mentally ill isn’t capable. Sometimes they [the family] feel like they’re too much to deal with, or they might think that the person isn’t trying hard enough, like there’s a lot of misunderstanding and misinformation about mental health [and mental illnesses] (Participant 9).
Participant accounts echo the need for familial education on mental illnesses to correct the existing misinformation about mental health issues to avoid needless discrimination against affected persons and rather offer them both practical and emotional support to help improve their mental health.
Stories of acceptance and support
While the focus was on experiences of stigma, several participants were also intentional in sharing the positive journeys they had with their family members. They shared explicit ways in which family members showed acceptance. This included noting family members’ understandings of mental illnesses, which resulted in providing both practical and emotional support. Some participants stated:
My [participant] family has been very supportive. Once my therapist confirmed that I [participant] needed a year off, they were supportive. … When I was taking my year off, I was still living at home, so I got to live with them full time. They took me to appointments when needed, and I could talk with them. When I was feeling upset and just needed to vent. … (Participant 23).
Um, so they [participant’s family] play a very big role, they’re usually able to find out triggers and kind of bring me out of them or not, place me in situations where I [participant] feel I’m threatened or understand that I might need a little bit more redirecting during the day or during an activity, being more patient and, you know, pushing me to seek more support and help, and just being there so they do play a very big role (Participant 2).
The viewpoints of participants imply that having the full support of family members within one’s immediate environment and feeling love without any intimidation and restrictions is key to their mental health recovery. Moreso, some participants perceived their families as safety nets anytime they felt overwhelmed with emotions. Practical and emotional support from family members made some participants feel included within their families. A participant noted:
…, there can be some financial support from my mom, she’ll try [to get me] groceries or other things. They [participant’s family] live in a different city with my stepdad, but when they’re here. They will try and help me, like if I [participant] need to go pick up a prescription. They’ll help, because I don’t drive so they’ll help me do that. She [mom] used to go to the doctor with me if I needed her support of listening, is a big thing. When it comes down to it, if it’s three in the morning and something is really bad, she’ll pick [me] up. … (Participant 7).
‘My husband has been supportive of anything that I needed to do. Whether it be conversational or going on medication when I was on that or talking to somebody else’ (Participant 31).
Where relationships were positive and free of stigma, family members were seen as part of the recovery journey: ‘…But when I do eventually move out, I can still talk to them if I’m having any issues or seek advice or just vent if there’s something I need to talk about’ (Participant 23).
Confronting potential familial mental illness stigma
Participants actively shared ways in which they were confronting familial mental illness stigma themselves. Participants expressed strategies to confront familial mental illness stigma in four subthemes: ‘education’ (social contact-based education and familial education); ‘normalizing the symptoms of mental illnesses’; ‘selective versus full disclosure’; and ‘concealment’.
Education : Because familial mental illness stigma is an outcome of broader social stigma, as noted in the theme above, participants recommended public education as a pathway to reducing personal experiences of stigma. Participants saw ongoing public dialogue and understanding of mental illness as beneficial:
…We have to keep talking about [mental illnesses] more positively, like what Bell Let’s TalkFootnote 1 is doing of late …. I think that diagnoses that are less common or more severe mental illnesses need to be seen in the light more because we hear about anxiety and depression so much. Whereas, you know, personality disorders are looked at with a more negative point of view, people with schizophrenia are very misunderstood [and are] thought to be dangerous. So, I think …, debunking a lot of myths, which is just going to take time and effort on people’s part, and people who have a position of power, who, you know, people are listening to. Outside of that, I’m not really sure. I think until you’ve lived it. I think a lot of people have a kind of closed mind, or a lack of understanding, until they’ve lived it and walked in someone else’s shoes (Participant 7).
Participants reiterated the need to modify societal knowledge on mental illnesses through contact-based education with intentionality. This will inform members of the public about the multifaceted nature of mental illnesses and the need to come close to them to better understand their predicaments and ways to curb stigma towards them.
Another participant centred on their lived experiences of individuals in this type of education:
I [participant] think the more people listen instead of just trying to get a response that they think they want and then respond. I think listening is the biggest key. I think if I were more listened to instead of just talking to them. I think my outcome would be a lot different (Participant 28).
Many participants also highlighted the need for mass media to change their approach towards the presentation of mental health problems in the news. Participants questioned why news reporters and presenters often concentrated mostly on the negative aspects of persons with mental illnesses without showing the good things that some individuals with mental health issues had done or could do:
I think a lot of it [mental illness stigma] is from the media. …I remember the movie ‘Split’ came out a number of years ago, and the person had multiple personality disorder, and one of the personalities was a serial killer, and that was the plot. And so, it just emphasizes that people with mental illness are bad or are harmful…. I think especially with the more serious diagnoses like schizophrenia, we [society] have a fear of it. It’s somehow scary or bad when, in fact, it’s just people living their lives. In fact, in my first year, I took a psychology course, and I realized how wrong I was about what I thought schizophrenia was until I was taught, because that was just my perception, from the media, growing up… (Participant 23).
This participant blames the media for the increase in stigma around mental illnesses, particularly when criminality in media is often tied to a psychiatric diagnosis and highly criminals in various movies are tagged with personality disorders. This, according to the participant, adds to the misconceptions associated with mental illnesses. They, therefore, admonish the media to correct this impression by replacing such negative connotations with positive ones to sanitize the public space and help close the ‘us and them’ gaps in society. For instance, the use of movie characters to portray positive achievements of persons living with mental illnesses can be helpful in reducing the negative perceptions connected to mental health issues than the frequent display of negativities.
When it comes to familial education in particular, participants noted that persons with mental illnesses (PWMIs) are often put in the position of needing to educate their own families to reduce stigma. They noted that this should be better done through formal support:
…meeting people where they are and listening to their [persons with mental illnesses] stories. I think it is important because if we only know the experiences that we’re seeing on TV of those extreme cases or somebody’s portrayal of mental illness versus their daily life, then we’re going to be biased and learning that mental illness is multifaceted out there (Participant 31).
Normalizing the symptoms of mental illnesses : Participants suggested anti-stigma campaigns to make mental health concerns part of everyday conversation. Several participants pointed to correcting the myriad of false impressions about persons with mental illnesses regarding their capabilities and inabilities. A participant requested that society pay more attention to the competencies of persons with mental illnesses than to their challenges:
I [participant] think we need to stop treating people with mental illness as if they are incapable or that they are less. And I think that we [society needs to] change the language that we use towards people with mental illness. … Same thing if you see somebody [who] is manic, it is that they’re crazy, and people get all these preconceived notions, so I think really the language that we use is a big one, and policymakers as well. I think that we need to be looking at our health care system and how we handle mental illness, when it comes to seeking out help at every level, whether it is accessible therapy or needing to go to the hospital for additional supports or a lifelong waitlist to see a psychiatrist…. (Participant 31).
For some participants, the normalization of mental illnesses could be done by engaging the media to continue the talk about the positive contributions of PWMI. That is, emphasizing the acceptance of PWMI within the social realm will also pave the way for family members to de-stigmatize and support their loved ones with a diagnosis:
I [participant] think more education and more de-stigmatizing it [mental illnesses], like more people talking about it. And it’s being a normal part of conversations without the [usual] judgment. So, I think like the media, they’ve done some great things with having more people in high-status roles, actors or sports or whatever, speaking about it [mental illnesses], because it normalizes it even more… (Participant 17).
Another participant made a similar point:
Just lots of education of the public, lots of awareness raising…. You [participant] know through movies [and] advertisements, even through [the] school curriculum. … I think government efforts to educate the public on signs and symptoms [of mental illness]. I think normalizing is key (Participant 12).
Disclosure : That is, leading the conversation. For some participants, being open about their experiences and driving the normalization of mental illnesses was a part of how they personally confronted stigma. For these participants, disclosure to family members about their mental illnesses offered an opportunity for support and to educate them or redirect them to mental health professionals for the best answers to difficult questions about their diagnosis. The participants believed full disclosure was an important step in reducing familial stigma:
Yes, they [friends] do know. …. They were completely supportive, didn’t treat me any differently, and just asked if there was anything that they could do to help with it [diagnosis], …. He [romantic partner] was the one who encouraged me to seek out the diagnosis (Participant 17).
Using disclosure as a strategy to confront potential familial mental illness stigma, other participants remarked:
…I [participant] sought out a diagnosis, I openly talk about my struggles to demystify, inform my partner, and my children…
In my professional experience as a frontline worker with a mental illness experiencing workplace trauma, moral injury, and the stigma that comes with being unwell in the workplace, I openly talk about it, but attempt to mask and cover a lot of the time. In my career, many of us are unwell and injured from the work, and many of us cope with that differently… (Participant 2).
Yes, I believe in building awareness about it [mental illness], and if you don’t talk about it. Then it becomes complex…. Yeah, everyone who knows me knows about it [mental illness]. Yeah, I don’t hide it by any means, you know. Sometimes you’re talking to some other person who’s gone through something you don’t know [about] them. And then you’ll just go into a dialogue with them (Participant 8).
The quotes from these two participants suggest the importance of public disclosure as a good step where affected persons can share their lived experiences of mental illness for social support and coping strategies, especially with people who have gone through similar experiences and with close relatives.
Discussion
Persons living with mental illnesses can face ongoing stigma, including that enacted by their close relatives – familial mental illness stigma. The study findings suggest that familial mental illness stigma is very much interconnected with the broader public mental illness stigma. Rather than being fully distinct, participants saw value in addressing mental illness stigma both within and beyond families. By using a phenomenological approach, the researchers centred the experiences of participants to understand the contextual relationships; for example, noting how for some having a formal diagnosis of mental illness creates clarity and understanding, and for others, it is seen as increasing their risk of stigmatization.
The researchers have proposed five aspects of familial mental illness stigma notable among participants. These included: diagnosis as a ‘double-edged sword (positive and negative effects following a diagnosis), potential familial isolation (possible exclusion once a diagnosis is confirmed), familial stigma as societal stigma localized (familial mental illness stigma engrained in broader social stigma), stories of acceptance, and confronting potential familial mental illness stigma (strategies to reduce familial mental illness stigma). Each of these domains was present in some stories of participants, although there were notable differences in levels of support and levels of stigma experienced by participants. Some participants shared directly about their experiences of stigma within their families. Others who had very positive personal experiences speculated more generically on the familial mental illness stigma encountered by others.
Across the experiences, there is a considerable potential compounded impact of familial mental illness stigma. Those whose symptoms were not understood in advance of diagnosis often encountered increased stigma at diagnosis, or hid diagnoses, and lived with ongoing challenges with family (such as isolation). In a Canadian context where the family often plays a key role in supporting ongoing recovery, stigma did not simply influence how participants felt about themselves but could also directly impede their recovery journey. These conclusions are congruent with the findings of previous studies that underscore the after effects of persons labeled with mental illnesses to include the potential for loss of social status, poor housing or homelessness, unemployment, social isolation, and poor health care and suicidality (Link and Phelan, Reference Link and Phelan2001; Oexle et al., Reference Oexle, Rüsch, Viering, Wyss, Seifritz, Xu and Kawohl2017, Rüsch et al., Reference Rüsch, Corrigan, Waldmann, Staiger, Bahemann, Oexle and Becker2018; Mejia-Lancheros et al., Reference Mejia-Lancheros, Lachaud, Woodhall-Melnik, O’Campo, Hwang and Stergiopoulos2021). As well, isolation due to mental illness stigma can result in self-stigma and its social and psychological implications on the individual’s self-esteem and self-efficacy – having validated their circumstances against the public perception of mental illnesses (Rüsch et al., Reference Rüsch, Angermeyer and Corrigan2005; Corrigan et al., Reference Corrigan, Larson and Rüsch2009; Dubreucq et al., Reference Dubreucq, Plasse and Franck2021).
Another significant finding identified by this study was the risk of breakdown of romantic relationships. Romantic relationships are often the most important familial relationship, and participants spoke to both impediments and breakdown of relationships with partners due to mental illness stigma. While some of participants were still married and receiving maximum support from their partners towards recovery, several others suffered divorce or separation that they attributed directly to their illnesses. This further impacted their mental health and impeded recovery. This observation is consistent with earlier studies which found that a diagnosis of mental illness can lead to a breakdown in relationships, or concealment as a protective process capable of creating issues of credibility (Amankwaa, Reference Amankwaa2003; Rivera-Segarra et al., Reference Rivera-Segarra, Rivera, López-Soto, Crespo-Ramos and Marqués-Reyes2014; van der Sanden et al., Reference van Der Sanden, Bos, Stutterheim, Pryor and Kok2015; Ladd, Reference Ladd2018).
Noticeably, familial mental illness stigma is entrenched in broader social stigma. Societal views on mental illnesses are not differentiated from individual families, as families are part of society. Therefore, the misconceptions connected with mental health problems within public settings also diffuse to various families at the community level, which are then enacted in households. For instance, the perceived dangerousness of persons with mental illnesses reported by some participants in this study could be a cumulative effect of what exists within public narratives regarding serious mental illness. This can be a very specific stigma related to exclusive conditions such as schizophrenia which are framed as ‘dangerous’ within public narratives (Watson et al., Reference Watson, Hanrahan, Luchins and Lurigio2001; Gottfried and Christopher, Reference Gottfried and Christopher2017; Ghiasi et al., Reference Ghiasi, Azhar and Singh2022). The alleged dangerousness of affected individuals through media reporting can be attributed to why some family members might isolate PWMI within the family system.
Exclusion from the circle of information within the family was another challenge that PWMIs faced. Several of the study participants revealed that their families considered them as ‘lesser’ due to their illness. The family, therefore, excluded them from family discussions, especially important matters that needed attention from all family members. Some individuals experience a loss of status at the family level, particularly where affected persons were highly positioned within the family structure before their mental illness diagnosis. Loss of status within one’s family can have cumulative effects on their self-worth and further deteriorate their ability to exercise autonomy in the family as one becomes mindful of the socially endorsed exclusions. This finding is consistent with a considerable body of evidence that loss of social status within the family unit among PWMIs leads to negative psychological effects (Iseselo et al., Reference Iseselo, Kajula and Yahya-Malima2016; Larson and Corrigan, Reference Larson and Corrigan2008; Umberson and Karas Montez, Reference Umberson and Karas Montez2010; Rössler, Reference Rössler2016).
The recovery of PWMIs is linked to the combined support of family members, social support services, and health professionals (Public Health Agency of Canada, 2006; Larson and Corrigan, Reference Larson and Corrigan2008; O’Reilly et al., Reference O’Reilly, Paul, McCahon, Shankar, Rosen and Ramzy2019; Bjørlykhaug et al., Reference Bjørlykhaug, Karlsson, Hesook and Kleppe2021). This documented evidence is paralleled to the current findings that regardless of the difficulties confronting families when a relative is diagnosed with one or more mental illnesses, continuous understanding and support (practical and emotional) within the family is vital to the recovery and rehabilitation of affected family members. Some participants saw this support as a safety net to rely on as part of a positive recovery journey. Likewise, some participants attested to a myriad of support received from health professionals while taking steps to improve their mental health. This finding aligns with that of Larson and Corrigan (Reference Larson and Corrigan2008) that psychiatrists and other health professionals have contributed immensely to reducing the negative impact of family stigma. If there are available social support systems with commitments from family members of PWMIs, individuals will be able to better manage their recovery.
Given the many roles played by the family unit in supporting PWMI, it could be difficult for affected individuals in their home environment if they are victimized by some family members with stigmatizing beliefs. Some study participants disclosed selective versus full disclosure and concealment as strategies to deal with familial mental illness stigma. Strategic or selective disclosure is a known approach used by persons with PWMIs to carefully identify whom to share their diagnosis with to sidestep the societal discrimination and devaluation that at times comes with full disclosure of mental health problems (Hyman, Reference Hyman2008; Karnieli-Miller et al., Reference Karnieli-Miller, Perlick, Nelson, Mattias, Corrigan and Roe2013; Corrigan et al., Reference Corrigan, Rüsch and Scior2018; Rüsch and Kösters, Reference Rüsch and Kösters2021). In their quest to reduce the harmful consequences of familial mental illness stigma, some participants of this study employed strategic disclosure to share their mental health issues with a few reliable relatives for support. On the contrary, other participants fully disclosed their mental health diagnosis to family members for support and to prevent the psychological stress of having to hide their symptoms during critical periods. For these participants, educating family members about their conditions to correct any preconceived notions about mental illnesses before a disclosure helped in reducing stigma at the family level. Although disclosure of a mental illness diagnosis in the social realm comes with both advantages and disadvantages (Hyman, Reference Hyman2008; Evans-Lacko et al., Reference Evans-Lacko, London, Japhet, Rüsch, Flach, Corker, Henderson and Thornicroft2012; Quinn, Reference Quinn, Major, Dovidio and Link2018; Rüsch et al., Reference Rüsch, Malzer, Oexle, Waldmann, Staiger, Bahemann, Wigand, Becker and Corrigan2019), disclosure within one’s immediate environment has the likelihood to reduce stigma, strengthen intimate relationships, improve social support, and quality of life (Corrigan and Rao, Reference Corrigan and Rao2012; Rüsch et al., Reference Rüsch, Malzer, Oexle, Waldmann, Staiger, Bahemann, Wigand, Becker and Corrigan2019; Brouwers et al., Reference Brouwers, Joosen, van Zelst and Van Weeghel2020; Corrigan, Reference Corrigan2022). Despite the social benefits connected with the disclosure of a mental illness diagnosis within one’s family, some participants of this study adopted concealment to reduce familial mental illness stigma because they were unsure of the consequences of disclosure. This observation closely aligned with the findings of past studies that concealment in a stigmatizing environment is a realistic choice that is usually not driven by self-stigma or shame (Rüsch and Kösters, Reference Rüsch and Kösters2021). That said, irrespective of the environment of PWMIs, their previous experiences of stigma within the public space can play a role in hindering their ability to disclose a diagnosis (Bril-Barniv et al., Reference Bril-Barniv, Moran, Naaman, Roe and Karnieli-Miller2017; Rüsch et al., Reference Rüsch, Rose, Holzhausen, Mulfinger, Krumm, Corrigan, Willmund and Zimmermann2017). Further, concealment in this sense was a necessity to receive equal treatment and to prevent any conflict that their disclosure might bring to the family in the long-term (Bril-Barniv et al., Reference Bril-Barniv, Moran, Naaman, Roe and Karnieli-Miller2017). A few of the participants reported on familial-driven concealment, particularly where family members were aware of their mental health challenges and pressured them to conceal their illness to protect the family and the affected individual against the impacts of social stigma. This presupposes that stigmatizing behaviours of some family members against their loved ones may be well-intentioned. That is, by concealing the mental illness, families may be striving to be supportive or to protect them from possible societal discrimination. While this strategy can help protect the family’s interest in keeping news of the illness among themselves, it could have ramifications for both the family and PWMIs regarding access to support.
Research implications
The findings of this current study highlight the existence of mental illness stigma within family systems. Findings also point to issues confronting PWMIs concerning decision-making and information sharing within families, with implications for self-stigma and future concealment. Further, the findings – combined with those of previous studies – underscore disclosure and concealment as strategies to reduce familial and other forms of mental illness stigma. Both approaches have downstream impacts on PWMI and their relatives (Bril-Barniv et al., Reference Bril-Barniv, Moran, Naaman, Roe and Karnieli-Miller2017; Rüsch et al., Reference Rüsch, Malzer, Oexle, Waldmann, Staiger, Bahemann, Wigand, Becker and Corrigan2019). To help curtail these consequences, some participants recommended public education in the form of persuasive communication on serious mental illness using social contact-based education and familial education. For these participants, all forms of mental illness stigma start from social stigma; hence, transformative education to sensitize public perceptions could help reduce familial mental illness stigma. Therefore, the investigators propose an increase in discussions around social contact-based education with intentionality, where persons with lived experiences of mental illnesses and those without will converge to have conversations on mental health issues and ways to reduce stigma. The investigators also recommend that practitioners pay more attention to family members to understand their potential for stigmatizing beliefs while supporting affected persons in recovery. While future research should be focused on strategies to prevent the ongoing familial mental illness stigma for all mental health challenges, investigators recommend that future research also focus on understanding the nuances of why family members themselves might at times contribute to stigma.
Policy implications
Based on the findings of this recent study, reducing familial mental illness stigma at the family level requires action by policy-makers to develop systems that ensure a transformative approach to curb societal stigma against PWMIs. For instance, there is the need for some community and social service resources to be directed towards public education (transformative and social contact-based education) to reduce the known preconceived notions about mental illnesses within society at large, as seen in the work of the Mental Health Commission of Canada (MHCC) and Headspace in Australia. In this context, the experiences of PWMIs will be appreciated by society to help bridge the existing ‘us and them’ gap. The researchers suggest that such anti-stigma campaigns should continue to be enhanced to make mental illness part of everyday conversation and continue the normalization process of mental illness symptoms in the social realm. Further, the normalization of mental illnesses could be achieved through continuous engagement of both traditional and social media providers to confront stigmatizing presentations of mental illness as they occur.
Limitations
This study is limited by the age restriction (24 and above), which prevented the researchers from including adolescents or children living with mental illnesses. The study is also narrowly focused in terms of gender, given that only three males participated in the study compared to eleven females, all of whom were Caucasian. The study, therefore, lacks diversity, as most of the findings were from English-speaking, adult, and white female perspectives. Data were collected through the Zoom platform owing to the COVID-19 restrictions, which made it challenging to directly recruit more participants and to ensure diversity across participants. Future researchers wishing to build on the conclusions of this study should pay specific attention to the context in which these data were collected.
Conclusion
This study has contributed to knowledge on mental illness stigma, particularly familial mental illness stigma among participants who live in a high-income country. Participants’ stories indicated familial stigma experiences negatively affected their psychological well-being and personal empowerment. This study affirms the existence of familial mental illness stigma, even though it is often the most unspoken or unacknowledged form of stigma. Familial mental illness stigma at times results in relationship bias or unfair treatment within families and further impacts some participants’ mental health and impedes their recovery. It is worth mentioning that not all family members stigmatized their relatives with mental illnesses per the study participants’ narratives. Some participants had the full support of family members towards their mental health recovery, while others felt mistreated. Some of this mistreatment seemed explicitly ill-intended, whereas other actions appeared to be attempts by family members to protect their loved one, but in doing so demonstrated how their condition was stigmatized or stigmatizing. Most notably, the study revealed familial mental illness stigma as a societal stigma localized at the family level. That is, family members’ fear of social stigma due to their association with relatives diagnosed with mental illnesses (associative stigma) may have compelled some of them to save face, but in doing so made their loved one feel more isolated. The findings help the researchers understand the interconnected nature of different forms of mental illness stigma. The study participants recommended broader discussions on the future of mental illness and social stigma using social contact-based education. The researchers propose further studies to include longitudinal research that comprises PWMIs, family members, and health professionals to explore the connections between associative stigma and familial mental illness stigma.
Acknowledgements
The researchers would like to thank all participants who shared their unique stories with the research team on this sensitive topic. Hopefully, this work will promote broader conversations around familial mental illness stigma to influence policy and practice to create enabling environments at the family level to foster all-inclusiveness.
Financial support
This research was supported by the Arthur Labatt Family Chair in Nursing Leadership in Health Equity (R4930A30).
Competing interests
The researchers have no conflict of interest.
Ethical standard
Ethical approval for this study was obtained from the institutional review board of Western University (#119602).

 Open access
Open access