


Introduction
Approximately 322 million people around the world suffer from depressive disorders, such as major depressive disorder and persistent depressive disorder (World Health Organization, 2017), and recent estimates indicate that millions more people developed these disorders due to the chronic stress of the COVID-19 pandemic (Santomauro et al., Reference Santomauro, Herrera, Shadid, Zheng, Ashbaugh, Pigott, Abbafati, Adolph, Amlag and Aravkin2021). If left untreated, depressive disorders interfere with academic, occupational, and social functioning (Adler et al., Reference Adler, McLaughlin, Rogers, Chang, Lapitsky and Lerner2006; Heiligenstein et al., Reference Heiligenstein, Guenther, Hsu and Herman1996; Hirschfeld et al., Reference Hirschfeld, Montgomery, Keller, Kasper, Schatzberg, Hans-Jurgen, Healy, Baldwin, Humble and Versiani2000; Kessler, Reference Kessler2012; Kessler et al., Reference Kessler, Berglund, Demler, Jin, Koretz, Merikangas, Rush, Walters and Wang2003; Whooley et al., Reference Whooley, Kiefe, Chesney, Markovitz, Matthews and Hulley2002), and increase risk of physical health conditions and suicide (Ferrari et al., Reference Ferrari, Charlson, Norman, Patten, Freedman, Murray, Vos and Whiteford2013; Mezuk et al., Reference Mezuk, Eaton, Albrecht and Golden2008; Rugulies, Reference Rugulies2002). Although effective treatments exist for depressive disorders (Bauer et al., Reference Bauer, Whybrow, Angst, Versiani and Möller2002; Davidson, Reference Davidson2010), most people do not receive even minimally adequate treatment (Thornicroft et al., Reference Thornicroft, Chatterji, Evans-Lacko, Gruber, Sampson, Aguilar-Gaxiola, Al-Hamzawi, Alonso, Andrade and Borges2017). This treatment gap is partly driven by physical and psychological barriers that hinder access to high-quality care, such as stigma, fear of being seen accessing mental health services, mobility issues, and geographical location (Andrade et al., Andrade et al., Reference Andrade, Alonso, Mneimneh, Wells, Al-Hamzawi, Borges, Bromet, Bruffaerts, De Girolamo and De Graaf2014; Clement et al., Reference Clement, Schauman, Graham, Maggioni, Evans-Lacko, Bezborodovs, Morgan, Rüsch, Brown and Thornicroft2015; Mohr et al., Reference Mohr, Hart, Howard, Julian, Vella, Catledge and Feldman2006; Moroz et al., Reference Moroz, Moroz and D’Angelo2020; Sareen et al., Reference Sareen, Jagdeo, Cox, Clara, ten Have, Belik, de Graaf and Stein2007). Therefore, there is pressing need to improve the accessibility and equity of treatment for individuals with depressive disorders.
Virtual care, or the use of digital technology to provide health services remotely, represents a promising approach for reducing barriers to accessing high-quality depressive disorder treatment (Lamb et al., Reference Lamb, Pachana and Dissanayaka2019; Naslund et al., Reference Naslund, Aschbrenner, Araya, Marsch, Unützer, Patel and Bartels2017; Richardson et al., Reference Richardson, Frueh, Grubaugh, Egede and Elhai2009; Stoll et al., Reference Stoll, Müller and Trachsel2020). Virtual care allows communication between healthcare providers and patients and encompasses multiple modalities, such as videoconferencing, telephone, text, and live-chat messaging. Compared with in-person care, virtual care facilitates broader and more equitable access to mental health services by reaching individuals living in remote communities with few or no mental health providers and services, reducing the cost of services (e.g. no transportation or parking costs), enhancing the convenience of services (e.g. reduce need for childcare and limit time taken off from work), as well as by circumventing the stigma associated with physically presenting to a mental health clinic (Aboujaoude et al., Reference Aboujaoude, Salame and Naim2015; Bashshur et al., Reference Bashshur, Shannon, Bashshur and Yellowlees2016; Chakrabarti, Reference Chakrabarti2015; Gros et al., Reference Gros, Morland, Greene, Acierno, Strachan, Egede, Tuerk, Myrick and Frueh2013; Myers, Reference Myers2019; Stoll et al., Reference Stoll, Müller and Trachsel2020). Moreover, evidence suggests that virtual care is a feasible, acceptable, and effective method for delivering diagnostic assessment and treatment services across diverse clinical presentations, populations, and age groups (Andrews et al., Reference Andrews, Cuijpers, Craske, McEvoy and Titov2010; Bashshur et al., Reference Bashshur, Shannon, Bashshur and Yellowlees2016; Chakrabarti, Reference Chakrabarti2015; Drago et al., Reference Drago, Winding and Antypa2016; Luo et al., Reference Luo, Sanger, Singhal, Pattrick, Shams, Shahid, Hoang, Schmidt, Lee and Haber2020; Varker et al., Reference Varker, Brand, Ward, Terhaag and Phelps2019). Although its uptake had been slow prior to the pandemic, virtual care surged globally during the COVID-19 pandemic because of its ability to enable access to care and accommodate physical distancing requirements (Gratzer et al., Reference Gratzer, Torous, Lam, Patten, Kutcher, Chan, Vigo, Pajer and Yatham2021; Montoya et al., Reference Montoya, Kogan, Rebello, Sadowska, Garcia-Pacheco, Khoury, Kulygina, Matsumoto, Robles and Huang2022). Due to the need to alleviate the suffering associated with elevated rates of depressive disorders since the onset of the pandemic (Ettman et al., Reference Ettman, Abdalla, Cohen, Sampson, Vivier and Galea2020; Santomauro et al., Reference Santomauro, Herrera, Shadid, Zheng, Ashbaugh, Pigott, Abbafati, Adolph, Amlag and Aravkin2021), virtual care is poised to remain a robust option for providing mental health services post-pandemic, even in spite of diminishing physical distancing requirements (Gangamma et al., Reference Gangamma, Walia, Luke and Lucena2022; Lo et al., Reference Lo, Rae, Amin and Cox2022; Zentner et al., Reference Zentner, Gaine, Ethridge, Surood and Abba-Aji2022; Zhu et al., Reference Zhu, Paige, Slone, Gutierrez, Lutzky, Hedriana, Barrera, Ong and Bunnell2021).
Cognitive behavioural therapy (CBT) is an evidence-based treatment for a wide range of mental health disorders, including depressive disorders (Hofmann et al., Reference Hofmann, Asnaani, Vonk, Sawyer and Fang2012), and is well-suited for virtual care. CBT is a brief, highly structured, and typically manualized treatment that follows a sequential progression, emphasizes self-responsibility, self-monitoring, as well as between-session homework (Beck, Reference Beck1995), all of which can be feasibly implemented and supported remotely. A common virtual care modality used to deliver CBT is videoconferencing (Backhaus et al., Reference Backhaus, Agha, Maglione, Repp, Ross, Zuest, Rice-Thorp, Lohr and Thorp2012; Berryhill et al., Reference Berryhill, Culmer, Williams, Halli-Tierney, Betancourt, Roberts and King2019). This modality closely resembles traditional in-person therapy by facilitating real-time communication between therapists and patients at different locations using both audio and video input. Studies have shown that videoconference CBT is a feasible and highly acceptable form of treatment (Khatri et al., Reference Khatri, Marziali, Tchernikov and Shepherd2014; Matsumoto et al., Reference Matsumoto, Sutoh, Asano, Seki, Urao, Yokoo, Takanashi, Yoshida, Tanaka and Noguchi2018), and preliminary evidence suggests that it is equally effective in reducing depressive symptoms as in-person CBT (Berryhill et al., Reference Berryhill, Culmer, Williams, Halli-Tierney, Betancourt, Roberts and King2019; Lamb et al., Reference Lamb, Pachana and Dissanayaka2019; Luo et al., Reference Luo, Sanger, Singhal, Pattrick, Shams, Shahid, Hoang, Schmidt, Lee and Haber2020). Additionally, treatment attendance, drop-out and satisfaction have been shown to be comparable between videoconference and in-person CBT for depressive disorders (Luo et al., Reference Luo, Sanger, Singhal, Pattrick, Shams, Shahid, Hoang, Schmidt, Lee and Haber2020; Nelson et al., Reference Nelson, Barnard and Cain2003; Stubbings et al., Reference Stubbings, Rees, Roberts and Kane2013).
Although promising evidence suggests that CBT delivered via videoconference demonstrates comparable outcomes as CBT delivered in-person, much of this work has focused on individual rather than group CBT (Backhaus et al., Reference Backhaus, Agha, Maglione, Repp, Ross, Zuest, Rice-Thorp, Lohr and Thorp2012; Lamb et al., Reference Lamb, Pachana and Dissanayaka2019). Yet, group therapy offered via videoconference has the potential to be a cost-effective and resource-efficient way of treating depression (e.g. more patients can be seen concurrently with fewer therapists and without the need for more physical space). Group therapy also provides unique therapeutic benefits to patients beyond those of individual therapy, such as receiving social support from peers, a sense of belonging, and learning from others who have had similar experiences (Whitfield, Reference Whitfield2010; Yalom and Leszcz, Reference Yalom and Leszcz2005). Although studies suggest that group CBT for depressive disorders is equally effective as individual CBT through an in-person format (Cuijpers et al., Reference Cuijpers, Noma, Karyotaki, Cipriani and Furukawa2019; Huntley et al., Reference Huntley, Araya and Salisbury2012; McDermut et al., Reference McDermut, Miller and Brown2001), research comparing group CBT delivered via videoconference versus in-person is scarce. One prior study that compared videoconference to in-person group CBT found that these treatment modalities showed similar effectiveness, but this study examined a small (n=18), mixed diagnostic sample of out-patients (i.e. primary diagnosis of a mood, anxiety, or adjustment disorder; Khatri et al., Reference Khatri, Marziali, Tchernikov and Shepherd2014). Thus, further research is needed to establish the effectiveness of videoconference group CBT for depressive disorders.
The goal of the current study was to examine whether group CBT administered via videoconference demonstrates comparable clinical outcomes as treatment provided in-person. We compared these treatments in a tertiary care specialist mood disorders clinic that, like many other mental health services during the COVID-19 pandemic, rapidly shifted from providing treatment in-person to videoconference. Using a non-randomized study design, data on clinical outcomes, treatment attendance, drop-out, and satisfaction were collected from groups delivered through videoconference during the pandemic and compared to respective data from in-person groups collected prior to the pandemic. Consistent with prior research (Khatri et al., Reference Khatri, Marziali, Tchernikov and Shepherd2014; Luo et al., Reference Luo, Sanger, Singhal, Pattrick, Shams, Shahid, Hoang, Schmidt, Lee and Haber2020; Nelson et al., Reference Nelson, Barnard and Cain2003; Stubbings et al., Reference Stubbings, Rees, Roberts and Kane2013), we hypothesized that group CBT delivered via videoconference would show similar outcomes in terms of symptom change, treatment attendance, drop-out, and satisfaction as group CBT delivered in-person. Additionally, we conducted exploratory analyses to examine whether symptom change between videoconference and in-person group CBT was robust to patient-level characteristics, including age, sex, psychiatric co-morbidities, and anti-depressant medication use.
Method
Participants
Participants were out-patients of a tertiary care mood disorders clinic in a public hospital in Hamilton, Ontario, who consented to the inclusion of their demographic and clinical information in a program evaluation database. Participants were referred to treatment through either the mood disorder program, a different specialty clinic within the hospital or by their community primary care physician. Inclusion criteria for research participation paralleled the eligibility criteria for treatment, including age 18 or older, a current Diagnostic and Statistical Manual of Mental Disorders, fifth edition (DSM-5) mood disorder diagnosis, and English language proficiency. Exclusion criteria included other more pressing clinical issues (e.g. another disorder causing more distress/impairment, high suicide risk, including strong intent or plan to die, and/or severe substance use). For the purposes of the current analyses, we also excluded participants who had a current diagnosis of bipolar disorder (I or II), as well as participants who did not complete the pre-treatment questionnaires. Based on these criteria, final samples involved 255 in-person and 113 videoconference participants. Of these participants, 110 in-person and 36 videoconference participants completed the post-treatment questionnaires. A participant flow chart is presented in the Supplementary material (see Fig. S1). The Supplementary material also presents the results of a series of independent t-tests and chi-square tests which compare demographic and pre-treatment variables between participants who either completed (110 in-person; 36 videoconference) or did not complete the post-treatment questionnaires (145 in-person; 77 videoconference) within each treatment modality.
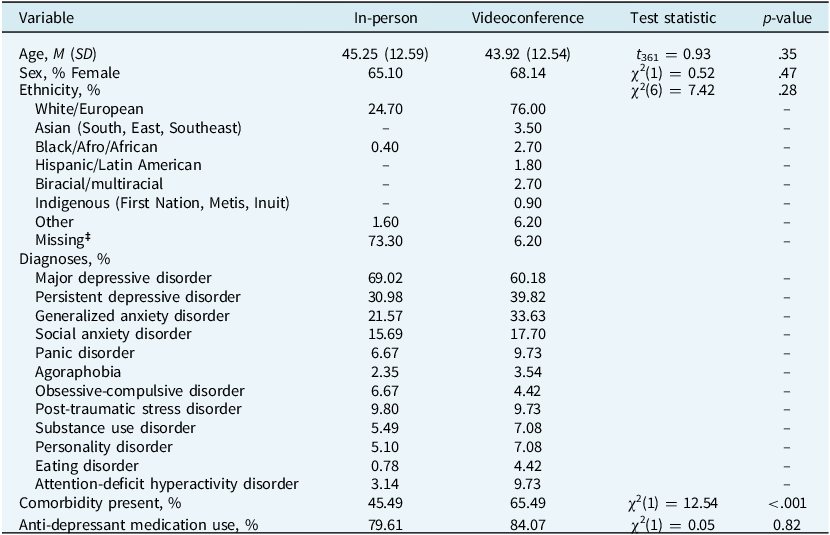
Participants’ mean age was 44.83 years (SD=12.57, range=18–72). The majority were women (n=243, 66%). All participants had a primary diagnosis of major depressive disorder or persistent depressive disorder as determined by semi-structured diagnostic interview conducted by a psychologist or psychiatrist at the mood disorders clinic. One-hundred and ninety participants (52%) had at least one co-morbid disorder, most commonly an anxiety disorder. Table 1 presents demographic and clinical characteristics of participants who were enrolled in in-person or videoconference group CBT.
Descriptive statistics of participants’ demographic and clinical characteristics for those who completed group cognitive-behavioural therapy (CBT) either in-person (n = 255) or via videoconference (n = 113)

Note: DASS-21 = Depression, Anxiety and Stress Scales-21. ‡ Ethnicity data were missing for 187 in-person and 7 videoconference participants.
Treatment
In-person and videoconference CBT were facilitated using a 14-session manualized CBT group protocol for depression. The treatment manual was developed at our clinic based on existing widely used CBT protocols (Beck et al., Reference Beck, Rush, Shaw and Emery1979; Beck, Reference Beck1995; Burns, Reference Burns1999; Greenberger and Padesky, Reference Greenberger and Padesky2016). The same manuals were used for both treatment modalities. Each session followed a consistent structure, beginning with setting the agenda and a check-in, during which participants shared one positive experience and one thing they were grateful for from the past week. The group then reviewed any feedback from the previous session, followed by a discussion of homework. New learning was introduced, and a 15-minute break was provided halfway through. The session concluded with assigning homework for the following week. Session content over the 14-week treatment protocol included psychoeducation (session 1), behavioural activation (sessions 2–3), cognitive restructuring (sessions 4–7), review (session 8), problem-solving and acceptance (session 9), assertiveness training (session 10), behavioural experiments (session 11), managing rumination and procrastination (session 12), gratitude and acts of kindness (session 13), and relapse prevention (session 14; see Table S1 in the Supplementary material for more details).
To prepare for the delivery of the videoconference groups, our clinic consulted other teams with experience in videoconferencing treatment, reviewed the literature on virtual treatments, and held meetings to discuss procedures for risk management. For both in-person and videoconference modalities, 2-hour weekly group sessions were co-facilitated by two clinicians: a registered clinical psychologist and a registered social worker. In some groups, a clinical learner (e.g. a Master’s- or PhD-level student in psychology, psychiatry, or social work) also participated as a third facilitator. The same group of experienced clinicians, consisting of four social workers and three psychologists working in the clinic, rotated through facilitating the groups across both modalities. The mean number of participants in each group was 12.08 (SD=1.89, range=7–15) for in-person and 10.21 (SD=1.90, range=6–13) for videoconference treatment.
In-person groups were conducted in conference rooms at the clinic, with participants seated around a large table. A whiteboard was used to explain and deliver some of the treatment content. Videoconference groups were conducted through a secure, Health Insurance Portability and Accountability Act (HIPAA)-compliant teleconferencing platform (Zoom Video Communications, Inc.), which participants accessed through their electronic medical record. Participants attended the videoconference sessions from their home or other private setting. At the start of the videoconference group, participants were provided with instructions on how to use the videoconference platform as well as guidelines to ensure appropriate decorum and participation using the platform. To approximate face-to-face treatment, participants were instructed to keep their camera on with their face showing and to turn on ‘gallery view’ so that therapists and other group members would be seen simultaneously. Videoconference sessions were provided in real-time. A screen share function was used to display a virtual whiteboard on which homework was presented and reviewed; content from the treatment manual was also screen shared.
Measures
Chart review and data extraction
Participants’ demographic and clinical characteristics were collected from the pre-treatment questionnaire or were extracted from referral, assessment or consultation notes located in their electronic medical records. The following information was extracted from medical records: participants’ age; sex; ethnicity; current psychiatric diagnosis (or diagnoses) determined by a semi-structured psychodiagnostic interview; as well as use of anti-depressant medication prior to treatment. Treatment attendance (possible range=1–14) was also extracted from medical records. Demographic questions (i.e. age, sex, ethnicity) were not included in the pre-treatment questionnaire for in-person group CBT participants; this information was extracted from these participants’ medical charts. Ethnicity data were missing for 187 in-person group CBT participants (73% of the sample) because this information was not recorded in their medical charts. Additionally, ethnicity data were missing for seven videoconference group CBT participants (6% of the sample) because these individuals selected ‘prefer not to answer’ to this question on the pre-treatment questionnaire.
Diagnostic status
Prior to treatment, all participants completed the Diagnostic Assessment Research Tool (DART; McCabe et al., Reference McCabe, Milosevic, Rowa, Shnaider, Pawluk and Antony2017) with a psychiatrist or psychologist at the mood disorders clinic. The DART is a semi-structured diagnostic interview with a modular design that assesses a wide range of mental disorders based on the DSM-5 (American Psychiatric Association, 2013), including anxiety disorders, depressive disorders, bipolar and related disorders, obsessive compulsive and related disorders, trauma- and stressor-related disorders, substance-related and addictive disorders, feeding and eating disorders, and somatic symptom and related disorders. Each module consists of mandatory criterion-based questions as well as optional clarifying questions to ensure diagnostic accuracy. All participants enrolled in treatment met criteria for a current unipolar mood disorder (i.e. major depressive disorder and/or persistent depressive disorder). The DART has demonstrated excellent construct validity, as well as good convergent and discriminant validity (Schneider et al., Reference Schneider, Pawluk, Milosevic, Shnaider, Rowa, Antony, Musielak and McCabe2022).
Self-report questionnaires
At pre- and post-treatment, participants completed the short-version of the Depression Anxiety Stress Scale (DASS-21; Henry and Crawford, Reference Henry and Crawford2005; Lovibond and Lovibond, Reference Lovibond and Lovibond1995). The DASS-21 is a 21-item self-report measure that assesses symptoms of depression (e.g. dysphoria, hopelessness, lack of interest/involvement, and anhedonia), anxiety (e.g. autonomic arousal, anxious affect, and worry), and stress (i.e. nervous tension, difficulty relaxing, and irritability). Participants rated the extent to which they experienced each symptom over the past week on a 4-point scale, ranging from 0 (not at all) to 3 (most of the time), with higher scores indicating increased depression, anxiety, and stress symptoms. Subscale scores were calculated by summing the scores for each of the subscale’s seven items, and then doubling them (i.e. total scores for each subscale range can from 0 to 42). In the current study, internal consistency reliability was good for the depression (pre-treatment α=.89; post-treatment α=.94), anxiety (pre-treatment α=.84; post-treatment α=.89) and stress subscales (pre-treatment α=.84; post-treatment α=.91).
At post-treatment, participants answered the following statement to assess satisfaction with treatment: ‘How satisfied were you with the overall treatment experience?’ rated on a 7-point scale, ranging from 1 (not at all) to 7 (very much so). Additionally, a subset of participants who completed videoconference treatment (n=26) rated seven additional items, which specifically assessed their satisfaction with the videoconference treatment experience on a 7-point scale, ranging from 1 (not at all) to 7 (very much so).
Attendance and drop-out
Group therapists recorded weekly treatment attendance in participants’ medical records. Attendance could range from 1 to 14 sessions. Across both treatments, the first 13 weekly sessions consisted of the key components of CBT and the 14th session involved reviewing treatment components and developing a relapse prevention plan. Consistent with prior research (Heatherington et al., Reference Heatherington, Harrington, Harrington, Niemeyer, Weinberg and Friedlander2014; Oei and Kazmierczak, Reference Oei and Kazmierczak1997; Pfund et al., Reference Pfund, Peter, McAfee, Ginley, Whelan and Meyers2021), drop-out was defined as failure to complete a full treatment protocol (i.e. attending fewer than 13 sessions).
Procedure
Participants were referred to group CBT for depression if they had a primary diagnosis of a unipolar depressive disorder. Those who were enrolled in group CBT between June 2017 to December 2019 (i.e. pre-pandemic) received in-person treatment, and those who were enrolled between November 2020 to November 2021 (i.e. during pandemic) received videoconference treatment. All in-person groups were completed by 5 March 2020, before the province of Ontario declared a public health emergency and implemented physical distancing measures on 17 March 2020, at which point our hospital ceased in-person services.
Participants who attended in-person treatment completed pre- and post-treatment self-report measures by paper-and-pencil. Participants were allotted time to complete these questionnaires before the first treatment session and after the last treatment session. Participants who attended videoconference treatment completed pre- and post-treatment self-report measures electronically via Research Electronic Data Capture (REDCap) software (Harris et al., Reference Harris, Taylor, Thielke, Payne, Gonzalez and Conde2009). They received email links and were asked to complete the measures before the first treatment session, and after the last treatment session.
Statistical analyses
Statistical analyses were conducted using SPSS (version 28; IBM Corp., Armonk, NY) and R (version 4.1.0; R Core Team, 2021). To examine whether our data were missing completely at random (MCAR) within each treatment modality, we conducted Little’s MCAR test (Little, Reference Little1988). The results of these analyses are provided in the Supplementary material. Pearson’s chi-square and independent t-tests were conducted to examine whether participants’ age, sex (0=male, 1=female), ethnicity, psychiatric co-morbidities (0=co-morbidity absent; 1=co-morbidity present), anti-depressant medication use (0=anti-depressant medication absent; 1=anti-depressant medication present) differed between treatment modalities.
Subsequently, to examine the effects of modality (in-person vs videoconference) and time (pre- vs post-treatment) on depression, anxiety, and stress symptoms, we conducted three repeated-measures two-level multi-level models using the lme4 package (Bates et al., Reference Bates, Mächler, Bolker and Walker2015). We structured our models such that DASS-21 surveys (measured at pre- and post-treatment) were nested within participants. Separate models were run for each of the three symptom measures (i.e. depression, anxiety, and stress). Each model included a random intercept for each participant, fixed effects for modality (in-person=0, videoconference=1) and time (pre-treatment=0, post-treatment=1) as well as cross-level interaction term between modality and time.
To examine whether the effects of modality and time on depression, anxiety and stress symptoms were robust to patient-level demographic and clinical characteristics, we repeated the same three models described above and entered participants’ age, sex (0=male, 1=female), co-morbidities (0=co-morbidity absent; 1=co-morbidity present) and anti-depressant medication use (0=anti-depressant medication absent; 1=anti-depressant medication present) as covariates. An intent-to-treat approach was used for all models to maximize sample size and enhance external validity. All models were estimated using restricted maximum likelihood (REML) with unstructured variance-covariance matrices. There were no convergence issues.
Next, we conducted an independent t-test and Pearson’s chi-square to examine whether treatment attendance and drop-out rates differed between treatment modalities. Finally, to compare post-treatment satisfaction ratings between treatment modalities, we conducted a Mann–Whitney U-test. All statistical tests were two-tailed and had a significance level of p<.05. Effect sizes were estimated by calculating standardized beta coefficients (β) and Cohen’s d. The magnitude of effect sizes was defined according to Cohen (Reference Cohen1988) criteria: 0.20 (small), .50 (medium) and .80 (large).
Results
Descriptive statistics
As indicated in Table 1, participants’ age (t 361=0.93, p>.05, d=0.11, 95% CI [–0.12, 0.33]), sex (χ2(1)=0.52, p>.05), ethnicity (χ2(6)=7.42, p>.05), and anti-depressant medication use (χ2(1)=0.05, p>.05) did not significantly differ between modalities. However, participants who received videoconference group CBT were more likely to have at least one co-morbid disorder than participants who received in-person group CBT (χ2(1)=12.54, p<.001). Table S2 in the Supplementary material presents the observed means of pre- and post-treatment symptoms for both the intent-to-treat and treatment completer samples (i.e. attended at least 13 sessions).
Effects of modality and time on depression, anxiety, and stress symptoms
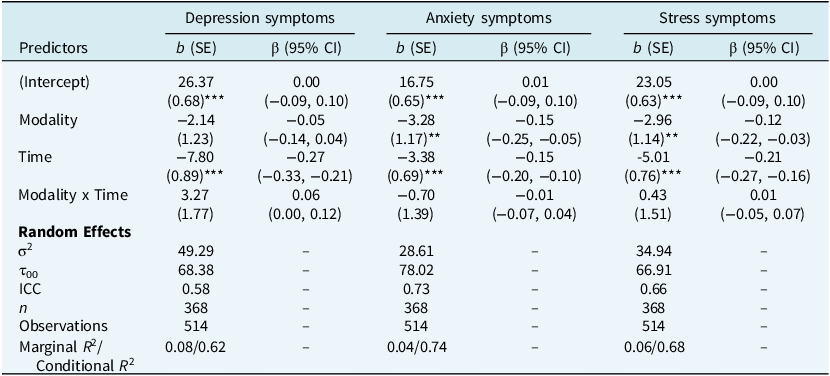
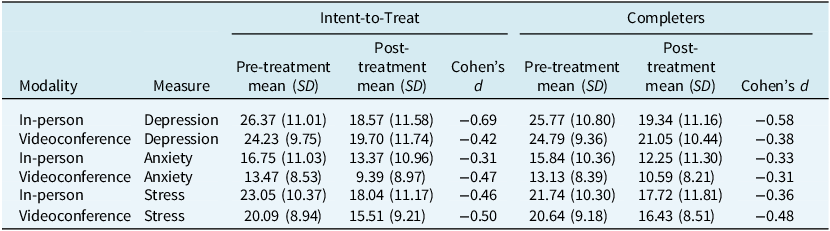
Results of the multi-level model analyses examining the effects of modality (in-person vs videoconference) and time (pre-treatment vs post-treatment) on depression, anxiety, and stress symptoms are presented in Table 2 and Fig. 1. As indicated in Table 2, we observed significant main effects of time on all three DASS-21 subscales, such that depression, anxiety, and stress symptoms decreased from pre- to post-treatment across both in-person and videoconference treatments. Additionally, there were significant main effects of modality on anxiety and stress symptoms, indicating that participants who received in-person treatment reported greater symptoms of anxiety and stress across pre- and post-treatment time-points compared to participants who received videoconference treatment. We did not observe significant interactions between modality and time on all three DASS-21 subscales, indicating that in-person and videoconference group CBT did not have differential effects on depression, anxiety, and stress symptoms from pre- to post-treatment. Table 3 presents estimated means of pre- and post-treatment symptoms from the linear mixed effects models, along with within-group effect sizes (Cohen’s d), for both the intent-to-treat and treatment completer samples.
Results from the multilevel model analyses examining the effects of modality (in-person n = 255 vs videoconference n =113) and time (pre-treatment vs post-treatment) on depression, anxiety, and stress symptoms

Note: Modality: 0 = in-person, 1 = videoconference; Time: 0 = pre-treatment, 1 = post-treatment; 95% CI = 95% confidence interval. ***p< .001; **p< .01; *p< .05.
Plots depicting the effects of modality (in-person n=255 vs videoconference n=113) and time (pre-treatment vs post-treatment) on depression, anxiety, and stress symptoms. Pre-Tx = pre-treatment; Post-Tx = post-treatment; shaded areas represent 95% confidence intervals.

Estimated means, observed standard deviations, and within-group effect sizes for pre- and post-treatment depression, anxiety, and stress symptoms in the intent-to-treat and treatment completer samples

Note: Cohen’s d was calculated based on estimated means from the linear mixed effects-models and the pooled standard deviation from the observed means.
To examine whether the effects of modality and time on depression, anxiety and stress symptoms were robust to demographic and clinical individual difference factors, we repeated the same three models described above and entered participants’ age, sex, co-morbidities, and anti-depressant medication use as covariates (see Table S3 in the Supplementary material). The results of these analyses were very similar to the results described above.
To assess the robustness of our findings, we conducted three sensitivity analyses. First, we re-ran our models including only treatment completers (i.e. attended at least 13 sessions) within the in-person (n=77) and videoconference groups (n=53; see Table S4 in the Supplementary material). Second, given the low completion rates of post-treatment symptom questionnaires (in-person: 43%; videoconference: 32%), we examined the potential influence of missing data by re-running our models with only participants who completed both pre- and post-treatment symptom measures (see Table S5 in the Supplementary material). Third, since the mean number of participants per group was significantly higher for in-person CBT (M=12.08) than videoconference CBT (M=10.21; t 356=8.62, p<.001), we re-ran our models with group size included as a covariate (see Table S6 in the Supplementary material). The results of these sensitivity analyses were consistent with our main findings.
Additionally, in an exploratory analysis, we compared post-treatment questionnaire non-completion rates between treatment modalities. Participants in the videoconference group were significantly less likely to complete these questionnaires than those in the in-person group (in-person: 57% non-completion vs videoconference: 68% non-completion; χ2(1)=4.16, p=.04).
Effects of modality on treatment attendance and drop-out
Results of the independent t-test comparing attendance between treatment modalities indicated that treatment attendance was significantly higher for participants who completed videoconference (M=10.43, SD=4.00, range=1–14) compared to in-person group CBT (M=9.07, SD=4.20, range=1–14; t 366=2.91, p<.01, d=0.33, 95% CI [0.11, 0.55]). Moreover, results of the Pearson’s chi-square test comparing drop-out between treatment modalities indicated that drop-out was lower for participants who completed videoconference (60 participants or 53% of the sample dropped out) compared to in-person group CBT (178 participants or 70% of the sample dropped out; χ2(1)=9.57, p<.01). We then conducted exploratory analyses to examine whether demographic and clinical factors were associated with drop-out within each treatment modality. As indicated in the Supplementary material, within the in-person group, participant sex was a significant predictor of drop-out (χ2(1)=4.57, p<.05), such that women (125 participants or 70% of the in-person sample that dropped out) were more likely to drop out than men (53 or 30% of the in-person sample that dropped out).
In the Supplementary material, we report the results of a sensitivity analysis comparing drop-out rates between in-person and videoconference group CBT using a lower session cut-off (i.e. attended fewer than seven sessions). Additionally, we report correlations examining associations between group size and treatment attendance, drop-out, and satisfaction within each modality; none was statistically significant (p>.05).
Effect of modality on treatment satisfaction
Post-treatment satisfaction ratings did not significantly differ between participants who completed in-person (M=6.07, SD=1.05) compared to videoconference group CBT (M=6.07, SD=0.92; Z=–0.27, p>.05). Box plots depicting responses from the subset of participants (n=26) who completed seven additional items that assessed their satisfaction with the videoconference treatment experience are presented in Fig. 2. As indicated in Fig. 2, mean ratings were approximately equal to or greater than a score of 5 (i.e. scores on each item could range from 1 (not at all) to 7 (very much so) on each item), indicating that the videoconference group was generally experienced positively.
Box plots depicting participants’ satisfaction ratings with group cognitive behavioural therapy (CBT) delivered via videoconference (n=26). Each item was rated on a 7-point scale, ranging from 1 (not at all) to 7 (very much so). The whiskers represent the maximum and minimum, the grey line represents the median, and the black ‘×’ represents the mean.

Discussion
The present study compared outcomes of in-person and videoconference group CBT for depressive disorders. Consistent with our hypotheses, decreases in depression, anxiety, and stress symptoms from pre- to post-treatment did not significantly differ between videoconference and in-person group CBT. These associations held even when adjusting for participants’ age, sex, co-morbidities, and anti-depressant medication use. Moreover, post-treatment satisfaction did not significantly differ between in-person and videoconference group CBT, and videoconference-specific satisfaction ratings suggest that this modality was feasible and well tolerated by participants. Combined, these data suggest that videoconference group CBT demonstrates similar symptom and satisfaction outcomes as in-person group CBT for depressive disorders.
These results are consistent with prior studies that have compared videoconference and in-person CBT for depression within an individual format (Luxton et al., Reference Luxton, Pruitt, Wagner, Smolenski, Jenkins-Guarnieri and Gahm2016; Nelson et al., Reference Nelson, Barnard and Cain2003; Stubbings et al., Reference Stubbings, Rees, Roberts and Kane2013) and extends this work by demonstrating that these treatment modalities are associated with similar reductions in depressive symptoms as well as high levels of patient satisfaction within a group format. The small-to-medium effect sizes we observed in symptom changes over time are also in line with previous research (Karyotaki et al., Reference Karyotaki, Efthimiou, Miguel, genannt Bermpohl, Furukawa, Cuijpers, Riper, Patel, Mira and Gemmil2021; Okumura and Ichikura, Reference Okumura and Ichikura2014; Strachan et al., Reference Strachan, Gros, Ruggiero, Lejuez and Acierno2012; Stubbings et al., Reference Stubbings, Rees, Roberts and Kane2013), as are the small and non-significant effect sizes we observed between treatment modalities on symptom measures (Giovanetti et al., Reference Giovanetti, Punt, Nelson and Ilardi2022; Milosevic et al., Reference Milosevic, Cameron, Milanovic, McCabe and Rowa2022; Stubbings et al., Reference Stubbings, Rees, Roberts and Kane2013).
Additionally, videoconference group CBT occurred during the COVID-19 pandemic, a period of high stress and uncertainty in which we might anticipate poorer depression treatment outcomes relative to the pre-pandemic in-person CBT group. This was not the case in our study. Given that group therapy delivered via videoconference reduces access-to-care barriers and offers the additional benefits of group treatment (e.g. resource efficiency, social support from peers, a sense of belonging; Luo et al., Reference Luo, Sanger, Singhal, Pattrick, Shams, Shahid, Hoang, Schmidt, Lee and Haber2020; Madigan et al., Reference Madigan, Racine, Cooke and Korczak2021; Richardson et al., Reference Richardson, Frueh, Grubaugh, Egede and Elhai2009), our data suggest that videoconference group CBT is a promising and effective modality to provide depressive disorder treatment during and beyond the pandemic.
Interestingly, videoconference group CBT was associated with higher treatment attendance and lower drop-out rates compared to in-person group CBT. Although inconsistent with the results of some previous studies (Luo et al., Reference Luo, Sanger, Singhal, Pattrick, Shams, Shahid, Hoang, Schmidt, Lee and Haber2020; Nelson et al., Reference Nelson, Barnard and Cain2003; Stubbings et al., Reference Stubbings, Rees, Roberts and Kane2013), the data suggest that convenience factors associated with videoconferencing, such as remote access to treatment in one’s home and reduced or eliminated commuting time and/or transportation costs, may improve group CBT attendance and retention. Alternatively, the higher attendance and lower drop-out rates for videoconference participants could be attributed to the pandemic, during which alternative treatment options, like in-person therapy, were limited or unavailable. As treatment modality is confounded with the presence or absence of the pandemic in our study, future research should compare group CBT delivered via videoconference and in-person outside the pandemic context to explore these possibilities further.
Although our results support the effectiveness of videoconference group CBT for reducing depressive symptoms, this modality may pose challenges for both patients and therapists. These challenges include privacy and confidentiality concerns, increased potential for environmental and/or online distractions during sessions, decreased connection with other group members, as well as lack of access to a reliable internet connection and required technology (Bean et al., Reference Bean, Aurora, Maddox, Mekota and Updegraff2022; Madigan et al., Reference Madigan, Racine, Cooke and Korczak2021). Moreover, therapists require training to develop competencies in delivering treatment via videoconference, including remotely managing crisis situations (e.g. suicide and homicide risk), ensuring that groups are accessed in a secure manner, and are unable to provide treatment outside of their licensing province or state (Madigan et al., Reference Madigan, Racine, Cooke and Korczak2021; Maheu et al., Reference Maheu, Wright, Neufeld, Drude, Hilty, Baker and Callan2021; Martin et al., Reference Martin, Millán and Campbell2020). It is important to note here, however, that videoconference participants reported high levels of satisfaction with developing connections with other group members, accessing and using videoconference technology and with the protocols and procedures for maintaining confidentiality and privacy (see Fig. 2), suggesting that participants in our sample did not encounter some of the challenges associated with receiving treatment via videoconference. Although our clinic rapidly adapted group CBT to a virtual format during the pandemic to ensure continued service delivery, our team took important steps to optimize treatment access and engagement. These included researching and preparing videoconference-specific adaptations, where relevant, and providing extensive support to help patients become comfortable with the technology. Nonetheless, future research will be needed to better understand the challenges of videoconference treatment for both patients and therapists, as well as work that examines potential strategies to overcome these barriers.
Strengths of the present study include its comparison of the effects of group CBT delivered in-person versus videoconference on multiple clinical outcomes in a relatively large sample of patients with depressive disorders. Moreover, we show that our results are robust to patient-level demographic and clinical factors, providing evidence to support the use of videoconference group CBT for treating depressive disorders across diverse patient populations. Nonetheless, the current study has several limitations that inform directions for future research. First, participants who received videoconference group CBT were primarily White/European, and ethnicity data was missing for 73% of the in-person group CBT sample. Given that individuals with minority racial-ethnic identities are especially vulnerable to depressive disorders due to existing structural inequities (Bailey et al., Reference Bailey, Mokonogho and Kumar2019; Marrone, Reference Marrone2007), future studies with careful assessment of race and ethnicity will be needed to examine whether the results presented here generalize to these populations.
Second, the low completion rates of post-treatment symptom questionnaires in both treatment modalities may limit the generalizability of our findings (i.e. 145 and 77 participants did not complete post-treatment measures in the in-person and videoconference groups, respectively). These low completion rates were due to participants choosing not to complete the measure rather than non-attendance, as all participants were sent the post-treatment questionnaires regardless of whether they completed the full treatment or dropped out early. This attrition rate is comparable to similar group CBT studies (McEvoy et al., Reference McEvoy, Burgess and Nathan2013; Spek et al., Reference Spek, Nyklíček, Smits, Cuijpers, Riper, Keyzer and Pop2007), and our post-treatment questionnaire sample sizes exceed those of prior studies (e.g. n values range from 8 to 14 per group; Khatri et al., Reference Khatri, Marziali, Tchernikov and Shepherd2014; Nelson et al., Reference Nelson, Barnard and Cain2003; Stubbings et al., Reference Stubbings, Rees, Roberts and Kane2013). Moreover, our analyses of selection bias indicated that demographic and pre-treatment variables did not influence questionnaire completion. Although completion rates were low across both modalities, exploratory analyses showed that participants in the videoconference group were less likely to complete post-treatment questionnaires compared to those in the in-person group. Completion of pre- and post-treatment questionnaires was voluntary, and many videoconference participants who did not complete them still attended most sessions. Of the 77 non-completers, the average number of sessions attended was 9.51, with a third (n=27) completing the full treatment (i.e. attending 13 or more sessions). Thus, while non-completion of post-treatment questionnaires represents some attrition, it does not necessarily indicate disengagement from treatment. Lower completion rates in the videoconference group may be due to pandemic-related stress, screen fatigue, or differences in how the questionnaires were administered. For instance, in-person participants completed their questionnaires at the clinic immediately after their final session, whereas videoconference participants had to complete them remotely and on their own time, which may have reduced adherence. Future studies should examine factors influencing non-completion in both modalities to improve data retention.
Third, the methods used to collect the pre- and post-treatment symptom measures differed between the two treatment modalities (e.g. in-person participants completed paper-and-pencil questionnaires at the clinic, while videoconference participants completed them via an online survey), which may have influenced the pattern of results observed. Additionally, neither group underwent a post-treatment diagnostic assessment, meaning our data cannot speak to whether the two modalities differed in their effectiveness at achieving remission from depression. Future work should consider employing standardized procedures for assessing pre- and post-treatment symptoms across modalities as well as incorporating post-treatment diagnostic assessments to complement self-reported symptom changes.
Fourth, drop-out rates for videoconference and in-person treatment modalities were high (i.e. 53% of videoconference participants and 70% of in-person participants did not complete a full treatment protocol). These drop-out rates are comparable to those reported in other CBT studies of depression (Fernandez et al., Reference Fernandez, Salem, Swift and Ramtahal2015; Hans and Hiller, Reference Hans and Hiller2013), and 71% of in-person and 82% of videoconference participants attended at least seven of the 14 weekly treatment sessions (i.e. half of the treatment). Additionally, most demographic and clinical factors, including pre-treatment depression symptoms, were not significantly associated with drop-out within each treatment modality, indicating that these factors likely did not contribute to the drop-out rates we observed. We would note here, however, that women were more likely to drop out of in-person group CBT than men, possibly because women may have faced more barriers associated with completing in-person treatment (e.g. difficulties with taking time off work or securing childcare to attend treatment on a weekly basis). In contrast, drop-out from videoconference group CBT did not differ between men and women, suggesting that depressive disorder treatment provided by videoconference may be more accessible to women. Future research is needed to identify possible barriers to completing depressive disorder group treatment among women and to examine factors that might support women’s increased retention in videoconference treatment.
Fifth, because the same group of clinicians facilitated both treatment modalities, participants in the videoconference group CBT received treatment from clinicians with more clinical experience, as this modality was implemented later – during the COVID-19 pandemic – than the in-person group CBT. As we do not have detailed records of each clinician’s years of practice prior to joining our clinic, we are unable to assess the potential impact of clinician experience on our findings. Nonetheless, having the same clinicians facilitate both modalities helps reduce any bias that can affect treatment outcomes due to differences between therapists. Future research comparing in-person and videoconference group treatment should consider tracking clinician experience and accounting for its potential influence on treatment outcomes.
Finally, participants were not randomized to receive in-person or videoconference treatment, and so our results are preliminary and should be interpreted with caution. Future studies will be needed to determine whether our findings replicate when using a randomized treatment study design and larger sample sizes.
In summary, the results of the present study replicate previous work indicating that videoconference and in-person CBT demonstrate similar symptom change and satisfaction outcomes (Luxton et al., Reference Luxton, Pruitt, Wagner, Smolenski, Jenkins-Guarnieri and Gahm2016; Nelson et al., Reference Nelson, Barnard and Cain2003; Stubbings et al., Reference Stubbings, Rees, Roberts and Kane2013) and provide new evidence that group CBT for depressive disorders can be successfully delivered via videoconference, even during a pandemic. Future longitudinal research is needed to examine outcomes of videoconference group CBT, as well as other evidence-based therapies for depressive disorders, over time and in diverse patient populations. Ultimately, this work will be needed to support videoconference group CBT as a viable alternative to in-person treatment, which may, in turn, enhance the accessibility and equity of mental health services for individuals with depressive disorders.
Supplementary material
To view supplementary material for this article, please visit https://doi.org/10.1017/S1352465825100957
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request. The data are not publicly available due to privacy considerations of the patients who participated.
Acknowledgements
None.
Author contributions
Aislinn Sandre: Conceptualization (lead), Formal analysis (lead), Investigation (supporting), Writing - original draft (lead), Writing - review & editing (equal); Vraj Shah: Investigation (supporting), Writing - review & editing (equal); Anastasiya Slyepchenko: Formal analysis (supporting), Writing - review & editing (equal); Brenda Key: Writing - review & editing (equal); Sharon Simons: Project administration (supporting), Writing - review & editing (equal); Julie Sgambato: Project administration (lead), Writing - review & editing (equal); Caitlin Davey: Conceptualization (supporting), Investigation (lead), Supervision (lead), Writing - original draft (supporting), Writing - review & editing (equal).
Financial support
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Competing interests
The authors declare none.
Ethical standards
The Hamilton Integrated Research Ethics Board provided permission for participant data to be collected and published for research purposes and approved all study procedures (approval number: 14157-C). All methods followed the Declaration of Helsinki.





Comments
No Comments have been published for this article.