

1. Introduction
Mass personalisation (MP) has become a relevant direction in product development because it allows individually adapted products to be created within modelling workflows that remain compatible with serial production. Instead of relying on fixed product ranges, design teams increasingly use parametric and data-driven processes that allow each product instance to be adjusted while still following structured modelling procedures (Reference Ozdemir, Verlinden and CasciniOzdemir et al., 2022). Such processes depend on the ability of different roles to interpret information about form, constraints, and intended use in a consistent way. Within such digitally supported processes, computer-aided design (CAD) tools are used by different roles to express design requirements in geometric form and act as shared reference points during collaborative design sessions. Research on collaboration with CAD tools shows that shared models can support joint work but also introduce problems when several roles depend on the same representation. Studies of distributed and cloud-based collaboration report challenges in following changes in shared models and maintaining continuity when different roles join the process at different stages (Reference Cheng, Davis, Zhang, Zhou and OlechowskiCheng et al., 2023; Reference Marion, Olechowski and GuoMarion et al., 2021). These observations highlight that collaboration with CAD tools relies not only on technical infrastructures but also on how information is organised and presented so that it can be understood across different roles. In parallel, research has examined CAD models as shared reference points that link design-related information across roles. Prior studies show that models may include additional parameters and process-related data that connect decisions between roles (Reference Heikkinen and ElghHeikkinen & Elgh, 2017). Building on this, CAD models can function as boundary objects, meaning that they support participants with different expertise while still providing a shared representation through which assumptions and constraints can be communicated (Reference Panarotto, Bertoni and JohanssonPanarotto et al., 2019; Reference Star and GriesemerStar & Griesemer, 1989). This perspective emphasises that the CAD model supports collaboration by allowing each role to use and interpret the same representation without requiring identical domain knowledge. Despite these developments, little is known about how CAD models are prepared before collaboration begins. Existing research does not explain how professionals decide which input data, parameters, and representational elements are required to support boundary objects (CAD models), especially in contexts where each product instance is individually adapted. One of the few studies addressing this issue proposes a parametric procedure for structuring models for design meetings (Reference Khatib, Fleche, Mahdjoub, Bluntzer and SagotKhatib et al., 2016), but it does not examine how professionals themselves describe the information they require when using the model in collaborative design sessions. This study addresses this gap by examining how professionals describe the preparation and use of CAD models in collaborative design processes for MP products. The aim is to identify which forms of input data, representational elements, and role-dependent interactions are seen as necessary for shared interpretation and collaborative work. Insights from the analysis are subsequently used to inform the development of an initial parametric CAD model intended to support future collaborative design sessions.
2. Literature review
The increasing demand for MP has led to design methodologies that combine digital tools, structured input data, and parametric modelling. Reference Ozdemir, Verlinden and CasciniÖzdemir et al. (2022) describe MP through the concept of seed design, where parametric structures are created so that individual product instances can be generated from a shared setup. Their study emphasises product variability and the systematic use of user-specific information as key features of mass-personalised design. At the same time, they identify challenges that are directly relevant to CAD-based processes, including how individual requirements are translated into parametric inputs and the limited capabilities of existing CAD tools to accommodate such variability within stable modelling processes. Collaboration in digital processes has become increasingly central to these modelling practices. Studies of cloud-based CAD tools show that shared access to model data enables professionals to work together across locations but also introduces problems when several roles depend on the same representation. Reference Marion, Olechowski and GuoMarion et al. (2021) describe challenges that arise when professionals rely on shared models during distributed work, while Reference Cheng, Davis, Zhang, Zhou and OlechowskiCheng et al. (2023) report problems related to following changes in shared models and maintaining continuity when different roles enter the process at different moments. Complementing these findings, Reference Asuzu, Cheng and OlechowskiAsuzu et al. (2024) analysed a professional CAD team and showed that collaborative behaviour often emerges through informal role patterns, which influence how professionals interact with shared geometry during collaborative design sessions. These studies illustrate that collaboration with CAD tools is affected not only by the underlying tools but also by how model information is structured so that it can be interpreted by different roles. A related line of research focuses on the informational content embedded in CAD models. Reference Heikkinen, Johansson and ElghHeikkinen et al. (2018) showed that CAD models may integrate multidisciplinary information when extended beyond their initial geometric definition, including geometric constraints, material data, and production-related information. Their earlier empirical study (Reference Heikkinen and ElghHeikkinen & Elgh, 2017) demonstrated that such enriched models support information transfer and reuse across roles. At the same time, research shows that roles interpret CAD models in different ways depending on expertise. Reference Robertson, Walther and RadcliffeRobertson et al. (2007) found that users with varying backgrounds attend to distinct geometric cues, while Reference Ekströmer and WeverEkströmer and Wever (2019) reported that small changes in geometry can shift how roles understand constraints or intended function. These findings suggest that CAD models serve not only as geometric representations but also as shared reference points through which roles communicate assumptions, constraints, and expectations. In this sense, CAD models can function as boundary objects (Reference Panarotto, Bertoni and JohanssonPanarotto et al., 2019; Reference Star and GriesemerStar & Griesemer, 1989), enabling collaboration between roles with different expertise but rely on the same representation. Despite these insights, limited attention has been given to how CAD models are prepared before collaborative work begins. Al Reference Khatib, Fleche, Mahdjoub, Bluntzer and SagotKhatib et al. (2016) proposed one of the few structured approaches by mapping functional requirements into parametric elements to support design meetings. Reference Schweigert-Recksiek and LindemannSchweigert-Recksiek and Lindemann (2018) showed that problems arise when professionals do not share the same expectations about what the model should include, emphasising the need to understand how different roles define model content and purpose before collaboration. Existing research, however, rarely examines how professionals describe the preparation of CAD models or which input data, parameters, and representational elements they consider necessary for shared interpretation. This study therefore addresses this gap by analysing how professionals describe the preparation and use of CAD models in collaborative design sessions for MP products.
3. Methodology
The methodological approach was structured to address the aim of the study: understanding how professionals describe the preparation and use of CAD models in collaborative design processes for MP products. Because this aim requires empirical insight into decision-making before collaboration begins, the study needed a case in which CAD models are routinely adapted to individual requirements and used as boundary objects between different roles. The present study focuses on CAD model preparation and preparatory collaboration practices reported in interviews. Synchronous joint review sessions are planned as the next step for empirical evaluation of the prototype.
Dental implant prosthetics provide such a case. The design of each custom abutment depends on patient-specific geometry and clinically defined constraints. Custom abutments were therefore selected as the reference case for examining how professionals determine what information a CAD model must contain before it is used in collaborative work. An implant-abutment assembly consists of three interconnected parts: the implant placed in the bone, the abutment that attaches to it, the screw and the visible restoration such as a crown or a bridge. This structure is shown on the left side of Figure 1. The right side presents the abutment and highlights its segments that are relevant for CAD modelling. The abutment forms the link between the implant and the restoration, and its geometry must be adapted to the implant position and the surrounding soft tissue conditions (Reference Kosec, Gulin and ŠkecKosec et al., 2024a). While the implant connection follows a standardised system and platform defined by the manufacturer, the remaining segments require patient-specific shaping. The transgingival segment passes through the soft tissue and defines the gingival profile. The prosthetic connection segment supports the crown or bridge and must align with the intended morphology and angulation of the restoration.
Implant abutment assembly (left) and geometry of a custom abutment segment (right)

Figure 1 Long description
A diagram of an implant abutment assembly and the geometry of a custom abutment segment. Panel A: The left side of the diagram shows the implant abutment assembly. It includes a crown, abutment, screw, and implant. The crown is the visible part of the tooth, the abutment connects the crown to the implant, the screw secures the abutment to the implant, and the implant is embedded in the jawbone. Panel B: The right side of the diagram illustrates the geometry of a custom abutment segment. It is divided into several segments: the prosthetic connection segment, gingival profile, transgingival segment, and implant connection segment. Each segment has a specific role in the overall structure and function of the abutment.
To investigate this, semi-structured interviews were used to examine how professionals work with CAD tools, interpret boundary objects (CAD models), and describe information exchange within a shared digital process. Before the main data collection, a pilot interview was conducted with a professional who had experience in clinical work, laboratory work, and CAD, ensuring that the interview guide was understandable across both roles. The purpose of the pilot interview was to refine the question structure, check the clarity of dental terminology, and confirm the expected duration of the interviews. Ten interviews were carried out with professionals directly involved in the digital process: five dental technicians and five clinicians. These two groups were selected because they represent the complementary roles responsible for producing and evaluating custom abutments, and their perspectives provide insight into how CAD models are interpreted across laboratory and clinical tasks. Participants had between five and sixteen years of experience, with six women and four men in total. Each interview lasted between 45 and 90 minutes, resulting in approximately 12 hours of recorded material. The size of the sample aligns with previous qualitative studies that used semi-structured interviews to examine design-related work. Comparable research that analysed collaboration or CAD-related practices also relied on samples of a similar scale (e.g., Reference Asuzu, Cheng and OlechowskiAsuzu et al., 2024; Reference Cheng, Davis, Zhang, Zhou and OlechowskiCheng et al., 2023; Reference Joshi and ChakravarthyJoshi & Chakravarthy, 2021; Reference Schweigert-Recksiek and LindemannSchweigert-Recksiek & Lindemann, 2018). In this study, ten interviews provided sufficient depth and variation across roles to reach data saturation.
The interview structure consisted of five sections: background information, the steps involved in custom abutment design, interaction with CAD tools used in dental practice, communication regarding model-related information, and closing reflections. The questions were open-ended and invited participants to explain how they exchange information, describe their own actions, and interpret features within the CAD model. This aligns with the purpose of semi-structured interviews, which follow a predefined set of topics while allowing the interviewer to adjust wording and question order according to the flow of the conversation (Reference Robson and McCartanRobson & McCartan, 2011). Table 1 presents example questions from each section to illustrate the interview structure and the type of problems explored.
Overview of interview sections and example questions

The interviews were conducted individually, recorded with consent, and transcribed before being imported into NVivo 15 to support the organisation and coding of qualitative data. Thematic analysis was selected because it enables the systematic identification of patterned meaning across interviews without imposing predetermined analytical categories (Reference Braun and ClarkeBraun & Clarke, 2006). This made it suitable for exploring how professionals describe information needs, the way they work with CAD tools, and how they communicate through boundary objects. The analysis followed the six-phase procedure outlined by Reference Braun and ClarkeBraun and Clarke (2006). In the first phase, the researcher familiarised herself with the data through repeated reading of transcripts and early notetaking. In the second phase, initial codes were generated. Codes are short labels assigned to meaningful excerpts of text and capture ideas, actions, concerns, or interpretations expressed by the professionals. Coding was conducted systematically across the data and formed the basis for subsequent theme development. In the third phase, codes were examined for relationships and grouped into preliminary clusters that indicated broader analytical directions. The fourth phase involved reviewing these themes in relation to the coded segments and the data to ensure that each theme represented a coherent pattern. The fifth phase focused on defining and naming the themes by specifying their scope and analytical contribution. The final phase involved integrating the themes into a structured narrative that addressed the research question and connected the findings with relevant literature. NVivo 15 supported the organisation and retrieval of coded material, while the interpretative process remained researcher driven. This procedure resulted in three themes that reflect how clinicians and technicians understand the preparation and use of CAD models within collaborative design processes.
4. Results
Thematic analysis of the interview data revealed patterned ways in which participants described the information they require for modelling, the actions they perform when working with CAD tools, and the perspectives through which they evaluate a boundary object. Three themes concern the input data needed before modelling begins, the additional information that supports interaction with the model, and the role-specific ways in which the model is interpreted. These themes are presented in the following sections and together outline the aspects that participants considered essential when preparing CAD models for MP products.
4.1. Input data for CAD model
The first theme concerns the information that participants described as necessary before any modelling can begin. Both technicians and clinicians referred to this as the basis of the design task, since all later steps depend on how complete and reliable the initial data are. Participants consistently emphasised that their work begins with a set of digital scans obtained in the clinic (Figure 2). These include the scan of the working jaw (the jaw for which the abutment is being designed), the antagonist scan (the opposite jaw), the scan-body scan (that transfers implant position and orientation information into the digital tool) and the bite scan (that records the occlusal relationship).
Key intraoral scans for abutment design

In some cases, a pre-operative scan is also provided, which enables comparison with the current state and supports interpretation during early modelling decisions. Together, these inputs establish the digital starting point from which the model is later designed and checked. Participants repeatedly noted that incoming data vary across cases and that this variation requires verification before any parametric adjustments or design actions are made. Differences in scanning procedures, file formats, and ways in which the files are sent mean that technicians must inspect the scans after import, check alignment, and confirm that essential features of the scans are captured correctly. These include the visibility of the scan body, the clarity of the gingival margin, and the correct articulation between the working and antagonist jaws. Several technicians remarked that receiving scans of both jaws in occlusion is important for establishing contacts and vertical dimensions. When the data are complete and correctly aligned (i.e., when the scanned jaws match in occlusion and key surfaces correspond spatially), subsequent modelling steps were described as more predictable. When they are not, participants noted that additional clarification between clinicians and technicians is often needed to confirm missing or unclear information. In addition to the geometric scans, participants highlighted the importance of correctly identifying the implant type, platform, and connection configuration. These details define which digital and physical components correspond to each other and therefore influence the selection of compatible elements within the CAD tool. Some technicians also noted that they temporarily adjust visual contrast or apply colour differentiation within the imported scans to make anatomical boundaries easier to interpret before modifying the geometry. Across interviews, participants described the early stage of data intake as a conceptual filter that determines how the model can be shaped later. Rather than pointing to specific tool functions, they stressed that clear, structured, and complete inputs reduce unnecessary back-and-forth communication and allow both roles to begin from a shared understanding of the case. The implications of these observations are taken up in the Discussion, where the organisational and tool related aspects of handling input data are examined in more detail.
4.2. Interaction with the CAD model
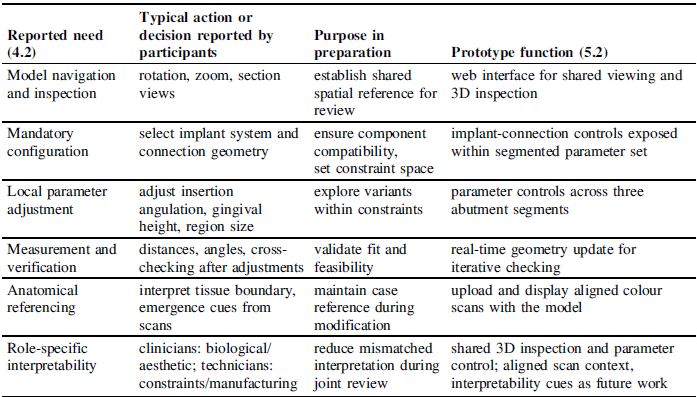
The second theme describes how participants interacted with the CAD model after verifying the scan set and alignment of the input data. Both clinicians and technicians portrayed this stage as an analytical activity in which the digital model is examined, adjusted, and compared with clinical and manufacturing requirements. Rather than treating the model as a static object, participants engaged with it through a combination of visual inspection and parameter adjustment. Technicians described that most interactions begin with navigating the model through different viewing modes. Rotational and cross-sectional inspection were consistently mentioned as essential because they allow users to examine the overall form and the fit of the design within the surrounding anatomy. Through these views, participants checked whether the design follows the intended shape and whether it corresponds to relevant spatial relationships (such as how the component passes through soft tissue, how much of it extends below the tissue line, or whether the angulation supports the planned prosthetic restoration). These observations form the basis for deciding where local adjustments are required. Parametric adjustments were the second recurring element of interaction. Participants reported that dental CAD workflows involve mandatory selections, including implant system and connection geometry, which define compatibility constraints and delimit subsequent parameter adjustments. Beyond these selections, interaction was described as repeated alternation between inspection actions (for example, rotation, sectioning, and measurement) and parameter changes that modify local geometry. Table 2 summarises the reported interaction aspects and maps each need to the prototype in Section 5.2.
Recap of reported CAD model interactions and mapping to prototype functionality

4.3. CAD interpretation across roles
The third theme examines how clinicians and technicians understand and use the same CAD model in different ways. Although they work on the same digital representation, their attention is directed toward different properties of the model due to the forms of expertise they contribute to the design process. Recognising these differences is important for understanding how a single CAD model can support collaboration in MP product development. Technicians described their work with the model as guided by parameters defined within dental CAD tools. They focused on characteristics such as implant system type, connection geometry, implant orientation, and allowable ranges for dimensions that must remain compatible with manufacturing constraints. Their interaction with the model therefore involves checking fit, ensuring positional alignment between components, and adjusting design features within the limits provided by the tool. Several technicians explained that some elements, such as the connection geometry supplied by the implant manufacturer, are fixed, whereas others, such as margin depth or abutment-wall height, can be adjusted within defined boundaries. Their work proceeds step by step, combining parameter adjustments with continuous inspection through sectional and rotational views. Clinicians, in contrast, rely on the model primarily to understand how the abutment will integrate into the patient’s oral environment. Their evaluation includes biological and aesthetic aspects, such as the transition between the abutment and soft tissue, the appearance of the emergence line, and the anticipated visual outcome once the restoration is placed. Many clinicians noted that current dental CAD interfaces do not provide a natural representation of soft tissues or surface appearance, which makes it challenging to judge how the restoration will function and appear in the patient’s mouth. As a result, they often complement the CAD view with photographs or direct communication with technicians to clarify design decisions. These findings show that the CAD model is interpreted differently depending on professional background. While technicians approach it as a parameter-defined structure that must satisfy mechanical and manufacturing requirements, clinicians view it as a reference for understanding biological adaptation and visual integration. This divergence can lead to situations in which clinicians and technicians understand decisions about geometry or parameter choices in different ways. Participants explained that these differences arise because clinicians focus on biological and aesthetic aspects of the case, while technicians attend to parameters, manufacturing limits, and the positional relationships defined within the CAD tool. Both clinicians and technicians emphasised that viewing the model through a shared visual and informational representation is important for ensuring that design decisions are understood consistently and for reducing later revisions. Clinicians described the need for clearer views that show how the abutment relates to surrounding tissues, whereas technicians noted the importance of indications that reflect parameter settings and their effect on implant-related constraints. Both clinicians and technicians emphasised that a shared representation is needed to reduce mismatched interpretation and to support alignment during anticipated joint review. Participants described recurring convergence points, including insertion direction and angulation, emergence-related geometry relative to the soft tissue boundary, and clearance conditions affecting restoration placement and occlusion. Clinicians described these points in terms of biological adaptation and aesthetic integration, whereas technicians described them in terms of parameter constraints and manufacturing feasibility. Across accounts, convergence was described as reaching an agreed interpretation of these shared evaluation criteria using the same geometric reference and case-specific scan context. These convergence points are reported from interview accounts, while empirical observation of real-time resolution mechanisms remains a focus for future work.
5. Discussion
This study examined how clinicians and technicians understand and describe the preparation and use of CAD models when contributing to the design of MP products. The findings were organised into three themes that describe needs related to input data, analytical inspection of the model, and role-specific interpretation. The following discussion connects these findings with prior studies on digital support for collaborative design and highlights the implications they raise for CAD tools used collaboratively by clinicians and technicians.
5.1. Understanding how professionals work with CAD models in MP design
The first theme (input data) shows that case starting conditions shape how reliably a CAD model can support later work. Participants emphasised the completeness of the scan set, correct implant connection information, and clear visual cues for interpreting anatomical boundaries. This aligns with prior work stressing structured preparation before collaborative design, where well-defined inputs reduce clarification cycles (Reference Khatib, Fleche, Mahdjoub, Bluntzer and SagotKhatib et al., 2016), and where integrating relevant contextual data increases the usefulness of CAD models as multidisciplinary representations (Reference Heikkinen, Johansson and ElghHeikkinen et al., 2018). The present findings build on this work by showing that professionals require not only complete geometric inputs but also contextualised scan data that preserve spatial and visual relationships. Participants described this as essential for understanding how the digital model relates to clinical constraints and for ensuring that subsequent modelling actions remain aligned with the intended functional and aesthetic goals. These insights are particularly relevant for MP, where each product instance depends on accurate digital inputs that consistently reflect individual requirements. In this sense, the results extend existing findings by clarifying which input elements professionals consider necessary for a model to serve as a dependable basis for collaborative reasoning.
The second theme concerns the role of analytical information in how participants work with CAD models. Interviewees described that once the initial scans are verified, the model must support inspection and evaluation through measurable indicators. They routinely used sectional views, distance measurements, and numerical parameters to examine fit, angulation, soft tissue adaptation, and the limits imposed by implant geometry. These accounts show that the model is understood not only as a geometric object but as a source of analytical cues that guide design decisions. This observation is consistent with earlier findings that emphasise the importance of integrating relevant information into digital models. Prior studies demonstrated that the inclusion of additional parameters and structured data improves clarity and enables teams to interpret design decisions more consistently (Reference Heikkinen and ElghHeikkinen & Elgh, 2017). Studies in conceptual design similarly noted that digital representations gain communicative value when they capture the reasoning behind design choices, not only their final shape (Reference Vuletic, Duffy, Hay, McTeague, Pidgeon and GrealyVuletic et al., 2018). The present results build on these insights by clarifying how analytical information is used in mass-personalised product design. Participants relied on measurable feedback, such as distances, angles, insertion direction, and soft tissue reference lines, to judge whether the emerging geometry aligns with functional, biological, and manufacturing constraints. In this sense, analytical information acts as a bridge between parameter settings and visual inspection. Rather than serving as a separate layer, it anchors the model to verifiable design considerations and helps participants understand how local adjustments influence overall feasibility. This use of the model strengthens collaboration between roles by making design assumptions more explicit and reducing ambiguity during joint evaluation.
The third theme examines how participants from different roles interpret the CAD model through distinct professional lenses. Interviewees described that clinicians attend primarily to biological and aesthetic considerations, whereas technicians focus on geometric constraints, manufacturability, and the relationships between parameters. These perspectives are not contradictory but reflect how each role contributes a different form of expertise to the design process. Earlier studies have shown that CAD tools shape how users frame and articulate design decisions (Reference Robertson, Walther and RadcliffeRobertson et al., 2007) and that the interpretation of digital representations influences how information is communicated between collaborators (Reference Ekströmer and WeverEkströmer & Wever, 2019). The present findings refine this understanding by showing how these interpretive differences manifest in MP product design, where the same model must support multiple forms of reasoning. These differences do not obstruct collaboration; instead, they highlight the need for representations that make role-specific reasoning visible. The communication challenges identified in clinical–laboratory collaboration (Reference Ismail and Al-MoghrabiIsmail & Al-Moghrabi, 2023) provide further evidence that mismatched assumptions about what the model should display can reduce shared understanding. The current results suggest that these challenges can be mitigated when the CAD model presents information in layers that include both domain-specific and shared elements. A model that allows participants to switch between clinically relevant views and manufacturing-oriented parameters can support more coherent interpretation across roles and reduce the need for clarification. Such capabilities would enable a CAD model to operate as a shared reference for decision-making while still accommodating the distinct informational needs of clinicians and technicians. In this way, the model can support collaborative reasoning without forcing users into a single mode of interpretation, which is essential for collaboration in MP design.
Although the empirical setting is custom dental abutments, the findings describe transferable needs for preparing CAD models that function as boundary objects across roles in mass-personalised work. Participants emphasised structured intake of case-specific inputs, iterative inspection coupled with constrained parameter changes, and role-relevant cues anchored to a shared geometric reference. Similar boundary-object dynamics have been discussed in other domains that rely on shared digital models to support cross-role collaboration.
5.2. Translating insights into a parametric CAD model for collaborative design
To translate the identified needs into a functional prototype, a parametric CAD model was developed with Grasshopper and deployed through ShapeDiverFootnote 1 . Grasshopper was selected for parametric control of NURBS geometry suited to implant platforms and emergence-related profiles. Prior work reports that solid-based tools offer limited control for individually shaped abutments and that many dental CAD parameters are fixed (Reference Huić, Kosec, Martinec and ŠkecHuić et al., 2025). NURBS-based modelling, by contrast, enables more adaptable shaping of curvature transitions and emergence profiles, which are central to custom abutment design. Reference Kosec, Huić, Gulin, Škec, Anisic and ForzaKosec et al. (2024b) similarly reported that many parameters in dental CAD tools are predefined and cannot be altered, restricting controlled variation during design. These findings indicated that Grasshopper provides the parametric environment required for modelling individualised abutments. ShapeDiver was selected to provide browser-based access, parameter control, and aligned colour scan upload, consistent with the reported need for shared viewing and scan context. Table 2 maps the interaction needs (Section 4.2) to prototype functions. Role-specific interpretability cues are noted as future work. The resulting model includes parameters for the three structural segments relevant to abutment design: the implant-connection segment, the transgingival segment, and the prosthetic segment. Parameters that control the implant-connection region (for example, angle, R1, R2, and H1) represent the range of geometric adjustments discussed by technicians in relation to implant position and insertion direction. Parameters such as shoulder width and shoulder thickness allow adaptations at the prosthetic region that clinicians considered important for clinical interpretation. The model also incorporates the loading of aligned colour scans to maintain spatial and visual cues identified earlier as necessary input conditions for collaborative work.
Parametric CAD model for collaborative design developed in ShapeDiver

The model supports the loading of aligned colour scans, parameter control across the relevant regions of the abutment, and real-time interaction through a web interface. These capabilities reflect how the empirical insights obtained from the interviews can be translated into a usable digital model that supports shared examination of design options. Allowing users to adjust parameters while observing their geometric effects responds directly to the identified need for interaction that links visual assessment with quantitative control. Likewise, incorporating colour scans provides visual reference information that strengthens the spatial understanding required for individualised design. This implementation represents an initial step toward future synchronous collaborative sessions in which clinicians and technicians can explore and evaluate design variations together. The results also contribute to the wider discussion on CAD models as shared artefacts that support communication between professionals with complementary expertise. This connects with earlier studies that described digital models as mediators of collaboration in distributed design processes (Reference Marion, Olechowski and GuoMarion et al., 2021). It also addresses challenges previously identified by Reference Cheng, Davis, Zhang, Zhou and OlechowskiCheng et al. (2023), who noted that challenges in interpretation and maintaining a common reference often persist despite advances in collaborative tools. The present study adds to this discussion by showing that some of these challenges can be mitigated within the CAD model itself through explicit structuring of parameters, contextual inputs, and role-specific information. In doing so, the model supports a more coherent exchange of perspectives within MP product design.
The prototype is an initial implementation derived from interview accounts and has not yet been evaluated in synchronous joint review sessions. The qualitative design and the dental abutment case support analytical rather than statistical generalisation. Future work will evaluate the prototype in synchronous joint review sessions to examine alignment and resolution mechanisms and may also examine multimodal interaction for collaborative CAD (Reference Niu, Leeuwen, Hao, Wang and LachmannNiu et al., 2022).
6. Conclusion
This study examined how clinicians and technicians describe the preparation and use of CAD models in collaborative design processes for MP products. Three needs emerged from the interviews: the need for complete input data, additional information that supports interaction with the model, and interpretation that reflects role-specific perspectives. These insights informed the development of an initial parametric CAD model in ShapeDiver, designed to demonstrate how empirical findings can guide tool development. Future work will test this model in synchronous collaborative sessions to evaluate how it supports communication and joint design decisions. These needs are likely transferable to other MP settings where a shared CAD model mediates cross-role collaboration and requires structured inputs, constrained parameter changes, and role-relevant interpretation cues.
Acknowledgement
This research was funded by the project NPOO.C3.2.R3-I1.04.0121: Generative Design for Mass Personalization of Dental Implantoprosthetic Abutments (GENKON).





 Open access
Open access