


SSRIs are the most commonly prescribed antidepressants for major depressive disorder (MDD). First-line treatment with SSRIs effectively reduces depressive symptoms in approximately half of patients with depression, but many others experience an insufficient response. Reference Rush, Trivedi, Wisniewski, Nierenberg, Stewart and Warden1 SSRIs are also often limited by a slow onset of therapeutic effect Reference Browning, Cowen and Sharp2 (though see Taylor et al Reference Taylor, Freemantle, Geddes and Bhagwagar3 and Khoo et al Reference Khoo, Demchenko, Frey, Milev, Ravindran and Parikh4 for evidence of early treatment effects), common side effects such as sexual dysfunction Reference Balon5 (though see Weber et al Reference Weber, Frokjaer, Armand, Nielsen, Knudsen and Joergensen6 for improvements in some patients) and limited benefit for cognitive impairment. Reference Colwell, Tagomori, Chapman, Gillespie, Cowen and Harmer7 Considering the global prevalence of MDD, 8 identifying alternative treatments to tackle these limitations is essential.
Emotional processing model of antidepressant action
A key mechanism of SSRI action is their ability to ameliorate negative biases in information processing common to MDD, Reference Godlewska and Harmer9 such as greater recall of negative (versus positive) information and a greater likelihood of interpreting ambiguous stimuli negatively. Reference Roiser, Elliott and Sahakian10 The SSRI citalopram, for example, reduces negative biases in the recall of self-referential words and the interpretation of facial expressions, Reference Harmer, O’Sullivan, Favaron, Massey-Chase, Ayres and Reinecke11 and attenuates neural response to negative faces in the amygdala and associated networks. Reference Godlewska, Browning, Norbury, Cowen and Harmer12 These changes occur early in treatment, are associated with later symptom improvement and are seen across several existing antidepressant treatments with different pharmacology, suggesting they may reflect a common or converging mechanism. Reference Ma13,Reference Williams, Korgaonkar, Song, Paton, Eagles and Goldstein-Piekarski14 Emotional processing models have therefore been used in antidepressant drug development as an early biomarker of antidepressant action. Reference Post, Smart, Krikke-Workel, Dawson, Harmer and Browning15
The potential of serotonin 4 receptor (5-HT4R) agonists
One approach for developing novel antidepressant treatments is selective targeting of serotonin receptor subtypes involved in mood and cognition. Of particular interest is the potential of selective serotonin 4 receptor (5-HT4R) agonists in the treatment of depression and cognition. Reference Murphy, de Cates, Gillespie, Godlewska, Scaife and Wright16 Positron emission tomography (PET) studies have shown reduced 5-HT4R binding in MDD Reference Köhler-Forsberg, Dam, Ozenne, Sankar, Beliveau and Landman17 and preclinical work demonstrates that 5-HT4R agonists produce antidepressant- and anxiolytic-like effects in rodent models, including the forced-swim test, sucrose preference and elevated plus maze. Reference Lucas, Rymar, Du, Mnie-Filali, Bisgaard and Manta18–Reference Pascual-Brazo, Castro, Díaz, Valdizán, Pilar-Cuéllar and Vidal20 Notably, these studies found effects consistently occur more rapidly with 5-HT4R agonism than with SSRIs (two to three times faster), which may be due to a rapid induction of neuroplastic changes, and the direct excitation of serotonin cells in the dorsal raphe nucleus. Reference Faye, Hen, Guiard, Denny, Gardier and Mendez-David21 Together, these findings suggests that 5-HT4R is a promising fast-acting antidepressant target.
Aim of current study
The current experimental medicine study aimed to investigate the translation of these preclinical antidepressant effects of 5-HT4R agonism to human models of antidepressant action, in participants with unmedicated MDD. Specifically, we used a novel, highly selective 5-HT4R partial agonist (PF-04995274) to investigate early effects (6–9 days) on behavioural and neuroimaging models of emotional cognition previously shown to be sensitive to the effects of SSRIs. We hypothesised that PF-04995274 would reduce negative emotional biases and reduce the neural response to negative stimuli, similar to the effects seen with SSRIs. We included a group randomised to citalopram as a positive control to confirm expected SSRI-induced changes. As this was the first investigation of 5-HT4R agonism in MDD, we also measured effects on depression symptoms.
Method
Participants
Between 1 August 2018 and 29 July 2022, 90 participants (aged 18–61) with MDD (DSM-5) were recruited. Diagnosis was confirmed by study psychiatrists, using the Structured Clinical Interview for DSM Disorders (SCID). Participants had received no drug or face-to-face psychological treatment for their depression within the previous 6 weeks, and were not taking any other psychotropic medication. Participants were adults of any gender, fluent in English, with no contraindications to 5-HT4R agonism or citalopram. We excluded potential participants who had failed to respond to antidepressant medication in their current episode of depression, or were at clinically significant risk of suicide. We also excluded those who may have been at increased risk of adverse events (e.g. severe gastro-intestinal problems). See Supplementary Materials available at https://doi.org/10.1192/bjp.2026.10664 for a full list of inclusion and exclusion criteria.
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2013. All procedures involving human subjects/patients were approved by the South-Central NHS Research Ethics Committee (18/SC/0076). The protocol was pre-registered with clinicaltrials.gov (NCT03516604). Participants gave written and verbal informed consent. Participants were paid £200 for their participation (or £170 if the magnetic resonance imaging (MRI) scan was omitted due to contraindication).
Study design
This was a between-subject, double-blind, randomised, placebo-controlled experiment. Participants received 7 days of PF-04995274 (15 mg once daily), citalopram (20 mg once daily) or placebo, taken orally; up to 2 additional days’ dosing was allowed to accommodate scheduling.
The study included four visits in total: (a) Screening; (b) Dosing Visit; (c) Research Visit One (including facial magnetic resonance imaging (fMRI) scan) on day 6–9, and (d) Research Visit Two (including all cognitive tasks and end-of-study symptom assessment) on day 7–9 (Supplementary Fig. S1). By day 6 when scanning took place, steady state plasma levels were expected; the half-life (t 1/2) of PF-04995274 is ∼30 h, and citalopram is ∼35 h. All visits occurred at the Warneford Hospital, Oxford University Department of Psychiatry. Scanning took place at the Oxford Centre for Human Brain Activity (OHBA), part of the Oxford Centre for Integrative Neuroimaging (previously the Wellcome Centre for Integrative Neuroimaging).
Interventions
PF-04995274 is a highly selective 5-HT4R partial agonist, developed by Pfizer, and provided (alongside matched placebo tablets) via the Medical Research Council (MRC)-Industry Asset Sharing Initiative. It has been previously tested in human clinical trials of healthy volunteers, with PET studies establishing that 5 mg of PF-04995274 produced >80% receptor occupancy of brain 5-HT4R 4 h after the first dose, and that 15 mg was well tolerated. 22
Citalopram is an SSRI, and is a safe, well tolerated, licensed treatment for MDD. It was provided and encapsulated (alongside matched placebo capsules) by the Cardiff and Vale University Health Board, St. Mary’s Pharmaceutical Unit.
The first dose was administered on site, with participants monitored for 3 h post dosing. All subsequent administration occurred at home.
Randomisation and blinding
The research team and participants were blinded to group allocation. The randomisation code (stratified by gender) was drawn up and held by the Oxford Health Foundation Trust Pharmacy (Clinical Pharmacy Support Unit – CPSU – Kennington), using an online randomisation tool (Sealed Envelope); they also stored and dispensed the medication. Group allocation was concealed using sequential numbered containers (see Supplementary Materials for more details).
Power calculation
Based on previous citalopram–placebo comparisons, Reference Harmer, Shelley, Cowen and Goodwin23 19 participants per group would provide 90% power (α = 0.05) for behavioural measures. To accommodate potential exclusions, subtler effects in fMRI analyses, and the less well characterised effects of 5-HT4R agonism, we aimed for 25 participants with complete behavioural and fMRI data per group. Including 13 participants who completed behavioural assessments but not MRI (due to contraindications), 90 participants were recruited.
Behavioural measure of emotional cognition
Emotional cognition was assessed at Research Visit Two (day 7–9) with a battery of cognitive tasks from the Emotional Test Battery (P1vital® Limited Products), Reference Thomas, Higgs and Dourish24 including the Facial Expression Recognition Task (FERT): participants viewed briefly presented (500 ms) faces depicting basic emotions (happiness, fear, anger, disgust, sadness, surprise, neutral) at varying intensities and were asked to classify each via button press. There were 250 trials in a fixed pseudorandomised order.
(See Supplementary Materials for details of other emotional cognition tasks. Results from non-emotional cognition tasks are reported elsewhere.) Reference de Cates, Gillespie, Scaife, Martens and Carson25
Neuroimaging measure of emotional cognition
Neural activity during emotional processing was assessed using an implicit emotional cognition task conducted during an fMRI scan. Briefly, emotionally valenced faces (fearful or happy) were presented on screen for 100 ms. Participants were instructed to indicate the assumed gender of the face (male or female) as quickly as possible using a button press. No reference was made to face emotion during the instructions. There was a rest block at the start of the experimental run, and then the task followed an A–B–Rest design (condition A, fearful faces, 18 s; condition B, happy faces, 18 s; rest, 12 s). Seven repetitions yielded 126 s per emotional condition and 96 s rest. This version was a recent modification of the task, which we have shown to be sensitive to the acute effects of antidepressants on neural processing. Reference de Cates, Martens, Wright, Gould van Praag, Capitão and Gibson26 The task software was written using Psychopy version 1.84.2, on a Windows platform (software available at https://github.com/psychopy/psychopy/releases/).
Blood-oxygenation-level-dependent (BOLD) fMRI and T1-weighted anatomical images were acquired using a 3-Tesla Siemens Prisma scanner, equipped with a 32-channel head matrix coil (Siemens, Erlangen, Germany). Foam padding and a head restraint were used to control head movement. In the scanner, participants also completed a memory encoding task and resting-state scan (reported elsewhere), Reference de Cates, Gillespie, Scaife, Martens and Carson25 and an arterial spin-labelling (ASL) scan. The full acquisition protocol is available here: https://osf.io/ycgdk/files/kx5yv.
Clinical assessment and questionnaire measures
To obtain an observer-related measure of depression severity, trained researchers assessed participants at baseline and at end of study using the 17-item Hamilton Rating Scale for Depression (HAM-D). Reference Hamilton27
To obtain a self-report measure of depression severity, participants completed the Beck Depression Inventory-II (BDI-II) Reference Beck, Steer, Ball and Ranieri28 at baseline and at end of study, as well as the Snaith-Hamilton Pleasure Scale (SHAPS) Reference Snaith, Hamilton, Morley, Humayan, Hargreaves and Trigwell29 to measure anhedonic symptoms. At baseline, the Spielberger State–Trait Anxiety Inventory, Trait Version (STAI-T) Reference Spielberger30 and the Eysenck Personality Questionnaire Reference Eysenck, Eysenck and Barrett31 were also completed, to assess baseline trait anxiety and personality. State affect and anxiety were measured at both research visits using: the Positive and Negative Affect Scale (PANAS); Reference Watson, Clark and Tellegen32 visual analogue scales (VAS); Reference Bond and Lader33 and the Spielberger State–Trait Anxiety Inventory, State Version (STAI-S). Reference Spielberger30
Commonly reported side-effects (checklist in Supplementary Materials) were also measured at each visit, and at home across the study period. At the end of the study, participants were asked to guess their group allocation with a multiple-choice question.
Statistical analysis
Behavioural and clinical data
R (version 4.3.3, https://cran.r-project.org/bin/windows/base/old/, on Windows platform) was used for all data processing and analysis. Scripts and data are publicly available.
For all behavioural data, outliers were determined based on blinded visual inspection of histogram plots. Outlier removal/sensitivity checks were determined on 12 January 2023, prior to unblinding. There was determined to be one outlier participant in the FERT data, who was removed during sensitivity checks.
Demographic characteristics and baseline clinical measures are reported descriptively. For all analyses, the citalopram group was first compared with the placebo group to confirm expected SSRI effects. The 5-HT4R group was then compared with placebo to determine the effect of PF-04995274. Group differences in cognitive task performance and clinical outcomes were assessed using ANOVA, with group as the between-participant factor and task condition (e.g. valence) as the within-participant factor. For scales where baseline measures were collected (HAM-D, BDI and SHAPS), baseline severity was included as a covariate. Chi-square tests were used to assess group differences in number of reported side-effects. A p value less than 0.05 was used to denote statistical significance. Partial eta-squared is reported as a measure of effect size.
As the STAI-S, PANAS and VAS measures were not completed an equal number of times for all participants (due to differences in MRI scanning compatibility and thus completion of one or two research visits), an average score across research visits was calculated for each participant to indicate overall end-of-study affect.
Magnetic resonance imaging data
fMRI data were pre-processed and analysed using FEAT (FMRI Expert Analysis Tool), version 6.0.4, part of FSL (FMRIB’s Software Library2, https://fsl.fmrib.ox.ac.uk). See Supplementary Material for pre-processing steps.
In the first-level analysis, individual activation maps were computed using the general linear model with local autocorrelation correction. Three explanatory variables were modelled: ‘happy’ and ‘fear’ images and explicit fixation cross, to replicate the models in our previous papers. Reference de Cates, Martens, Wright, Gould van Praag, Capitão and Gibson26 Temporal derivatives were included in the model. Variables were modelled by convolving each block with a haemodynamic response function with a standard deviation of 3 s and a mean lag of 6 s. Two participants had significant movement (one allocated to citalopram, one allocated to placebo) and were therefore excluded from fMRI analysis prior to unblinding. All other absolute displacements were less than 2.2 voxels and relative displacements less than 0.2 voxels. The FSL motion outliers tool was used to reduce the influence of remaining motion. At the whole-brain level, we contrasted fearful images with happy and fixation cross: (a) fear > fixation; (b) happy > fixation; (c) fear > happy; (d) happy > fear; (e) mean (of happy and fearful faces) > fixation.
In the second-level analysis, whole-brain individual data were combined at a group level (placebo versus active drug – either citalopram or PF-04995724) using a mixed-effects group analysis across the whole brain corrected for multiple comparisons. Groups were contrasted with each other using the following comparisons: (a) placebo > active; (b) active > placebo; (c) mean of active + placebo participants. Brain activations showing significant group differences were identified using cluster-based thresholding (Z > 3.1, p < 0.05 FWE corrected). Significant interactions from whole-brain analyses were further explored by extracting percentage BOLD signal change with Featquery for each type of contrast.
As the amygdala Reference Tassone, Gholamali Nezhad, Demchenko, Rueda and Bhat34 and prefrontal cortex Reference Pizzagalli and Roberts35 were a particular focus of our hypothesis, the amygdala, medial-frontal cortex (MFC) and orbito-frontal cortex (OFC) were pre-specified as regions of interest (ROI). A functional ROI mask was created for each by multiplying mean activation (mean>fixation contrast) for all participants (placebo, citalopram and PF-04995274) by the Harvard-Oxford subcortical atlas anatomical mask at a 50% threshold. Percentage BOLD signal change for each contrast in each hemisphere was then extracted.
Results
Sample demographics
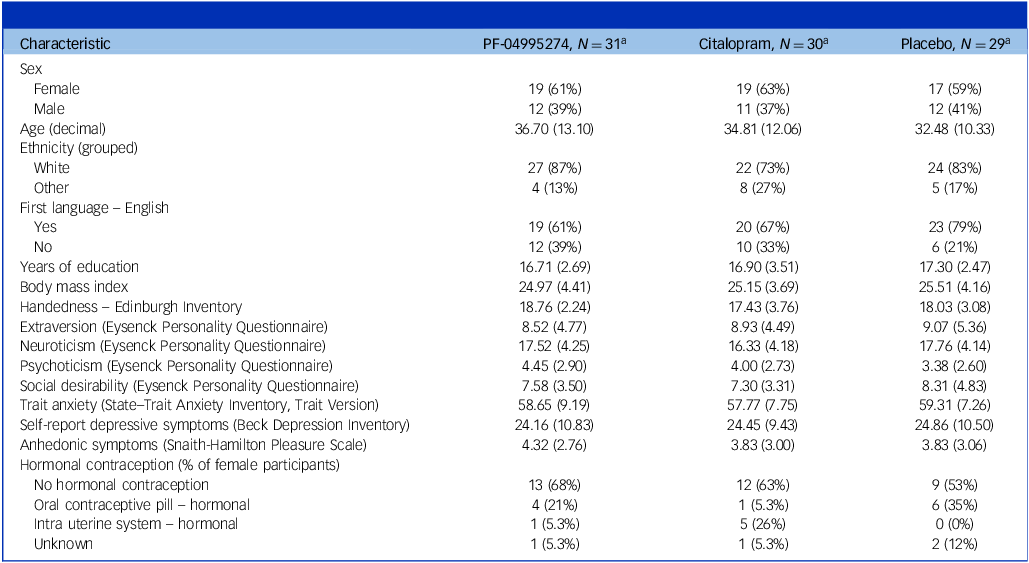
Ninety participants completed the full period of study medication and the final research visit. Seventy-seven of these had no scanning contraindications and completed an MRI scan visit prior to their final research visit (see CONSORT diagram, Fig. 1). Participants were predominantly white, native English speakers aged 20–40, with education equivalent to completion of an undergraduate degree (Table 1, and Supplementary Table S1 for comorbidities).
RESTAND CONSORT diagram. MDD, major depressive disorder, MR, magnetic resonance.

Demographics and baseline self-report – all participants

a. n (%); mean (s.d.).
Ethnicity, other, self-defined: PF-04995274 = Chinese, Eastern European, Ashkenazi Jewish; Citalopram = Asian (n = 4), Black, Mixed, Mixed Indian and British; Placebo = Asian, Thai, Chinese, Mixed, Mixed Welsh/Indo Guaynese.
On a behavioural measure of emotional cognition, participants who received the 5-HT4 agonist did not show the reduced negative bias seen with citalopram
When comparing citalopram with placebo, there was no main effect of group (F(1,56) = 0.49, p = 0.49, ηp2 = 0.009) but there was a significant interaction between medication group and valence on total percentage accuracy of emotional face classification (F(1,56) = 4.30, p = 0.043, ηp2 = 0.07). Consistent with previous reports, the citalopram group showed relatively greater accuracy for positive faces and reduced accuracy for negative faces, compared with placebo (Fig. 2(a)).
In a facial expression recognition task, only the citalopram versus placebo group comparison showed a significant interaction with valence on accuracy and reaction; compared with placebo, the citalopram group displayed reduced accuracy and slower reaction times to identify negative faces relative to positive faces. (a) Citalopram versus placebo, comparing percentage accuracy for negative versus positively valenced faces. (b) PF-04995274 versus placebo, comparing percentage accuracy for negative versus positively valenced faces. (c) Citalopram versus placebo, comparing reaction time (RT) for negative versus positively valenced faces. (d) PF-04995274 versus placebo, comparing reaction time for negative versus positively valenced faces. *p < 0.05, for interaction between group and valence on ANOVA. Error bars show standard error of the mean. Placebo group data is shown in both citalopram versus placebo plots ((a) and (c)), and in PF-04995274 versus placebo plots ((b) and (d)).

Similarly, when comparing reaction times for the citalopram group to placebo, there was no main effect of group (F(1,56) = 0.98, p = 0.325, ηp2 = 0.02) but there was a significant interaction between group and valence on speed of emotional face classification (F(1,56) = 6.78, p = 0.012, ηp2 = 0.11), with the citalopram group showing slower reaction times for negative faces (Fig. 2(c)).
In contrast, when comparing the PF-04995274 group with placebo, there was no main effect of group on accuracy (F(1,57) = 0.76, p = 0.39, ηp2 = 0.01) or reaction time (F(1,57) = 1.14, p = 0.289, ηp2 = 0.02), and no interaction between group and valence for accuracy (F(1,57) = 1.09, p = 0.301, ηp2 = 0.02) or reaction time (F(1,57) = 1.39, p = 0.244, ηp2 = 0.02) (Fig. 2(b)/(d)).
The significance, size and pattern of all results remained consistent in all sensitivity checks (using an adjusted accuracy measure which accounts for response bias, transforming the data to address skew, removing a potential outlier participant). See Supplementary Materials for results on misclassification rates.
On a neuroimaging measure of emotional cognition, participants who received the 5-HT4 agonist showed a distinct pattern of neural changes to those on citalopram, with increased medial-frontal activation across emotional face valences
Whole brain analyses
When comparing citalopram with placebo, there was no difference for mean of emotional faces (fear + happy) versus fixation, but there was significant differential activation for fear versus happy in six clusters covering angular gyrus, lateral occipital cortex, cerebellum, middle temporal gyrus and fusiform gyrus. In all clusters, the placebo group showed greater activation for fearful faces and the citalopram group showed greater activation for happy faces (p < 0.01, Supplementary Fig. S2 and Supplementary Table S6). When comparing the PF-04995274 group with placebo, there were no significant differences on any contrast.
For behavioural data (accuracy and reaction time for gender discrimination) and broad task effects in the fMRI data, see Supplementary Materials.
ROI analyses
In the left amygdala, when comparing citalopram with placebo, there was a main effect of group (F(1,90) = 4.008, p = 0.048, ηp2 = 0.04), but no significant interaction between group and face valence on % BOLD signal change (F(1,90) = 0.001 p = 0.97, ηp2 = 0.0001), i.e. the citalopram group showed reduced amygdala BOLD response across valences (Fig. 3(a)). There was no main effect or interaction for the right amygdala (p > 0.4). When comparing the PF-04995274 group to placebo, there was no significant main effect or interaction (p > 0.15) for the left or right amygdala (p > 0.08).
In regions of interest analysis of an implicit emotional faces task using functional magnetic resonance imaging, citalopram was associated with reduced amygdala blood-oxygenation-level-dependent (BOLD) response across valences and PF-04995274 was associated with increased medial-frontal BOLD response across valences. The figure shows % mean BOLD signal change in (a) left amygdala, (b) right amygdala, (c) medial-frontal cortex and (d) orbito-frontal cortex, defined using functional mask. Values extracted separately for fearful > fixation and happy > fixation, comparing citalopram group versus placebo group and then PF-04995274 group versus placebo group. ***p < 0.001, for interaction between group and valence on analysis of variance. Error bars show standard error of the mean. Placebo group data are shown in both citalopram versus placebo plots (upper row), and in PF-04995274 versus placebo plots (lower row).

In the medial-frontal cortex, there was a main effect of group when comparing the PF-04995274 group with placebo (F(1,100) = 5.98, p = 0.016, ηp2 = 0.06), but no significant interaction between group and face valence (F(1,100) = 0.042, p = 0.84, ηp2 = 0.0004), i.e. the PF-04995274 group showed greater BOLD response across valences (Fig. 3(b)). There was no main effect or interaction when comparing citalopram group with placebo (p > 0.7).
In the orbito-frontal cortex, there was no significant difference for any group comparison, on any contrast (Fig. 3(c)).
After 1 week, participants given either PF-04995274 or citalopram showed significant decreases in depressive symptoms
Observer-rated symptoms
At baseline, the mean HAM-D score for the whole sample was 16.1 (s.d. = 2.78), indicating mild to moderate depression. Reference Zimmerman, Martinez, Young, Chelminski and Dalrymple36 Groups were reasonably well matched, with marginally lower severity in the citalopram group (mean = 15.2, s.d. = 2.8) compared with the placebo (mean = 16.9, s.d. = 2.88) and PF-04995274 (mean = 16.2, s.d. = 2.51) groups.
Controlling for baseline severity, the citalopram group scored significantly lower on the HAM-D at the final research visit (mean = 12.7, s.d. = 5.20) compared to placebo (mean = 15.5, s.d. = 3.9) (F(1, 54) = 5.50, p = 0.02, ηp2 = 0.09), as did the PF-04995274 group (mean = 12.7, s.d. = 4.04) (F(1, 56) = 7.61, p = 0.008, ηp2 = 0.12) (Fig. 4). The significance and size of these effects remained, or increased, in sensitivity analyses (removing the sleep subscale, or removing potential outlier participants), both groups scored significantly lower if analysis was restricted to core depressive subscale, and only the PF-04995274 group scored significantly lower on the anxiety subscale (Supplementary Table S2).
Participants given either PF-04995274 or citalopram displayed significantly reduced depressive symptoms on Hamilton Depression (HAM-D) ratings after 7–9 days. (a) Citalopram group versus placebo group. (b) PF-04995274 group versus placebo group. *p < 0.05, **p < 0.01 for main effect of group on analysis of variance, controlling for baseline score. Error bars show standard error of the mean. Placebo group data is shown in both citalopram versus placebo plot (a), and in PF-04995274 versus placebo plots (b).

Self-reported symptoms and affect
Controlling for baseline severity, the PF-04995274 group – but not the citalopram group – reported significantly lower depressive symptoms (BDI) at the final visit than placebo. Similarly, only the PF-04995274 group reported lower state anxiety (STAI-S) than placebo at the final visit. Both groups reported significantly lower negative affect at final visits compared with placebo, with double the effect size in the PF-04995274 versus citalopram group. Only the citalopram group reported significantly lower positive affect at final visits compared with placebo. Neither group significantly differed from placebo on any other scales. See Supplementary Tables S3 and S4 for all statistics.
Success of blinding
There was a significant association between medication group and guessed medication (X 2 (6, N = 90) = 12.92, p = 0.04), driven by the citalopram group (citalopram versus placebo, X 2 (3, N = 59) = 8.09, p = 0.04; PF-04995274 versus placebo, X 2 (3, N = 60) = 2.06, p = 0.56). Specifically, 43.34% of participants allocated to citalopram correctly guessed their allocation (v. 9.78% of those allocated to PF-04995274), and 60% correctly guessed they had an active drug (v. 25.81% of PF-04995274 participants).
Side-effects
The PF-04995274 group reported new fatigue significantly more often (X 2 = 6.5, p = 0.04), all reports of which were described as mild to moderate. There were no other significant group differences in new reported side-effects (p > 0.1), though only participants in the PF-04995274 group reported increased appetite (not systematically recorded) (see Supplementary Table S5).
Five participants (two on placebo, two on citalopram, one on PF-04995274) withdrew from the study due to adverse events, all of which resolved within 24 h of discontinuation.
Discussion
The primary finding of this double-blind, randomised study is that unmedicated depressed participants who received the novel 5-HT4R agonist (PF-04995274) did not display the profile of behavioural and neural changes in emotional cognition observed with citalopram, and anticipated based on previous SSRI research. Reference Harmer, O’Sullivan, Favaron, Massey-Chase, Ayres and Reinecke11,Reference Godlewska, Browning, Norbury, Cowen and Harmer12 However, participants who received the 5-HT4R agonist did show distinct neural changes during emotional cognition, and both groups reported significant reductions in depressive symptoms after one week of administration compared with placebo.
On a behavioural facial expression recognition task, participants randomised to citalopram displayed indications of ameliorated negative bias; they showed relatively reduced recognition of – and slower reaction times to – negative faces, and increased recognition of – and faster reaction times to – positive faces, compared with the placebo group. Concurrently, in an implicit emotional faces fMRI task, whole-brain analyses revealed significantly reduced activity in response to fearful versus happy faces, compared with placebo, across a number of relevant brain regions including the angular gyrus, lateral occipital cortex, middle temporal gyrus and fusiform gyrus. Additionally, pre-registered ROI analysis showed reduced left amygdala activation to emotionally valenced faces in the citalopram group. Collectively, these findings align with previous literature on the neural effects of SSRIs during emotional processing, which are thought to be a key mechanism of SSRI efficacy. Reference Godlewska and Harmer9
In contrast, the 5-HT4R agonist group showed no significant differences on any behavioural measures of emotional cognition or in amygdala BOLD response to emotional stimuli, and no valence-specific neural changes. This broadly aligns with our previous research using 1 and 6 days of the 5-HT4R agonist prucalopride (1 mg). However, in ROI analysis, the 5-HT4R agonist group did demonstrate significantly increased medial-frontal cortex activation in response to both negative and positive faces. The medial-frontal cortex modulates amygdala activity, and is thought to be involved in higher-level processing of emotional cognition and affective state, including representation of interpersonal relationships; Reference Klein-Flügge, Bongioanni and Rushworth37 interestingly, meta-analytic evidence in studies of patients with MDD/anxiety disorders indicates that psychotherapy such as CBT (but not conventional SSRIs) is typically associated with increased activity in this region. Reference Nord, Barrett, Lindquist, Ma, Marwood and Satpute38 This differs from our findings with prucalopride in healthy volunteers, which found 5-HT4R agonism was associated with reduced activity in the medial-prefrontal cortex and the inferior parietal lobule during the same task. It is unclear whether this may be due to important differences between the compounds; while early studies with PF-04995274 characterised brain receptor occupancy, 22 as it was developed with neurocognitive use in mind, this is less well established for prucalopride which is known primarily for its effects on 5-HT4R in the gastrointestinal system, Reference de Cates, Martens, Wright, Gould van Praag, Capitão and Gibson26,Reference Murphy, Wright, Browning, Cowen and Harmer39 a system which may independently be relevant for depression. Reference Bastiaanssen, Cussotto, Claesson, Clarke, Dinan and Cryan40 Alternatively, it may highlight the importance of translating findings into a clinical population; PET studies have already shown that the relationship between 5-HT4R function and cognitive and physiological domains (e.g. memory, cortisol awakening response) is reversed in healthy volunteers compared with participants with depression. Reference Köhler-Forsberg, Dam, Ozenne, Sankar, Beliveau and Landman17,Reference Jakobsen, Fisher, Dyssegaard, McMahon, Holst and Lehel41,Reference Vulpius, Köhler-Forsberg, Ozenne, Larsen, Nasser and Svarer42
Participants receiving either active drug scored significantly lower on observer-rated depression severity at the end of the study compared with placebo. While somewhat unexpected considering the short duration of the study (7–9 days), early SSRI efficacy has been previously reported in some studies (e.g. Taylor et al Reference Taylor, Freemantle, Geddes and Bhagwagar3 and Khoo et al Reference Khoo, Demchenko, Frey, Milev, Ravindran and Parikh4 ). In the 5-HT4R agonist group, this was accompanied by significant reductions in self-reported depression, state anxiety and negative affect. The specific improvement in anxiety symptoms – also seen in analysis of the anxiety subscale of the HAM-D – is noteworthy given evidence that anxiety is a consistent predictor of worse clinical outcomes. Reference De Carlo, Calati and Serretti43,Reference Solmi, Cortese, Vita, De Prisco, Radua and Dragioti44 While the citalopram group had significant unblinding, blinding was well maintained in the 5-HT4R group. Interestingly, the citalopram group reported significant reductions in both negative and positive affect, perhaps suggestive of emotional blunting. Reference Masdrakis, Markianos and Baldwin45 Our fMRI finding of non-specific reduction in amygdala activation to emotional faces may correspond with this; however, the lack of amygdala differentiation between the valences of the faces across the whole group, as in our previous use of the task, Reference de Cates, Martens, Wright, Gould van Praag, Capitão and Gibson26 may instead indicate that features of this version of the task (namely, more tightly cropped face images) reduce differentiation between emotional expressions.
Interpretation of clinical outcomes should be cautious; this study was not designed as a clinical efficacy trial, so depression severity was not our primary outcome and study duration was short. Exclusion criteria were also restrictive and participants had mild to moderate depression severity, so may not be representative of the patients prescribed antidepressants (which may have also limited the effect sizes). We did not collect baseline measures of emotion cognition, and so could not directly investigate the association between within-participant change in emotional cognition and change in clinical outcomes. Also, while we collected data on contraception use (due to findings indicating that oral hormonal contraception use reduces 5-HT4R binding Reference Larsen, Köhler‐Forsberg, Dam, Poulsen, Svarer and Jensen46 ), and report averages for behavioural and clinical outcome measures split by hormonal contraception use (see Supplementary Table S6), our sample was not powered to explore subgroup analyses. Nonetheless, we provide interesting preliminary experimental evidence in a clinical population that 5-HT4R agonism displays promise for antidepressant drug development. This is consistent with a recent emulated target trial from our group using large-scale USA electronic health records, which found that prescription of prucalopride is associated with reduced incidence of first-ever depression, relative to other anti-constipation agents. Reference de Cates, Harmer, Harrison, Cowen, Emmanuel and Travis47
Collectively, these results suggest that any antidepressant efficacy of 5-HT4R agonism likely operates via mechanisms distinct from conventional SSRI antidepressants, and should be a focus for future research, particularly as this raises the possibility of complementary combination therapy. In our previous work with prucalopride, we reported pro-cognitive effects of 5-HT4R agonism on learning and memory tasks Reference de Cates, Martens, Wright, Gould van Praag, Capitão and Gibson26,Reference Murphy, Wright, Browning, Cowen and Harmer39,Reference de Cates, Wright, Martens, Gibson, Türkmen and Filippini48 and our finding of increased medial-frontal activity during emotional cognition may provide additional support for this. One speculation may be that 5-HT4R agonism indirectly improves mood by ameliorating cognitive impairment. Elsewhere, we report on additional results from the current study suggesting that 5-HT4 agonism also has therapeutic potential for treating cognitive symptoms of depression; Reference de Cates, Gillespie, Scaife, Martens and Carson25 however, any causal link between cognitive improvement and overall clinical improvements remains unexplored.
In conclusion, this first randomised, experimental study in patients with depression found that 6–9 days of 5-HT4R agonism with PF-04995274 produced neural and behavioural and neuroimaging effects that contrasted with those seen with conventional SSRI antidepressants, showing no reduction in negative bias but instead increased medial-frontal cortex activity. Participants receiving the novel 5-HT4R agonist also reported significantly lower depressive symptoms after 7–9 days, a finding that warrants confirmation in clinical trials and in populations with more severe symptoms, alongside further experimental work to clarify the distinct underlying mechanisms.
Supplementary material
The supplementary material is available online at https://doi.org/10.1192/bjp.2026.10664
Acknowledgements
We would like to thank numerous research assistants for their support with data collection (James Carson, Lucy Wright, Ingrid Martin, Evie Watson) and data processing (Esther Teo and Anutra Guru); numerous medics for support with clinical cover (Michael Browning, Riccardo De Giorgi, Tarek Zghoul, Paul Harrison, Sara Costi); Cassandra Gould Van Praag for her support with the scanning protocol and analysis pipelines; numerous staff (medical, nursing and administrative) at the Oxford Health Clinical Research Facility; the radiographers at the OHBA; Orla MacDonald, Jo Galloway and others at CPSU (Oxford Health) for their pharmaceutical support; and the Oxford Health Biomedical Research Centre Patients Active in Research Group who provided consultation on study adverts and protocol. Finally, we would like to extend a huge thank you to all of the participants who took part in the study, especially as this involved specifically giving their time and energy during ongoing depressive episodes.
Author contributions
A.L.G. – methodology, investigation, formal analysis, data curation, writing – original draft, writing – review and editing, visualisation, project administration. A.N.d.C. – methodology, investigation, data curation, writing – review and editing. J.S. – methodology, investigation, data curation, writing – review and editing. M.B. – investigation, data curation, writing – review and editing. M.A.G.M. – data curation, software, writing – review and editing. D.G. – investigation, data curation, writing – review and editing. B.R.G. – methodology, investigation, writing – review and editing. W.H. – writing – review and editing, project administration, resources. P.J.C. – funding acquisition, conceptualisation, methodology, investigation, writing – review and editing, supervision. S.E.M. – funding acquisition, conceptualisation, methodology, writing – review and editing, supervision. C.J.H. – funding acquisition, conceptualisation, methodology, investigation, writing – review and editing, supervision.
Funding
This study was funded by the MRC: MR/P012604/1 and Pfizer under the MRC asset-sharing scheme. This study has been delivered through the National Institute for Health and Care Research (NIHR) Oxford Health Biomedical Research Centre (BRC) including the Oxford Health Cognitive Health Clinical Research Facility, and the Oxford Centre for Human Brain Activity part of the Wellcome Centre for Integrative Neuroimaging. The views expressed are those of the author(s) and not necessarily those of the MRC, the NIHR or the Department of Health and Social Care. A.N.d.C. is funded by an NIHR Clinical Lectureship and also receives funding and support from the NIHR Mental Health Translational Research Collaboration Mental Health Mission and the NIHR Oxford Health BRC. She has previously received funding from the Guarantors of Brain and a Wellcome Trust Clinical Doctoral Research Fellowship (216430/Z/19/Z). A.L.G. and M.A.G.M. are also supported by the NIHR Oxford Health BRC.
Declaration of interest
C.J.H. has received consultancy fees from P1vital Ltd., Jannsen Pharmaceuticals, UCB, Compass Pathways and Lundbeck. She is a co-director of TnC Psychiatry and Neuroscience. S.E.M. has received consultancy fees from Zogenix, Sumitomo Dainippon Pharma, P1vital Ltd. and Johnson & Johnson Pharmaceuticals. C.J.H. and S.E.M. recently held grant income from Zogenix, UCB Pharma and Janssen Pharmaceuticals and ADM. C.J.H., S.E.M. and P.J.C. recently held grant income from a collaborative research project with Pfizer. A.L.G. has received consultancy fees from Zogenix and Johnson & Johnson Pharmaceuticals. B.R.G. has received consultancy fees from Tiefenbatcher Pharmaceuticals via Lindus Health Clinical Research Organization. M.A.G.M., M.B., J.S., D.G., W.H. and A.N.d.C. have no declarations of interest. A.N.d.C. and B.R.G. are members of the editorial board of BJPsych; they did not take part in the review or decision-making process of this paper.







 Open access
Open access
eLetters
No eLetters have been published for this article.