


Introduction
Many children have been labeled as allergic to antibiotics, yet almost 95% of these labels are inaccurate. Reference Shenoy, Macy, Rowe and Blumenthal1 Inaccurate allergy labels are a major driver of overuse of broad spectrum antibiotics in children, Reference Hersh, Shapiro, Zhang and Madaras-Kelly2 increasing risk of adverse events. Reference Stone, Trubiano, Coleman, Rukasin and Phillips3 Evaluating and removing inaccurate labels (i.e., delabeling) represents a critical antibiotic stewardship initiative. Reference Shenoy, Macy, Rowe and Blumenthal1,Reference Stone, Trubiano, Coleman, Rukasin and Phillips3 In light of calls to increase antibiotic allergy delabeling in pediatrics, Reference Mitri, Reynolds and Copaescu4 it is critical to understand how parents and caregivers (hereafter caregivers) perceive these efforts and react to tests that contradict their prior beliefs (i.e., indicating no allergy for their child). While prior studies have primarily examined caregiver views of antibiotic allergy labels in clinical contexts, less is known about caregivers’ broader attitudes toward allergy evaluation and their anticipated reactions to negative test results. Reference Carter, Kaman and Baron5,Reference Antoon, Grijalva and Carroll6 Here, we surveyed US caregivers about their preferences for antibiotic allergy evaluation and hypothetical reactions to a negative allergy test for their child.
Methods
The University of Utah Institutional Review Board deemed this study exempt with a waiver of informed consent. From March to April 2024, we recruited a national, nonprobability sample of US adults to an online survey about antibiotics (completion, 1560 of 1738 [89%]), including 356 (22.8%) parents and caregivers of a child younger than 18 years. These analyses are limited to the 37 caregivers reporting a child with an antibiotic allergy (10.4%). Details of the full survey are described elsewhere. Reference Thorpe, Lee and Szymczak7,Reference Thorpe, Lee and Szymczak8
Caregivers answered questions about their child’s allergy (e.g., type, severity), their allergy evaluation preferences (e.g., oral medication vs skin-scratch tests) for assessing whether the child was non-allergic, and their reactions to a hypothetical negative skin-scratch test for the child (Supplement). Descriptive statistics were used to summarize survey answers. Allergy evaluation preferences were compared using McNemar’s test. Tests were 2-sided with α=.05 and calculated using R version 4.2.2. Open-ended responses were reviewed for content.
Results
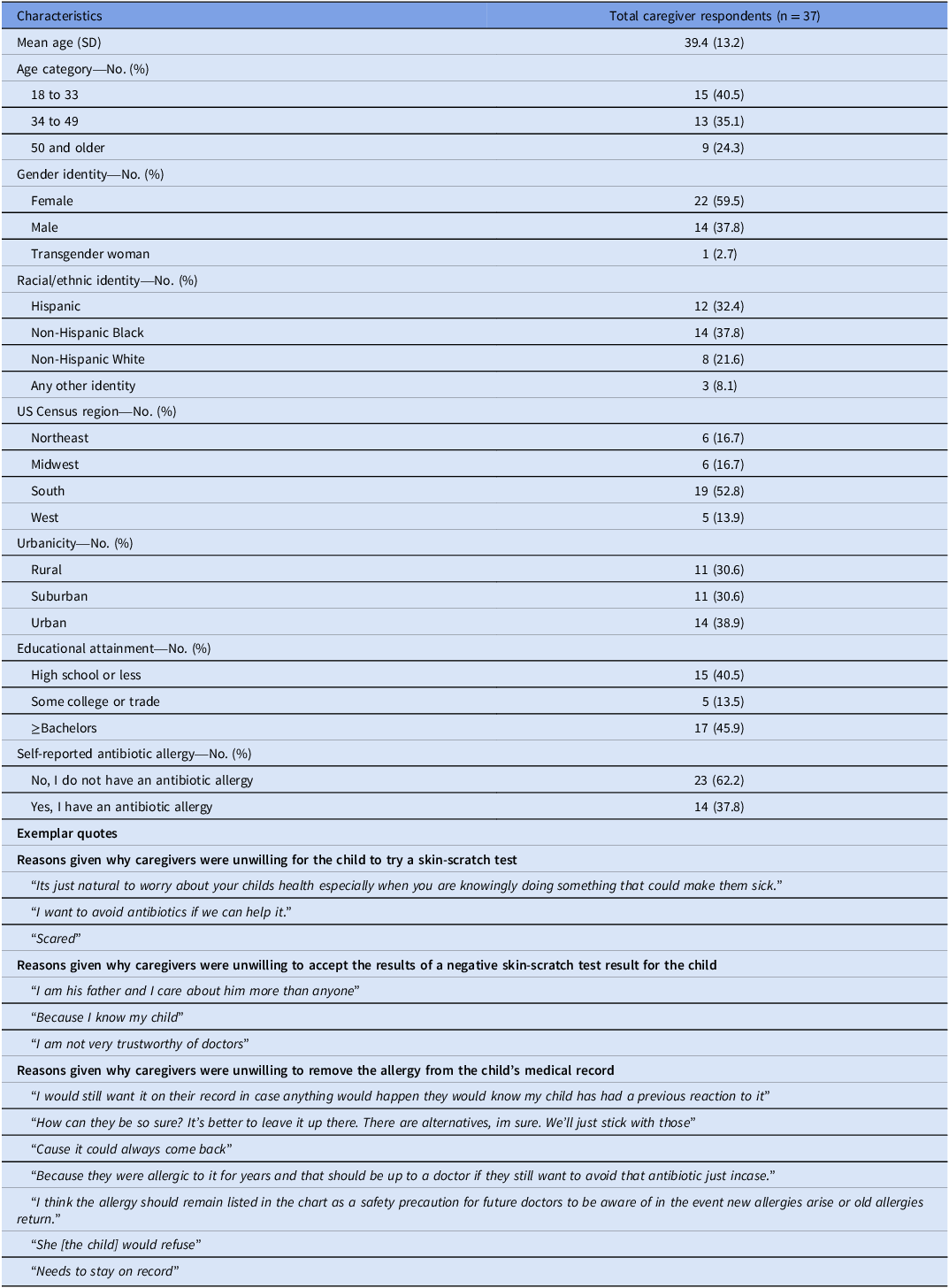
Among the 37 caregiver respondents, the mean (SD) age was 39 (13) years; 22 (59.5%) identified as women (Table 1). Most reported child allergies were to penicillin (27 of 37 [73.0%]) and were described as mild/moderate (31 of 37 [83.8%]). Most caregivers were willing to perform a test for delabeling, with a higher percentage favoring skin-scratch testing (33 of 37 [89.2%]) than oral challenge (26 of 37 [70.3%], P = .02; Figure 1). Yet, 21.6% of caregivers (n = 8) reported they would not accept a negative skin-scratch test result and 29.7% (n = 11) would not agree to remove the allergy from the child’s medical record, particularly for children with mild/moderate allergies (68.4% 13 of 19). Almost all caregivers (35 of 37 [94.6%]) would try to re-add the child’s allergy onto their medical record if removed after a negative test. Caregivers listed various concerns in free-text boxes including fear of harming or distressing the child, negative experiences with antibiotics, and distrust of clinicians (Table 1). Caregivers expressed the sentiment that it was better to be ‘safe than sorry’ (e.g., keeping allergy labels as a safety net in case the allergy returns).
Child allergy characteristics, caregiver willingness to assess whether the child was non-allergic, and reactions to a hypothetical negative test.

Respondent characteristics and exemplar quotes

Table 1. Long description
A table with 12 rows and 2 columns. The first column lists characteristics and the second column provides corresponding data for 37 caregiver respondents. Characteristics include mean age, age category, gender identity, racial/ethnic identity, US Census region, urbanicity, educational attainment, and self-reported antibiotic allergy. Each row provides specific data points for these characteristics. The table also includes exemplar quotes from caregivers explaining their unwillingness for the child to try a skin-scratch test, accept the results of a negative skin-scratch test, and remove the allergy from the child’s medical record.
Discussion
In this online survey of US adults, 22% of caregivers of children with antibiotic allergies would not accept a negative skin-scratch test result for the child, 30% would not agree to remove the allergy from the child’s record following a negative test, and 95% would try to re-add the allergy label if removed. Limitations include self-reported responses to a single scenario, a small sample, and underrepresentation of some populations (e.g., those without internet access).
Caregivers’ concerns about delabeling appeared to be rooted in underlying beliefs about the safety of keeping allergy labels and their responsibility to protect their child. Taken together, our findings suggest caregiver hesitancy may present a major barrier to antibiotic allergy delabeling in pediatric care. Strategies for informing caregivers about the benefits and risks of antibiotic allergy testing and addressing concerns that persist after negative tests are needed to promote optimal antibiotic use following allergy delabeling.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/ice.2026.10510.
Acknowledgments
The views expressed in this paper are those of the authors and do not necessarily represent the position or policy of the U.S. Department of Veterans Affairs or the United States Government.
The content is solely the responsibility of the authors and does not necessarily represent views of the Agency for Healthcare Research and Quality.
Dr. Thorpe had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the analysis.
Study materials are available on the project repository: Thorpe A, Lee RA, Szymczak JE, Fagerlin A, Vaughn VM. Psychological Research Insights for Messaging Effectively About Antibiotics (PRIME). Published Nov 1, 2024.
https://osf.io/h26jp/?view_only;=8b3362ee3cb64f08965ef25474d3af6a
Financial support
This study was funded by internal research funds for participant recruitment provided by the Departments of Population Health Sciences and Internal Medicine at the University of Utah (Dr. Fagerlin’s Jon M. Huntsman Presidential Endowed Chair and Dr. Vaughn’s Internal Research Funds) and the Department of Medicine at the University of Alabama at Birmingham (Dr. Lee’s Internal Research Funds). Dr. Thorpe was supported by an American Heart Association Career Development Award (25CDA1445490). Dr. Szymczak also received support from the Agency for Healthcare Research and Quality (5R01HS029879).
Competing interests
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Role of funder
None.




 Open access
Open access