

Introduction
Sexual harassment of doctors by doctors is ravaging the health care system, especially in developing and low resource countries like Nigeria, where there is a cultural and traditional preference for the male child. I am a victim of sexual harassment at the medical workplace. This has kindled my interest in the topic to investigate this problem in Nigeria. If I have the resources I will fight for the rights of women doctors to help victims of sexual harassment who are doctors. I conducted an international study in 2014 at the Medical Women’s International Association (MWIA) side event during the United Nations Commission on the Status of Women. The result of this pilot survey was presented during the MWIA conference in 2016 in Vienna. The presentation ignited the interest of the then MWIA president to conduct an international study of sexual harassment at the medical workplace, and I was part of the team that conducted the survey. The results of the study have been presented at different MWIA international and regional conferences, including other fora on women. I have also published articles on sexual harassment at the medical workplace titled ‘Sexual harassment at the workplace, an impediment to gender equality, a pilot study’ and ‘Sexual harassment against female residents, the role of hospital administrators and managers’. I suffered career retrogression and would not want anyone to have the same experience as a result of being sexually harassed by a senior colleague.
Gender in Nigerian Society
Nigeria is the most populous black nation in the world, the most populous country in Africa, the third most populous country in the world, and the biggest country in West Africa. (Reference Ogundare1) According to the 2006 population census, Nigeria has a population of 140,431,790 people with 69,086,302 females and 71,345,488 males. Nigeria occupies 923,769 square kilometres, where 909,890 square kilometres makes up the land mass and 13,879 square kilometres are water. (2) It is bounded by the Republic of Benin, Niger, Chad, Cameroon and the Gulf of Guinea. Of the Nigerian population, 17.50% of doctors were women in 2008. (3) The Federal Republic of Nigeria was divided into three divisions as at 1951. (Reference Ayate and Akwa4) These have given birth to thirty-six states with a capital territory at Abuja. Nigeria is also divided into six geopolitical zones namely North-East, North-West, North-Central, South-East, South-West, and South-South zone. Nigeria is a country where about 250 languages are spoken, with English acting as the lingua franca. Pidgin English is a creole language widely spoken in Nigeria, which is English mixed with words from the local languages. The tenses do not follow British, American or Australian English.
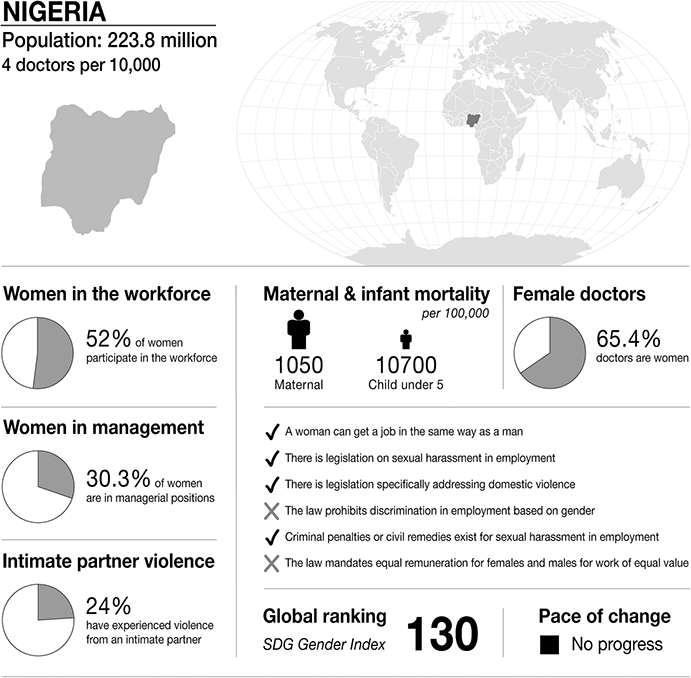
Infographic Nigeria. Infographics were provided by CartoGIS Services, The Australian National University. Population: from World Bank https://databank.worldbank.org/source/population-estimates-and-projections. Sustainable Development Progress, global ranking and statistics on women in the workplace, women in management and intimate partner violence: from United Nations SDGs Data Portal https://unstats.un.org/sdgs/dataportal. Female doctor percentage: from Global health workforce statistics www.who.int/data/gho/data/themes/topics/health-workforce. Legislation and law statements: from the World Bank gender data portal 2023 https://genderdata.worldbank.org/en/indicators. Maternal mortality statistics: from the Global Health Observatory 2020 https://mmr2020.srhr.org. Infant mortality statistics: from United Nations International Children’s Fund (UNICEF) https://data.unicef.org/topic/child-survival/under-five-mortality.

Figure 26.1 Long description
The infographic provides information about Nigeria, with a population of 223.8 million and 4 doctors per 10,000 people. It highlights several gender-related statistics. 52 per cent of women participate in the workforce. 30.3 per cent of women are in managerial positions. 24 per cent of women have experienced intimate partner violence. Maternal mortality is 1050 per 100,000. Infant mortality under 5 is 10700 per 100,000. 65.4 per cent of doctors are women.
The infographic lists the presence or absence of law and policy on gender equality. In Nigeria:
– a woman can get a job in the same way as a man.
– there is legislation on sexual harassment in employment.
– there is legislation specifically addressing domestic violence.
– criminal penalties or civil remedies exist for sexual harassment in employment.
– the law does not prohibit discrimination in employment based on gender.
– there is no law that mandates equal remuneration for females and males for work of equal value.
The S D G Gender Index global ranking is 130, and is stable.
In Nigeria, there is preference for the male child as families will prefer to have a son than a daughter, and this has affected girl-child education. It also affects the training of children, including the way females are treated from cradle to adulthood. Sons are given better feeds as children, and better education and health care. This is a problem where the girl-child may not be given formal education and may not be allowed to attend school. (Reference Tyeakaa, Amaka and Nor5) Some of the reasons for preference for the male child are religious misinterpretations, cultural beliefs, economic crisis, poverty, early marriage and teenage pregnancy. Women are expected to be at home and look after the children. Some people believe that educating a girl is a waste of resources as she will take the education to her husband’s house when she gets married. This is gradually changing as more parents are enrolling their daughters in school. Women are now occupying leadership positions in government. In some Nigerian cultures, women have traditional ceremonies they perform as rites of passage, celebration of womanhood and coming of age of the girl child. An example is the Iria ceremony performed by the Ibani people of Grand Bonny and Opobo of southern Nigeria.
Gender in Medicine
Choosing medicine as a career has increased among Nigerian women, (Reference Amadi6) though some specialties tend to be dominated by men. There remains a large gender difference in the choice of specialty. (Reference Jefferson, Bloor and Maynard7) Traditionally, women have assumed the responsibility for raising families and maintaining the household. (Reference Mobilos, Chan and Brown8) The gender roles defined by Nigerian society may affect the choice of medical specialty.
There are more Nigerian women doctors and medical students compared to earlier years. (Reference Amadi6) According to the Nigerian National Bureau of Statistics in 2015, 2016 and 2017 the proportion of doctors in Nigeria that were females was 34.1%, 34.1% and 34.6%, respectively. (Reference Diderichsen, Johansson, Verdonk, Lagrojanssen and Hanberg9)
Women have occupied leadership positions in health institutions, the Ministry of Health, hospital management boards and also politics both at the state and national levels. Dr Elizabeth Abimbola Oshodi was the first woman to be elected as president of the Nigerian Medical Association in 1988 for the 1988–1990 tenure. The Nigerian Medical Association is the umbrella association of all doctors and dentists practising in Nigeria. Prof Adenike Grange was the first Nigerian woman doctor appointed as a Nigerian minister of health. Other Nigerian women doctors have been provosts of medical colleges, deans and deputy vice-chancellors of universities and deputy governors of Nigerian states. Some of the reasons for the disparity in the proportion of male and female doctors are family and societal norms and beliefs which are being transferred to the health sector. (Reference Abdulgadir10)
Gradually, women doctors are penetrating the highly dominated male medical specialties such as orthopaedics, general surgery, burns and reconstructive surgery, obstetrics and gynaecology and urology. (Reference Amadi6; Reference Jefferson, Bloor and Maynard7; Reference Flyckt, White, Goodman, Mohr, Dutta and Zanotti11–Reference Yusufu, Ahmed, Odigie, Delia and Mohammed16). In Nigeria, females have dominated some specialties such as paediatrics, anesthesiology, internal medicine, ophthalmology, radiology, family medicine and community medicine. This reflects the cultural expectation that women will specialize more in fields of medicine that express the natural caring and nurturing nature of women as related to preventing diseases, helping and taking care of children (Reference Amadi6; Reference Abdulgadir10; Reference Chukwumah and Unweni17). There are few studies on sexual harassment among doctors practising in Nigeria and fewer on how women doctors are affected.
Medical Education
Medical education can be categorized into undergraduate and postgraduate medical education and continuing medical education. (Reference Malu18; Reference Ezeanolue19) Medical schools in Nigeria are known as colleges of medicine, colleges of health sciences or faculties of medicine, and are charged with the responsibility by law to train medical doctors (Reference Malu18; Reference Ezeanolue19) Undergraduate medical education takes six years and is regulated by the National University Commission (NUC) and the Medical and Dental Council of Nigeria (MDCN). (Reference Malu18; Reference Ibrahim20) After graduation, the young medical graduate undergoes internship followed by the National Youth Service Corps (NYSC). NYSC is a one-year compulsory programme which every Nigerian graduate thirty years and under must undergo irrespective of the course of study. Medical residency in Nigeria is largely sponsored by the government as only few missionary and privately owned hospitals offer residency training. Postgraduate academic degrees are awarded by the universities, (Reference Malu18) including postgraduate diplomas in some clinical specialties, for example anesthesiology. Residency training is regulated by the postgraduate medical colleges, which are the National Postgraduate Medical College of Nigeria (NPMCN) and the West African Postgraduate Medical College through its component colleges the West African College of Surgeons and the West African College of Physicians (Reference Malu18; Reference Ezeanolue19). These colleges periodically visit residency training accredited centres and medical colleges to see if they meet the approved guidelines for residency training. On completion of the residency training, the new consultant may be retained in the hospital where the residency training was done or asked to seek a job elsewhere. Junior doctors and medical students are vulnerable at every stage of their training to sexual harassment.
Law
Previously there was no legislation against sexual harassment at the workplace or in educational institutions. However, the National Industrial Court of Nigeria (NICN) in 2017 made an amendment of its civil procedure rules in which provision was made through Order 14, (21) titled ‘Sexual Harassment and Discrimination at the Workplace’. (22; 23) Sexual harassment is defined by the National Industrial Court of Nigeria as consisting physical conduct of a sexual nature, verbal and non-verbal forms of sexual harassment including quid pro quo harassment. (23) In 2019, a bill was proposed by the Nigerian Senate titled ‘Prevention, Prohibition and Redressal of Sexual Harassment in Tertiary Educational Institutions 2019’, which also defines sexual harassment and punishment for offenders if it occurs in higher institutions. (21) The law covers all students in tertiary institutions including medical students. Some medical schools and hospitals have their various guidelines and policies against sexual harassment. In institutions where there is no formal reporting system, the survivor reports to her supervisor, hospital management or authorities of the medical school or files the case in court. The supervisor may be a supervising consultant, head of department, faculty chair, dean, provost of a medical school, director of medical services, chairman of a medical advisory committee, head of a residency training programme or the chief medical director. A panel of enquiry is constituted to investigate the matter and make recommendations. Depending on the petition, the recommendations may or may not be considered by the hospital or medical school.
Medical Regulation
The practice of medicine and dentistry in Nigeria is regulated by the Medical and Dental Council of Nigeria (MDCN). (24) The MDCN ensures that medical and dental practice is conducted in an efficient way in Nigeria, safeguarding the health of its citizens. (Reference Ezeanolue19) Once a medical and dental student graduates from any Nigerian medical school, the new doctor is inducted and a temporary practising licence is issued, which is valid for two years to enable the doctor to practise medicine and dentistry as an intern under the tutelage and supervision of a consultant. At the end of the internship, the doctor applies to the MDCN, submitting the necessary assessment forms duly signed by the supervising consultants and the head of the hospital, which is the medical director or chief medical doctor of the hospital. Then a permanent practising licence is issued, which is renewed annually after attending the prescribed continuing medical education units. Medical and dental graduates from foreign universities sit for an examination conducted by the MDCN to enable them to practise in Nigeria.
The MDCN has published the ‘Code of Medical Ethics in Nigeria’, which guides medical practice in the country. (Reference Nwaohuocha25) Members of the public who feel aggrieved by any professional misconduct can report to the hospital management, the MDCN or the Nigerian Medical Association (NMA). If a report is made to the MDCN, a panel sits to investigate the allegation. Depending on the offences, the erring doctor may be suspended from medical or dental practice for a stipulated period of time or have his or her name permanently struck from the MDCN register.
Different hospitals have different policies and guidelines for disciplining erring doctors. A panel is set up to investigate any petition of misconduct and recommendations made to the hospital management. Punishments of doctors found guilty include apology to the patient, suspension for a number of months during which the salary of a doctor is withheld, removal from the workplace, and issuance of a query or warning letter. However, the health care sector includes a number of people and organisations with different expectations, opinions and backgrounds. Therefore, sometimes doctors who behave unprofessionally may be cautioned without any formal letter by their supervisor or fellow colleagues.
Case Study
Prelude
This case study involved interviewing a survivor of sexual harassment in which the perpetrator is a male doctor in a Nigerian teaching hospital. The survivor describes in her words what made her vulnerable:
I am single and generally in our society people look at single women as weak that can be humiliated as there is no one to speak for them. They are also seen as failures.
She identified single women in Nigeria as vulnerable to humiliation in the family, at the workplace and also in the community. Also, being a junior doctor is another factor of vulnerability to sexual harassment at the workplace. She was even confronted by male and female colleagues that she should deny the harassment and be quiet.
Assault
Dumebi is a female ophthalmology resident doctor at a Nigerian teaching hospital. She was happy about her job and was carrying out tasks assigned to her dutifully. In the department, they work in teams comprised of registrars, senior registrars, and consultants. When she joined the department, there was a senior registrar named Tosan who travelled to the United Kingdom for subspecialty training in a field whose training was not available in Nigeria. Tosan’s course lasted for six months, and he had already spent three months in the United Kingdom before Dumebi joined the faculty. Dumebi had not passed the primary examination which is the entry requirement for residency training in the postgraduate medical colleges in Nigeria.
Three months after Dumebi joined the department, Tosan returned from the United Kingdom. One day Dumebi and Tosan met at a taxi rank on their way to work and boarded the same taxi to work. While in the taxi they exchanged pleasantries and were engaged in a conversation. Tosan told Dumebi about a regional conference scheduled later that year overseas with sponsorship from the government. Dumebi told Tosan she was not interested as she just joined the department and was still familiarizing herself with the specialty and learning its rudiments. Tosan pressurized Dumebi to send a text message to the consultant in charge coordinating the trip and he forwarded the consultant’s number to Dumebi. After much pressure, Dumebi sent a text message to the coordinator of the trip. Tosan never mentioned to Dumebi that she would have to repay him after the conference.
One day, Tosan asked Dumebi for her USB drive, saying that he wanted to give her some academic resources to enable her to pass her residency primary examination. Dumebi gave Tosan her USB drive, and Tosan returned it back with his own USB drive of a higher capacity, as Dumebi’s could not contain all the resources. Dumebi thanked Tosan and took both drives, returning Tosan’s equipment in the next couple of days.
After the conference, Tosan started making sexual advances at Dumebi which she turned down, but he persisted. Tosan told Dumebi she had to pay him back for informing her about the conference. Tosan later reported Dumebi to their faculty chair, stating that Dumebi was disrespecting him. At this time, Dumebi had been sent for a three-month rotation in the surgery department and had been there just one week. Dumebi was recalled from her surgery rotation and told that a panel would be set in the department to investigate the issue. Dumebi was never sent back to complete her rotation in the surgery department.
At this time, Tosan was a candidate for the position of president of the junior doctors association of the hospital. Dumebi informed the association about what was going on. Her fellow junior doctors, both male and female, forced her to withdraw her complaint. Tosan sent a text message to Dumebi which read: ‘I do not think that life is all about squabbles. I still wonder why you would want to ridicule me.’ After some time, Dumebi’s name was removed from the departmental duty roster. Queries were issued to Dumebi titled, ‘insubordination to superior authority’, and a letter requesting Dumebi to seek medical help and send a report that she was medically fit. Dumebi had a mentor in the hospital who was a consultant in another department. One of the consultants in the hospital who was part of the hospital management committee sent Dumebi’s mentor a text message which reads: ‘Thank you madam good morning, please can you confirm if your girl Dr Dumebi has started treatment’. At this time, Tosan won his election and became president of the junior doctors’ association.
There was an offer for the purchase of land. Dumebi was interested and submitted the necessary documentation. After paying for the land, Tosan refused to give proper documents to Dumebi as her name was written in initials in the deed of conveyance. When Dumebi requested Tosan to write her name in full and not in initials; he refused. Instead he sent a text message to Dumebi: ‘Who knows why all the typists make the same mistake in your name. I did the right thing for all the allottees but the evil in your heart will not allow you to know good. Posterity will judge me but the evil in your heart must hunt you for life.’
Limbo
The survivor in this case never had the intention of reporting; worse is that there was no formal reporting system nor policies against sexual harassment in the hospital. This is an interesting case because usually it is the victim that reports first, but here the perpetrator reported that his victim was disrespecting him. When Dumebi was reported by the perpetrator, a panel was set up in the department to investigate the issue and it included both a male and female consultant. She and the perpetrator were interviewed separately and later together. At the end of both sessions, Dumebi was told that what she was claiming never happened as she had no evidence and was just making up stories against her perpetrator. Before then the perpetrator told Dumebi that once they got into the panel, she should start apologizing to him. The survivor said she was strong enough to face whatever it is as she will not give into any pressures mounted on her. A second panel was also set up by the hospital management, made up of professors and doctors from other departments. She attended the panel, but the recommendations of the two panels were never communicated to her. In her own way, she met with several senior doctors to intervene in the matter, but nothing was done.
Exposure
This case was different as her name was known from the beginning. There were a lot of gossips and false accusations as a result of the sexual harassment. Even a female ophthalmology senior registrar told the survivor that she was the cause of the sexual harassment and should apologize to the perpetrator. Reporting to female doctors did not save the situation as they all supported the perpetrator. She was never concerned about the grapevines (gossips and rumours at the workplace) as they are common in any workplace. Dumebi never blamed herself for what happened as she never saw anything wrong with her action. The only thing she thought was wrong is that she should not have given in to the pressure mounted on her by the perpetrator to joining the trip for the overseas conference, as there are two Nigerian proverbs that say, ‘free things can purge the stomach’ and ‘nothing goes for nothing’. She never argued with anyone since within her she knew she was sexually harassed even though she never saved all the discussions and text messages received from Tosan. She kept her cool and encouraged herself.
Aftermath
The abuse that occurred impacted on the personal and professional life of the survivor positively and negatively. The impact was positive on her personal life as she leant not to be subject to any form of pressure especially when it is coming from the opposite sex and someone of a higher cadre. She also learnt to avoid receiving favours that she does not merit as it may be bait. In this case, if she had not attended the conference, the perpetrator would not have had any opportunity of asking her for payback. The negative impact was that she was not allowed to complete her residency training in her specialty of choice. She experienced career retrogression and was tagged a ‘troublemaker and troublesome person’. It did not bother her. She is still a medical doctor practising her profession in another hospital. She was able to recover fully and never had any emotional and psychological breakdown because she never allowed it to disturb her and she self-encouraged herself. She had the will power and determination to become an ophthalmologist. Her incident became an eye opener in the first hospital where she worked, as other male doctors were surprised that with everything done to Dumebi, she never compromised her integrity, morality and self-esteem. She hopes to write a report about her experience to the United Nations to bring this problem to light, so that an international day can be dedicated to sexual harassment at the workplace. She also wishes to have a movement and foundation to help women doctor victims of sexual harassment by providing counselling and legal protection, and by helping them secure residency placement elsewhere if necessary. A part of her plans is to provide stipends to other victims if their salaries are stopped or their appointment terminated.
Discussion
In Nigeria generally, women are blamed if they are single as they are seen as being wayward with a bad character: that is why no man has taken her as his wife. Worse is if the female is a professional, for example a medical doctor. She is viewed as being choosy, selecting and setting high standards for suitors. Nigerian single women have been discriminated and stigmatized against in their families, at the workplace, in religious places and in the community, including doctors, as generally in Nigeria, marriage is viewed as a benchmark for measuring the decency of women. (Reference Nwaohuocha25) There are three groups of single women: the never married, the divorced and the widowed. The never married is the worst hit with discrimination and sexual harassment – including women doctors. It is considered abnormal in Nigerian society if a woman, even if she is a doctor, is still single beyond the conventional age considered for marriage in Nigeria. (Reference Ntoimo and Isingo-Abanihe26) In this case, this puts the woman at risk of sexual harassment at the workplace as she is seen as someone without a helper. She can be discriminated against and stigmatized by both male and female doctors. It is worse that even older single women doctors will also stigmatize and discriminate against a younger single female doctor. For instance, in the case discussed, the survivor was not protected by her fellow female colleagues. Even when she told a female professor who is also a doctor about what happened, the first question she asked the survivor was, ‘why are you not married?’ One begins to wonder if marital status is now a criterion for jobs at the medical workplace. Another woman doctor told the survivor that she knows the perpetrator very well, that he is a married man, and that she knows his wife and that therefore he cannot woo another woman. Even when panels are sent to investigate allegations of sexual harassment in Nigeria, if the victim is single most times the panel will start asking the victim why she is single, stating that it is man’s world, and intruding into the victim’s private life, asking questions like, ‘Are you engaged? Are you in a relationship? What happened in your last relationship? Are your parents or family worried that you are not yet married? Is there any other doctor or man in the hospital wooing you?’ She may even be told that she should be happy that a man is wooing her, that she should not see the harassment as unwelcome.
Job and work stress is a consequence of sexual harassment. Doctors are dealing with the lives of other people, hence when a survivor is experiencing job and work stress from sexual harassment by a male doctor it endangers the lives of her patients. She is at risk of making medical errors that can lead to wrong diagnosis or management, which can lead to accusations of negligence. Litigation may also be filed against her. Stress related to work impacts on the health of the woman doctor due to its psychosocial risks, and this affects the woman doctor herself and her family. (Reference Nkporbu and Douglas27) Trainers subject trainees to various forms of bullying. (Reference Yusufu, Ahmed, Odigie, Delia and Mohammed16) There is no protection for the trainees as it is the trainers that constitute panels of enquiry for sexual harassment, and it is also they who are the policy makers in the hospital and medical schools.
Due to various cultural norms and beliefs in Nigeria, women, including doctors, are held down from reaching their full potential or achieving the aspirations that they have in life. (Reference Abara28) Women are sexually harassed wherever they are. This is always influenced by culture. (Reference Abara28) Sexual harassment has a lot of organizational effects on women as it affects their career path and progression. (Reference Akinfala and Tuned29) The Nigerian traditions and customs discourage women doctors affected by sexual harassment from speaking out. (Reference Johnson30) Sexual harassment in the medical workplace is professional misconduct and a serious problem. It is a display of power. The victim/survivor is usually a subordinate to the perpetrator. The perpetrator is usually a male and a person of authority or someone higher in the hierarchy than the survivor. (29) Sexual harassment at the workplace is an impediment to gender equality in the medical community.
Current Situation in Nigeria
Culture affects the way women are treated wherever they are. Survivors of sexual harassment should have self-encouragement and strong self-esteem. They should not rely on anyone as even female doctors cannot be trusted when it comes to issues of sexual harassment. They should not allow the incident to disturb them emotionally and psychologically. They should develop deaf ears to all grapevines (gossips and rumours) in the hospital about the matter.
Sexual harassment at the workplace leads to a hostile work environment and career stagnation. This takes different forms, which includes retaliation, false allegations, demotion and stigmatization. One of the barriers to getting justice for sexual harassment is the stigmatization that follows it. In this case study, some women doctors approached the survivor, forcing her to keep quiet. Some were even angry with the survivor, saying that she was making false accusation against the perpetrator, that it is a common thing that happens at the medical workplace, and therefore there is nothing wrong even if it ever happened, as it is a normal thing for men to flirt even with their subordinates at the medical workplace and male doctors are not exceptions. As the perpetrator is a married man, letting people know about the incident may get to the ears of his spouse, and therefore it may disturb his marriage. A female consultant who was a member of one of the panels of enquiries told the survivor that she wants to put fire into another woman’s marriage. One begins to wonder if the survivor invited another woman’s husband to sexually harass her, yet she is blamed for being sexually harassed. Survivors do not report because they are ashamed and afraid of termination of their appointment if the incident of sexual harassment is reported to the hospital management and medical school authority. (Reference Johnson30) The case discussed is different as it was the perpetrator that reported his victim to a higher authority; this shows the level of injustice women doctors get when they are victims of sexual harassment.
Directions to Prevent Sexual Harassment in the Nigerian Health Sector
Strategies can be taken to prevent and manage sexual harassment of female doctors by male doctors in the Nigerian medical workplace:
1. A formal reporting system in all health institutions and medical schools with an office in the Federal Ministry of Health and Women’s Affairs dedicated to sexual harassment, where women can lodge such complaints. The Ministry of Justice should also provide legal aid to survivors. This will encourage survivors to come forward and lodge their complaints.
2. Establishment and implementation of policies against sexual harassment at the medical workplace and in medical schools to protect women doctors and female medical students.
3. Panels set up to investigate allegations of sexual harassment of doctors by doctors should have no bias. There should be justice. Survivors should be protected from any form of retaliation, victimization and discrimination, including making employment decisions and benefits dependent on unwelcomed sexual activity.
4. Perpetrators should also be disciplined appropriately no matter their rank or the position they occupy in the hospital.
5. Policies and strategies should be established against trainer–trainee bullying in all health institutions and medical schools irrespective of whether they are accredited for residency or not, to protect junior doctors, especially women doctors, resident doctors and early career doctors, from any form of trainer–trainee bullying by doctors.
6. Counselling should be made available for survivors who develop emotional and psychological breakdown following incidents of sexual harassment.
Recommendations
Various stakeholders in the health sector have roles to play in the management and prevention of sexual harassment against medical practitioners. This includes:
Supervisors and consultants
Hospital management, which includes the hospital management board, primary health care board and the hospital management committees
Heads of departments, deans, provosts of medical colleges and faculty chairs
The Nigerian Medical Association
The Medical Women’s Association of Nigeria
The National Association of Resident Doctors of Nigeria (NARD), which is the association of early career doctors/junior doctors in Nigeria.
Conclusion
Sometimes the survivor may consider quitting her job, especially due to the rumours and gossip that will be going on about her within the medical community. The survivor may also be at risk of demotion or dismissal and may not be allowed to attend conferences or update and refresher courses, including being sent for special rotations in other departments and hospitals required for the specialty by the postgraduate medical college that will qualify her to write the residency training examinations. The survivor may never get justice, as she may even be asked to refute the claims and apologize to her perpetrator. Strategies should be put in place by hospital managements and medical school authorities to prevent reoccurrence.

 Open access
Open access