


1. Introduction
While health technologies aim to improve patients’ health, it is increasingly acknowledged that their impact may extend beyond the patient. These effects are also known as spillover effects (Al-Janabi et al., Reference Al-Janabi, van Exel, Brouwer and Coast2016a; Mendoza-Jiménez et al., Reference Mendoza-Jiménez, van Exel and Brouwer2024). Patients' health may, for instance, affect the health of people in their network indirectly through the burden of providing informal care – the ‘caregiving effect’ – but also directly through anxiety or grief from the health prospects of a loved one – the ‘family effect’ (Bobinac et al., Reference Bobinac, Van Exel, Rutten and Brouwer2011). In addition, the death of a patient may affect the health and well-being of their loved ones directly through bereavement (Stroebe et al., Reference Stroebe, Schut and Stroebe2007).
In the UK, more than 9.3 million people (14.2 per cent of the population) together provided approximately 9.5 billion hours of informal care in 2016, which averages at 19.7 h per week (Pena-Longobardo and Oliva-Moreno, Reference Pena-Longobardo and Oliva-Moreno2021). More than 70 per cent of these carers reported feeling tired and 60 per cent reported feeling stressed due to providing care (Adult Social Care Statistics Team, 2022). The burden of caregiving is associated with the health status of patients (e.g. Van Exel et al., Reference Van Exel, Scholte op Reimer, Brouwer, van den Berg, Koopmanschap and van den Bos2004; Chiao et al., Reference Chiao, Wu and Hsiao2015). Interventions that improve patient health can also reduce the volume and gravity of informal care patients require and, therefore, reduce the burden for carers. As such, interventions aimed at improving patient health can also impact patients' carers. Considering the various impacts of patient health not only on informal carers, but also on others, taking spillover effects into account in economic evaluations of new health technologies and subsequent funding decisions seems relevant from both a societal and healthcare system perspective (Brouwer, Reference Brouwer2019; Henry et al., Reference Henry, Al-Janabi, Brouwer, Cullinan, Engel, Griffin, Hulme, Kingkaew, Lloyd, Payakachat, Pennington, Peña-Longobardo, Prosser, Shah, Ungar, Wilkinson and Wittenberg2024). After all, if the aim of a healthcare system is to maximise population health from a given budget, this should also assess the health of those experiencing health effects as a direct or indirect consequence of changes in patients' health. In this paper, the focus is on including the health effects for informal carers in economic evaluations.
In a systematic literature review, Krol et al. (Reference Krol, Papenburg and Van Exel2015) found that including informal care in cost-effectiveness analyses can influence the incremental cost-effectiveness ratio (ICER) significantly (Krol et al., Reference Krol, Papenburg and Van Exel2015). A more recent systematic review of UK cost-utility analyses (CUAs) conducted between 1999 and 2021 showed that ICERs were mostly lower when spillover effects on carers were included (Scope et al., Reference Scope, Bhadhuri and Pennington2022). This review further showed that the methods used to include carer health-related quality of life (carer HRQoL) in economic evaluations varied considerably and argued for more consistency in methodology. A systematic literature review showed that only a few CUAs included family spillover effects, and also showed that applied methodologies varied substantially between included studies (Lamsal et al., Reference Lamsal, Yeh, Pullenayegum and Ungar2024). Again, the authors concluded that more guidance is needed on how to include spillover effects in economic evaluations.
Although including carer HRQoL effects in economic evaluations was mentioned by the National Institute for Health and Care Excellence (NICE) in its methods guide for health technology evaluation in 2013 (National Institute for Health and Care Excellence, 2013), it was not specified how to include carer HRQoL effects. To inform revisions of the NICE guidelines, various Task & Finish Groups were established in 2020 in different methodological areas (Dawoud et al., Reference Dawoud, Lamb, Moore, Bregman, Rupniewska, Paling, Wolfram, Lovett and Dent2022). One such group, the Health-Related Quality of Life Task & Finish (HRQoL T&F) Group, provided input on the inclusion of carer HRQoL, and proposed a set of minimum evidence standards (MES) for considering carer HRQoL in appraisals (National Institute for Health and Care Excellence, 2020). Their MES summarise the type of evidence that might be useful, such as published carer burden studies, and suggest that carer HRQoL should be measured using EQ-5D for consistency with patient HRQoL data and comparability among appraisals. Additionally, the MES suggest that carer HRQoL effects should only be considered for the ‘primary carer’ and that family and bereavement effects should not be included in economic models.
These MES were consulted for the most recent NICE methods guide published in 2022 (National Institute for Health and Care Excellence, 2022), but were not integrated in the guidelines because information was considered still incomplete (Dawoud et al., Reference Dawoud, Lamb, Moore, Bregman, Rupniewska, Paling, Wolfram, Lovett and Dent2022). The methods guide states that ‘all relevant health effects, whether for patients, or, when relevant, other people (mainly carers)’ should be included. The methods guide further states that ‘evidence should be provided to show that the condition is associated with a substantial effect on carer's health-related quality of life and how the technology affects carers’, but without specifying what is considered ‘substantial’. This could, e.g. refer to a certain minimum absolute effect on carers, but also to a relative effect on carers compared to the effect of the intervention on patients. The methods guide also does not provide guidance on how effects on carers (or others) should be included. Considering the relevance of including carer HRQoL in economic evaluations combined with the lack of methodological guidance for when and how to do so, this paper addresses two questions by examining past appraisals and available literature on the topic. First, when is inclusion of carer HRQoL justified and how could inclusion be substantiated? Second, how should carer HRQoL be measured and included in health economic models? The UK makes an interesting case study for three reasons. First, while NICE guidelines allow for the inclusion of carer HRQoL in economic evaluations, carer HRQoL is included in only a small proportion of appraisals (Scope et al., Reference Scope, Bhadhuri and Pennington2022). It can be helpful for future submissions to investigate these cases and determine which factors can enhance the chances for acceptance of inclusion of carer HRQoL. Second, previous appraisals are readily available on NICE's website in English language. Third, NICE's eminent position in the health technology assessment (HTA) landscape results in their methodologies and assessments having a global impact, both through NICE and NICE Decision Support Unit guidance, and because global health economic models are frequently designed for implementation in the UK and country adaptations consequently build on modelling choices made for the UK.
2. To what extent has carer HRQoL been included in recent appraisals?
To answer the two research questions, it is important to know to what extent carer HRQoL has been used in prior appraisals in the UK. In this respect, prior to the 2022 publication of the NICE methods guide, Pennington (Reference Pennington2020) reviewed NICE appraisals from NICE's website inception in 2000 to January 2019 for the inclusion of carer HRQoL in economic evaluations (Pennington, Reference Pennington2020). For this purpose, Pennington first searched the final appraisal determinations (FADs for all technology appraisals [TAs]) and final evaluation documents (FEDs for all highly specialised technologies [HSTs]) for the terms ‘carer’ and ‘caregiver’. Subsequently, those FADs and FEDs that included carer or caregiver were screened for eligibility (step 2) and final inclusion of carer HRQoL in the CUA (step 3). Table 1 summarises the results of Pennington's review and also provides an update of the same review until March 2022, performed for this current study and using the same methodology. A PRISMA flow diagram of the updated review is presented in Figure 1. Pennington showed that 3 per cent (12/414) of TAs and 50 per cent (4/8) of HST evaluations included carer HRQoL (as submitted by the company). Since then, the proportion of appraisals that included carer HRQoL has increased (6 per cent [13/226] of TAs and 78 per cent [7/9] of HST evaluations). Also, carer HRQoL was more often included in base-case analyses rather than scenario analyses, indicating a growing role of carer HRQoL in NICE appraisals. Similar to the Pennington review, the appraisals that include carer HRQoL predominantly concern orphan indications, paediatric populations, and/or neurological conditions. Since the Pennington review, when all HRQoL estimates originated from published sources, 35 per cent of submissions used de novo estimates (either from EQ-5D or vignette studies). Carer HRQoL was most commonly included in economic models by linking carer disutilities to patient health states.
Carer HRQoL in NICE appraisals

HRQoL, health-related quality of life; QALY, quality-adjusted life years.
a Since inception of NICE website.
b Proportion of total appraisals.
c Proportion of appraisals that included carer HRQoL.
d Some proportions do not add to 100 per cent due to rounding.
PRISMA flow diagram.

3. When should carer HRQoL be included in economic evaluations?
Including carer HRQoL in economic evaluations was found to be supported by public preferences in the UK, although the public gave less weight to HRQoL effects in carers than in patients (Al-Janabi et al., Reference Al-Janabi, Wittenberg, Donaldson and Brouwer2022). Inclusion can be justified on several grounds, regardless of the perspective of the economic evaluation (e.g. healthcare or societal). From an efficiency argument, all health effects of interventions are important, including effects on others than the patient (Brouwer, Reference Brouwer2019). In addition, there is an equity argument for including these broader health effects, as carers are more frequently female and often have lower socio-economic status (Pena-Longobardo and Oliva-Moreno, Reference Pena-Longobardo and Oliva-Moreno2021). Moreover, as society expects people in the network of the patient to contribute to their care, the impact on the health of carers and any spillover effects should be monitored and considered in HTAs, particularly if these effects are substantial. This may be especially relevant in situations where patients require higher levels of assistance, e.g. when a large proportion of patients receives informal care, caregiving time is substantial or multiple carers are involved. Therefore, the relevance to consider carer HRQoL might be dependent on the therapeutic indication or the context in which care is required, and interventions can impact carer HRQoL through various mechanisms (Al-Janabi et al., Reference Al-Janabi, McLoughlin, Oyebode, Efstathiou and Calvert2019). For instance, providing care to your elderly partner might be considered a normal part of life, whereas providing care to your seriously or chronically ill child is not. On the other hand, considering carer HRQoL might be less relevant when there is no plausible treatment effect on carers, either directly or indirectly (i.e. when there is no clear relation between patient health and carer HRQoL) or in populations with limited social networks, but these situations are likely to be the exception rather than the rule. Hence, while theoretically the consideration of carer utilities is always justified, and preferred for reasons of efficiency, equity, and comparability, the relevance of its inclusion may be limited if the treatment effect on carer HRQoL is expected to be negligible. The relevance of including carer HRQoL should therefore be weighted against the burden of collecting data in carers.
When values or assumptions are uncertain or of disputable quality, NICE might question the appropriateness of including carer HRQoL. In one instance (TA738), the Evidence Review Group (ERG) expressed doubts on the clinical plausibility of the values and the poor reporting of the methods. In such cases, values from high-quality de novo studies and literature (including previous appraisals) can be argued to best substantiate the clinical plausibility of the proposed approach. Focus should be on the plausible causal link between the intervention and carer HRQoL, and on the plausibility of the magnitude of the carer impact relative to the patient impact.
The distinction between the caregiving effect (i.e. the indirect effect of providing informal care on carer HRQoL) and the family effect (i.e. the direct effect of having an ill family member on carer HRQoL) is important to consider when determining the effects on carers (Bobinac et al., Reference Bobinac, Van Exel, Rutten and Brouwer2010). The HRQoL T&F Group proposed not to consider family effect in economic evaluations since evidence in this area is scarce. The NICE methods guide does not specifically exclude non-carers from the evaluation, although it mentions that ‘other people’ affected by the intervention are mainly carers. However, excluding family effects could mean that a real and substantial effect is not accounted for in appraisals. Moreover, previous studies showed that disentangling the carer and family effects is complicated (Bobinac et al., Reference Bobinac, Van Exel, Rutten and Brouwer2010; Hoefman et al., Reference Hoefman, Van Exel and Brouwer2013), making guidance to exclude family effects – which may also occur in informal carers, next to the caregiving effect – challenging to implement in practice.
4. How should carer HRQoL be measured and included in health economic models?
4.1 Prospective measurement using existing measures
There is an abundance of instruments available for measuring the impact of providing care on carers’ lives (Deeken et al., Reference Deeken, Taylor, Mangan, Yabroff and Ingham2003; Hoefman et al., Reference Hoefman, Van Exel and Brouwer2013; Mosquera et al., Reference Mosquera, Vergara, Larrañaga, Machón, Del Rio and Calderón2016; McLoughlin et al., Reference McLoughlin, Goranitis and Al-Janabi2020). These include disease-specific and generic measures of carer outcomes, and also generic measures of (non-carer specific) outcomes. Disease-specific, like the C-DEMQOL for carers of people with dementia (Brown et al., Reference Brown, Page, Daley, Farina, Basset, Livingston, Budgett, Gallaher, Feeney, Murray, Bowling, Knapp and Banerjee2019), CAREQOL-MS for carers of people with multiple sclerosis (Benito-León et al., Reference Benito-León, Rivera-Navarro, Guerrero, de las Heras, Balseiro, Rodríguez, Belló and Martínez-Martín2011), and carer-specific instruments, like the caregiver strain index (CSI) (Robinson, Reference Robinson1983) and Self-Rated Burden (SRB) scale (Van Exel et al., Reference Van Exel, Scholte op Reimer, Brouwer, van den Berg, Koopmanschap and van den Bos2004), may have the advantage of being more sensitive to context-specific effects but complicate the comparison of effects across contexts and the incorporation of effects in economic evaluations (Hoefman et al., Reference Hoefman, Van Exel and Brouwer2013). Generic measures of HRQoL, like the health utilities index (Horsman et al., Reference Horsman, Furlong, Feeny and Torrance2003) or the EQ-5D (Brooks, Reference Brooks1996), which is NICE's preferred measure for patient HRQoL (National Institute for Health and Care Excellence, 2022), facilitate the aggregation of carer and patient effects and inclusion of these effects in an ICER. The use of the same outcome measure for patients and carers has also been advocated by the Spillovers in Health Economic Evaluation and Research Task Force (Henry et al., Reference Henry, Al-Janabi, Brouwer, Cullinan, Engel, Griffin, Hulme, Kingkaew, Lloyd, Payakachat, Pennington, Peña-Longobardo, Prosser, Shah, Ungar, Wilkinson and Wittenberg2024). However, such generic measures have been argued to lack sensitivity to capture effects relevant to carers, although empirical evidence is mixed (e.g. Bhadhuri et al., Reference Bhadhuri, Jowett, Jolly and Al-Janabi2017; Reed et al., Reference Reed, Barrett, Lebrec, Dodel, Jones, Vellas, Wimo, Argimon, Bruno and Haro2017; McLoughlin et al., Reference McLoughlin, Goranitis and Al-Janabi2020; Valcárcel-Nazco et al., Reference Valcárcel-Nazco, Ramallo-Fariña, Linertová, Ramos-Goñi, García-Pérez and Serrano-Aguilar2022). A recent qualitative study showed that although the error rate of EQ-5D is low, carers prefer a care-related QoL measure (McLoughlin et al., Reference McLoughlin, Goranitis and Al-Janabi2023). These broader care-related QoL measures, such as the ASCOT-Carer, CarerQol, or Carer Experience Scale (Brouwer et al., Reference Brouwer, Van Exel, Van Gorp and Redekop2006; Al-Janabi et al., Reference Al-Janabi, Coast and Flynn2008; Rand et al., Reference Rand, Malley, Netten and Forder2015), are argued to be more sensitive for use in carers. These instruments generate preference-weighted scores (in contrast to carer-specific instruments like CSI and SRB), allowing for comparisons of carer experiences across diseases and caregiving contexts. However, these measures do not generate utility values in terms of quality-adjusted life years, as measured from patient HRQoL instruments, necessary for economic evaluations. Lacking utility values hampers aggregation with patient health effects and their use in economic evaluations of patient interventions. Exchange rates between care-related scores and EQ-5D utilities have been estimated in an exploratory UK study, but these are still of limited use due to methodological issues (Dhanji et al., Reference Dhanji, Brouwer, Donaldson, Wittenberg and Al-Janabi2021). Alternatively, generic measures of well-being could be used for measuring the effects on carers and family members. For example, a recent study demonstrated the construct validity of the EQ Health and Well-being in a sample of informal carers (Kuharic et al., Reference Kuharic, Mulhern, Sharp, Turpin and Pickard2024). Although these are conceptually the broadest measures, including them in economic evaluations would only work if effects in patients are also measured in well-being terms, which currently is not common practice. Therefore, to facilitate combining patient and carer utility values on the benefit side of economic evaluations, the use of EQ-5D for measuring carer HRQoL appears to be the most successful strategy in the UK context. This is substantiated with the conclusions of McLoughlin et al., stating that EQ-5D(−5L) is a valid outcome measure when the focus of economic evaluations is on health maximisation (McLoughlin et al., Reference McLoughlin, Goranitis and Al-Janabi2020). Likewise, Bhadhuri et al. (Reference Bhadhuri, Jowett, Jolly and Al-Janabi2017) concluded that EQ-5D is a valid measure for incorporating carer HRQoL impacts in economic evaluations (Bhadhuri et al., Reference Bhadhuri, Jowett, Jolly and Al-Janabi2017).
Pennington's review of NICE appraisals (Pennington, Reference Pennington2020) and its update showed that most evaluations that included carer HRQoL used EQ-5D to measure carer HRQoL or derived estimates based on mapping of, or assumptions on, EQ-5D values (Table 1). Use of EQ-5D is also in line with HRQoL T&F Group's proposed MES (National Institute for Health and Care Excellence, 2020).
Primary data collection is preferred to obtain EQ-5D estimates in carers because this ensures that the carer population corresponds to the indication and intervention of interest. It also enables necessary subgroups (e.g. patients' health states) to be studied, although stratification for subgroups may require larger sample sizes. However, depending on the indication and the intervention, primary data collection may be difficult. Carers are not always easy to identify or reach and completing a survey might be burdensome for them next to the caregiving tasks and their other responsibilities (Whitebird et al., Reference Whitebird, Kreitzer, Lewis, Hanson, Crain, Enstad and Mehta2011; Horrell et al., Reference Horrell, Stephens and Breheny2015).
In recent cases, concerns for of including carer HRQoL in the base-case analysis by NICE has often focused on the (perceived) low quality and uncertainty of the evidence, including the clinical plausibility of (de novo) values (e.g. TA748, TA754), the magnitude of effects (e.g. TA738, TA753, TA754), number of caregivers (e.g. TA753), and proportion of patients receiving care (e.g. TA748), leading to rejection of inclusion of carer HRQoL as modelled in the base-case analysis. This highlights the importance of robust studies.
4.2 Measurement when EQ-5D data cannot be collected
There are some alternatives to collecting primary EQ-5D data in carers. One frequently used option is a vignette study, in which (hypothetical) health state descriptions or scenarios are used to obtain HRQoL estimates (Matza et al., Reference Matza, Stewart, Lloyd, Rowen and Brazier2021). The descriptions are informed by expert input (e.g. patients, carers, clinicians) and valued in a preference elicitation task. A disadvantage of vignettes is that they are not able to fully reflect patient experiences in each state, and therefore are inferior to primary EQ-5D data in eliciting patient HRQoL for NICE submissions (Brazier and Rowen, Reference Brazier and Rowen2011); the same applies for carer HRQoL estimates. Nonetheless, a vignette study is convenient, as it does not require direct measurement of carer-level data. This may particularly be an advantage in subgroups where data collection is challenging, e.g. for practical or ethical reasons (e.g. rarely occurring health states, paediatric indications, end-of-life health states) (Matza et al., Reference Matza, Stewart, Lloyd, Rowen and Brazier2021). Also, vignettes allow assessing the impact of specific attributes on carer HRQoL. However, the comparability and transferability of estimates obtained using vignettes is limited, as the descriptions are treatment and indication specific. In 4 out of 20 of NICE appraisals that included carer HRQoL, estimates were derived from vignette studies (Table 1). In three of these appraisals, the values used in the health economic models were criticised by the committee and in two appraisals the inclusion of carer HRQoL was transferred to the scenario analyses in response to committee's critique.
Another alternative to primary data collection is using estimates from the literature or previous appraisals, albeit HRQoL data might be scarcely available, especially by health state. Using estimates that have been accepted by NICE in previous appraisals may also be accepted in later appraisals for the same indication, depending on the comparability of the health states and intervention. In the absence of indication-specific data, models used for NICE submissions have been populated using carer HRQoL values from other indications. In one NICE appraisal (HST16), estimates from another indication have been accepted, while in another NICE appraisal (TA748), estimates from another indication were deemed not transferable. In such cases, it is crucial to corroborate the similarities between indications. When using international data, researchers should take caution of differences between countries (e.g. cultural, healthcare system, valuation of health states) (Pennington et al., Reference Pennington, Eaton, Hatswell and Taylor2022).
Finally, carer HRQoL estimates could be obtained by mapping other instruments onto EQ-5D, as it is often done for HTA submissions in situations where patient EQ-5D data are unavailable (Longworth and Rowen, Reference Longworth and Rowen2013). However, the development of mapping algorithms has proven to be complex and available evidence largely concerns mapping to patient EQ-5D values. Mapping requires conceptual overlap between instruments, which complicates mapping carer-specific instruments, focusing on care-related quality of life, onto EQ-5D, focusing on HRQoL. Gheorghe et al. (Reference Gheorghe, Hoefman, Versteegh and Van Exel2019) succeeded in mapping patients' EQ-5D to caregiving hours, but their attempt to map to the carer-specific CarerQoL instrument did not lead to satisfying results (Gheorghe et al., Reference Gheorghe, Hoefman, Versteegh and Van Exel2019). Dixon et al. (Reference Dixon, Walker and Salek2006) also found explanatory power for relationships between patient and carer utilities to be low (Dixon et al., Reference Dixon, Walker and Salek2006). In addition, Al-Janabi et al. (Reference Al-Janabi, Manca and Coast2017) tried to predict carer EQ-5D using patient EQ-5D in a sample of 497 carer–patient dyads with long-term disabilities stemming from meningitis, which provided some evidence for relations between patient and carer HRQoL on an aggregate level, but did not allow for predictions on an individual level (Al-Janabi et al., Reference Al-Janabi, Manca and Coast2017). Given the lack of empirical evidence, further research into estimating carer HRQoL impacts based on commonly measured patient outcomes is recommended.
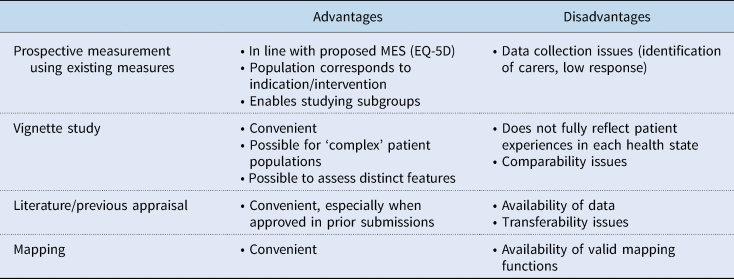
Table 2 provides an overview of advantages and disadvantages of different methods to obtain carer HRQoL estimates.
Advantages and disadvantages of methods to obtain carer HRQoL estimates
4.3 Number of carers
Next to carer utility values, data are needed on the proportion of patients receiving informal care and the number of carers providing care per patient. The HRQoL T&F Group proposed that only a single carer should be considered, particularly because evidence on the primary carer is likely to be more robust. Nonetheless, 45 per cent of recent NICE appraisals included more than one caregiver (Table 1), which NICE accepted in several cases. Ideally, the effects for the entire network of the patient are considered, as all health effects in the population should be equally important when maximising health. However, the identification of a patient's informal care network can be complicated, because of the subjective nature of defining informal care (e.g. some carers might not identify themselves as such) and the diversity of care relationships (e.g. some carers might remain out of scope of researchers). The size and composition of a patient's network may depend on the condition and the patient's health state; particularly in paediatric and elderly care, the network might be larger than in other conditions. When including multiple carers, it is important to acknowledge that not all carers may experience similar effects on providing care (Broese van Groenou et al., Reference Broese van Groenou, de Boer and Iedema2013). In particular, the size of health effects is likely to decline with increasing social distance from the patient. This has been shown in a case study on meningitis (Al-Janabi et al., Reference Al-Janabi, Van Exel, Brouwer, Trotter, Glennie, Hannigan and Coast2016b), but this distance-decline can be expected more generally. Extrapolating data collected in the primary carer to the caregiving network, e.g. by multiplying the obtained disutility value by the number of carers involved, is likely to overestimate the total carer HRQoL impact. Preferably, HRQoL estimates that reflect the relationship between patient and carer would be used, but this would require a higher level of granularity in the data.
4.4 Carer HRQoL in health economic models
Economic models are generally developed to represent the disease and patient HRQoL effects as accurately as possible, and carer HRQoL effects are added to this structure, if at all. Several options exist for including carer HRQoL in existing models, dependent on model structure. The review of NICE appraisals showed that carer HRQoL was previously included in economic models in different ways (Table 1): (dis)utilities as a function of the patient's health state or disease severity (25/36), (dis)utilities as a function of the patient's treatment (6/36), and (dis)utilities related to an adverse event (2/36). Pennington et al. (Reference Pennington, Eaton, Hatswell and Taylor2022) showed that both utilities and disutilities were used in different countries, and did not consider either approach superior (Pennington et al., Reference Pennington, Eaton, Hatswell and Taylor2022).
When carer HRQoL estimates are appended to existing health states, carer HRQoL estimates per health state are required. However, more mechanisms might play a role in this relationship and might not be represented in the model health states, including management of care and timing or location of services (Al-Janabi et al., Reference Al-Janabi, McLoughlin, Oyebode, Efstathiou and Calvert2019). Also, if it can be argued that the intervention affects carer HRQoL both directly (e.g. through factors such as location, timing, information provision, and involvement of family) and indirectly (i.e. through changes in patient health), treatment-dependent carer HRQoL data might be applied to model health states. The underlying mechanisms at play are ideally corroborated by data, so that the treatment's impact on carer HRQoL can be correctly integrated in economic models.
Finally, carer utility values, the proportion of patients receiving informal care, and the number of carers involved are all surrounded with uncertainty. This uncertainty should be included in the model like other parameters (Henry et al., Reference Henry, Al-Janabi, Brouwer, Cullinan, Engel, Griffin, Hulme, Kingkaew, Lloyd, Payakachat, Pennington, Peña-Longobardo, Prosser, Shah, Ungar, Wilkinson and Wittenberg2024).
5. Consistency and comparability of outcomes
To maintain comparability of cost-effectiveness outcomes across diseases, interventions, and over time, it is important that the rationale and method for including carer HRQoL in economic evaluations is applied consistently. Therefore, future economic evaluations should preferably present analyses with and without carer HRQoL (Pennington et al., Reference Pennington, Eaton, Hatswell and Taylor2022). In this way, evidence is provided on the impact of the intervention on carers while comparability is maintained with evaluations that exclude carer HRQoL, either conducted in the past or for which carer HRQoL is not relevant, and with common cost-effectiveness thresholds.
6. Directions for future research
Attention towards carer HRQoL is growing, but there still are several unsolved issues. Important issues concern substantiating when inclusion of carer HRQoL is relevant and capturing elements that affect carer HRQoL adequately and comprehensively. Disease, interventions and patient group-specific elements play a role here.
Although the utilitarian approach in cost-effectiveness studies provides a systematic framework for evaluating new interventions, maximising health benefits under a budget constraint may not fully capture societal and individual preferences or the subjective experiences of patients and their carers related to the disease, the intervention, and their impacts. There is a difference in what is relevant for carers (e.g. the patient's and their own well-being, or their employment, career prospects, and financial situation) and for decision makers (i.e. HRQoL in the healthcare perspective). As the EQ-5D focuses on HRQoL, such other aspects of value to carers may not be adequately captured. The use of other instruments can be particularly valuable if these instruments can be used to produce utility values. This requires additional research into how such utilities can be combined with utilities derived from EQ-5D. Until then, carer-specific utilities could be included in scenario analyses.
It is also important to consider that inclusion of carer HRQoL in HTAs may have distributional impacts, if they are considered in decision-making. After all, because an outcome category is added to the evaluation, interventions that have a positive effect on carer HRQoL may then result in more (health) value for money than interventions that have no, or a negative, impact on informal carers. The magnitude and direction of this effect may depend on characteristics of the patient group, their condition, the number of carers included in the economic evaluation, the context, and the intervention, and could be relevant to both a healthcare and a societal perspective. Of course, ignoring carer HRQoL is also associated with distributional impacts, albeit implicitly, as potentially relevant health effects in carers are left out of consideration in decision-making (Brouwer, Reference Brouwer2019), skewing decision-making away from interventions that benefit carers and patients with conditions associated with informal care.
Another important aspect is how bereavement affects carers and families (Henry et al., Reference Henry, Al-Janabi, Brouwer, Cullinan, Engel, Griffin, Hulme, Kingkaew, Lloyd, Payakachat, Pennington, Peña-Longobardo, Prosser, Shah, Ungar, Wilkinson and Wittenberg2024). In one appraisal (TA755), NICE explicitly mentioned that accounting for the bereavement effect was important, but it proved to be complex to incorporate this in a health economic model. Dealing with grief in health economic models is largely unexplored but could entail modelling beyond patients' lifetime time horizon, as carers and family members may experience grief for long after a patient's death, especially in paediatric indications. Interventions that greatly improve life expectancy could, therefore, result in a significant impact on carer and family HRQoL. The HRQoL T&F Group argued that bereavement should not be considered, because the methods to quantify these effects are not well developed and the impact is unpredictable. Further research is thus needed on how to measure and model the effects of bereavement in HTAs and the way in which decision-makers may want such data presented.
Finally, it may be helpful to shift the burden of proof for future appraisals from demonstrating that effects on carers are substantial and hence relevant, as is currently advised by NICE, for demonstrating that this is not the case, reiterating the conclusions from the review by Goodrich et al. (Reference Goodrich, Kaambwa and Al-Janabi2012). This would acknowledge the importance of incorporating carer HRQoL in economic evaluations and consequently promote the consideration of carer HRQoL routinely in economic evaluations, in line with the aim of maximising population health.
Acknowledgement
The authors thank Matthijs Versteegh, PhD, for his role in the concept and design of the study.
Financial support
The study was sponsored by Takeda UK, Ltd. The deliverable of the project was a publication. Two employees of the sponsor are co-authors of the publication. The publication of the study results was not contingent on the sponsor's approval or censorship of the manuscript.
Competing interests
Kanters and van Hezik-Wester received grants from Biogen Netherlands outside the submitted work. Boateng and Cranmer were employed by Takeda UK, Ltd. Al-Janabi received personal fees from Ferring, Curta, Roche, and PHMR. Van Exel received grants from National Institute for Public Health and the Environment, ZonMw, European Commission, Erasmus Trustfonds, Convergence Health & Technology, and GSK. Kvamme and Santi have no competing interests.




 Open access
Open access