



Social media summary
Early-life adversity may intensify menopause symptoms among Latine adults but is not linked to earlier menopause.
Introduction
The menopausal transition is a life stage with significant health implications for biologically female individuals, often marking a shift in physical, psychological, and social well-being. The onset of natural menopause occurs as the by-product of ovarian ageing and follicular atresia, a form of programmed cell death of oocytes. The resultant hormonal changes due to the depletion of the ovarian reserve contribute to a range of menopausal symptoms, including vasomotor symptoms (VMS) such as hot flashes and night sweats (Butler & Santoro, Reference Butler and Santoro2011; Talaulikar, Reference Talaulikar2022). While the normative, biomedical definition of menopause is often discussed in contexts conflating sex and gender, menopausal individuals are not inherently cisgender. The use of ‘female’ or ‘biologically female’ in this paper is meant to be inclusive of all individuals who are born with female reproductive anatomy – regardless of their gender identity – that has the capacity to senesce and undergo the menopausal transition.
The timing and experience of the menopausal transition are highly variable and can contribute to elevated disease risk during the postmenopausal stage (Cortés & Marginean, Reference Cortés and Marginean2022; Lock & Kaufert, Reference Lock and Kaufert2001; Melby & Lampl, Reference Melby and Lampl2011). VMS are associated with increased risk of cardiovascular disease, poor mental health, and reduced quality of life among both low-income communities and people of colour compared to their non-Latine White counterparts in the US (‘Latine’ is used as a gender-inclusive alternative to Latino/a; Biglia et al., Reference Biglia, Cagnacci, Gambacciani, Lello, Maffei and Nappi2017; Cortés et al., Reference Cortés, Marginean and Berry2021; Gold et al., Reference Gold, Colvin, Avis, Bromberger, Greendale, Powell, Sternfeld and Matthews2006; Green & Santoro, Reference Green and Santoro2009; Uddenberg et al., Reference Uddenberg, Safwan, Saadedine, Hurtado, Faubion and Shufelt2024; Wise et al., Reference Wise, Krieger, Zierler and Harlow2002). As examined through the local biologies framework, variations in menopausal experiences may in part be an embodied product of how biological states develop and modify in interaction with local environments (Lock, Reference Lock1993). For instance, the lower reporting of VMS among Japanese individuals compared to North Americans is thought to be shaped by dietary, linguistic, cultural, and medical norms that affect how menopause is experienced, discussed, and physiologically expressed (Lock, Reference Lock1998).
It is also important to contextualize variations in menopausal experiences within the scope of structural violence, inequalities, and historical subjugation of marginalized groups that function as facets of local biologies (Leatherman & Goodman, Reference Leatherman and Goodman2020). This array of environmental factors can shape differences in basal hormonal levels that may affect VMS experience during the menopausal transition. It has been posited that the lower levels of estradiol among Asian pre- and perimenopausal adults compared to Latine, African American, and white individuals in the Study of Women’s Health Across the Nation (SWAN) may be related to the observations of reduced symptom reporting, possibly due to a less marked fall in estradiol levels (Randolph et al., Reference Randolph, Sowers, Gold, Mohr, Luborsky, Santoro, McConnell, Finkelstein, Korenman, Matthews, Sternfeld and Lasley2003). In this same study, higher estradiol and lower testosterone levels were observed among Latine participants, potentially suggestive of an increased risk for VMS (Cortés et al., Reference Cortés, Marginean and Berry2021; Randolph et al., 2003). Proximately, obesity, health behaviours such as smoking, and negative affect are also thought to drive differences in VMS experience (Thurston & Joffe, Reference Thurston and Joffe2011).
Human evolutionary and developmental frameworks on early-life adversity and senescence offer additional insights as to why menopausal experiences may vary. It has been hypothesized that exposure to early-life adversity may influence senescence by shaping developmental patterns of energy allocation among growth, reproduction, and somatic maintenance (Ellis et al., Reference Ellis, Figueredo, Brumbach and Schlomer2009; Jasienska, Reference Jasienska2009). While early-life adversity has been proposed to serve as a potential cue of extrinsic mortality risk, recent theoretical work in life history theory emphasizes that early adversity should not be assumed to consistently accelerate life history strategies due to the uncertainty of the underlying assumption about environmental continuity across the life-course (Nettle & Frankenhuis, Reference Nettle and Frankenhuis2020). Instead, increased extrinsic mortality in early life is posited to slow life history unless adult mortality is also increased (André & Rousset, Reference André and Rousset2020; Nettle & Frankenhuis, Reference Nettle and Frankenhuis2020). Early-life adversity, along with ecological harshness, resource constraints, and environmental stressors, may nonetheless bias patterns of resource allocation towards reproductive function over somatic maintenance, potentially altering the rate of reproductive senescence (Ding et al., Reference Ding, Xu, Kondracki and Sun2024; Ellis et al., Reference Ellis, Figueredo, Brumbach and Schlomer2009; English & Bonsall, Reference English and Bonsall2019; Jasienska, Reference Jasienska2020; Suvorov, Reference Suvorov2022).
Within this framework, early-life adversity may hasten the depletion of the ovarian reserve not because menopause is selected for, but because reduced investment in repair and maintenance may accelerate reproductive senescence as a by-product (Peccei, Reference Peccei2001). Empirical evidence supports this interpretation as psychological stress has been associated with both higher antral follicle count (AFC; a marker of the ovarian reserve) among younger premenopausal individuals and a higher rate of AFC loss across the sample, suggesting that greater stress may transiently enhance reproductive function at the cost of accelerated reproductive ageing (Bleil et al., Reference Bleil, Adler, Pasch, Sternfeld, Gregorich, Rosen and Cedars2012). Relatedly, stress-mediated acceleration of pubertal development may elicit related trade-offs that shorten the reproductive lifespan, as exemplified by both earlier age at menarche and menopause among individuals with a history of sexual abuse (Ellis & Giudice, Reference Ellis and Giudice2019; Magnus et al., Reference Magnus, Anderson, Howe, Joinson, Penton-Voak and Fraser2018). This life history informed perspective further aligns with broader epidemiological trends where earlier age at menopause is found among low- and middle-income populations in addition to those who were exposed to conditions such as poor nutrition, high infectious disease burden, and parental divorce early in life (Duarte et al., Reference Duarte, de Sousa, Cadarso-Suarez, Rodrigues and Kneib2014; Elias et al., Reference Elias, van Noord, Peeters, den Tonkelaar and Grobbee2003; Fraser et al., Reference Fraser, Johnman, Whitley and Alvergne2020; Mishra et al., Reference Mishra, Hardy and Kuh2007; Murphy et al., Reference Murphy, Sievert, Begum, Sharmeen, Puleo, Chowdhury, Muttukrishna and Bentley2013; Ruth et al., Reference Ruth, Perry, Henley, Melzer, Weedon and Murray2016). For instance, one study found that individuals who experienced lower socio-economic status in childhood tended to reach menopause earlier; furthermore, the longer one spent in disadvantaged conditions, the earlier the onset of menopause (Hardy & Kuh, Reference Hardy and Kuh2005). Additionally, population-level differences in ovarian reserve biomarkers, such as those observed among Mayan individuals in Campeche, Mexico, and Bangladeshi immigrants in the UK, may similarly reflect cumulative ecological constraints on somatic maintenance (Begum et al., Reference Begum, Muttukrishna, Sievert, Sharmeen, Murphy, Chowdhury, Kasim, Gunu and Bentley2016; Kyweluk et al., Reference Kyweluk, Sievert, Huicochea-Gómez, Cahuich-Campos, McDade and Brown2018).
A growing body of literature on adverse childhood experiences (ACEs) illustrates how early-life adversity, including abuse, neglect, and household dysfunction, may later negatively impact menopausal experiences, including the frequency of VMS and the timing of menopause. ACEs may influence these outcomes through downstream pathways including lower educational attainment, economic instability, and chronic psychosocial stress across the life-course (Yang et al., Reference Yang, Kuo, Hart, Zia and Grigsby2025). The effects of both early and chronic stress are understood to influence VMS and the timing of menopause through developmentally plastic, stress-linked alterations of the hypothalamic–pituitary–adrenal (HPA) and hypothalamic–pituitary–ovarian (HPO) axes in humans. Notably, age at menopause and VMS reflect related but distinct biological processes. Age at natural menopause primarily indexes cumulative reproductive ageing driven by ovarian reserve depletion (Forman et al., Reference Forman, Mangini, Thelus-Jean and Hayward2013). In contrast, VMS during the menopausal transition are associated with the magnitude and dynamics of reproductive hormone withdrawal, as well as individual differences in neuroendocrine stress responsivity and thermoregulatory sensitivity (Thurston, Reference Thurston2024). Empirically, associations between earlier age at menopause and VMS burden are inconsistent (Freeman et al., Reference Freeman, Sammel, Lin, Liu and Gracia2011; Gibson-Helm et al., Reference Gibson-Helm, Teede and Vincent2014). As such, these outcomes may be influenced by early-life exposures while remaining partially independent in their underlying mechanisms.
Studies have shown that prolonged exposure to stressors may result in the chronic activation of the HPA axis, resulting in elevated levels of cortisol that can have an inhibitory effect on gonadotropin signalling (Bale & Epperson, Reference Bale and Epperson2015; Toufexis et al., Reference Toufexis, Rivarola, Lara and Viau2014). Inhibition of the HPO axis causes a downstream inhibitory effect on gonadotropin-releasing hormone (GnRH) that reduces luteinizing hormone and follicle-stimulating hormone secretion, which may accelerate the depletion of the ovarian reserve with potential implications on the timing of the menopausal transition (Hall, Reference Hall2015). Relatedly, animal studies have shown that increased glucocorticoid secretion suppresses gonadotropin secretion via a reduction in GnRH pulse frequency among follicular-phase ovariectomized ewes (Oakley et al., Reference Oakley, Breen, Clarke, Karsch, Wagenmaker and Tilbrook2009; Phumsatitpong et al., Reference Phumsatitpong, Wagenmaker and Moenter2021). While growing evidence suggests a potential association between early-life adversity and earlier onset of menopause (Cleland et al., Reference Cleland, McLeod, Dhakal, Fenton, Welch, Horwood and Boden2022; Hardy & Kuh, Reference Hardy and Kuh2005), researchers have reported mixed findings including earlier menopause after exposure to threat-related adversity (Yuan et al., Reference Yuan, Yu, Liu and Sun2022) as well as no association between ACEs and age at natural menopause (Kling et al., Reference Kling, Saadedine, Faubion, Shufelt, Mara, Enders, David and Kapoor2023).
Stress exposure in early life may also shape VMS experience via dysregulation of central thermoregulatory mechanisms and the HPA axis (Gibson et al., Reference Gibson, Thurston and Matthews2016). This pattern of neuroendocrine dysregulation may reflect sensitization of the stress response following exposure to early environmental adversity, which may increase vulnerability to VMS later in life (Peña, Reference Peña2025; Russell et al., Reference Russell, Tasker, Lucion, Fiedler, Munhoz, Wu and Deak2018). Increased stress reactivity shaped by early-life adversity may impact the autonomic nervous system as well as further exacerbate fluctuations and declines in estradiol, contributing to the occurrence of VMS (Gibson et al., 2016; Monteleone et al., Reference Monteleone, Mascagni, Giannini, Genazzani and Simoncini2018). In line with this hypothesized pathway, past research has demonstrated that childhood abuse and neglect were associated with increased reporting of both hot flashes and night sweats among African American and White participants from SWAN (Thurston et al., Reference Thurston, Bromberger, Chang, Goldbacher, Brown, Cyranowski and Matthews2008). However, studies have heavily relied on predominantly White samples with high socio-economic status, which limits the understanding of these effects on broader populations. Latine people remain significantly underrepresented in menopause research, often excluded entirely or comprising only a small fraction of study samples.
Grounded in a life history perspective, we examine the association between early-life adversity and the menopausal transition among a sample of predominantly Mexican immigrant individuals living in an agricultural community in California. Specifically, we examine the association of ACEs and (1) age at natural menopause and (2) experience of hot flashes and night sweats, respectively. We hypothesize that greater exposure to ACEs will predict (1) an earlier age at natural menopause, reflecting accelerated reproductive senescence associated with constrained resource allocation towards maintenance following early-life adversity. Additionally, we hypothesize that greater exposure to ACEs will predict (2) the experience of VMS as a by-product of neuroendocrine dysregulation. Accordingly, we examine age at natural menopause and VMS as related but distinct outcomes that may reflect overlapping developmental pathways shaped by early-life adversity.
Methods
Study population
Data used for this analysis come from the Center for the Health Assessment of Mothers and Children of Salinas–Maternal Cognition Study (CHAMACOS-MCS), a community-based cohort of mid-life adults in California’s Salinas Valley who have been long-time participants in a study focused on environmental exposures and child health (Torres et al., Reference Torres, Calderon, Kogut, MacCuish, Warner, Rodriguez, Garcia, Romero, Morga, McDowell-Sanchez, Perez-Rocha, Rojas-Saunero, Deardorff and Eskenazi2025). Details of the CHAMACOS study have been presented elsewhere (Eskenazi et al., Reference Eskenazi, Bradman, Gladstone, Jaramillo, Birch and Holland2003). Briefly, from October 1999 to October 2000, the study recruited pregnant adults who were obtaining prenatal care at clinics in the Salinas Valley. Eligible individuals were at least 18 years old, less than 20 weeks of gestation, proficient in Spanish or English, and were eligible for California’s Medicaid program (i.e., MediCal). Of the 1,130 eligible adults, 597 enrolled and completed a baseline visit after which 525 mother–child dyads were followed until a livebirth. To refresh the cohort, additional mother–child dyads were recruited from local schools and community organizations/events in 2009–2011 when the children were 9 years old, culminating in a maternal sample of 635 participants. For the refresher cohort, eligible individuals needed to be Spanish- or English-speaking and to have qualified for Medicaid during the index pregnancy, received prenatal care in the Salinas Valley, and delivered in the years 2000–2002 at maternal age 18 or older in a California hospital. The intent was to ensure that refresher participant dyads were from the same underlying population as the original cohort. Between 2009 and 2021, all cohort dyads were invited to complete multiple data collection visits through children aged 18.
Between May 2022 and July 2024, all CHAMACOS mothers who had participated in the study at any point since 2014 were recruited to participate in the CHAMACOS-MCS. Informed by a life-course perspective, the MCS aims to quantify the associations between social adversity, pesticide exposure, and cognitive performance among mid-life Latine biologically female adults (Torres et al., Reference Torres, Calderon, Kogut, MacCuish, Warner, Rodriguez, Garcia, Romero, Morga, McDowell-Sanchez, Perez-Rocha, Rojas-Saunero, Deardorff and Eskenazi2025). Of the 635 eligible mothers, 577 had recently updated contact information (from at least 2014 or later). Participants were recruited through personal phone calls by a field coordinator whom they had known since their initial enrollment in the study. In total, 519 individuals completed baseline Maternal Cognition Study visits. Additional recruitment occurred through October 2025, but data were not available in time to be included in this analysis. As previously reported (Torres et al., Reference Torres, Calderon, Kogut, MacCuish, Warner, Rodriguez, Garcia, Romero, Morga, McDowell-Sanchez, Perez-Rocha, Rojas-Saunero, Deardorff and Eskenazi2025), CHAMACOS-MCS participants are generally comparable to participants who completed baseline visits in 1999–2000 or 2009–2011, but did not participate in CHAMACOS-MCS, although CHAMACOS-MCS participants are slightly more likely to be immigrants and to have lived at or below the federal poverty line and have diabetes or high blood pressure at baseline. Compared to other Salinas Valley females of similar age (based on American Community Survey data), CHAMACOS-MCS participants were more likely to be immigrants, to have lower educational attainment, and to be living in poverty (Torres et al., Reference Torres, Calderon, Kogut, MacCuish, Warner, Rodriguez, Garcia, Romero, Morga, McDowell-Sanchez, Perez-Rocha, Rojas-Saunero, Deardorff and Eskenazi2025). All participants completed written informed consent, and study procedures were approved by the University of California, Berkeley Office for the Protection of Human Subjects (Protocol ID 2021-02-14055).
Exclusion criteria
For the current analysis, any participants with missing data across the variables of interest, who reported having had surgical menopause (N = 32), or who currently use hormonal contraceptives (N = 22) were excluded, leaving a final analysis sample of 459.
Measures
The CHAMACOS-MCS makes use of a rich set of historical data and samples collected from participants at earlier stages of CHAMACOS data collection. All study visits have included detailed maternal questionnaires facilitated by a bilingual/bicultural interview in the mother’s language of choice (English or Spanish) to collect information on demographics, health, and the social and built environment.
Adverse childhood experiences
The ACEs questionnaire is a 10-item measure that assesses exposures to various forms of childhood abuse, neglect, and household challenges between ages 0 and 18 (Felitti et al., Reference Felitti, Anda, Nordenberg, Williamson, Spitz, Edwards, Koss and Marks1998). ACEs were collected from mothers via interviews at the 18-year visit (i.e., when index children were age 18). Because 8.88% of mothers declined to answer individual ACEs questions at 18 years, the study team administered the ACEs questionnaire in a less invasive way at the baseline MCS visit for participants who were missing it. For this group, ACEs were presented as a list of the 10 items and participants were asked to report whether they had experienced 0, 1, 2, 3, 4, or 5 or more of the 10 experiences presented to them. For the analysis, ACEs data were coded into three categorical groups of 0 ACEs, 1–3 ACEs, and 4+ ACEs.
Age at menopause and VMS
Starting with the 12-year study visit (i.e., 10 years prior to the MCS visit) and at every approximately biennial visit thereafter, participants self-reported their menstruation status. Participants were asked the following series of questions, with later questions conditional on responses to earlier questions: (1) Have you had a menstrual period in the past 12 months? (‘No’, ‘Yes’, and ‘Don’t know’); (2) If yes to question 1: In the past year, what best describes your menstrual period? (‘Regular periods naturally’; ‘Regular periods because you take hormones, such as birth control pills’; ‘Irregular periods’; and ‘Don’t know’); (3) If yes to irregular periods: what do you think is the reason that you have had irregular periods in the past year? (‘Always irregular’, ‘Getting close to menopause’, ‘Other reason’, and ‘Don’t know’); and (4) If no to question 1: what do you think is the reason that you did not have a menstrual period in the past 12 months? (‘Natural menopause’, ‘Surgery [a hysterectomy or removal of both your ovaries]’, ‘Recent pregnancy/breastfeeding’, ‘Contraceptives or family planning’, ‘Chemotherapy or radiation therapy’, and ‘Don’t know’).
Postmenopausal participants were asked the date of their last menstrual period (LMP). For those who did not know, they were asked how old they were at their LMP, and if they did not know, they were asked how many years had passed since their LMP. This information was used with the current age to calculate the imputed age at LMP and was used as the age at menopause for postmenopausal participants who could not recall their age at menopause.
Based on participants’ responses about their menstrual status, and in accordance with the Staging of Reproductive Aging Workshop (STRAW) + 10 guidelines, we categorized participants into premenopausal, perimenopausal, and postmenopausal groups (Harlow et al., Reference Harlow, Gass, Hall, Lobo, Maki, Rebar, Sherman, Sluss and de Villiers2012). The STRAW + 10 is the gold standard for staging reproductive ageing that can be applied regardless of a person’s age, ethnicity, body size, or lifestyle characteristics, providing a standardized framework to define menopausal stages based on menstrual bleeding patterns. Premenopausal individuals were those who reported regular menstruation, perimenopausal individuals reported irregular menstruation, and postmenopausal individuals reported no menstruation in the past 12 months due to natural menopause.
All participants, regardless of menopausal status, were also asked about their experience of VMS, including hot flashes and night sweats, respectively, over the past 2 weeks. For both questions, participants reported from the following options: ‘Not at all’, ‘1–5 days’, ‘6–8 days’, ‘9–13 days’, and ‘Every day’. Due to the sparse data across the response (Supplementary Table S1), both variables were binarily collapsed into ‘Yes’ or ‘No’ to capture whether participants experienced any amount of the specified VMS in the 2 weeks prior to the study visit.
Statistical methods
Data were analysed using R version 4.4.1 (Tāmaki Makaurau, Aotearoa/Auckland, NZ). Bivariate associations were conducted to estimate the relationship between ACEs, age at menopause, hot flashes, night sweats, and covariates. To evaluate the relationship between ACEs and age at natural menopause, Kaplan–Meier survival analysis was used to calculate the median age at natural menopause. Time-to-event was defined as time from age at menarche to age at menopause or study end for participants who were premenopausal or perimenopausal. A Cox proportional hazards model was used to quantify the relationship between ACEs and the risk of menopause at any given age after menarche while controlling for covariates. Scaled Schoenfeld residuals were generated for the final multivariate model to test the proportional hazard assumption.
To evaluate the relationship between ACEs and VMS, we fitted two separate binary logistic regression models to estimate the relationship between ACEs and the odds of reporting hot flashes and the odds of reporting night sweats. In our primary estimates, we estimated these associations in the full sample, although we additionally estimated these associations stratified by menopausal status in sensitivity analyses.
Using a directed acyclic graph, covariates were selected based on their association with both the exposure and outcome, with particular attention to early-life factors that temporally precede both ACEs and menopausal outcomes to minimize over-control for potential mediators of our relationships of interest (Supplementary Figure S1) (Hernán & Robins, Reference Hernán and Robins2023). Covariates include age at data collection (continuous variable, years), country of origin (categorical variable, Latin America or US), and educational attainment (categorical variable, ≤6th grade, 7–12th grade, ≥high school [HS] graduate). In sensitivity analyses, we re-estimated associations among the subset of participants who were born outside the US.
Results
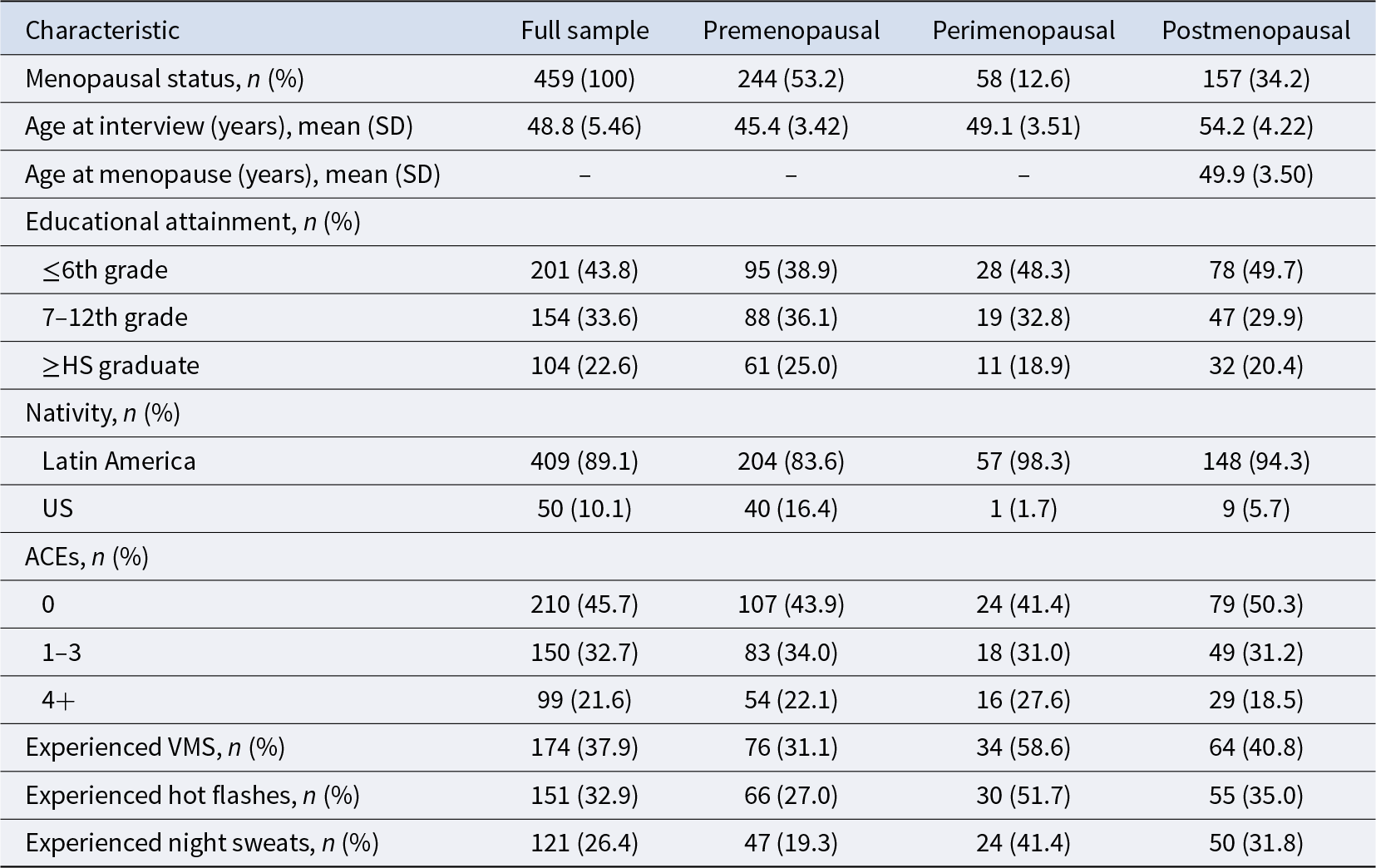
Table 1 describes the characteristics of our analytic sample (N = 459). The average age was 48.8 years, the majority of the sample (89.1%) was born in Latin America, and 43.8% achieved a 6th-grade level of education or less. Across the three levels of ACEs, 45.7% of the sample reported no ACEs, 32.7% reported 1–3 ACEs, and 21.6% reported 4 or more. The prevalence of each menopausal status group was as follows: 53.2% premenopausal, 12.6% perimenopausal, and 34.2% postmenopausal. Among the postmenopausal group, the recalled mean age at menopause was 49.9 years. 32.9% of participants reported experiencing any amount of hot flashes, and 26.4% reported experiencing any amount of night sweats during the 2 weeks before the study visit. VMS symptoms were experienced at the greatest frequency among individuals in perimenopause (58.6%), followed by postmenopausal (40.8%) and premenopausal (31.1%) adults.
Descriptive characteristics of study participants

In bivariate analyses, exposure to ACEs was associated with minimal differences in age at menopause (1–3 ACEs: β = 0.34, 95% confidence interval [CI]: −0.92 to 1.61; 4+ ACEs: β = 0.00, 95% CI: −1.51 to 1.51). Bivariate associations between ACEs and hot flashes indicated higher reported prevalence of hot flashes with ACEs exposure (X 2(2, N = 459) = 16.06, p < 0.05) as well as a moderate increase in night sweat reporting with ACEs exposure (X 2(2, N = 459) = 8.28, p < 0.05).
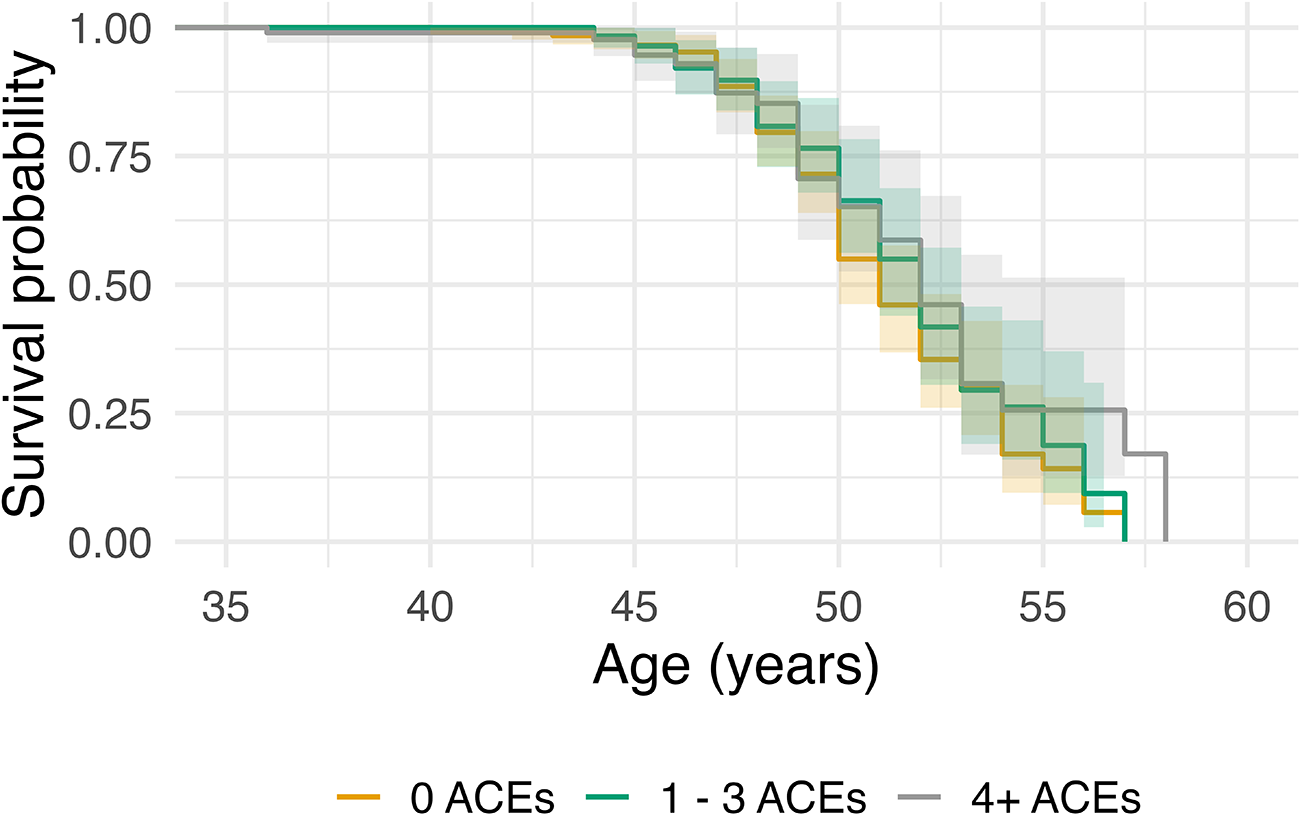
Figure 1 depicts the Kaplan–Meier curve of age at natural menopause across ACEs subgroups. The median age at natural menopause for participants with 0 ACEs was 51 (95% CI: 50–52), 1–3 ACEs was 52 (95% CI: 51–53), and 4 or more ACEs was 52 (95% CI: 51–57). The results of the adjusted Cox regression indicate that relative to reporting 0 ACEs, 1–3 ACEs (hazard ratio [HR] = 0.85, 95% CI: 0.59–1.22), and 4 or more ACEs (HR = 0.68, 95% CI: 0.44–1.07) are negatively associated with age of menopause, although estimates were imprecise and included the null (Table 2). Scaled Schoenfeld residuals showed no evidence of violation of the proportional hazards assumption for any covariate (global test p = 0.58).
Kaplan–Meier estimates of age at natural menopause by ACEs exposure (0 ACEs, 1–3 ACEs, and 4+ ACEs). Note: Entry age is the age at menarche.

Multivariate Cox proportional hazards model estimating the association between adverse childhood experiences (ACEs) and age at natural menopause (N = 459). Controls for educational attainment and nativity

Note: Values are hazards ratios (HR) with 95% confidence intervals (CI). Reference groups: 0 ACEs, ≤6th grade, and Latin America.
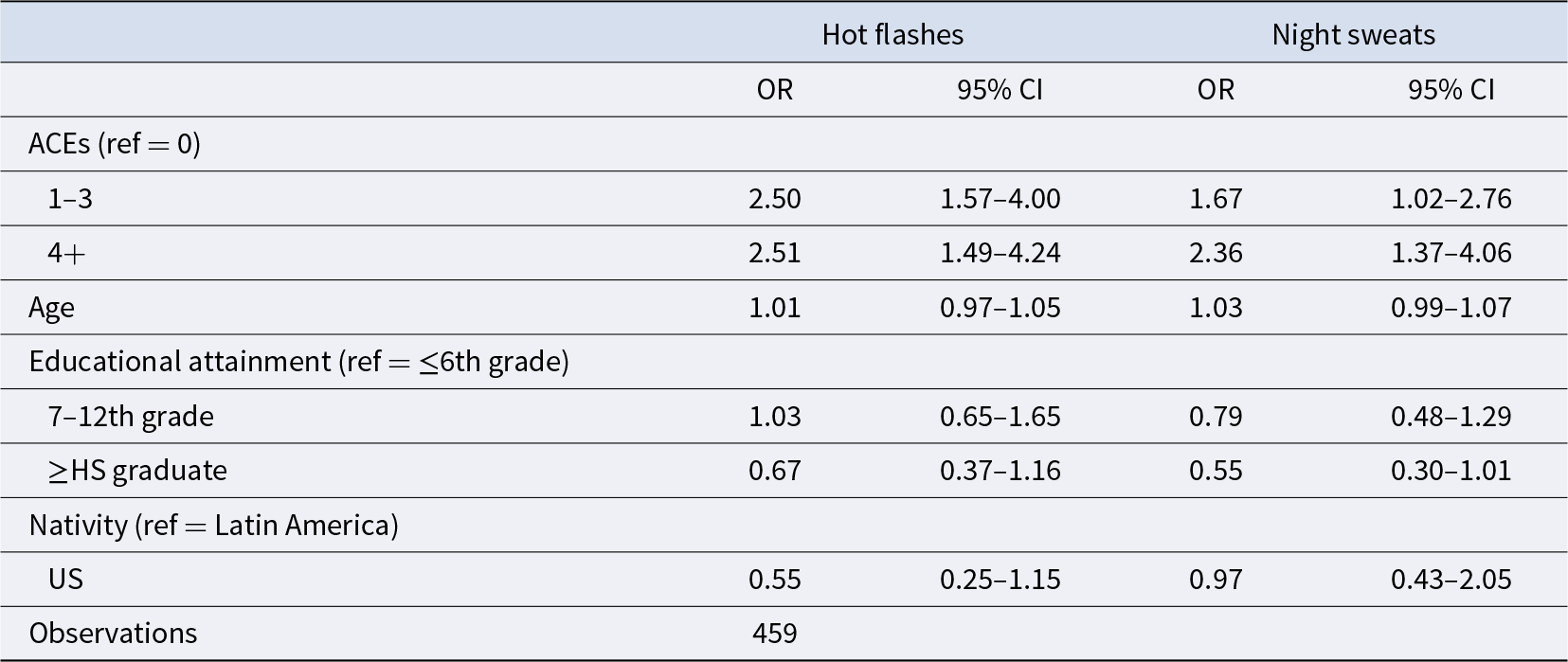
In the adjusted logistic regression model, ACEs were associated with reporting hot flashes (Table 3). Reporting 1–3 ACEs (vs. no ACEs) was associated with over twofold greater odds of reporting hot flashes (odds ratio [OR] = 2.50, 95% CI: 1.57–4.00). Those who reported 4 or more ACEs (vs. no ACEs) had similarly elevated odds of hot flashes (OR = 2.51, 95% CI: 1.49–4.24). Similarly, in the adjusted model, reporting 1–3 ACEs (vs. no ACEs) was associated with higher odds of reporting night sweats (OR = 1.67, 95% CI: 1.02–2.76) while reporting 4 or more ACEs (vs. no ACEs) was associated with over twofold greater odds of reporting night sweats (Table 3; OR = 2.36, 95% CI: 1.37–4.06).
Logistic regression models estimating the association between adverse childhood experiences (ACEs) and experience of vasomotor symptoms (N = 459). Controls for age, educational attainment, and nativity

Note: Values are odds ratios (OR) with 95% confidence intervals (CI). Reference groups: 0 ACEs, ≤6th grade, and Latin America.
Sensitivity analyses
Results of our sensitivity analyses stratified by menopausal status yielded substantively similar associations between ACEs and VMS (Supplementary Tables S2 and S3). In some cases, CIs shifted to include or exclude the null hypothesis, but associations remained in the same direction, and CIs overlapped in every case.
Excluding participants born in the US yielded similar patterns of association between ACEs and VMS, with the CI shifting to include the null hypothesis for the association between 1 – 3 ACEs (vs. no ACEs) and night sweats, although the association remained in the same direction (Supplementary Table S4). Additionally, excluding participants born in the US yielded substantively similar results in the multivariate Cox proportional hazards model estimating the association between ACEs and age at natural menopause (Supplementary Table S5).
Discussion
In this cross-sectional analysis of predominantly Mexican immigrant adults with a high prevalence of ACEs living in an agricultural community in California, greater exposure to ACEs was associated with experiencing VMS—hot flashes and night sweats—at mid-life. Specifically, reporting ACEs (vs. none) was associated with more than double the odds of experiencing hot flashes; effect estimates were similar for fewer (1–3) and more (4+) ACEs. ACEs were also associated with a greater odds of experiencing night sweats, with estimates being the largest for those who experienced four or more (vs. no) ACEs. However, the association of ACEs with age at natural menopause was in the opposite direction from what we hypothesized, although our estimates are highly imprecise and preclude a clear conclusion. These findings suggest that the sequelae of childhood adversity may persist throughout the life-course and impact VMS burden. This analysis is the first study, to our knowledge, to examine the relationship between ACEs and menopausal experiences among a Latine immigrant population.
Our unexpected, albeit highly imprecise, findings regarding ACEs and age at natural menopause in this sample may be explained by our inability to examine the temporal specificity of ACEs across child development. Researchers have shown that the rate of follicular atresia is at its highest early in life, such that stressors experienced in early childhood may have the most effect on the onset of the menopausal transition and age at menopause (Rothchild, Reference Rothchild2003; Rulu & Sievert, Reference Rulu, Sievert, Howell and Harrod2023). For instance, one study found that low weight at 2 years but not 7 was associated with age at menopause (Hardy & Kuh, Reference Hardy and Kuh2002), while another found that individuals who reported experiencing famine conditions from ages 2 to 6 during the Dutch famine experienced earlier menopause than those who were not exposed (Elias et al., Reference Elias, van Noord, Peeters, den Tonkelaar and Grobbee2003). These patterns may be indicative of an abbreviated developmental window during which stressors may have the most effect on shaping the reproductive lifespan by influencing rates of follicular loss, potentially via energetic trade-offs (Forman et al., Reference Forman, Mangini, Thelus-Jean and Hayward2013; Goldberg et al., Reference Goldberg, Tawfik, Kline, Michels, Wei, Cirillo, Cohn and Terry2020; Sievert, Reference Sievert2014, Reference Sievert2024). While the timing of this critical period in early life remains unclear, it is possible that the experience of ACEs during a specific age window may have the greatest impact on the timing of menopause at mid-life. Additionally, in the present sample, individuals reporting any ACEs tend to have higher childhood and current socio-economic status than those with no ACEs (Supplementary Table S6). Despite adjusting for education, other dimensions of socio-economic position across the life-course may shape menopausal outcomes, contributing to residual confounding.
Our findings of an association between ACEs and hot flashes and night sweats are consistent with previous findings. One study assessing ACEs and symptom burden via the Menopause Rating Scale among a sample of predominantly White mid-life adults found that greater childhood adversity was associated with a higher menopausal somatic symptom score, a measure that includes the experience of hot flashes (Kapoor et al., Reference Kapoor, Okuno, Miller, Rocca, Rocca, Kling, Kuhle, Mara, Enders and Faubion2021). This finding is similar to that of the aforementioned SWAN assessment that demonstrated an association between childhood abuse and neglect with increased reporting of hot flashes and night sweats (Thurston et al., Reference Thurston, Bromberger, Chang, Goldbacher, Brown, Cyranowski and Matthews2008). Stress-induced physiological adaptations, such as alterations to the HPA axis in response to ACEs throughout childhood and adolescence, may in part explain how menopausal symptom burden could be a by-product of neuroendocrine dysregulation following early-life stress. Specifically, beyond the aforementioned critical window of development, ACEs may alter HPA axis function, which may in turn impact the HPO axis, further aggravating normal hormonal imbalances caused by the depletion of the ovarian reserve, leading to increased vulnerability to VMS during the menopausal transition (Freedman et al., Reference Freedman, Kruger and Wasson2011; Gordon et al., Reference Gordon, Rubinow, Thurston, Paulson, Schmidt and Girdler2016; Kalmakis et al., Reference Kalmakis, Meyer, Chiodo and Leung2015; Meldrum et al., Reference Meldrum, Defazio, Erlik, Lu, Wolfsen, Carlson, Hershman and Judd1984; Worthman & Kuzara, Reference Worthman and Kuzara2005). Although VMS physiology remains to be fully elucidated, it is possible that hormonal dysregulation across the HPA and HPO axes in response to early-life adversity plays a role in shaping VMS experience.
Further, individuals with greater exposure to ACEs may have altered autonomic function that contributes to differences in VMS experience, as exemplified by prior findings linking childhood abuse and trauma exposure to lower heart rate variability in adulthood (Dale et al., Reference Dale, Carroll, Galen, Hayes, Webb and Porges2009; Stone et al., Reference Stone, Amole, Cyranowski and Swartz2018). Additionally, observed differences in autonomic nervous system activity between wake and sleep VMS may reflect distinct underlying mechanisms for hot flashes and night sweats (Thurston et al., Reference Thurston, Carson, Koenen, Chang, Matthews, von Känel and Jennings2020). This was evidenced in one study that utilized both physiological and prospective self-report VMS monitoring among a sample of predominantly White peri- and postmenopausal adults enrolled in the MsHeart Study, which identified an association between childhood maltreatment and physiologically documented VMS during sleep but not wake (Carson & Thurston, Reference Carson and Thurston2019). Additionally, the observed difference between hot flashes and night sweats may in part be due to differential recall of waking and sleep VMS. Previous research has found that individuals who are at neither extreme of symptom frequency often underreport when using retrospective reporting (Crawford et al., Reference Crawford, Avis, Gold, Johnston, Kelsey, Santoro, Sowers and Sternfeld2008). As VMS frequency is positively associated with severity, relying on recall may also result in underreporting from individuals with milder symptoms (Crawford et al., Reference Crawford, Avis, Gold, Johnston, Kelsey, Santoro, Sowers and Sternfeld2008). This is further supported by other studies that have indicated that menopausal adults underreport VMS compared to physiological monitoring (Fu et al., Reference Fu, Matthews and Thurston2014; Mann & Hunter, Reference Mann and Hunter2011). It is possible that individuals in this sample who did not perceive sleep disturbances may have underreported night sweats.
Variation in the timing of menopause is an important factor when assessing long-term health risks associated with the menopausal transition. Latine adults in the US have been shown to reach menopause earlier than non-Latine White adults, specifically with non-US-born Latine adults reaching menopause the earliest compared to their US-born counterparts (Henderson et al., Reference Henderson, Bernstein, Henderson, Kolonel and Pike2008). This difference is exemplified by the average age of menopause being 52 years in the US, compared to 47.8–47.9 years among people in Mexico (Gold et al., Reference Gold, Crawford, Avis, Crandall, Matthews, Waetjen, Lee, Thurston, Vuga and Harlow2013; Legorreta et al., Reference Legorreta, Montaño, Hernández, Salinas and Hernández-Bueno2013; Sievert et al., Reference Sievert, Huicochea-Gómez, Cahuich-Campos, Whitcomb and Brown2021). Comparatively, the average age at menopause in this sample of predominately non-US born Latine adults is 49.9 years. However, it may also be beneficial to expand this perspective to include the onset and overall duration of the menopausal transition and associated symptoms such as VMS. In the US, VMS lasts on average 7.4 years but has been found to last a median of nearly 12 years for individuals who begin to experience VMS during premenopause and early perimenopause (Avis et al. Reference Avis, Crawford, Greendale, Bromberger, Everson-Rose, Gold, Hess, Joffe, Kravitz, Tepper and Thurston2015). In our sample, this may be indicative of a prolonged menopausal transition for the 31.1% of premenopausal adults who reported experiencing VMS. Prolonged experience of VMS is of particular concern as VMS are associated with poor mental health, reduced quality of life, elevated cardiovascular risk, and reduced bone health (Biglia et al., Reference Biglia, Cagnacci, Gambacciani, Lello, Maffei and Nappi2017; Crandall et al., Reference Crandall, Aragaki, Cauley, Manson, LeBlanc, Wallace, Wactawski-Wende, LaCroix, O’Sullivan, Vitolins and Watts2015; Muka et al., Reference Muka, Oliver-Williams, Colpani, Kunutsor, Chowdhury, Chowdhury, Kavousi and Franco2016; Nappi et al., Reference Nappi, Kroll, Siddiqui, Stoykova, Rea, Gemmen and Schultz2021; Utian, Reference Utian2005; Worsley et al., Reference Worsley, Bell, Gartoulla, Robinson and Davis2017). Further research should consider the role of ACEs in relation to the onset of VMS independent of menopause status.
This study should be interpreted in light of several limitations. The specificity of this study sample limits the generalizability of the findings to the broader US Latine population. Further, the observational and cross-sectional design of the study does not allow for the assessment of causal relationships between ACEs and VMS. The use of self-reported data introduces the potential for recall bias, affecting participants’ ability to accurately report age at menarche, age at menopause, and frequency of VMS. Additionally, the use of Western biomedical terminology, even when translated into Spanish (e.g., ‘hot flashes or flushes’), may have resulted in symptom underreporting. ACEs were measured via retrospective self-report, which is prone to underreporting, and the study utilizes cumulative scores for ACEs, which limits the ability to assess the differential impact and effect sizes of specific ACE types. Additionally, the ACEs questionnaire does not capture frequency or duration of exposure, such that we are unable to evaluate the impacts of any dose–response relationships or shorter vs. extended duration of ACEs. The structure of the menstrual cycle questionnaire only allowed a partial assessment of hormonal contraceptive use and could introduce misclassification in our exclusion criteria; participants were only asked about use of hormonal contraceptives in the context of their reason for cycle regularity or the reason their periods stopped, rather than as a universal screening question. Additionally, participants were not asked about hormone replacement therapy. This could lead to under-identification of participants who should have otherwise been excluded. Other limitations include the small sample size, particularly of peri- and postmenopausal individuals within our cohort; this resulted in limited precision such that wide CIs made it difficult to draw conclusions even when point estimates were meaningful.
Future work should consider examining the associations between prospectively collected ACEs measures—including the frequency and duration of ACEs—with menopausal timing and VMS; whether ACEs are associated with the frequency and severity of VMS; and the potential underlying mechanisms linking early-life adversity to menopausal symptoms. Moreover, future work may consider utilizing mediation analyses or longitudinal data to assess the effects of ACEs on the menopausal transition via downstream pathways. Additionally, given the elevated burden of menopausal symptoms and associated health risks among marginalized communities, further research should examine these associations among other racial/ethnic minority groups in order to identify factors influencing observed differences in symptom burden and inform targeted interventions.
Conclusion
In this study of mid-life Latine adults living in an agricultural community in California, we found that ACEs were associated with the experience of VMS; associations with age at menopause were highly imprecise, although effect estimates were in the opposite direction we hypothesized. ACEs were highly prevalent in this sample, with more than half of the participants reporting at least one early-life adversity. These data suggest that the experience of stressors in early life may have lasting impacts on female reproductive health; however, additional research is needed to better elucidate the mechanistic role of fast life history trade-offs in shaping menopausal experiences at mid-life. Our findings highlight the importance of a lifespan perspective when considering symptomatology among racial and ethnic minority populations throughout the menopausal transition.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/ehs.2026.10049.
Acknowledgements
We gratefully acknowledge the CHAMACOS field staff, community partners, the participants, and their families. Thank you Dr. Lynnette Leidy Sievert, for providing helpful feedback on the manuscript and Kelsey MacCuish for code review.
Author contributions
AWK, JMT, MW, and KGH conceptualized and designed the study. LEC and KRK conducted data gathering and curation. SAGZ performed statistical analyses and wrote the article. AWK, KGH, JD, KRK, MW, LEC, BE, and JMT reviewed and edited the article.
Financial support
This work was supported by the National Institute of Environmental Health Sciences (BE, grant number R01ES026994); the National Institute on Aging (JMT, grant number R01AG069090); the National Institute of Environmental Health Research (KGH, grant number U24ES028529); and the Graduate Research Fellowship, National Science Foundation (SAGZ, grant number DGE 2146752). This material is based upon work supported by the National Science Foundation Graduate Research Fellowship Program under Grant No (DGE 2146752). Any opinions, findings, and conclusions or recommendations expressed in this material are those of the author(s) and do not necessarily reflect the views of the National Science Foundation. The CHAMACOS Study was established and followed longitudinally with support from NIEHS (BE, grant numbers P01 ES009605,R01 ES017054), EPA (BE, grant numbers R82670901, RD83171001, RD83451301), and NIDA (JD, grant number R01 DA035300).
Competing interests
SAGZ, AWK, KGH, JD, KRK, MW, LEC, BE, and JMT declare none.
Research transparency and reproducibility interest
These data (de-identified) and associated documentation/metadata will be made available to others in the scientific community upon reasonable request as permitted by relevant institutional review boards and under a data-sharing agreement consistent with the University of California data-sharing policies (https://cerch.berkeley.edu/investigators).




 Open access
Open access