


Introduction
The European School Survey Report on Alcohol and Other Drugs (ESPAD) report investigated recent substance use among 15–16-year-olds across Europe, noting 47% reported alcohol use, 20% cigarette use, and 7.1% cannabis use. Irish rates are 37%, 16%, and 9%, respectively (ESPAD 2020). Beyond single-substance prevalence, recent non-clinical evidence from Ireland indicates that concurrent use of these substances is common, with 43% engaged in cannabis, alcohol and tobacco by age 20 (Brennan et al. Reference Brennan, Mongan, Doyle, Millar, Cavallaro, Zgaga, Smyth, Nixon, Ivers, Galvin, Walsh, McCrory and McCarthy2026). Earlier European estimations also suggested substantial levels of adolescent polysubstance use, with nearly 30% of 15–16-year-olds across 22 countries engaged in polysubstance use, defined as the consumption of two or more substances (EMCDDA 2009). Polysubstance use is likewise evident in clinical settings. In Ireland, 57% of substance use treatment cases in 2022 involved polysubstance use, with cannabis (40%) and alcohol (36%) being the most common co-morbid substances (Ivers et al. Reference Ivers, Killeen and Keenan2022; O’Neill et al. Reference O’Neill2023; Tomczyk et al. Reference Tomczyk, Isensee and Hanewinkel2016).
Single substance use during adolescence, such as cannabis, alcohol, or nicotine (including e-cigarettes), is associated with adverse mental health outcomes, including psychosis, mania, depression, anxiety, and suicidal ideation (Aseltine et al. Reference Aseltine, Schilling, James, Glanovsky and Jacobs2009; Becker et al. Reference Becker, Arnold, Ro, Martin and Rice2021; Cederlöf et al. Reference Cederlöf, Kuja-Halkola, Larsson, Sjölander, Östberg, Lundström, Kelleher and Lichtenstein2017; Chang et al. Reference Chang, Sherritt and Knight2005; Di Forti et al. Reference Di Forti, Marconi, Carra, Fraietta, Trotta, Bonomo, Bianconi, GardnerSood, OConnor, Russo, Stilo, Marques, Mondelli, Dazzan, Pariante, David, Gaughran, Atakan, Iyegbe and Murray2015; Di Forti et al. Reference Di Forti, Quattrone, Freeman, Tripoli, Gayer-Anderson, Quigley, Rodriguez, Jongsma, Ferraro, La Cascia, La Barbera, Tarricone, Berardi, Szöke, Arango, Tortelli, Velthorst, Bernardo, Del-Ben and van der Ven2019; Fergusson et al. Reference Fergusson, Boden and Horwood2009; Ferreira et al. Reference Ferreira, Jardim, Sousa, Rosa and Jardim2019; Flensborg-Madsen et al. Reference Flensborg-Madsen, Mortensen, Knop, Becker, Sher and Grønbaek2009; Gobbi et al. Reference Gobbi, Atkin, Zytynski, Wang, Askari, Boruff, Ware, Marmorstein, Cipriani, Dendukuri and Mayo2019; Lima et al. Reference Lima, Sims and O’Donnell2020; Livingston et al. Reference Livingston, Chen, Kwon and Park2022; Marconi et al. Reference Marconi, Di Forti, Lewis, Murray and Vassos2016). Polysubstance use has been linked to more severe mental health outcomes, though causality remains unclear within a topic with limited research i.e., it is unclear if existing psychopathology increases vulnerability to polysubstance use, or if indeed there is shared underlying risk factors which explain both (Steinfeld and Torregrossa Reference Steinfeld and Torregrossa2023). Furthermore, evidence to date undervalues the critical component nicotine plays in substance administration, such as cannabis and tobacco in a cigarette (Bunting et al. Reference Bunting, Shearer, Linden-Carmichael, Williams, Comer, Cerdá and Lorvick2024).
Within the available evidence, cross-sectional associations have demonstrated the relationship between increased usage (including legal and illicit substances e.g., alcohol, opioids, etc) and lower emotional well-being, heightened depression and anxiety, as well as increased psychotic symptoms, though cross-sectional associations do not establish directionality (Connor et al. Reference Connor, Gullo, Chan, Young, Hall and Feeney2013; Inchausti et al. Reference Inchausti, Gorostiza, Gonzalez Torres and Oraa2022; Jongsma et al. Reference Jongsma, Turner, Kirkbride and Jones2019; Kelly et al. Reference Kelly, Chan, Mason and Williams2015; Weerakoon et al. Reference Weerakoon, Henson-Garcia, Abraham, Vidot, Messiah and Opara2025). However, a systematic review exploring patterns of substance use among adolescents, reported only 16% of studies included data on both substance use combinations and mental health indicators, such as externalising and internalising problems (Halladay et al. Reference Halladay, Woock, El-Khechen, Munn, MacKillop, Amlung, Ogrodnik, Favotto, Aryal, Noori, Kiflen and Georgiades2020). Therefore, research gaps persist, including limited diverse populations, sparse evidence of co-occurring polysubstance use and mental health symptoms, and lack of standardised measurements.
In a sample of 231 youth, cannabis was reported as a significant correlate of psychopathology, including psychotic experiences (PE), with the largest effect size compared to other substances i.e., almost threefold increased odds (Colins et al. Reference Colins, Vermeiren, Vreugdenhil, Schuyten, Broekaert and Krabbendam2009). However, prior research found that while cannabis use was associated with higher schizotypy scores, the relationship was largely accounted for by polydrug use, including nicotine, ecstasy, etc. Furthermore, individuals who used both cannabis and other substances reported greater psychosis-like symptoms compared to those who used only cannabis (Van Dam et al. Reference Van Dam, Earleywine and DiGiacomo2008). A systematic review exploring PE reported significant concerns involving substance use, particularly cannabis, noting its major contribution in the incidence rather than persistence, of such experiences (Staines et al. Reference Staines, Healy, Murphy, Byrne, Murphy, Kelleher, Cotter and Cannon2023). However, this review did not account for polysubstance use as a risk factor or assess whether the included studies considered co-occurring substance misuse. Therefore, from the available evidence, polysubstance use is consistently associated with higher levels of externalising and internalising concerns, albeit restricted by the limitations mentioned above. On the other hand, far less evidence is available regarding the relationship between commonly accessible polysubstance use and PE, particularly during adolescence. Additionally, available evidence is primarily cross-sectional, and the association between polysubstance use and mental health is theoretically bidirectional, with both factors mutually reinforcing each other.
Patterns of single and polysubstance use frequently vary by gender, with males being more prone to these behaviours (Brennan et al. Reference Brennan, Mongan, Doyle, Millar, Cavallaro, Zgaga, Smyth, Nixon, Ivers, Galvin, Walsh, McCrory and McCarthy2026; Goodwin et al. Reference Goodwin, Moskal, Marks, Clark, Squeglia and Roche2022). Evidence from Growing up in Ireland data similarly found that polysubstance was more common among men (Brennan et al. Reference Brennan, Mongan, Doyle, Millar, Cavallaro, Zgaga, Smyth, Nixon, Ivers, Galvin, Walsh, McCrory and McCarthy2026). However, evidence is mixed, with other recent data has indicated a shift in usage patterns, with no significant difference in cannabis use reported between adolescent males and females, indicating the need for gender-related evidence (O’Dowd et al. Reference O’Dowd, Fleury, Power, Dooley, Quinn, Petropoulos, Healy, Smyth and Cannon2024). However, of those engaging in substance use (alcohol, cannabis, nicotine, and other illicit substances), existing evidence suggests that a higher proportion of adolescent females experience internalising behaviours (Baggio et al. Reference Baggio, Studer, Mohler-Kuo, Daeppen and Gmel2014; Edokpolo et al. Reference Edokpolo, Nkire and Smyth2010; Trudeau et al. Reference Trudeau, Spoth, Randall and Azevedo2007). Research on gender-diverse populations also remains limited, predominantly restricted to adult cohorts, and gender identities underexplored (Goodwin et al. Reference Goodwin, Moskal, Marks, Clark, Squeglia and Roche2022; Halladay et al. Reference Halladay, Woock, El-Khechen, Munn, MacKillop, Amlung, Ogrodnik, Favotto, Aryal, Noori, Kiflen and Georgiades2020). A review exploring substance use in gender-diverse populations highlighted the increased risk of mental health concerns among transgender individuals engaging in substance and polysubstance use (Cotaina et al. Reference Cotaina, Peraire, Boscá, Echeverria, Benito and Haro2022). Of the 20 included articles, a small proportion examined youth and only one study was conducted in Europe, leading the reviewers to call for further research into the experiences and specific needs of this population (Cotaina et al. Reference Cotaina, Peraire, Boscá, Echeverria, Benito and Haro2022).
This study aims to explore the cross-sectional associations between polysubstance use and psychopathology in a large population based sample of young people in Ireland. A secondary aim is to explore gender differences in the relationship between polysubstance use and mental health outcomes.
Methods
Study design
This study analysed biannual cross-sectional adolescent data from the Planet Youth Programme Ireland East, collected in 2021 around the time of the COVID-19 pandemic and associated restrictions (Dooley et al. Reference Dooley, Power, Healy, Cotter and Cannon2024; Planet Youth Partner Ireland, 2021). The Icelandic Prevention Model developed by the Icelandic Centre for Social Research and Analysis (ICSRA) at Reykjavik University, was created to reduce Icelandic youth substance use rates (Sigfúsdóttir et al. Reference Sigfúsdóttir, Thorlindsson, Kristjánsson, Roe and Allegrante2009). This is a collaborative upstream model created in the early 1990s to identify and reduce factors related to youth substance use within the community (Halsall et al. Reference Halsall, Lachance and Kristjansson2020), through the use of repeated surveys (Carver et al. Reference Carver, McCulloch and Parkes2021). The Planet Youth Programme Ireland East surveys were completed on computers or tablets in September–November 2021. The survey was completed in a mix of urban, suburban, and rural areas (North Dublin, Cavan, and Monaghan). Secondary schools and YouthReach centres (a national programme for early school departures) were also invited.
Participants
The target population were fourth/fifth year secondary school students i.e., approximately aged 15–16 years. Students and parents of participating schools were given information about the survey and an opt-out option.
Ethical information
The study employed an opt-out consent process wherein participants were automatically included unless they, or their parents, actively declined participation. This approach is justified in contexts where participation poses minimal risk and explicit opting-in may reduce response or introduce selection bias. All eligible pupils and their parents received information detailing the study’s objectives, procedures, and privacy safeguards. Alternative activities were organised for students who were opted out of the study. After survey completion, participants were provided information on mental health, social care, and well-being services in their community. The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committee on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008. The authors assert that ethical approval for publication of this study has been provided by their local Ethics Committee (Research Ethics Committee of the Royal College of Physicians in Ireland RECSAF 144; dated 21st June 2021).
Predictors
Polysubstance use is defined as the use of more than one substance, characterised by the substances involved (e.g., number, type), timing (e.g., daily, weekly, monthly), and intent (e.g., intentional or unintentional) (Bunting et al. Reference Bunting, Shearer, Linden-Carmichael, Williams, Comer, Cerdá and Lorvick2024). In this study, polysubstance use was measured using four survey items assessing cannabis, alcohol, cigarettes, and e-cigarette use within the past 30 days. Cigarettes and e-cigarettes were combined into a single ‘nicotine’ variable. Responses to all items ranged from ‘never’ to ‘40 times or more’. For the purpose of analyses, responses were collapsed into ‘never’ or ‘ever.’ Any reported use of a substance within the past month, regardless of frequency, was classified as ‘ever.’ These base variables were used to create the polysubstance use predictor: ‘Cumulative Polysubstance use’
-
Cumulative polysubstance use: To examine the quantity and cumulative effect of polysubstance use, the ‘cumulative polysubstance use’ variable was created. This was based on a count of the type of substances used within the past 30 days. Levels included ‘None’ (reference) to ‘three substances’.
Outcomes: psychopathology measures
Measures included the Adolescent Psychotic-like Symptoms Screener (APSS; Kelleher et al. Reference Kelleher, Harley, Murtagh and Cannon2011) and the Strengths and Difficulties Questionnaire (SDQ; Goodman Reference Goodman1997). All binary transformations presented were derived from established, psychometrically validated cut-off scores indicating significant mental health concerns.
-
Psychotic Experiences
-
APSS: This self-reported instrument includes 7-items indicating PE and has been validated against clinical interviews (Kelleher et al. Reference Kelleher, Harley, Murtagh and Cannon2011). Respondents can select one of the following responses; ‘not true’, ‘somewhat true’ or ‘definitely true’. A binary outcome consisting of a score of 2 or over was used, indicating endorsement of PE.
-
General Psychopathology
-
SDQ: This self-reported questionnaire includes 25 items assessing emotion, conduct, hyperactivity/inattention, peer and pro-social behaviours. For the purposes of this study, respondents can select one of the following; ‘not true’, ‘somewhat true’ or ‘certainly true’. The total difficulties scores of 20 or more, was deemed as clinically relevant and psychopathology. This cut-off refers to ‘very high’ scores with respect to population norms (4-band categorisation for 4–17-year-olds; https://www.sdqinfo.org/py/sdqinfo/c0.py) indicating likely psychopathology (Goodman and Goodman Reference Goodman and Goodman2009; Goodman et al. Reference Goodman, Meltzer and Bailey1998; Lundh et al. Reference Lundh, Wångby-Lundh and Bjärehed2008; Muris et al. Reference Muris, Meesters and van den Berg2003; Vugteveen et al. Reference Vugteveen, de Bildt, Theunissen, Reijneveld and Timmerman2021).
-
SDQ-Int: This was derived from the SDQ by combining; emotional and peer behaviour subscales. A binary outcome was used, with scores over 10 indicating internalising psychopathology including depression, anxiety, or other emotional behavioural difficulties (Goodman and Goodman Reference Goodman and Goodman2009).
-
SDQ-Ext: This was derived from the SDQ by combining; conduct and hyperactivity subscales. A binary outcome was used, with scores over 11 indicating externalising psychopathology including outwardly directed conduct behavioural difficulties (Goodman and Goodman Reference Goodman and Goodman2009).
Co-variates
-
Gender: Individuals were asked about their gender identity, choosing from four categories (male/female/transgender or non-binary/prefer not to say). Gender identity was collapsed to ‘male’ (reference), ‘female’ and ‘gender diverse’, the latter of which also included questioning youth who selected ‘prefer not to say’.
-
Socio-economic status: Individuals were asked how well off financially they think their family was in comparison to other families. Responses ranged from ‘much worse off’ to ‘similar to others’ to ‘much better off’. This was collapsed to ‘low’ ‘middle’(reference) and ‘high’.
-
Urbanicity: The questionnaire was completed in three locations (North Dublin, Cavan and Monaghan). Regions included the sample contain a spectrum of urban-rural areas. However, given that Dublin is predominantly urban and both Cavan Monoghan are predominantly rural, these were collapsed to a binary variable (Urban/Rural), with North Dublin defined as Urban (reference).
-
Ethnicity: Individuals were asked to select the ethnic/cultural group which aligned with their identity i.e., white Irish (reference), other white background, or Black, Asian or other minority.
Data analysis
We report the descriptive statistics when stratified into those with and without each outcome (see Table 1). Associations between outcomes and exposure were explored using separate mixed-effects logistic regression models (schools were used as a random effect). Within these models, the reference category was ‘no substance use’ to estimate associations between each substance-use pattern and outcomes relative to substance-naïve participants, to provide a clear, policy-relevant reference point. Multivariable models adjusted for all covariates (socio-economic status, urbanicity, gender and ethnicity). Assumptions were assessed including tests for multicollinearity using variance inflation factors. Odds ratios were reported with 95% confidence intervals and the significance level set at 5% (p < 0.05). Gender analyses were investigated by stratification of each model by gender groups (male, female, gender-diverse). Gender × polysubstance use interaction terms were initially considered and examined for moderation effects. However, small cell sizes across several gender and polysubstance use categories limited statistical power. As such, interactions terms were not retained in the final model. A false discovery rate (FDR) correction was applied across all models, including gender-stratified models, to account for multiple comparisons. Statistical analysis software was STATA, version 18. Interpretations of small (i.e., OR < 1.5), medium (i.e., OR ≈ 3.5) and large (i.e., OR > 5) effect sizes were in line with previous recommendations (Chen et al. Reference Chen, Cohen and Chen2010; Rosenthal Reference Rosenthal1996). In line with the cleaning process performed in Reykjavik, respondents were removed for a series of reasons, i.e., insufficiently completed surveys (<15%), insufficient demographical data, reporting a fictitious drug, or reporting trying all substances (Data Center - Planet Youth, 2024).
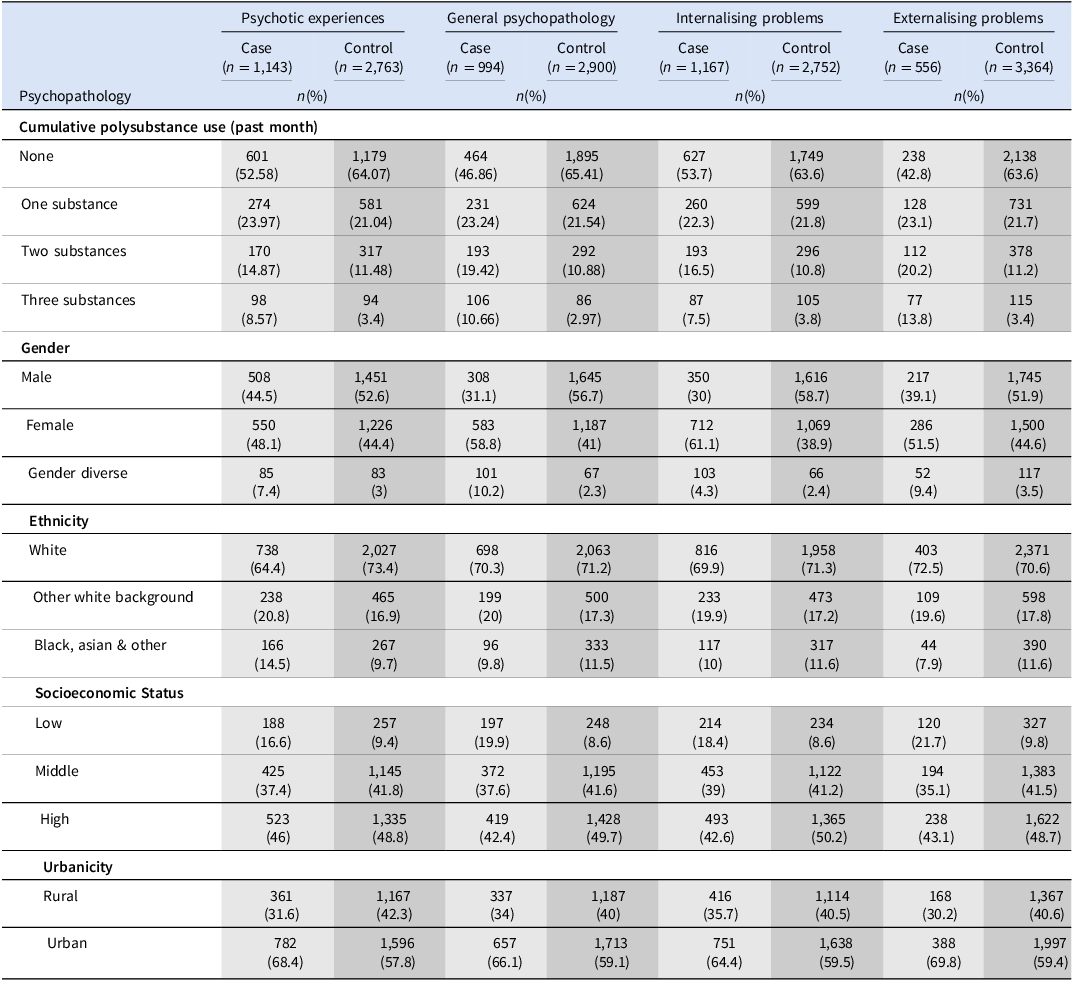
Demographics of the sample when stratified by psychopathology outcome

Note: Cases are individuals with the outcome of interest, while controls are those without it. Urbanicity includes Cavan and Monaghan (Rural) and North Dublin (Urban). Gender-diverse includes transgender/non-binary individuals and prefer-not-to-say. Please note, the non-mutual exclusivity between all outcome stratified groups.
Results
Sample characteristics
A total of 45 schools were invited to participant in the survey, with 40 schools agreeing to surveying (88.9%). Response rates and other characteristics of the data can be found in prior publications (Dooley et al. Reference Dooley, Power, Healy, Cotter and Cannon2024; O’Dowd et al. Reference O’Dowd, Fleury, Power, Dooley, Quinn, Petropoulos, Healy, Smyth and Cannon2024). We found that, 29.3% of the sample reported PE and 25.5% met the criteria for general psychopathology (SDQ > 20). 29.8% had internalising behaviours (SDQ-Int > 10) and 14.2% had externalising behaviours (SDQ-Ext > 11). Sixty per cent were substance naïve within the past 30 days, 22.3% engaged in single substance use, while 12.4% and 4.9% of the sample had used two and three substances, respectively. Over 50% of individuals engaging in polysubstance use (two or more substances) met the criteria for general psychopathology. 45.3% of youth engaging in polysubstance use (three substances) met the criteria for internalising problems, while 40.1% met the criteria for externalising behaviours. Over half (51%) of young people engaging in polysubstance use (three substances) reported PE (see Table 1).
Univariable and multivariable analyses
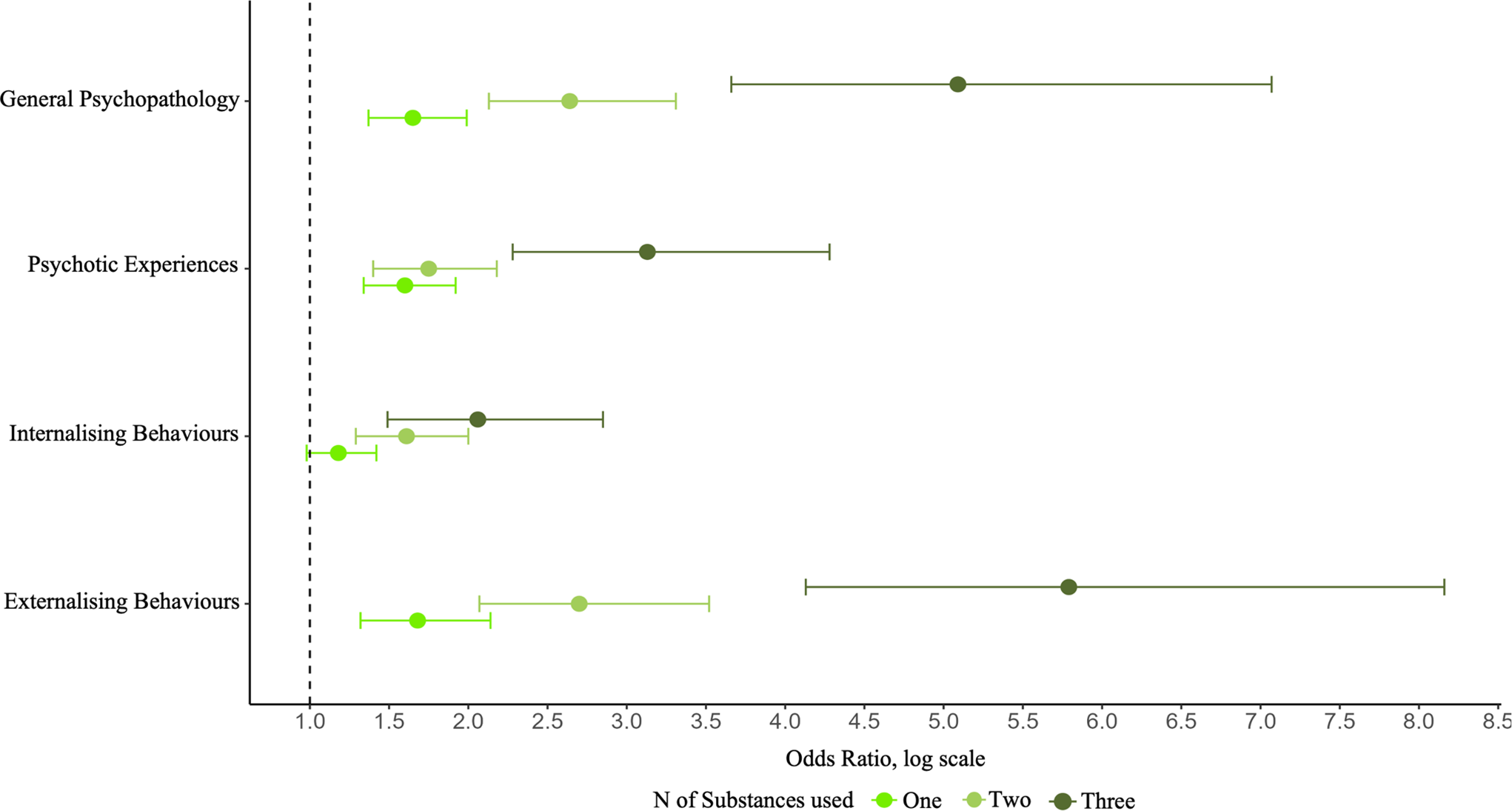
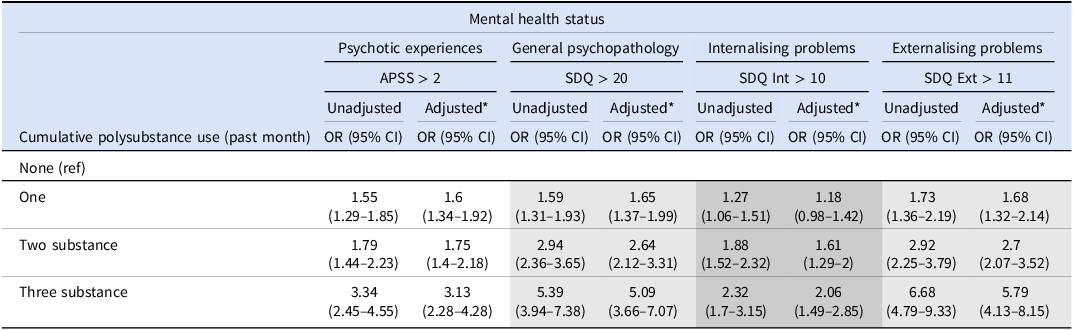
The unadjusted and adjusted odds ratios for the relationship between polysubstance use and each outcome are reported in Table 2. A stepwise increase in the odds of psychopathology was observed with each additional substance used in the past month. Using any one substance (cannabis, alcohol or nicotine) was associated with an increased odds of PE, general psychopathology, and externalising behaviours (aOR range: 1.2–1.7). Dual substance use was also associated with a significant increase in the odds of all outcomes (aOR range: 1.6–2.9). Using all three substances was strongly associated with externalising behaviours (aOR: 5.8), and internalising behaviours (aOR: 2.1) (see Figure 1). Broadly, adjustment for confounders had limited impact on the effect size of any of these associations (see Table 2). After applying the false discovery rate (FDR) correction for multiple comparisons, all previously significant associations remained robust (adjusted p < 0.001).
Multivariable analysis of the associations between polysubstance use and each outcome of psychopathology.

Univariable and multivariable analyses of the associations between ‘cumulative polysubstance use’ and psychopathology

Note: *adjusted for gender, ethnicity, socioeconomic status, and urbanicity. OR= odds ratio. CI = confidence interval.
Gender analyses
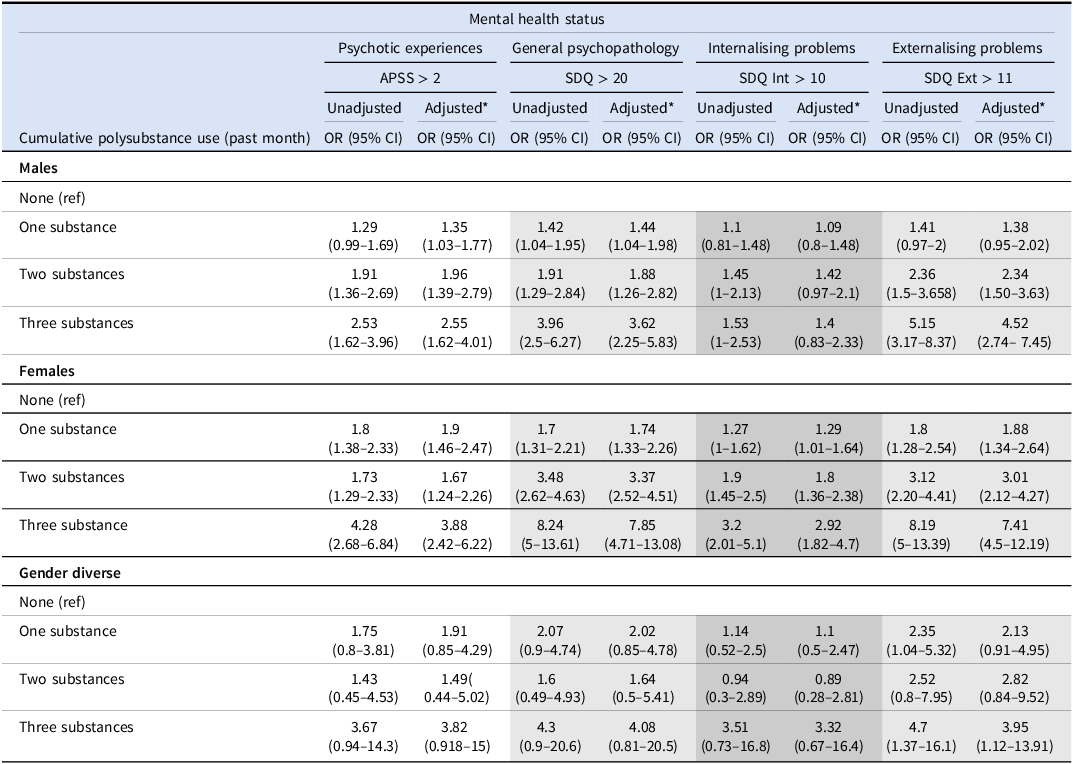
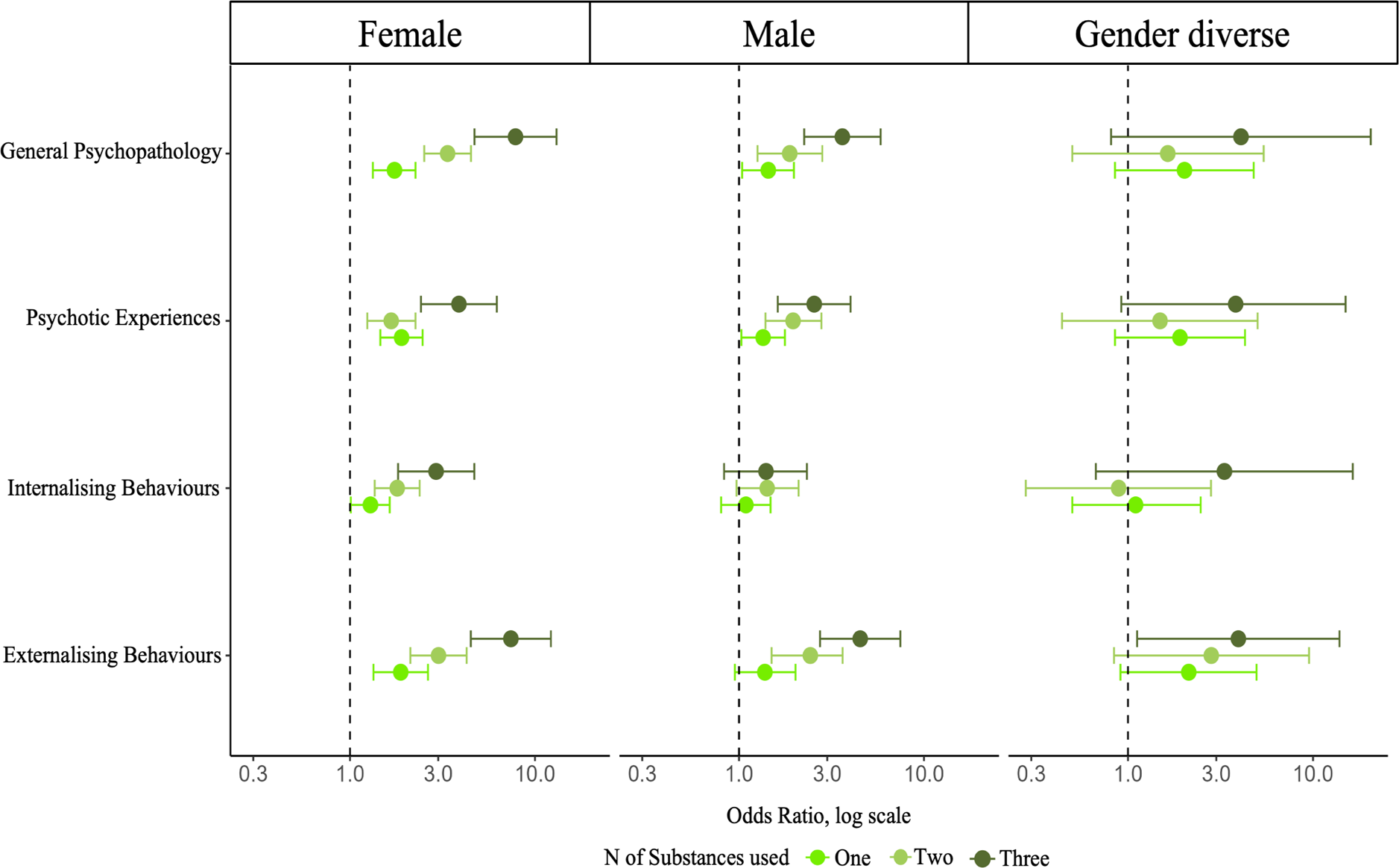
Gender stratified analyses including unadjusted and adjusted odds ratios are found in Table 3. Males engaging in single substance use (cannabis, alcohol, or nicotine) compared to substance-naive males demonstrated weak to moderate significantly increased odds for PE and general psychopathology (aOR range: 1.3–1.4). A stepwise increase in the odds was apparent for males engaging in two substances (aOR range: 1.8–2.3) across all outcomes apart from internalising behaviours, where no association was found. Similarly, polysubstance use (three substances) in males was not associated with internalising behaviours; however, moderate to strong increased odds were found for PE, general psychopathology, and externalising behaviours (aOR range: 2.5–4.5).
Gender-stratified univariable and multivariable regression analyses of the associations between ‘cumulative polysubstance use’ and psychopathology

Note: Model 1 was univariable. Model 2 was adjusted for ethnicity, socioeconomic status, and urbanicity. OR = odds ratio. 95% CI = 95% confidence interval.
Females engaging in all forms of substance use (single or polysubstance) were found to have higher odds of each outcome. A large stepwise increase in the odds was apparent for females engaging in polysubstance use (two), particularly for general psychopathology (aOR: 3.4 and externalising behaviours (aOR: 3). Females engaging in all three substances were strongly associated with all outcomes, most notably PE (aOR: 3.9) and externalising behaviours (aOR: 7.4).
Gender-diverse individuals engaging in polysubstance use (three substance) were at significant risk of externalising behaviours once covariates were controlled for (aOR range: 2.1–3.9) (Figure 2). Again, after applying the FDR correction for multiple comparisons to all gender-stratified models, all previously significant associations remained robust (adjusted p < 0.001).
Gender-stratified multivariable analysis for the associations between polysubstance use and each outcome of psychopathology.

Discussion
This study examined the cross-sectional associations between polysubstance use and psychopathology, with a secondary aim to explore gender differences. Overall general psychopathology, internalising/externalising behaviours, and PE were examined with the exposure variable ‘cumulative polysubstance use’. The prevalences of mental health concerns reported above may be higher compared to other studies, due to the timing of the surveys analysed as part of this study, i.e., the first wave of COVID-19 in Ireland, when lockdown conditions were associated with elevated rates of adolescent mental health concerns (Dooley et al. Reference Dooley, Power, Healy, Cotter and Cannon2024). Furthermore, other studies using repeated population-based surveys have similarly shown that adolescent mental health symptoms increased during the pandemic and, although some improvement has been observed post-pandemic, symptom levels remained elevated relative to pre-pandemic baselines (Haskell et al. Reference Haskell, Sigmarsdottir, Thorisdottir, Valborgarson, Bonilla Aparicio, Kiviruusu, Suvisaari, Chang, Ystrom, Butwicka, Asgeirsdottir, Valdimarsdottir, Sigfusdottir, Allegrante and Halldorsdottir2025). The results from this study indicate two notable findings: 1; Polysubstance use (i.e., two or three substances) during adolescence is associated with significantly increased odds, particularly for general psychopathology, and externalising concerns. Furthermore, 40.1% to 55.4% of individuals engaging in polysubstance use (three substances) had at least one form of psychopathology, 2; females engaging in polysubstance use were more likely to exhibit psychopathology and had stronger associations with psychopathology than males and gender diverse.
Psychotic experiences
Polysubstance use was strongly associated with PE, with adjusted odds ratios ranging from small (aOR: 1.7) to moderate (aOR: 3.1), depending on the number of substances used. These findings align with previous research highlighting a significant association between PE and substance use, as well as substance use disorder, with a threefold increased hazard ratio (Cederlöf et al. Reference Cederlöf, Kuja-Halkola, Larsson, Sjölander, Östberg, Lundström, Kelleher and Lichtenstein2017; Staines et al. Reference Staines, Healy, Murphy, Byrne, Murphy, Kelleher, Cotter and Cannon2023). Gender-stratified analyses revealed notable differences: females using three substances had nearly four-fold increased odds of PE compared to non-using females, whereas the association was non-significant among gender-diverse individuals and lower among males (a two-and-a-half-fold increase). This novel finding reports the heightened risks associated with polysubstance use among young females. Interestingly, these results contrast with the broader literature, which predominantly links increased psychosis risk to males (Jongsma et al. Reference Jongsma, Turner, Kirkbride and Jones2019). However, prior research has also highlighted significant challenges in replicating gender differences in studies on PE (Staines et al. Reference Staines, Healy, Murphy, Byrne, Murphy, Kelleher, Cotter and Cannon2023), emphasising the need for continued gender-specific research (Goodwin et al. Reference Goodwin, Moskal, Marks, Clark, Squeglia and Roche2022; Ruppert et al. Reference Ruppert, Kattari and Sussman2021). These findings have direct implications for policymakers and clinicians, particularly in treatment settings such as first-episode psychosis services (McDonell and Oluwoye Reference McDonell and Oluwoye2019). Given the complexity of polysubstance use, including cannabis, treatment approaches may require tailored interventions rather than a one-size-fits-all model (Mefodeva et al. Reference Mefodeva, Carlyle, Walter, Chan and Hides2022).
General psychopathology
There was a significant association between polysubstance use and psychopathology, ranging from small increased odds (aOR: 1.6) for single substance users, to large increased odds for those using three substances (aOR: 5.09). These findings corroborate the earlier evidence, indicating a significant relationship between polysubstance use and psychopathology (Connor et al. Reference Connor, Gullo, Chan, Young, Hall and Feeney2013; Kelly et al. Reference Kelly, Chan, Mason and Williams2015). Females engaging in polysubstance use had the highest increased odds of psychopathology of all gender groups (aOR range: 1.7–7.8). The elevated odds for females are particularly striking and exceed previous evidence (Baggio et al. Reference Baggio, Studer, Mohler-Kuo, Daeppen and Gmel2014; Edokpolo et al. Reference Edokpolo, Nkire and Smyth2010; Garcia-Cerde et al. Reference Garcia-Cerde, Lopes de Oliveira, Ferreira-Junior, Caetano and Sanchez2023). This suggests that females engaging in polysubstance use are a notable high-risk group and may require specific monitoring. This observed increase may also be of interest to those within treatment services, identifying gender-specific treatment pathways, differences in case presentation and ensuring effective accommodations to these unique needs.
Internalising behaviors
Characterised by depression, anxiety, and decreased emotional well-being (Goodman Reference Goodman1997), small increased odds were found for single substance users (aOR: 1.2), compared to moderately increased odds for polysubstance users (aOR: 2.06). These findings add to the limited body of existing research, as previously highlighted i.e., only 16% of studies had data on both substance use combinations and mental health indicators (Garcia-Cerde et al. Reference Garcia-Cerde, Lopes de Oliveira, Ferreira-Junior, Caetano and Sanchez2023; Halladay et al. Reference Halladay, Woock, El-Khechen, Munn, MacKillop, Amlung, Ogrodnik, Favotto, Aryal, Noori, Kiflen and Georgiades2020; Morley et al. Reference Morley, Lynskey, Moran, Borschmann and Winstock2015). Evidence relating to the association between cumulative polysubstance use (including cannabis, alcohol, cigarettes, e-cigarettes and opioids) and severe mental health episodes has indicated significant associations between the number of substances and suicidal thoughts, plans and attempts. Most notable was the four-fold increased odds of suicide attempts for those engaging in three substances (Moss et al. Reference Moss, Chen and Yi2014; Yang Reference Yang2024; Zuckermann et al. Reference Zuckermann, Williams, Battista, Jiang, de Groh and Leatherdale2020). However, this study differs from previous work (Baggio et al. Reference Baggio, Studer, Mohler-Kuo, Daeppen and Gmel2014; Goodwin et al. Reference Goodwin, Moskal, Marks, Clark, Squeglia and Roche2022; Trudeau et al. Reference Trudeau, Spoth, Randall and Azevedo2007) in that the associations between polysubstance use and internalising problems were confined to females, with weak to moderately increased odds depending on the number of substances used (aOR range: 1.29–2.92).
Externalising behaviours
Characterised by conduct and hyperactivity issues (Goodman Reference Goodman1997), we found strong associations between polysubstance use and externalising behaviours (aOR: 5.79). These findings align with data from three Nordic countries showing significant increased odds of externalising behaviours across a variety of substance use patterns (Pedersen et al. Reference Pedersen, Thomsen, Heradstveit, Skogen, Hesse and Jones2018; Ruppert et al. Reference Ruppert, Kattari and Sussman2021). Gender-stratified analyses revealed mixed results: Single and polysubstance-using females had higher odds of externalising concerns (aOR range: 1.88–7.41). Males engaging in polysubstance use also showed significant associations. However, single substance use was not statistically significant. This slightly differs from previous evidence indicating a strong association between single substance use and male externalising behaviours (Masroor et al. Reference Masroor, Khorochkov, Prieto, Singh, Nnadozie, Abdal, Shrestha, Abe and Mohammed2021). A possible explanation for this could be differences in how substance use has been defined in previous studies. Many prior investigations have focused on formal diagnoses of problematic substance use rather than examining substance use more broadly (Pedersen et al. Reference Pedersen, Thomsen, Heradstveit, Skogen, Hesse and Jones2018).
Strengths and limitations
A key strength of this study is the large sample size and school response rate, allowing the exploration of mental health and substance use during adolescence. This study furthers the current understanding of substance use behaviours, including cannabis, bridging gaps in polysubstance use and gender minorities research (Goodwin et al. Reference Goodwin, Moskal, Marks, Clark, Squeglia and Roche2022; Steinfeld and Torregrossa Reference Steinfeld and Torregrossa2023). Furthermore, the manner in which substance use was explored through our exposure variables (i.e., cumulative and specific combinations), allowed for valuable evidence into realistic polysubstance use as highlighted by previous evidence (Bunting et al. Reference Bunting, Shearer, Linden-Carmichael, Williams, Comer, Cerdá and Lorvick2024; Steinfeld and Torregrossa Reference Steinfeld and Torregrossa2023).
An important limitation is due to the cross-sectional nature of this data, causality cannot be established, and temporal directionality of polysubstance use and psychopathology is restricted. As vaping was included and combined with cigarettes under the term nicotine, the exact substance vaped is unknown. Substance use data limited extends further to quantity, reliable frequency, and importantly potency. Given how the data is collected, information related to individuals who did not take part in the study was not made available. Therefore, these individuals may have sociodemographically differed. However, participation rates were very high, giving confidence that the sample was representative. Due to the school-based study design, there is the potential for biased reporting of mental health concerns and substance use i.e., peer pressure. However, the anonymity of the survey is likely to have mitigated against this. While gender × polysubstance use interaction terms were examined, small cell sizes across several gender and polysubstance use categories limited statistical power to detect moderation effects. However, in order to address, we conducted exploratory gender-stratified models, which provided complementary insights.
Conclusion
This study aimed to examine the associations between polysubstance use, and psychopathology among school going adolescents. Findings revealed significant and concerning associations between polysubstance use and measures of psychopathology, particularly in young females. Across all psychopathology measures, female adolescents engaging in single and polysubstance use reported the largest increased odds compared to their female substance-naive counterparts. Future research should explore the longitudinal associations between polysubstance use and psychopathology, having implications for schools teachers, principals and others dealing with young people and their mental health concerns. The observed relationship between substance use and psychopathology highlights the need for staff working in substance use and mental health services to build competencies in addressing problems in the other domain. Rather than focusing solely on single substance prevention campaigns, health professionals should routinely assess polysubstance use. Additionally, public health messaging must emphasise the risks of polysubstance use to young people.
Acknowledgements
We wish to thank all young people who participated in the Planet Youth survey, as well as the school staff and study administrators that facilitated it. Many thanks also the Planet Youth Implementation Team for North Dublin, Cavan and Monaghan (https://planetyouthpartner.ie), including those from the Cavan and Monaghan Education and Training Board (Maureen McIntyre, Collette Deeney), the North Dublin Regional Drug and Alcohol Task Force (Bríd Walsh, David Creed), the North Eastern Regional Drug & Alcohol Task Force (Andy Ogle), and TUSLA (Ste Corrigan).
Author contributions
Conceptualisation, R.F, M.C.; Analysis, R.F. N.D, C.H, L.S; Data Interpretation, R.F, C.H, N.D, L.S, J.H, M.C.; Methodology, R.F, L.S, N.D.; Project administration, R.F.; Writing. R.F.; Reviewing, R.F, M.C, B.S, T.O.D, N.D, J.H, L.S, D.G. All authors have read and agreed to the published version of the manuscript.
Funding statement
R.F was supported by the Health Research Board (grant ILP-PHR-2022-006). F.O.H was supported by the Royal College of Surgeons in Ireland (Research Summer Studentship). J.H was supported by the Health Research Board Psychosis Ireland Structured Training and Research (PSI-STAR) Clinical Doctoral award CDA 2021-0005. N.D was supported by a DOROTHY fellowship (DTHY/2023/1705) which is partially funded by European Union’s Horizon 2020 research and innovation programme under the Marie Skłodowska-Curie grant agreement No 101034345.
Competing interests
The authors declare none.
Ethical standards
The study employed an opt-out consent process wherein participants were automatically included unless they, or their parents, actively declined participation. This approach is justified in contexts where participation poses minimal risk and explicit opting-in may reduce response or introduce selection bias. All eligible pupils and their parents received information detailing the study’s objectives, procedures, and privacy safeguards. Alternative activities were organised for students who were opted out of the study. After survey completion, participants were provided information on mental health, social care, and wellbeing services in their community. The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committee on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008. The authors assert that ethical approval for publication of this study has been provided by their local Ethics Committee (Research Ethics Committee of the Royal College of Physicians in Ireland RECSAF 144; dated 21st June 2021).

 Open access
Open access