



Impact statement
Mental illness affects millions of Nigerians, yet fewer than 1 in 10 people who need mental health care actually receive it. This gap exists not because people are unwilling to seek help, but because the formal health system cannot reach most of the population. In this vacuum, religious leaders like pastors and imams have become the primary mental health providers for millions of people across Nigeria and much of sub-Saharan Africa and South Asia. They are the first visit, the first attempt at understanding what is happening when someone in a family begins to struggle. This research matters because it is the first study to map, at the population level, the diversity of beliefs and attitudes held by religious leaders toward mental illness and to show that this diversity clusters into three distinct groups, each requiring a different engagement approach. Over a third of leaders hold strongly spiritual views of mental illness paired with restrictive social attitudes. Another third are already open to collaboration and need only practical skills and referral tools. A quarter are actively supportive and ready to become community champions. The practical implication is direct: programmes that train all religious leaders the same way are wasting resources on approaches that fit only some of them. A stratified approach (matching the strategy to the profile) is both more effective and more respectful of leaders’ diverse perspectives. Critically, education and prior training are the strongest predictors of supportive attitudes, identifying tractable targets for investment. Nigeria’s Mental Health Act 2021 makes formal faith–health partnerships legally possible. This study provides the evidence base for designing those partnerships wisely and offers a transferable framework wherever religious leaders function as informal mental health gatekeepers.
Introduction
The global mental health treatment gap remains one of the most consequential structural failures of health systems in low- and middle-income countries (LMICs). Across sub-Saharan Africa, fewer than 1 in 10 individuals experiencing a mental health condition receive any evidence-based care, a deficit driven by chronic under-investment, workforce scarcity and the geographic concentration of trained specialists in urban centres that leaves the vast majority of populations without accessible services (Fadele et al., Reference Fadele, Igwe, Toluwalogo, Udokang, Ogaya and Lucero-Prisno2024; Patel et al., Reference Patel, Saxena, Lund, Thornicroft, Baingana, Bolton, Chisholm, Collins, Cooper, Eaton, Herrman, Herzallah, Huang, Jordans, Kleinman, Medina-Mora, Morgan, Niaz, Omigbodun, Prince, Rahman, Saraceno, Sarkar, de Silva, Singh, Stein, Sunkel and UnÜtzer2018). Nigeria illustrates this disparity acutely: with approximately 0.09 psychiatrists per 100,000 population, biomedical mental health care remains structurally inaccessible to most of the country’s population (World Health Organization, 2025). The WHO’s Mental Health Gap Action Programme (mhGAP) and the broader task-sharing movement have established growing evidence base for redistributing defined mental health functions from scarce specialists to trained non-specialist community providers as a pragmatic response to these structural constraints (Eaton et al., Reference Eaton, McCay, Semrau, Chatterjee, Baingana, Araya, Ntulo, Thornicroft and Saxena2011; World Health Organization, 2008). What these frameworks have been slower to address is the role of an already-active, already-trusted and community-embedded tier of informal providers who currently manage much of the unmet need: religious leaders.
Across sub-Saharan Africa, South Asia and comparable pluralistic LMIC contexts, religious leaders (pastors, imams and priests) are among the most consistently documented de facto first contacts for mental distress (Burns and Tomita, Reference Burns and Tomita2015; Williams et al., Reference Williams, Baldeh, Bah, Dennis, Robinson and Adeniyi2025). They offer spiritual support, counselling and crisis management that congregants explicitly understand as responses to mental health problems, situated within meaning-making frameworks that biomedical services often cannot provide. In Nigeria specifically, approximately 26.2% of individuals with mental illness consult a religious leader before any contact with formal services (Adeosun et al., Reference Adeosun, Adegbohun, Adewumi and Jeje2013; Ikwuka et al., Reference Ikwuka, Galbraith, Manktelow, Chen-Wilson, Oyebode, Muomah and Igboaka2016; Coker et al., Reference Coker, Olibamoyo, Adewunmi, Osakwe, Taiwo and Alonge2019), positioning faith communities not as peripheral adjuncts to the health system but as its operational first tier. This pattern is not a Nigerian idiosyncrasy: systematic reviews confirm that religious and traditional healers are central to pathways to care across West Africa, East Africa and South Asia, suggesting that religious leaders constitute a structural feature of informal mental health systems in pluralistic LMICs rather than a culturally specific anomaly (Burns and Tomita, Reference Burns and Tomita2015; Williams et al., Reference Williams, Baldeh, Bah, Dennis, Robinson and Adeniyi2025).
Despite this established role, faith–health integration strategies have overwhelmingly defaulted to uniform engagement approaches: single training curricula, undifferentiated awareness campaigns and one-size-fits-all referral protocols that take no account of the substantial heterogeneity that exists among religious leaders themselves (James et al., Reference James, Igbinomwanhia and Omoaregba2014; Green and Colucci, Reference Green and Colucci2020). It should be acknowledged, moreover, that the informal mental health landscape in Nigeria and much of sub-Saharan Africa extends beyond Christianity and Islam to include practitioners of traditional African religions, whose explanatory models and gatekeeper roles may differ meaningfully from those studied here; their exclusion from this and most prior studies represents a gap with direct implications for the comprehensiveness of faith–health integration frameworks. This is an implementation problem, not merely an evidence gap. A leader who holds primarily biological causal beliefs, endorses benevolence toward people with mental illness and has prior mental health training requires a fundamentally different engagement approach than one who attributes mental illness exclusively to spiritual causes, holds socially restrictive attitudes and has no prior exposure to formal mental health discourse. Treating these as equivalent produces programmes mismatched to their target populations. What has been absent is a population-level typological evidence base capable of estimating not just that heterogeneity exists among religious leaders, but how much of the target population falls into meaningfully distinct profiles, and therefore what the realistic programme demand is for each engagement approach.
Within Nigeria’s pluralistic healthcare ecosystem (where Pentecostal deliverance ministries, Islamic spiritual interventions and an under-resourced biomedical sector operate simultaneously in the same social spaces) (Adebayo, Reference Adebayo2024), religious leaders function as cultural interpreters and informal health gatekeepers whose explanatory models directly shape community-level help-seeking, treatment adherence and the modulation of mental health stigma. Understanding the structure of these models and their attitudinal consequences is a prerequisite for designing interventions that engage with, rather than displace, existing frameworks.
This study is organised around an integrated analytic chain linking three established theoretical frameworks. Kleinman’s Explanatory Models framework (Kleinman et al., Reference Kleinman, Eisenberg and Good1978) provides the primary tool for characterising how causal beliefs structure triage and help-seeking decisions among religious leaders. Link and Phelan (Reference Link and Phelan2001)’s conceptualisation of stigma provides the mechanism through which causal beliefs translate into attitudinal orientations toward people with mental illness. The Community Attitudes toward Mental Illness (CAMI) framework (Taylor and Dear, Reference Taylor and Dear1981) operationalises those orientations across four empirically validated dimensions. The analytic chain is explanatory models structure causal attributions → causal attributions constitute the cognitive foundation of stigma-related attitudes → attitudes cluster into empirically separable typologies with direct implications for implementation planning.
Systematic research across sub-Saharan Africa confirms that spiritual causation is a dominant explanatory model. Studies in Ghana (Osafo, Reference Osafo2016; Kpobi and Swartz, Reference Kpobi and Swartz2018) and Uganda (Teuton et al., Reference Teuton, Bentall and Dowrick2007; Asiimwe et al., Reference Asiimwe, Nuwagaba-Kayongo, Dwanyen and Kasujja2023) document that religious leaders frequently attribute mental disorders to supernatural forces while retaining selective openness to biomedical intervention. Comparable patterns of compassionate-yet-restrictive attitudes have been observed in Lebanon and among South Asian populations (Nguyen et al., Reference Nguyen, Yamada and Dinh2012; Aramouny et al., Reference Aramouny, Kerbage, Richa, Rouhana and Richa2020), suggesting cross-cultural consistency in the co-occurrence of benevolence and social restriction among religious leaders. Within Nigeria, while general population surveys reveal mixed spiritual–biomedical models (Adewuya and Makanjuola, Reference Adewuya and Makanjuola2008), the specific belief–attitude structures of religious leaders remain significantly underexplored and, critically, have not been analysed using person-centred methods capable of generating population-level typologies (James et al., Reference James, Igbinomwanhia and Omoaregba2014; Oshodi et al., Reference Oshodi, Ogbolu, Nubi, Onajole, Thornicroft and Adeyemi2017; Green and Colucci, Reference Green and Colucci2020; Iheanacho et al., Reference Iheanacho, Nduanya, Slinkard, Ogidi, Patel, Itanyi, Naeem, Spiegelman and Ezeanolue2021).
This study therefore addresses five primary aims: (1) to characterise causal attribution patterns across biological, psychosocial and spiritual domains; (2) to assess attitudinal dimensions across the four CAMI subscales; (3) to examine belief and attitude differences between Christian and Muslim leaders; (4) to derive empirical belief–attitude typologies using LCA; and (5) to identify modifiable predictors of supportive attitudinal orientation. We hypothesise that spiritual causation will be most strongly endorsed; that benevolent attitudes will be tempered by restrictive tendencies; that distinct typologies will emerge; and that spiritual attributions will predict more restrictive attitudes, while biological attributions predict more supportive ones.
Methods
Study design and setting
This cross-sectional survey forms the attitudinal and typological component of the CLERIC (CLErgy and Religious leader Involvement in Community mental health) research programme. The present study constitutes an independent cross-sectional sample focused on belief structure and attitudinal outcomes. Lagos State was selected for its religious diversity, scale and status as a representative context for the intersection of biomedical and faith-based care across urban and peri-urban West Africa. Data collection occurred between March and August 2021.
This study is reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines (von Elm et al., Reference von Elm, Altman, Egger, Pocock, Gøtzsche and Vandenbroucke2007) for cross-sectional studies. Ethical approval was obtained from the Lagos State University Teaching Hospital Health Research Ethics Committee (Approval No: LREC/06/10/1433). All procedures adhered to the Declaration of Helsinki and Nigerian National Health Research Ethics Committee guidelines. Written informed consent was obtained from all participants.
Patient and public involvement
Prior to data collection, a separate community advisory group comprising five religious leaders and three mental health professionals, none of whom subsequently participated in the main study, reviewed draft survey instruments through two structured feedback sessions over a 4-week period, informing revisions to item wording, cultural appropriateness and face validity. This group was not involved in study design, data analysis or manuscript preparation. Service user perspectives were not formally incorporated; this is acknowledged as a limitation, and future co-design work should integrate the perspectives of people with lived experience of mental health conditions in Nigerian faith community settings.
Sex and gender reporting
Consistent with the SAGER guidelines (Heidari et al., Reference Heidari, Babor, De Castro, Tort and Curno2016), sex is reported here as a biological variable. Gender identity data were not systematically collected. The sample was 75.4% male (n = 156), reflecting the structural reality of formal religious authority in urban Lagos, where ordained pastoral and clerical leadership positions are overwhelmingly held by men. Female leaders were not formally excluded but were rarely identifiable through the eligibility criteria applied. The implications of this gender composition for typology generalisability are addressed in the Limitations section.
Participants and sampling
The target population comprised Christian and Muslim religious leaders in Lagos State.
Sample size was calculated to detect medium effect sizes (d = 0.5) in belief–attitude relationships with 80% power at α = .05, powered for primary correlation and between-group tests, yielding a target of 210. The final sample was 207 religious leaders: 133 Christian (64.3%) and 74 Muslim (35.7%). Practitioners of traditional African religions and indigenous healing systems were not included in the sampling frame. This was because the present study was designed to examine formal Christian and Muslim religious leadership structures in Lagos, where churches and mosques provide identifiable congregational sampling frames and constitute the dominant institutional religious pathways through which many people seek informal mental health support.
A stratified multi-stage sampling approach was used. Lagos State’s 20 Local Government Areas were stratified into urban (n = 12) and peri-urban (n = 8), from which 10 urban and 6 peri-urban LGAs were randomly selected. Separate sampling frames were constructed for major Christian denominations (Pentecostal, Anglican, Catholic) and Muslim sects (Sunni, Ahmadiyya). Inclusion criteria required participants to have held a formal religious leadership position for at least 2 years and to serve a congregation of 50 or more members. For this study, “formal religious leadership position” referred to an officially recognised role within a church or mosque that involved regular pastoral, clerical, teaching, counselling or congregational oversight responsibilities, such as pastor, priest, imam, assistant pastor, catechist, mosque teacher or comparable appointed leadership role. Individuals holding formal professional qualifications in psychiatry, psychology, social work or psychiatric/mental health nursing were excluded because the study sought to characterise the beliefs and attitudes of religious leaders who were not also trained mental health professionals.
Regarding sample size adequacy for LCA, the achieved N = 207 satisfies established thresholds for three-class LCA solutions (minimum N ≥ 200) (Bouckenooghe et al., Reference Bouckenooghe, Schwarz, Nguyen and De Clercq2025) and yields an entropy of 0.82, providing empirical support for reliable class recovery. The smallest class contained 54 participants, above the commonly recommended minimum of 50 per class (Nylund et al., Reference Nylund, Asparouhov and Muthén2007).
Instruments
-
• The Causal Beliefs Scale was an 8-item instrument adapted from the Mental Disorder Causal Beliefs Scale (Mannarini and Boffo, Reference Mannarini and Boffo2013). It assessed three domains on a five-point scale ranging from 1 = Not Important to 5 = Extremely Important: biological causation, comprising two items with a possible range of 2–10 and assessing genetic and neurochemical factors; psychosocial causation, comprising three items with a possible range of 3–15 and assessing life stress, social adversity and substance use; and spiritual causation, comprising three items with a possible range of 3–15 and assessing supernatural influences, weak faith and ancestral factors. Full item wording is provided in Supplementary File 1.
-
• The CAMI-16 was an adapted 16-item short form of the Community Attitudes toward Mental Illness scale (Taylor and Dear, Reference Taylor and Dear1981; Evans-Lacko et al., Reference Evans-Lacko, Malcolm, West, Rose, London, Rüsch, Little, Henderson and Thornicroft2013). It measured four subscales on a five-point Likert scale ranging from 1 = Strongly Disagree to 5 = Strongly Agree: Authoritarianism, Benevolence, Social Restrictiveness and Community Mental Health Ideology, with four items per subscale and possible scores ranging from 4 to 20. Authoritarianism and Social Restrictiveness were reverse-scored so that higher scores consistently indicated more positive attitudes, namely less authoritarian and less socially restrictive orientations. Full item wording is provided in Supplementary File 1.
-
• Cultural Adaptation: Both instruments underwent forward–backward translation into Yoruba and Nigerian Pidgin English, followed by expert panel review comprising five religious leaders, three mental health professionals and two medical anthropologists, who examined items for cultural appropriateness and conceptual equivalence. Local idioms, including were (madness), were incorporated where appropriate. Adapted instruments were pilot tested with 20 religious leaders, and final adjustments were made based on feedback. Full documentation is provided in Supplementary File 2.
Statistical analysis
All analyses were conducted using SPSS version 29.0 and Mplus 8.7, with significance set at p < .05 (two-tailed). Effect sizes were reported throughout. The analytical strategy proceeded in five stages: (1) descriptive analysis and psychometric assessment via Cronbach’s alpha and confirmatory factor analysis (CFA); (2) MANOVA and independent t-tests for denominational comparisons; (3) Pearson correlations and path analysis for belief–attitude relationships; (4) multiple linear regression, with psychosocial beliefs entered in all models regardless of significance; and (5) Latent Class Analysis (LCA) evaluating two- to four-class solutions, with model selection based on Akaike Information Criterion (AIC), Bayesian Information Criterion (BIC), entropy, bootstrapped likelihood ratio test (BLRT) and theoretical interpretability. Indirect effects were estimated using bootstrapped 95% confidence intervals (5,000 resamples).
Results
This section presents findings across five analytical stages: psychometric validation, descriptive belief and attitude patterns, denominational comparisons, latent typologies and belief–attitude relationships. Psychometric and detailed item-level data are provided in Supplementary File 1.
Participant characteristics and psychometric validation
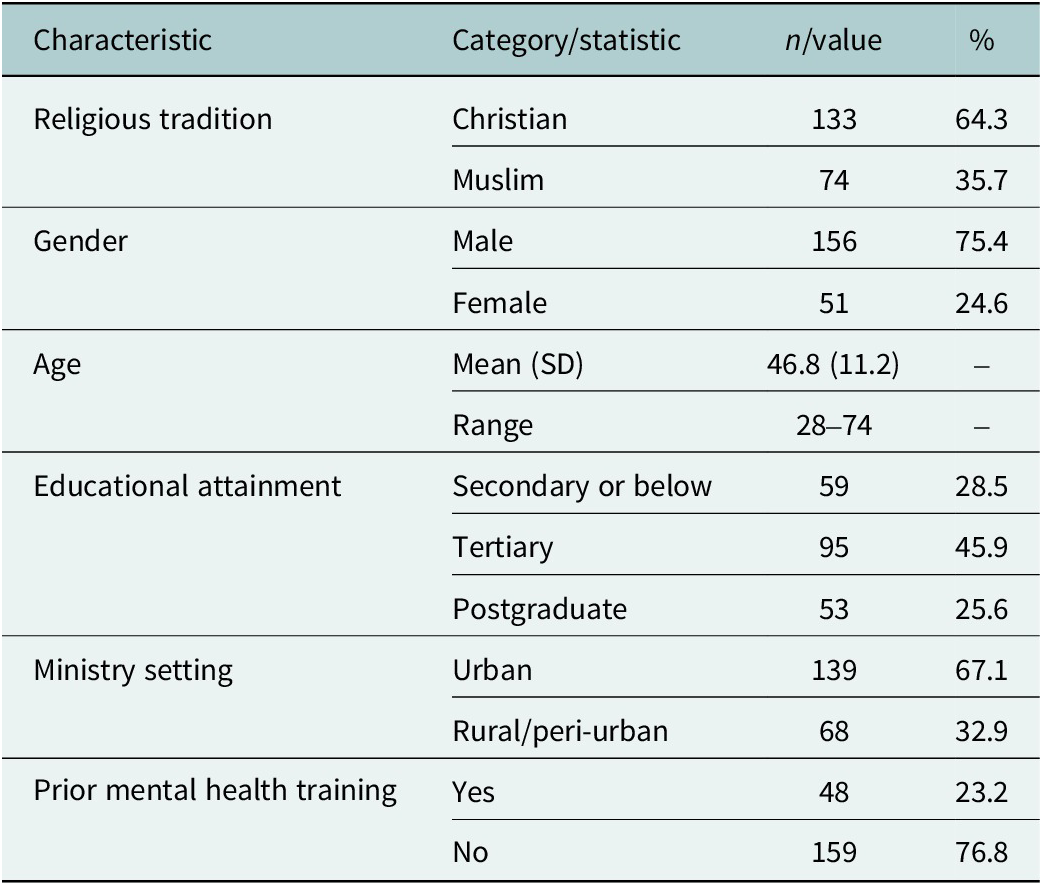
The sample (N = 207) comprised religious leaders from Christian (64.3%, n = 133) and Muslim (35.7%, n = 74) traditions. Participants were 75.4% male (n = 156) and 24.6% female (n = 51), with a mean age of 46.8 years (SD = 11.2, range 28–74). Just under half held tertiary education (45.9%), 25.6% held postgraduate qualifications and 23.2% reported prior mental health training (Table 1). The larger male composition reflects the gendered structure of formal religious authority in urban Lagos; its implications for generalisability are discussed under Limitations.
Socio-demographic characteristics of participants (N = 207)

Table 1. Long description
The table consists of four columns: Characteristic, Category/statistic, n/value, and percentage.
* Religious tradition: Christian at 133 (64.3 percent) and Muslim at 74 (35.7 percent).
* Gender: Male at 156 (75.4 percent) and Female at 51 (24.6 percent).
* Age: Mean (S D) is 46.8 (11.2) with a range of 28 to 74.
* Educational attainment: Secondary or below at 59 (28.5 percent), Tertiary at 95 (45.9 percent), and Postgraduate at 53 (25.6 percent).
* Ministry setting: Urban at 139 (67.1 percent) and Rural/peri-urban at 68 (32.9 percent).
* Prior mental health training: Yes at 48 (23.2 percent) and No at 159 (76.8 percent).
Both adapted scales demonstrated good-to-excellent psychometric properties. For the Causal Beliefs Scale, internal consistency was high across domains: spiritual causation (α = .82), psychosocial causation (α = .79) and biological causation (α = .85). For the CAMI-16, reliabilities were similarly strong: benevolence (α = .83), Community Mental Health Ideology (α = .79), Authoritarianism (α = .77) and Social Restrictiveness (α = .81). CFA supported both instrument structures: Causal Beliefs Scale (CFI = 0.95, RMSEA = 0.044 [90% CI: 0.02–0.07]); CAMI-16 (CFI = 0.98, RMSEA = 0.03 [90% CI: 0.00–0.06]). Full item-level data are in Supplementary File 1.
Causal belief and attitudinal patterns
Spiritual causation was the most strongly endorsed domain (M = 11.9, SD = 2.3; 79.3% of maximum possible score), followed by psychosocial (M = 10.6, SD = 2.7; 70.7%) and biological (M = 5.8, SD = 2.1; 58.0%). Mean endorsement across all three domains was well above scale midpoints, indicating layered, pluralistic causal frameworks in which multiple explanatory systems operate simultaneously rather than as mutually exclusive alternatives. This pattern has direct implications for integration feasibility, as it suggests that biomedical intervention is not categorically rejected by most leaders even where spiritual attribution dominates.
Attitudinal responses revealed a moderately supportive overall stance (total CAMI M = 53.3, SD = 9.4). Benevolence (M = 15.2, SD = 2.8) and Community Mental Health Ideology (M = 14.7, SD = 3.1) were the most strongly endorsed dimensions. After reverse-scoring, Authoritarianism (M = 12.1, SD = 3.2) and Social Restrictiveness (M = 11.3, SD = 3.5) yielded the lowest scores, indicating that restrictive and authoritarian orientations coexisted with benevolent ones to a meaningful degree.
MANOVA confirmed a significant overall multivariate difference between Christian and Muslim leaders (Wilks’ λ = .89, F (7, 199) = 3.41, p < .001, partial η 2 = .11). Muslim leaders endorsed spiritual causation more strongly (M = 12.4 vs. M = 11.6; t (205) = 2.31, p = .022, d = 0.35), whereas Christian leaders endorsed biological causation more strongly (M = 6.3 vs. M = 5.1; t (205) = 3.85, p < .001, d = 0.59). These denominational differences should be interpreted with caution: religious tradition in this sample was strongly associated with educational attainment, and education was itself a significant predictor of biological belief endorsement. Observed differences therefore likely reflect institutional and educational variation rather than doctrinal divergence per se (Table 2).
Denominational differences in causal beliefs and attitudes (N = 207)

Table 2. Long description
The table contains six columns: Measure, Christian M (S D), Muslim M (S D), t, p, and Cohen’s d.
Under the category Causal beliefs:
- Spiritual causation: Christian 11.6 (2.4), Muslim 12.4 (2.1), t equals minus 2.31, p equals .022, Cohen’s d equals 0.35.
- Psychosocial causation: Christian 10.8 (2.6), Muslim 10.3 (2.8), t equals 1.26, p equals .209, Cohen’s d equals 0.18.
- Biological causation: Christian 6.3 (2.2), Muslim 5.1 (1.8), t equals 3.85, p is less than .001, Cohen’s d equals 0.59.
Under the category C A M I 16 Subscales:
- Benevolence: Christian 15.7 (2.6), Muslim 14.5 (3.0), t equals 2.89, p equals .004, Cohen’s d equals 0.43.
- Community Mental Health Ideology: Christian 15.1 (2.9), Muslim 14.1 (3.4), t equals 2.15, p equals .033, Cohen’s d equals 0.32.
- Authoritarianism: Christian 12.3 (3.1), Muslim 11.8 (3.4), t equals 0.98, p equals .330, Cohen’s d equals 0.15.
- Social Restrictiveness: Christian 12.0 (3.3), Muslim 10.3 (3.7), t equals 3.22, p equals .001, Cohen’s d equals 0.51.
Note: Authoritarianism and Social Restrictiveness are reverse-scored subscales where higher scores indicate less authoritarian or restrictive attitudes.
Note: Effect size interpretations: small (0.2), medium (0.5) and large (0.8).
† Reverse-scored subscales; higher scores indicate less authoritarian/restrictive attitudes. Denominational differences in biological causation and social restrictiveness should be interpreted cautiously given the significant association between religious tradition and educational attainment in this sample.
* p <0.05 ** P<0.01 *** P<0.001
Latent class analysis: Implementation typologies
LCA was conducted on six continuous indicators: the three causal belief domain scores and the four CAMI-16 subscale scores, using Mplus 8.7 with TYPE = MIXTURE parameterisation. Models with one to four classes were estimated. The one-class solution confirmed substantial population heterogeneity (AIC = 3,056.2, BIC = 3,098.7). The two-class solution improved fit (AIC = 2,911.8, BIC = 2,974.1, Entropy = 0.74) but was theoretically under-differentiated. The three-class solution was selected on the basis of the lowest BIC among solutions with a significant BLRT, entropy of 0.82 (exceeding the ≥0.80 threshold) and clear theoretical interpretability (AIC = 2,847.3, BIC = 2,912.8). The four-class solution offered only marginal AIC improvement and a non-significant BLRT (p = .09), while BIC increased (2,925.5) and entropy decreased (0.76). Full model comparison statistics are provided in Supplementary File 3.
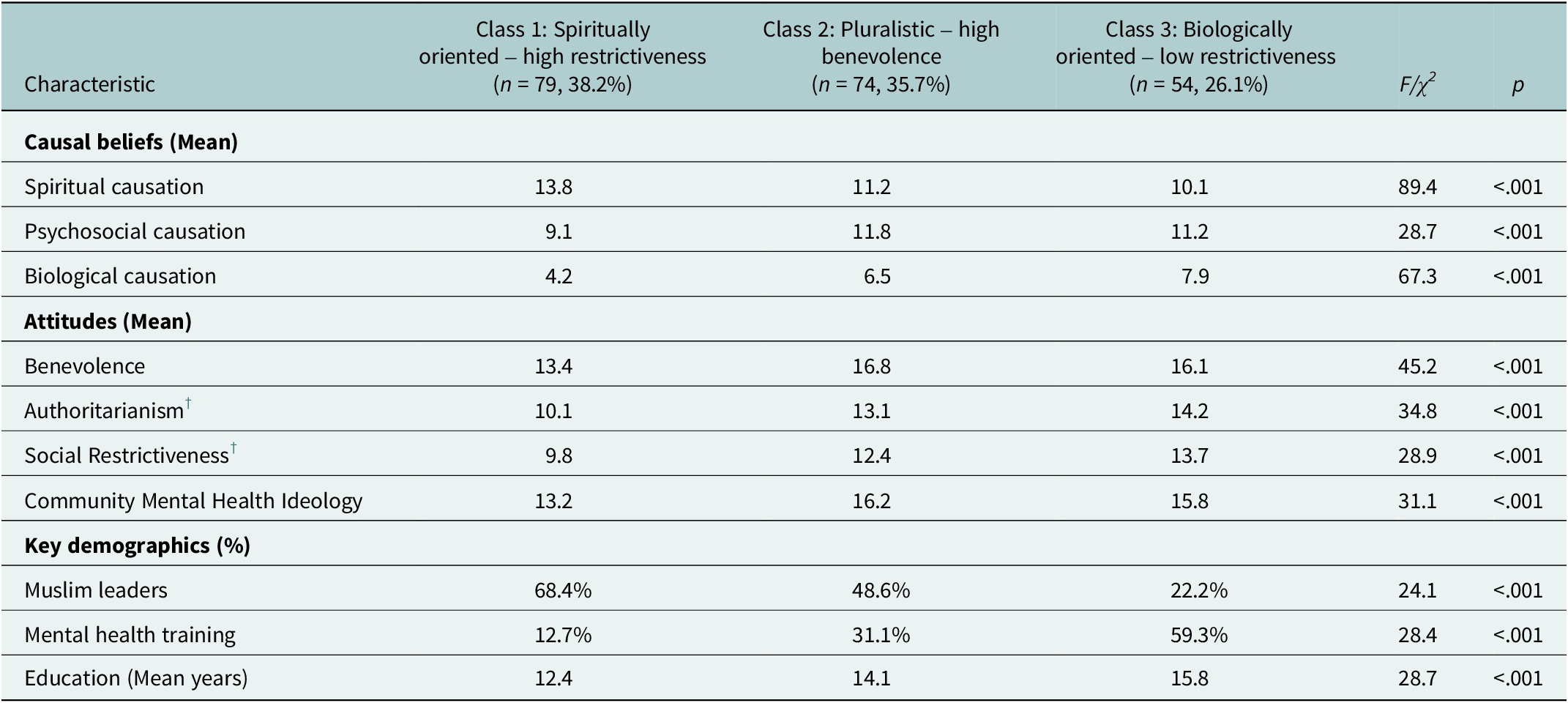
Three implementation-relevant typologies emerged (Table 3). Labels are analytically rather than normatively derived and reflect predominant empirical characteristics within each class:
-
• Class 1: Spiritually Oriented–High Restrictiveness (38.2%, n = 79). This largest class was defined by very high spiritual causation (M = 13.8), low biological endorsement (M = 4.2) and the most restrictive attitudinal profile: lowest benevolence and community support scores alongside elevated Authoritarianism and Social Restrictiveness. This class was predominantly Muslim (68.4%) and less formally educated. The fact that this profile comprises over one-third of the target population has direct programme planning implications, as universal training models would engage this group on terms fundamentally mismatched to their cognitive frameworks.
-
• Class 2: Pluralistic–High Benevolence (35.7%, n = 74). This class showed moderate endorsement across all three causal domains (spiritual M = 11.2, psychosocial M = 11.8, biological M = 6.5), reflecting genuine cognitive pluralism. Attitudinally, these leaders exhibited the highest benevolence (M = 16.8) and strong community ideology. Evenly distributed across religious traditions and more highly educated, this class represents the most immediately implementation-ready segment, requiring practical capacity-building rather than fundamental belief change.
-
• Class 3: Biologically Oriented–Low Restrictiveness (26.1%, n = 54). The smallest class displayed the highest biological causation scores (M = 7.9), high benevolence and the lowest Authoritarianism and Restrictiveness. Christian leaders predominated (77.8%), as did those with advanced education and prior mental health training. These leaders are natural candidates for early adopter and peer champion roles in scaled integration programmes.
Latent class analysis – Typology characteristics (N = 207)

Table 3. Long description
The table compares three classes across several characteristics with F or chi-squared statistics and p-values, all of which are less than .001.
Class 1: Spiritually oriented - high restrictiveness (n = 79, 38.2%).
Class 2: Pluralistic - high benevolence (n = 74, 35.7%).
Class 3: Biologically oriented - low restrictiveness (n = 54, 26.1%).
Causal beliefs (Mean scores):
- Spiritual causation: Class 1 (13.8), Class 2 (11.2), Class 3 (10.1).
- Psychosocial causation: Class 1 (9.1), Class 2 (11.8), Class 3 (11.2).
- Biological causation: Class 1 (4.2), Class 2 (6.5), Class 3 (7.9).
Attitudes (Mean scores):
- Benevolence: Class 1 (13.4), Class 2 (16.8), Class 3 (16.1).
- Authoritarianism (reverse-scored): Class 1 (10.1), Class 2 (13.1), Class 3 (14.2).
- Social Restrictiveness (reverse-scored): Class 1 (9.8), Class 2 (12.4), Class 3 (13.7).
- Community Mental Health Ideology: Class 1 (13.2), Class 2 (16.2), Class 3 (15.8).
Key demographics:
- Muslim leaders: Class 1 (68.4%), Class 2 (48.6%), Class 3 (22.2%).
- Mental health training: Class 1 (12.7%), Class 2 (31.1%), Class 3 (59.3%).
- Education (Mean years): Class 1 (12.4), Class 2 (14.1), Class 3 (15.8).
Note: F-statistics from one-way ANOVA for continuous variables; χ2 for categorical variables. LCA model fit: AIC = 2,847.3; BIC = 2,912.8; Entropy = 0.82. Typology labels are analytically derived and reflect predominant empirical characteristics within each class rather than normative valuations.
† Reverse-scored subscales; higher scores indicate less authoritarian/restrictive attitudes.
Class membership showed significant associations with education (χ2(4) = 28.7, p < .001), prior training (χ2(2) = 28.4, p < .001) and religious tradition (χ2(2) = 24.1, p < .001).
Predictors of attitudinal orientation
Correlational analysis confirmed that spiritual causation was positively associated with Authoritarianism (r = .34, p < .001) and Social Restrictiveness (r = .41, p < .001), indicating that stronger supernatural attribution consistently co-occurs with more restrictive orientations and suggesting that stigma among religious leaders is cognitively structured by causal frameworks rather than primarily dispositional. Biological causation was positively associated with benevolence (r = .28, p < .001) and community ideology (r = .35, p < .001), consistent with a model in which explanatory frameworks serve as upstream determinants of attitudinal orientation.
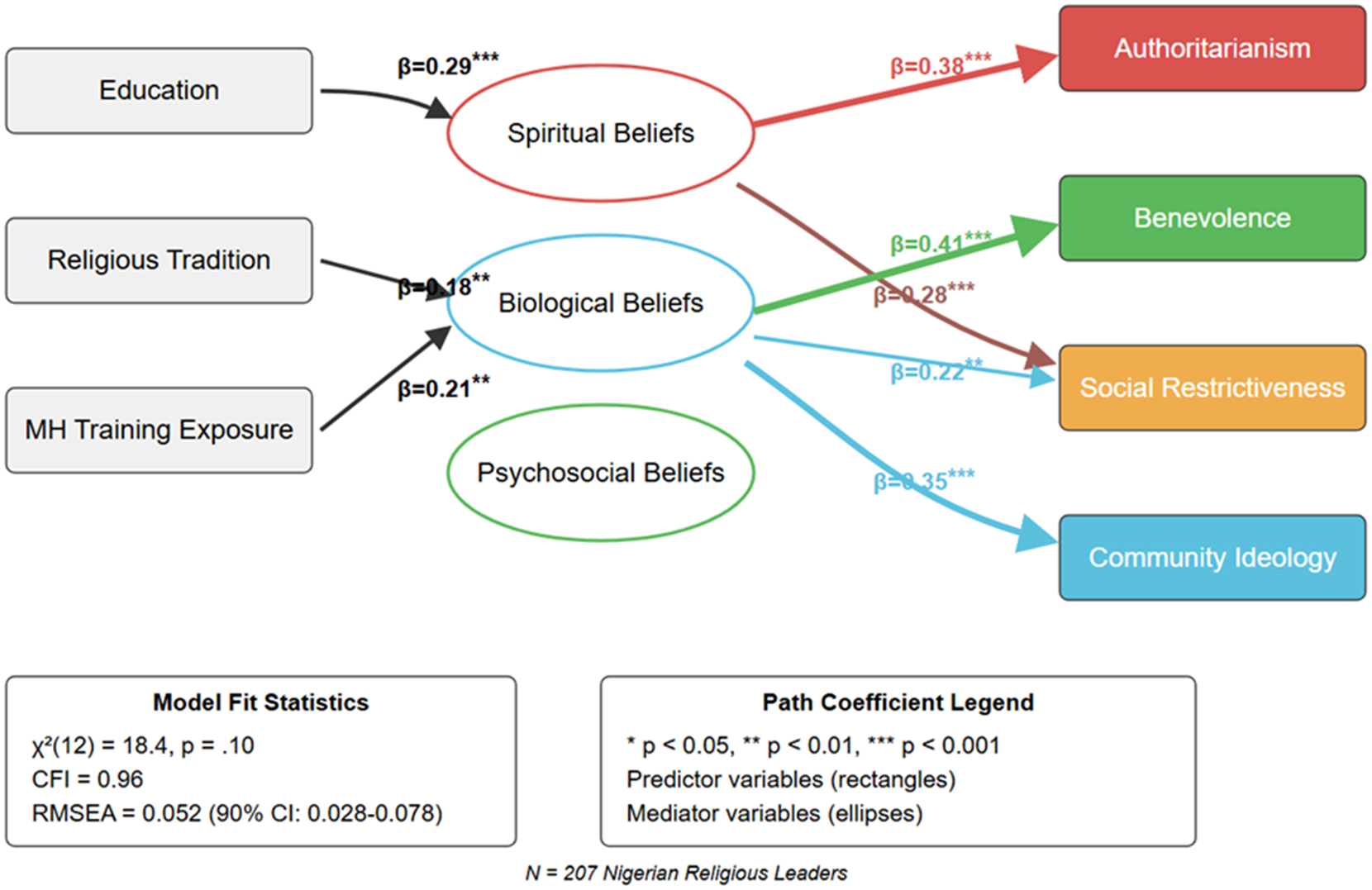
Path analysis indicated adequate model fit (CFI = 0.96; RMSEA = 0.052 [90% CI: 0.03–0.08]) (Figure 1). Stronger spiritual beliefs were associated with more restrictive attitudes (β = 0.38, p < .001), representing a practically meaningful elevation in authoritarian and socially restrictive orientation per standard deviation increase in spiritual belief endorsement, while stronger biological beliefs were associated with more supportive attitudes (β = 0.31, p < .001). These are path model coefficients; regression analyses below estimate multiple predictors simultaneously.
Path analysis of the relationships between demographics, causal beliefs and attitudes.
Note: Path analysis of relationships between demographics, causal beliefs and attitudes. The model demonstrates adequate fit (CFI = 0.96; RMSEA = 0.052 [90% CI: 0.03–0.08]). Spiritual beliefs predicted more authoritarian and restrictive attitudes (β = 0.38, p < .001). Biological beliefs predicted more benevolent and community-supportive attitudes (β = 0.31, p < .001). Standardised path coefficients shown on all arrows; non-significant paths omitted.

Figure 1. Long description
The diagram is organized into three vertical columns of nodes connected by arrows with beta coefficients.
Left Column (Predictor Variables in gray rectangles):
- Education has a path to Spiritual Beliefs (beta equals 0.29, p less than 0.001).
- Religious Tradition has a path to Biological Beliefs (beta equals 0.18, p less than 0.01).
- M H Training Exposure has a path to Biological Beliefs (beta equals 0.21, p less than 0.01).
Middle Column (Mediator Variables in ellipses):
- Spiritual Beliefs (red outline) has paths to Authoritarianism (beta equals 0.38, p less than 0.001) and Social Restrictiveness (beta equals 0.28, p less than 0.001).
- Biological Beliefs (blue outline) has paths to Benevolence (beta equals 0.41, p less than 0.001), Social Restrictiveness (beta equals 0.22, p less than 0.01), and Community Ideology (beta equals 0.35, p less than 0.001).
- Psychosocial Beliefs (green outline) has no significant paths shown.
Right Column (Outcome Variables in colored rectangles):
- Authoritarianism (red)
- Benevolence (green)
- Social Restrictiveness (orange)
- Community Ideology (light blue)
Bottom Section:
- Model Fit Statistics box on the left: chi-squared (12) equals 18.4, p equals 0.10; C F I equals 0.96; R M S E A equals 0.052 (90% C I: 0.028-0.078).
- Path Coefficient Legend box on the right: defines p-value significance levels and identifies rectangles as predictors and ellipses as mediators.
- Footer text: N equals 207 Nigerian Religious Leaders.
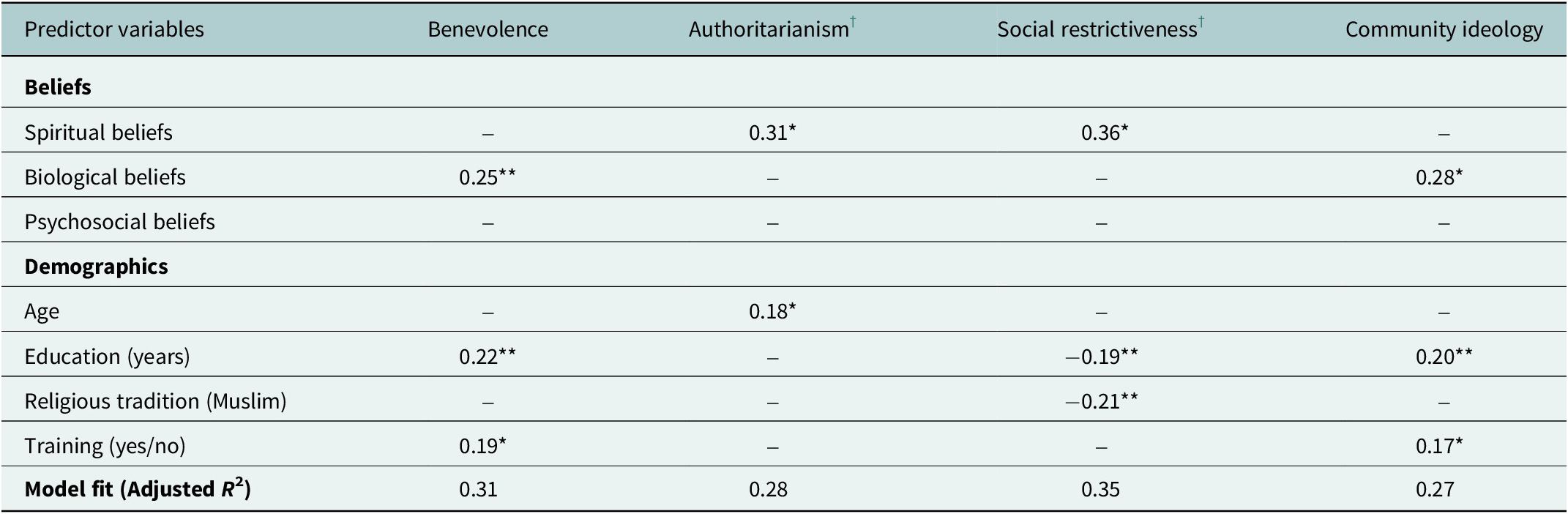
Multiple regression models (Table 4) identified independent predictors for each attitudinal dimension. Benevolence was best predicted by biological belief endorsement (β = 0.25, p < .01), higher education (β = 0.22, p < .01) and prior training (β = 0.19, p < .05; Adjusted R 2 = 0.31). Authoritarianism was predicted by stronger spiritual beliefs (β = 0.31, p < .05) and older age (β = 0.18, p < .05; Adjusted R 2 = 0.28). Social Restrictiveness was associated with spiritual beliefs (β = 0.36, p < .05), Muslim tradition (β = −0.21, p < .01) and lower education (β = −0.19, p < .01; Adjusted R 2 = 0.35). Community Mental Health Ideology was predicted by biological beliefs (β = 0.28, p < .05), higher education (β = 0.20, p < .01) and prior training (β = 0.17, p < .05; Adjusted R 2 = 0.27). Psychosocial beliefs were entered in all four models and were non-significant throughout (all p > .10).
Multiple regression models predicting attitude dimensions (N = 207)

Table 4. Long description
A table presenting multiple regression models for N = 207. The columns represent four attitude dimensions: Benevolence, Authoritarianism, Social restrictiveness, and Community ideology. The rows are categorized into Beliefs and Demographics.
Under Beliefs:
* Spiritual beliefs significantly predict Authoritarianism (0.31*) and Social restrictiveness (0.36*).
* Biological beliefs significantly predict Benevolence (0.25**) and Community ideology (0.28*).
* Psychosocial beliefs were non-significant across all models.
Under Demographics:
* Age significantly predicts Authoritarianism (0.18*).
* Education (years) significantly predicts Benevolence (0.22**), Social restrictiveness (-0.19**), and Community ideology (0.20**).
* Religious tradition (Muslim) significantly predicts Social restrictiveness (-0.21**).
* Training (yes/no) significantly predicts Benevolence (0.19*) and Community ideology (0.17*).
Model fit (Adjusted R super 2) values are 0.31 for Benevolence, 0.28 for Authoritarianism, 0.35 for Social restrictiveness, and 0.27 for Community ideology. All R super 2 values are significant at p < .001. Significance levels are indicated by * for p < .05 and ** for p < .01.
Note: β = standardised beta coefficient. A dash (–) indicates the variable was not a significant predictor. Psychosocial beliefs were entered in all four models and were non-significant throughout (all p > .10). All R 2 values were significant at p < .001.
† For reverse-scored scales, a positive β for Spiritual Beliefs indicates prediction of more negative (authoritarian/restrictive) attitudes; a negative β for Education or Tradition (Muslim) indicates prediction of more positive (less restrictive) attitudes.
*p<0.05; **p<0.01; ***P<0.001
Discussion
Summary of findings and their implementation significance
This study demonstrates that religious leaders, the de facto primary mental health contact for millions of Nigerians, are not a homogeneous target population but cluster into three empirically distinct typologies, each present in over a quarter of the sample, with coherent and meaningfully different belief–attitude profiles. This has a direct programme planning implication: uniform clergy training models, the dominant approach in the faith–health integration literature (James et al., Reference James, Igbinomwanhia and Omoaregba2014; Green and Colucci, Reference Green and Colucci2020), are poorly matched to the structural heterogeneity of their target population. Over a third of leaders (38.2%) hold profiles characterised by strong spiritual causation and restrictive attitudes: a profile for which literacy-focused training is neither the primary need nor likely the most effective first lever. A further 35.7% are already pluralistically oriented and attitudinally supportive, requiring practical capacity rather than belief change. Only by knowing the distribution of these profiles can programme designers allocate resources appropriately across a population.
Contextualisation within the global evidence base
These patterns are not unique to Nigeria. Research in Ghana (Osafo, Reference Osafo2016; Kpobi and Swartz, Reference Kpobi and Swartz2018), Uganda (Teuton et al., Reference Teuton, Bentall and Dowrick2007; Asiimwe et al., Reference Asiimwe, Nuwagaba-Kayongo, Dwanyen and Kasujja2023), Lebanon (Aramouny et al., Reference Aramouny, Kerbage, Richa, Rouhana and Richa2020) and among South Asian populations (Nguyen et al., Reference Nguyen, Yamada and Dinh2012) documents the co-occurrence of benevolent intent and social restriction among religious leaders, alongside pluralistic causal frameworks that accommodate biomedical intervention under specific conditions. The analytic advance provided by this study is the quantitative estimation of profile proportions at population scale: something that prior qualitative and cross-sectional studies without person-centred analytical approaches could not achieve. The three-class structure observed here is likely to have counterparts in comparable pluralistic health systems across sub-Saharan Africa and South Asia, where the interaction between strong spiritual attributional cultures, under-resourced formal health systems and high religious institutional density creates similar structural pressures on informal mental health provision.
The cognitive layering finding that all three causal domains were endorsed above scale midpoints directly challenges a common assumption underpinning many faith–health integration efforts: that spiritual belief and biomedical engagement are structurally incompatible. The Pluralistic–High Benevolence class, constituting 35.7% of this sample, is empirical evidence that integrated framing is already operative among a substantial minority of leaders. This aligns with Kpobi and Swartz’s Ghanaian findings and Osafo’s work on the structural conditions for collaboration (Osafo, Reference Osafo2016; Kpobi and Swartz, Reference Kpobi and Swartz2018) and supports the broader global mental health implementation science argument that community actors’ existing frameworks should be engaged rather than displaced (Nilsen, Reference Nilsen2015).
Within Nigeria, Oshodi et al. (Reference Oshodi, Ogbolu, Nubi, Onajole, Thornicroft and Adeyemi2017) and Iheanacho et al. (Reference Iheanacho, Nduanya, Slinkard, Ogidi, Patel, Itanyi, Naeem, Spiegelman and Ezeanolue2021) documented mixed patterns among clergy but did not generate population-level typologies. The finding that the Spiritually Oriented–High Restrictiveness class constitutes 38.2% of the sample is actionable in a way that prior descriptive accounts were not: it enables programme planners to estimate the proportion of a given faith community likely to require intensive trust-building and harm-reduction approaches rather than capacity-building alone, and to staff and budget accordingly.
The advance over prior typological work specifically deserves emphasis. While Ojelade et al. (Reference Ojelade, Oyerinde and Olaoye2023) and Esan et al. (Reference Esan, Appiah-Poku, Othieno, Kola, Harris, Nortje, Makanjuola, Oladeji, Price, Seedat and Gureje2019) provide valuable contextual evidence on religious leaders’ knowledge and practice, these studies relied on categorical self-classification rather than data-driven typology generation and were accordingly susceptible to social desirability distortion in a way that LCA, operating on continuous scale scores, is less so. The present typologies were induced from the data rather than imposed upon it, and their internal consistency, evidenced by the coherent alignment between causal domain scores and attitudinal profiles within each class, suggests they capture genuine cognitive structures rather than response artefacts.
Theoretical contributions
These findings extend Kleinman’s explanatory model framework (Kleinman et al., Reference Kleinman, Eisenberg and Good1978) by providing quantitative evidence for a “layered” or pluralistic mode of causal attribution in which spiritual, psychosocial and biological models are held concurrently rather than competitively. This challenges both simple replacement models (in which biomedical knowledge displaces spiritual belief) and models that assume supernatural attribution forecloses biomedical engagement. The Pluralistic–High Benevolence class exemplifies a coherent cognitive architecture in which different frameworks are mobilised for different functions: spiritual frameworks for meaning-making, psychosocial frameworks for social causation and biological frameworks for treatment rationale. This layered structure is arguably a prerequisite for designing interventions that are culturally resonant rather than culturally displaced, an insight increasingly central to decolonised approaches to global mental health implementation (Kirmayer, Reference Kirmayer2012; Antic, Reference Antic2024).
The findings also illuminate stigma formation within Link and Phelan (Reference Link and Phelan2001)’s framework. The consistent association between spiritual causal endorsement and authoritarian/restrictive attitudes suggests that stigma among religious leaders is cognitively structured by explanatory models rather than primarily emotional or dispositional in origin (Elliot and Ragsdale, Reference Elliott and Ragsdale2024). This has a specific intervention implication: attitude-change efforts that bypass causal beliefs and target stigma dimensions directly may be less efficient than those addressing the upstream causal framework. The regression models reinforce this interpretation: biological belief endorsement retains independent predictive power for benevolence even after controlling for education and training, indicating that the attitudinal benefit of biomedical literacy is not fully reducible to general educational attainment.
Two competing interpretations deserve acknowledgement. First, restrictive attitudes may partly reflect legitimate pastoral protective concern rather than stigmatising intent. Second, spiritual causation may function primarily as meaning-making rather than as a mechanism of social exclusion. These possibilities do not invalidate the observed associations but argue for engagement strategies that work within existing meaning-making frameworks rather than against them.
Implications for health systems integration
The three typologies provide an empirical foundation for a stratified implementation model consistent with WHO mhGAP task-sharing guidance (World Health Organization, 2008; Eaton et al., Reference Eaton, McCay, Semrau, Chatterjee, Baingana, Araya, Ntulo, Thornicroft and Saxena2011) and directly actionable through Nigeria’s Mental Health Act 2021 (Ogunwale, Reference Ogunwale2023), which provides legislative grounding for formal faith–health partnerships.
-
• For the Spiritually Oriented–High Restrictiveness group (38.2%), harm reduction and compassionate care framing are indicated rather than direct challenge to spiritual belief. Training co-designed with leaders from the biologically oriented class, deploying their credibility as internal rather than external change agents, may be more acceptable than clinician-delivered instruction. Messages framing depression and psychosis as conditions treatable through both medical care and pastoral support may gain more traction than those positioning biomedical explanation as incompatible with spiritual meaning-making. Structural exposure through supervised referral practice may be a more efficient pathway to behaviour change than attitude change alone.
-
• For the Pluralistic–High Benevolence group (35.7%), the principal need is practical capacity rather than belief or attitude change. Structured training in symptom recognition, suicide risk identification and referral navigation, combined with facility familiarisation visits and simple one-page referral guides, would address the structural know-how gap while building on existing attitudinal assets. These leaders are natural candidates for cultural broker roles in stepped-care implementation models.
-
• For the Biologically Oriented–Low Restrictiveness group (26.1%), engagement should focus on developing community champion and peer-educator capacity. Their credibility on biomedical framing positions them well for co-facilitating stigma-reduction campaigns and training other religious leaders. This group represents the appropriate early-adopter cohort for pilot integration programmes under Nigeria’s Mental Health Act 2021.
Across all three typologies, structural barriers (geographic inaccessibility, financial toxicity of formal services and fragmented referral infrastructure) operate as cross-cutting constraints. Evidence from the CLERIC programme’s companion qualitative study confirms that nearly half of willing leaders had never made a medical referral in the preceding year. Attitudinal change is necessary but structurally insufficient; enabling infrastructure must be built simultaneously.
Limitations
The cross-sectional design precludes causal inference; bidirectionality is plausible, as attitudinal orientations may also shape the salience of causal frameworks over time, particularly through training exposure. The sample’s largely male composition (75.4%) reflects the gendered structure of formal religious authority in urban Lagos and limits the generalisability of these typologies to female religious leaders, who may hold different profiles. Findings are restricted to Lagos State and may not generalise to rural Nigeria or to other LMIC contexts with different denominational compositions and healthcare access profiles. Measurement invariance across Christian and Muslim subgroups was not formally tested. Self-report measures carry a risk of social desirability bias. Traditional healers and practitioners of indigenous religions were not included, although they remain an important component of informal mental health provision in Nigeria and across several sub-Saharan African contexts. Their exclusion limits the generalisability of the typologies to Christian and Muslim institutional religious leaders and means that the findings should not be interpreted as representing the full ecology of faith-based and indigenous mental health care. Future work should examine whether comparable belief-attitude typologies are present among traditional African religion practitioners and indigenous healers.
Conclusion
Religious leaders in Nigeria are not a homogeneous population but cluster into three empirically distinct belief–attitude typologies with coherent profiles, meaningful proportional representation and different implications for implementation. The dominant typology (Spiritually Oriented–High Restrictiveness, constituting 38.2% of leaders) calls for harm-reduction and compassionate framing approaches rather than literacy-first models. Education and prior mental health training are the strongest modifiable predictors of supportive orientation, providing tractable leverage points for intervention that operate partially independently of causal belief change. These findings offer a stratified evidence base for faith–health partnership design, grounded in the empirical distribution of leader profiles rather than the assumption of homogeneity. Nigeria’s Mental Health Act 2021 now provides the legislative architecture for operationalising this stratified approach at a national scale. The typological framework proposed here is transferable to comparable pluralistic health systems across sub-Saharan Africa and South Asia (contexts that collectively account for a substantial proportion of the global mental health treatment gap) and is designed to be adapted to local denominational compositions and service infrastructure as these integration efforts scale.
Open peer review
To view the open peer review materials for this article, please visit http://doi.org/10.1017/gmh.2026.10253.
Supplementary material
The supplementary material for this article can be found at http://doi.org/10.1017/gmh.2026.10253.
Data availability statement
The data that support the findings of this study are not publicly available due to concerns about participant confidentiality in a relatively small and identifiable population of religious leaders. De-identified data may be made available from the corresponding author on reasonable request and subject to institutional and ethical approval.
Acknowledgements
The authors thank the religious leaders and congregations in Lagos State who generously contributed their time and perspectives to this study. We are grateful to members of the community advisory group, including the five religious leaders and three mental health professionals who provided critical feedback on the survey instruments and study procedures. We also acknowledge the administrative and technical support provided by the Lagos State University Teaching Hospital and the Lagos State University College of Medicine.
Author contribution
A.O.A. conceived the study, led the overall study design and supervised data collection and analysis. O.E.O. contributed to study design, coordinated fieldwork and led the drafting of the introduction and discussion. K.W. contributed to instrument adaptation, oversaw community engagement activities and supported interpretation of findings. A.R. led the quantitative data analysis and contributed to the methods and results sections. B.A. provided statistical oversight, advised on latent class modelling and contributed to the interpretation of implementation implications. All authors contributed to critical revision of the manuscript for important intellectual content, approved the final version for publication and agree to be accountable for all aspects of the work.
Financial support
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.”
Competing interests
A.O.A., O.E.O., K.O.W., A.R. and B.A. report no conflicts of interest related to this work.
Ethics statement
Ethical approval for this study was obtained from the Lagos State University Teaching Hospital Health Research Ethics Committee (Approval No. LREC/06/10/433). All procedures adhered to the Declaration of Helsinki and Nigerian National Health Research Ethics Committee guidelines, and written informed consent was obtained from all participants.




 Open access
Open access