


Introduction
Completing education, entering the labour market and achieving financial independence are key milestones in the transition to adulthood (Billari & Liefbroer, Reference Billari and Liefbroer2010; Buchmann & Kriesi, Reference Buchmann and Kriesi2011). This transition can be disrupted for adolescents and young adults who are not in education, employment or training (NEET). NEET exposes youth and young adults to psychosocial burdens and economic risks in later adulthood and can impose significant societal costs (Mascherini et al., Reference Mascherini, Salvatore and Meierkord2012; Ralston et al., Reference Ralston, Everington and Feng2022), which have made NEET a major public policy concern and an important indicator of the risk of social exclusion (OECD, 2010).
The risk of NEET is socially stratified and previous research has found that it is more prevalent amongst those from lower socioeconomic backgrounds, those with poor school performance and low educational attainment and those with health problems in adolescence (De Luca et al., Reference De Luca, Mazzocchi and Quintano2020; Gladwell et al., Reference Gladwell, Popli and Tsuchiya2022; Pitkänen et al., Reference Pitkänen, Remes and Moustgaard2021; Tamesberger & Bacher, Reference Tamesberger and Bacher2014). Most previous research focusses on predictors of NEET that are close in time, but does not consider antecedents early in the life course that lay the foundations for development and socioeconomic achievement later in life (Ben-Shlomo & Kuh, Reference Ben-Shlomo and Kuh2002; Heckman, Reference Heckman2006). Adverse health conditions during pregnancy and at birth, such as being born prematurely or with (very) low birth weight, have medical and social consequences, and influence, for instance, cognitive development, mental health and educational attainment, which in turn affect the risk of NEET (Black et al., Reference Black, Devereux and Salvanes2007; Cozzani & Härkönen, Reference Cozzani and Härkönen2023; Eves et al., Reference Eves, Mendonça and Baumann2021; Gladwell et al., Reference Gladwell, Popli and Tsuchiya2022; Moster et al., Reference Moster, Lie and Markestad2008; Mathiasen et al., Reference Mathiasen2009; Rodwell et al., Reference Rodwell, Romaniuk and Nilsen2018). Awareness of (very) early life course antecedents underlines the processes that shape the risk of exclusion from education and the labour market over the ‘long life’ (Mayer, Reference Mayer2009) and also draws attention to policies – such as obstetric, neonatal and infant healthcare – that target the early formative years but may also have long-term life course consequences (Bütikofer et al., Reference Bütikofer, Løken and Salvanes2019; Heckman, Reference Heckman2006).
In this study, we analyse the effects of perinatal health on the incidence of NEET in young adulthood in Finland with two main research questions. First, focussing on the effect of birth weight, we ask whether low (under 2500 g) and very low (under 1500 g) birth weight affect the incidence of NEET in young adulthood at ages 21–27 years. Low birth weight is a leading indicator of early health and adverse birth outcomes and previous research has linked it to compromised neurosensory, cognitive and socioeconomic outcomes (Mathiasen et al., Reference Mathiasen2009; Moster et al., Reference Moster, Lie and Markestad2008; Torche & Conley, Reference Torche and Conley2015; Zhou et al., Reference Zhou2025). Second, we ask whether the effects of (very) low birth weight are moderated by parental socioeconomic background, measured as maternal education. Both NEET (Gladwell et al., Reference Gladwell, Popli and Tsuchiya2022; Pitkänen et al., Reference Pitkänen, Remes and Moustgaard2021; Tamesberger & Bacher, Reference Tamesberger and Bacher2014) and (very) low birth weight (Finch, Reference Finch2003) are more prevalent amongst individuals from low socioeconomic backgrounds and we assess how early health effects interact with the socioeconomic environment and how these interactions shape social inequalities in the labour market integration.
To answer these questions, we use high-quality Finnish birth registers on 348,906 individuals born in 1987–1992, linked to register data on economic activity and educational enrolment in 2008–2019. In addition to providing a rich set of variables with low measurement error and a long follow-up period, our data allow for the linkage of siblings, which we use to estimate sibling fixed effects models to adjust for confounding due to factors shared by siblings born to the same mother, such as family background, neighbourhood characteristics, and genetic similarity. More specifically, we estimate sibling fixed effects Poisson regressions to analyse the effect of (very) low birth weight on the annual incidence of NEET in the early adulthood years.
Birth weight as a prenatal antecedent of neet
The term NEET – referring to young adults who are not in employment, education or training – originated in the UK in the early 2000s and has been widely adopted internationally (Mascherini, Reference Mascherini, O’Reilly, Leschke and Ortlieb2018). NEET summarises the occurrence of simultaneous vulnerabilities in labour market and educational integration and is an indicator of the risk of broader social exclusion, which can negatively affect an individual’s wellbeing and later socioeconomic opportunities (Bäckman & Nilsson, Reference Bäckman and Nilsson2016; Baggio et al., Reference Baggio, Iglesias and Deline2015; Ralston et al., Reference Ralston, Everington and Feng2022). Although the concept has been criticized for being individual-focussed, composed of too heterogeneous groups and for being dependent on the cultural context (Furlong, Reference Furlong2006; Guido, Reference Guido2015), it is considered a useful indicator and conceptual tool to summarise young adult disengagement and vulnerability (Contini et al., Reference Contini, Filandri and Pacelli2019).
NEET can be understood as an unsuccessful transition from education to employment (or further education and training), which is a key feature of the broader transition process from adolescence to adulthood. Cross-nationally, the prevalence of NEET is closely linked to the institutional configurations that regulate young people’s transitions and their integration into the labour market (Bäckman et al., Reference Bäckman, Jakobsen, Lorentzen, Österbacka and Dahl2015; Brzinsky-Fay, Reference Brzinsky-Fay2007; Pohl & Walther, Reference Pohl and Walther2007; Walther, Reference Walther2006). NEET is more common in Mediterranean Europe, which has a combination of dualistic labour markets, weak education and training systems and limited public support. It is also common in the United Kingdom, where youth unemployment is combined with higher levels of (female) young adults in unpaid care (Caroleo et al., Reference Caroleo, Rocca and Mazzocchi2020; Jongbloed & Giret, Reference Jongbloed and Giret2022). NEET is typically less common in the Nordic countries due to free education, active labour market policies and low youth unemployment rates. In Finland, 9.2% of male and 9.1% of female individuals were classified as NEET in 2023. The corresponding EU averages were 10.1% and 12.5%. In the EU area, the Netherlands has the lowest NEET rates, with 4.0% of male and 5.5% of female individuals. In contrast, Romania has the highest rates, with 14.1% of male and 24.8% of female individuals classified as NEET (Eurostat, 2024).
At the individual level, NEET is more common amongst young people with low educational attainment, immigrant background or with parents of low socioeconomic status (De Luca et al., Reference De Luca, Mazzocchi and Quintano2020; Duckworth & Schoon, Reference Duckworth and Schoon2012; Gladwell et al., Reference Gladwell, Popli and Tsuchiya2022; Tamesberger & Bacher, Reference Tamesberger and Bacher2014). Low skills, as exemplified by poor school performance and low educational attainment, are particularly important predictors of NEET, as they hinder employability as well as their opportunities for further education. The influence of socioeconomic background on NEET often operates through skills and educational attainment (Gladwell et al., Reference Gladwell, Popli and Tsuchiya2022). Along with poor school performance and low educational aspirations (Duckworth & Schoon, Reference Duckworth and Schoon2012; Gladwell et al., Reference Gladwell, Popli and Tsuchiya2022), health problems – and mental health problems, in particular – increase the risk of low educational attainment (Mikkonen et al., Reference Mikkonen, Remes and Moustgaard2021). These health problems can also prevent successful integration into the labour market and increase the risk of NEET (Cornaglia et al., Reference Cornaglia, Crivellaro and McNally2015; Pitkänen et al., Reference Pitkänen, Remes and Moustgaard2021).
From a life course perspective, the factors discussed above are temporally proximate predictors of NEET that do not take into account earlier antecedents and life course processes that influence poor educational performance, school dropout and unsuccessful labour market integration (Gladwell et al., Reference Gladwell, Popli and Tsuchiya2022). Our focus on perinatal health – and birth weight as a measure of it – considers very early risk factors for NEET.
Epidemiological life course research has long considered the importance of the perinatal period in shaping health through its impact on development during a period of rapid growth (Ben-Shlomo et al., Reference Ben-Shlomo, Mishra and Kuh2023). Besides health-related outcomes, the ‘fetal origins hypothesis’ has subsequently been adopted to understand how the very early (fetal) environment influences the life course development of human capital and socioeconomic outcomes by epidemiologists, economists and social scientists (Ahmed et al., Reference Ahmed, Pullenayegum and McDonald2024; Bilgin et al., Reference Bilgin, Mendonca and Wolke2018; Cozzani & Härkönen, Reference Cozzani and Härkönen2023; Torche & Conley, Reference Torche and Conley2015).
Following previous literature and World Health Organisation (WHO) standard practice, we use low birth weight (LBW, 1500–2499 g) and very low birth weight (VLBW, < 1,500 g) as indicators of perinatal risk and early health adversities (Torche & Conley, Reference Torche and Conley2015; WHO, 2022). Low and very low birth weight results from preterm birth (before 37 weeks’ gestation), poor fetal growth or both, due to the fetus’s physiological adaptations to adverse prenatal conditions such as inflammation, stress, nutritional deficiencies or health complications (Romero et al., Reference Romero, Dey and Fisher2014; Torche & Conley, Reference Torche and Conley2015). Next to birth weight, these processes can disrupt brain and other organ development (Boggini et al., Reference Boggini, Pozzoli and Schiavolin2021; Murray et al., Reference Murray, Fernandes and Fazel2015; Romero et al., Reference Romero, Dey and Fisher2014), which can have long-term negative consequences on cognitive and neurosensory development, school performance and physical and mental health (Bharadwaj et al., Reference Bharadwaj, Lundborg and Rooth2018; Chatterji et al., Reference Chatterji, Kim and Lahiri2014; Cheadle & Goosby, Reference Cheadle and Goosby2010; Jelenkovic et al., Reference Jelenkovic, Mikkonen and Martikainen2018; Lin & Liu, Reference Lin and Liu2009; Mathiasen et al., Reference Mathiasen2009; Moster et al., Reference Moster, Lie and Markestad2008; Zhou et al., Reference Zhou2025). In other words, (very) low birth weight restricts the development of skills that are rewarded in education and the labour market and can therefore increase the occurrence of NEET in young adulthood.
Despite the importance of birth weight and perinatal health more generally on many relevant socioeconomic and health outcomes, their role has been overlooked in research on NEET and social exclusion more broadly. A few studies on NEET have included birth weight as a covariate, amongst others (Bynner & Parsons, Reference Bynner and Parsons2002), or used it as a proxy to control for genetic endowments (Gladwell et al., Reference Gladwell, Popli and Tsuchiya2022). Because birth weight has not been the focal variable in these analyses, their model specifications can produce biased estimates of the effect of birth weight. Our contribution, on the contrary, focusses specifically on the effects of (very) low birth weight on NEET.
Does parental SES moderate the effects of birth weight?
The primary channels through which birth weight operates are biological, but can its effects be moderated by the social environment, and in particular, by the childhood family’s socioeconomic status (SES), typically measured through parental education, occupational status or income? If the effects of birth weight and socioeconomic background are additive, they affect NEET independently of one another and in an accumulative fashion, and where higher family SES neither reinforces nor buffers the effects of (very) low birth weight. Different theories have proposed mechanisms through which parental SES can moderate the effects of (very) low birth weight, and thus either reinforce or buffer its effects.
LBW children in less advantaged families often live in environments less conducive to their resilience (Bradley et al., Reference Bradley, Whiteside and Mundfrom1994), whereas higher-SES parents have more economic, social and cognitive resources to pave the way for favourable socioeconomic positions (Breen & Jonsson, Reference Breen and Jonsson2005). They can use these resources to buffer from adversities related to life course risks (Bernardi, Reference Bernardi2014). Unlike low-SES parents, high-SES parents tend to allocate more time and attention to their (V)LBW children as a way to minimise the adverse effects of (V)LBW. Higher-SES parents can be in a better position to reduce working hours to care for their (V)LBW infants (Nicoletti et al., Reference Nicoletti, Salvanes and Tominey2018), and they engage more in cognitively stimulating activities with them (Hsin, Reference Hsin2012). Higher-SES parents also have higher educational and occupational aspirations for their children, which they transmit to their children. Children’s educational aspirations can foster at-risk children’s school engagement and trust in their academic capabilities (Duckworth & Schoon, Reference Duckworth and Schoon2012). High-SES parents can therefore be more resourceful in supporting their (V)LBW children and buffer the negative effects of (very) low birth weight.
Alternatively, the effects of birth weight on NEET can be stronger amongst children of higher-SES parents. Becker & Tomes (Reference Becker and Tomes1976) theorised that families have an incentive to invest in the human capital of ‘better endowed children’ (as the returns to these investments are positively related to endowments) whilst compensating the ‘less endowed’ children with non-human capital transfers. The investment motive can be less relevant in a country with free education – such as Finland – but higher-SES parents can remain in a better position to financially support children who may be unable to work or pursue further education due to health problems.
Effects of LBW can also be stronger in high-SES families for other reasons. Socioeconomic adversities, such as NEET, are more common amongst children in low-SES families (Tamesberger & Bacher, Reference Tamesberger and Bacher2014), as such children can rely on fewer social and economic resources to support their transition from school to work (or further education). For these children, additional life course risk factors – such as (very) low birth weight – can have a smaller relative influence on adversity than for children with high-SES parents. For the latter, proximate risk factors of SES are fewer or absent, and major life course risks can therefore be more disruptive. As an example of such effects, Mogensen and colleagues (Reference Mogensen, Tettamanti and Frederiksen2024) reported that the effects of severe childhood cancers on not completing secondary education were stronger amongst children with highly educated parents. (Very) low birth weight can have similar impacts.
Previous research on whether parental SES moderates the effects of (V)LBW has yielded mixed results. Some studies suggest that high parental SES can mitigate the effect of LBW on educational outcomes (e.g. Lin et al., Reference Lin, Liu and Chou2007; Lin & Liu, Reference Lin and Liu2009) and cognitive skills (Zvara & Schoppe-Sullivan, Reference Zvara and Schoppe-Sullivan2010). Other studies have, however, indicated that the effects of SES on LBW are additive (e.g. Eryigit Madzwamuse et al., Reference Eryigit Madzwamuse, Baumann and Jaekel2015) and do not vary across socioeconomic backgrounds (Beach & Saavedra, Reference Beach and Saavedra2015; Black et al., Reference Black, Devereux and Salvanes2007; Cheadle & Goosby, Reference Cheadle and Goosby2010; Currie & Hyson, Reference Currie and Hyson1999).
Data and methods
Data
We used data on full cohorts of live births in Finland between 1987 and 1992 from the Finnish Medical Birth Register (FMBR), which were linked to information on education and economic activity during 2003–2019 from registers from the Population Information System of the Population Register Centre and Statistics Finland. FMBR, governed by the Finnish Institute of Health and Welfare, is a high-quality register dataset that includes data from maternity hospitals (maternity and neonatal wards) on the health of the mother and child during pregnancy and birth as well as socioeconomic data on the mother.
After excluding cohort members who died before the age of 21 years (N = 1,193) or had missing or no information on NEET at any point during the follow-up (N = 15,809), on birth weight (N = 491) or on the mother’s smoking during pregnancy (N = 7,300), the total sample consisted of 348,906 individuals. For the sibling fixed effects analysis, we further restricted our sample to families which had multiple children during the cohort window (covering approximately 47 per cent of the children) leading to 163,056 individuals nested in 76,693 families.
We restricted our NEET analysis to young adults aged 21–27 years. NEET prevalence is sometimes measured using 15–24-year-olds (OECD, 2010) or 15–29-year-olds (Eurostat, 2024), but such definitions are somewhat challenging for our purpose. In Finland, 15–16-year-olds are in compulsory education and nearly everyone attends some form of education at age 17 years. Most Finnish male individuals aged 18–20 years complete obligatory military or civil service. Additionally, the numerus clausus system delays entry into tertiary education, making gap years common. Thus some individuals might temporarily fall into the NEET category for some time without facing the actual risk of exclusion or vulnerabilities. The upper limit reflects the upper age for which we have data for the cohorts considered. In contrast to studies on NEET amongst adolescents, our focus was on the years when young adults typically establish themselves in the labour market, gain independence and start their partnership and family lives.
Dependent variable: NEET status
In this study, NEET was considered as ‘inactive NEET’, referring to youth who are neither in employment, education or training nor seeking work (Carcillo et al., Reference Carcillo, Fernández and Königs2015), as opposed to ‘unemployed NEET’. Some argue that especially when unemployment status refers to active job-seekers, they should be considered ‘available in the labour market’ and thus not NEET (Guido, Reference Guido2015). However, others argue that the causes and consequences of unemployment status are country-specific, and especially in the Nordic countries, being unemployed during young adulthood is mostly involuntary and should be considered as NEET (Kristensen et al., Reference Kristensen, Hanvold and Hasting2021).
Information on yearly NEET status was based on the individual’s main economic activity at the end of each calendar year during 2003–2019. Those who were unemployed for more than 165 days during a calendar year, not studying, nor in training or doing military or civil service and those receiving a pension were classified as NEET. Those who would fall within the NEET category according to the above-mentioned criteria but had children under the age of 3 years were considered stay-at-home-parents instead of NEET.
Our dependent variable was a count variable of the number of years as NEET during the follow-up period; individuals could be NEET from 0 to 7 years, and the NEET years could be either consecutive or non-consecutive. We use this count variable in a Poisson regression setting, explained below, to analyze the risk of being NEET. This approach allows us to include repeated NEET spells for those who are precariously attached to education and the labour market, even when the years as NEET are not consecutive.
Independent variables
Our main independent variable is birth weight. In line with previous literature and standard classifications (see WHO 2022), birth weight was classified as very low (VLBW, less than 1500 g), low (LBW, 1500–2499 g) and normal birth weight (NBW, more than or equal to 2500 g). Maternal education was measured at the time of birth and coded into three categories: compulsory, secondary and tertiary education. Information on maternal education was derived from Statistics Finland. We controlled for variables that are associated with both young adulthood socioeconomic outcomes (Clifford et al., Reference Clifford, Lang and Chen2012; Fishman & Min, Reference Fishman and Min2018; Härkönen, Reference Härkönen2014) and birth weight (Bohn et al., Reference Bohn, Vogel and Poulain2021; De Bernabé et al., Reference De Bernabé, Soriano and Albaladejo2004; Goisis et al., Reference Goisis, Remes and Barclay2017) and thus may confound the link between perinatal health and NEET status. These variables included child sex, birth order, information on multiple birth, maternal age and maternal smoking during pregnancy.
Poisson regression and sibling fixed effects framework
To analyse the effect of birth weight on NEET, we estimate Poisson models without and with sibling fixed effects (SFE). Poisson models are used to analyse count data, as they are robust, easy to interpret and they allow for zero counts (Allison, Reference Allison2009). The distribution of the number of years our population experienced NEET is strongly non-normal, with the majority not experiencing NEET in any year, which makes Poisson regression preferable to linear regression models. Poisson models also take account of the longitudinal aspect of the data and the outcome variable does not need to be categorized. In particular, Poisson models allow us to analyse the accumulation of NEET to the same individuals who may be NEET during several – though not necessarily subsequent – years, which indicates poor integration to the labour market and heightened risk of social exclusion. A shortcoming of Poisson models is that models are sensitive to overdispersion, which may lead to deflated or underestimated standard errors. Standard errors, however, can be corrected for overdispersion by using bootstrapping (Allison, Reference Allison2009).
The advantage of SFE is that models utilize the variation between siblings in the same family to identify the effects of perinatal health on adult outcomes. The models control for measured and unmeasured factors constant at the family level and shared by the siblings. This approach allows us to adjust for many potential confounders and reduces the bias caused by the unobserved confounding. SFE approach enables us to achieve less biased estimates and to provide stronger evidence for an independent role of early health. The drawback of the models is that they restrict the analytical sample to multi-child families and singletons are thus excluded. Further, if the confounding factors are not completely shared by the siblings, SFE models can lead to biased estimates. Measured confounders that vary between siblings were presented above. Scholars have also raised a question about the external validity of SFE estimations (Frisell et al., Reference Frisell, Öberg and Kuja-Halkola2012; Sjölander et al., Reference Sjölander, Frisell and Öberg2022). We report incidence rate ratios (IRRs) and their 95% confidence intervals (CIs). IRRs present the (multiplicative) effect of (very) low birth weight on the risk of being NEET.
Results
Descriptive analysis
Table 1 presents that the full sample and the sibling (within-family) sample were similar in terms of our dependent and independent variables. For the sibling sample, we also report within-family variance in standard deviations.
Descriptive statistics of applied variables. Full sample and sibling sample

Roughly one-fourth of the individuals were classified as NEET at least once during the follow-up period (Table 1). Around 11.0 per cent were NEET for 1 year and 5.5 per cent for 2 years during the follow-up, after which the percentage gradually diminished with increasing NEET years (3–7). Only about 1.6 per cent were NEET for all 7 years. In addition to the information presented in Table 1, we estimated that approximately one-fifth of those who were NEET during the follow-up period experienced more than one NEET spell and that the median duration of a NEET spell was four consecutive years.
In both samples, roughly 97.0 per cent were born with a normal weight, 3.0 per cent with a low weight and 0.4 per cent with a very low weight. Children born with LBW and VLBW were less common amongst tertiary-educated mothers compared with other mothers (Table S1). In both samples, half of the sample persons were women. The full sample included more first-born individuals (40.2 per cent) than the sibling sample (33.1 per cent).
On average, around 19.0 per cent of the mothers had only compulsory education, 47.5 per cent secondary education and 33.5 per cent tertiary education. Average maternal education was slightly higher in the within-family sample. Maternal smoking during pregnancy was slightly higher in the full sample (16.0 per cent) than in the sibling sample (13.7 per cent). The mean age of mothers at birth was 29 years in the full sample and 28 years in the sibling sample.
Figure 1 shows the number of NEET years according to birth weight categories. In the full sample, a substantial majority of individuals born with normal birth weight were never NEET. However, there are differences in the rates of never experiencing NEET according to birth weight: amongst those born with LBW, 66.3 per cent did not experience NEET, whilst 57.3 per cent of those with VLBW were not classified as NEET during the follow-up period. Further, children born with LBW and VLBW were more likely to experience two or more years in NEET, and the relative difference was particularly large amongst those who were persistently NEET for the 7 years of the follow-up. In addition, 8.9 per cent of those who were born with VLBW were NEET for 7 years, whilst the respective figures for LBW and NBW were 3.7 and 1.5 years, respectively.
The number of NEET years throughout the follow-up period according to birth weight categories (full sample).

Overall, the figure demonstrates a higher prevalence of being NEET amongst those born with low birth weight. In terms of incidence rate ratios (IRRs), those born with LBW and VLBW had a 1.48 (95% CI 1.43–1.58) and 2.30 (95% CI 2.13–2.48) times higher risk, respectively, than the NBW population of being NEET in a given year. The average duration of a NEET spell was 2.5 years for NBW, 2.9 for LBW and 3.6 for VLBW.
Poisson regression analysis
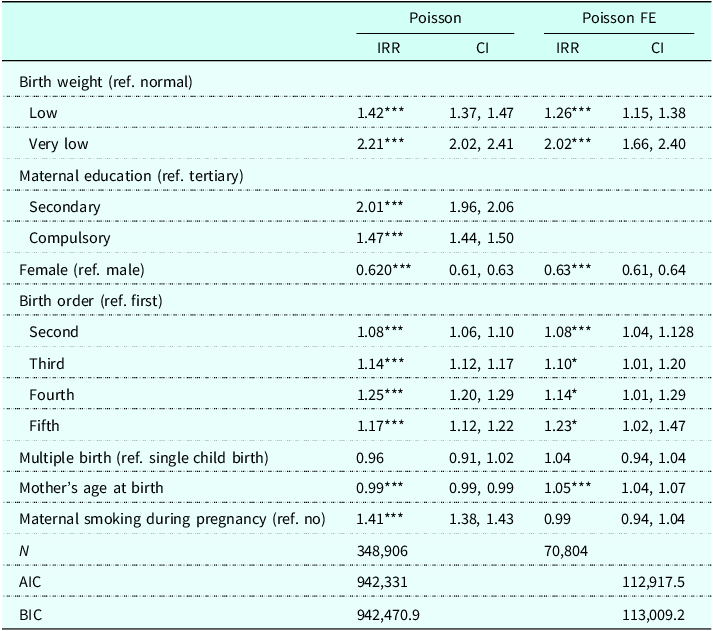
The regular Poisson regression model shows that those born LBW or VLBW were more likely to be NEET between the ages of 21 and 27 years (Table 2, left-hand panel). LBW was associated with a 1.42 (95% CI 1.372–1.472) and VLBW with a 2.21 (95% CI 2.024–2.411) times higher risk of NEET compared with NBW individuals. These increased NEET incidences were very similar to the gross incidence rate ratios (IRRs) reported above.
Poisson regression and Poisson sibling fixed effects regression on NEET. Incidence rate ratios with 95% confidence intervals

Note: Maternal education is constant amongst the siblings in the same family in Poisson FE and therefore not estimated. * p < 0.05. **p < 0.01. ***p < 0.001.
The results remained similar in the SFE model, showing that LBW was associated with a 1.26 (95% CI 1.15–1.38) and VLBW with a 2.02 (95% CI 1.66–2.40) times higher estimated risk of NEET compared with NBW (Table 2, right panel). All in all, the gross and the two regression-adjusted IRR estimates are very robust, suggesting that the associations between (V)LBW and NEET are not confounded neither by the measured variables nor by unmeasured factors that are shared by siblings from the same family.
Regarding the other variables, female individuals were less likely than male individuals to be NEET. The regular Poisson model also indicates differences in the incidence of NEET by parental education, and both models show that children of higher birth order were more likely than first-borns to be NEET. In the fixed effects setting, mothers’ smoking during pregnancy was not associated with NEET, in line with findings suggesting that the effects of maternal smoking on educational outcomes, for instance, are confounded by unobserved maternal characteristics (D’Onofrio et al., Reference D’Onofrio, Singh and Iliadou2010). Unlike in the regular Poisson model, higher maternal age is associcated with with an increased risk of NEET in the fixed effects model, which only compares siblings with the same mother. One should practice caution, however, in interpreting estimates of the control variables, because they are subject to overcontrol bias, as other variables included in the model are on the causal pathway from the control to the outcome variables (Elwert & Winship, Reference Elwert and Winship2014).
Next, we modelled the risk of NEET by maternal education using the fixed effects Poisson regression analysis (Figure 2). Those born with LBW had a NEET risk of 1.27, compared with those born with NBW across maternal educational groups. For VLBW, the risk of being NEET was the highest amongst those with tertiary-educated mothers (2.57, 95% CI 1.68–3.92) and the lowest amongst those with primary-educated mothers (1.61, 95% CI 1.19–2.18). However, as the confidence intervals were overlapping, the differences were not statistically significant. (For the covariates, see Table S2).
The effect of birthweight on NEET status by maternal education. A Poisson regression with fixed effects. Incidence rate ratios with 95% confidence intervals.

Sensitivity analysis
We also conducted a set of additional robustness checks. First, to tackle the potential sample selection bias (regarding the sibling sample), we performed the regular Poisson regression using the sibling sample. Results show that the coefficients from the full sample (including singletons) and sibling sample (restricted to siblings) were similar (see Table S3). This suggests that the sibling sample does not suffer from sample selection. Second, we replicated our analysis with two key determinants of birth weight; preterm birth (defined as being born before the thirty-seventh full gestational week) and being small for gestational age (defined as birth weight below two standard deviations from the sex and gestational age-specific birth weights), which have different aetiologies and potentially different consequences. In general, our results did not change substantially (see Tables S4 and S5). This indicates that perinatal health, regardless of the indicator used, is associated with the risk of being NEET in young adulthood. Finally, we tested the interaction between sex and birthweight categories, finding no interaction effect (χ 2 = 2.34, p = 0.31), indicating that birth weight has a similar effect on NEET amongst male and female individuals.
Discussion and conclusions
Adolescents and young adults who are not in education, employment or training (NEET) are a major public policy concern in Europe due to NEET’s costs for individuals and societies (Mascherini et al., Reference Mascherini, Salvatore and Meierkord2012; Ralston et al., Reference Ralston, Everington and Feng2022). NEET can create a disruption in the transition to adulthood, of which completion of education, successful labour market entry and financial independence are important markers (Billari & Liefbroer, Reference Billari and Liefbroer2010; Buchmann & Kriesi, Reference Buchmann and Kriesi2011), and have scarring effects on later labour market success (Ralston et. al. Reference Ralston, Everington and Feng2022). Consequently, NEET is considered an important indicator of social exclusion (OECD, 2010) and disengagement and vulnerability amongst young people (Contini et al., Reference Contini, Filandri and Pacelli2019).
Research on the predictors of NEET has focussed primarily on sociodemographic (De Luca et al., Reference De Luca, Mazzocchi and Quintano2020; Duckworth & Schoon, Reference Duckworth and Schoon2012; Gladwell et al., Reference Gladwell, Popli and Tsuchiya2022) or temporally proximate predictors, such as poor school performance (Duckworth & Schoon, Reference Duckworth and Schoon2012; Gladwell et al., Reference Gladwell, Popli and Tsuchiya2022) or health problems in young adolescence (Cornaglia et al., Reference Cornaglia, Crivellaro and McNally2015; Pitkänen et al., Reference Pitkänen, Remes and Moustgaard2021). Complementing this research, our study focussed on very early antecedents of NEET. We analysed the effect of birth weight – as an indicator of perinatal health – on NEET status amongst Finnish young adults (ages 21–27 years) by using rich and high-quality full population register data and sibling fixed effects Poisson models. LBW (< 2,500 g) increased the estimated incidence of NEET by 27 per cent and VLBW (< 1,500 g) doubled the incidence of NEET. Additionally, we studied whether the effect of birth weight was stratified by parental SES, measured by the mother’s educational level. Contrary to expectations derived from theories of compensatory advantage (Bernardi, Reference Bernardi2014), which consider parental socioeconomic resources as buffers against disadvantage (such as poor prenatal health), we did not find that the effects of birth weight were weaker amongst children of highly educated mothers. Rather, we found indications that the effects of VLBW were stronger amongst children of highly educated mothers, although the differences by educational background were not statistically significant.
The finding of a negative effect of (V)LBW on NEET in early adulthood is in line with much previous research on the effects of birth weight and other perinatal health issues on long-term socioeconomic outcomes (Cozzani & Härkönen, Reference Cozzani and Härkönen2023). This is particularly true for the VLBW children, who are at substantially higher risk of medical disabilities and compromised cognitive and neurosensory development, which are important mediators mechanisms that link birth weight with poorer socioeconomic outcomes in adulthood (Mathiasen et al., Reference Mathiasen2009; Moster et al., Reference Moster, Lie and Markestad2008). More broadly, the findings align with scholarship on early life conditions that form the foundations for development and socioeconomic achievement later in life (Ben-Shlomo & Kuh, Reference Ben-Shlomo and Kuh2002; Heckman, Reference Heckman2006). Several factors can link birth weight to NEET status. (V)LBW results from preterm birth and/or poor fetal growth due to adverse prenatal conditions such as inflammation, stress and nutritional deficiencies (Romero et al., Reference Romero, Dey and Fisher2014). These conditions can disrupt brain and organ development (Boggini et al., Reference Boggini, Pozzoli and Schiavolin2021; Murray et al., Reference Murray, Fernandes and Fazel2015), potentially leading to long-term negative effects such as lower intelligence quotient (IQ), learning disabilities and psychiatric disorders such as attention deficit hyperactivity disorder (ADHD) or anxiety disorder (Anderson et al., Reference Anderson, de Miranda and Albuquerque2021; Bharadwaj et al., Reference Bharadwaj, Lundborg and Rooth2018; Chatterji et al., Reference Chatterji, Kim and Lahiri2014; Eves et al., Reference Eves, Mendonça and Baumann2021). These conditions, independently and collectively, increase the risk of academic underperformance, school dropout and difficulties in labor market attachment.
Our finding that the effects of LBW on NEET are similar across maternal educational levels points to additive, rather than interactive, effects of parental SES and birth weight, where socioeconomic background and birth weight affect NEET independently of one another. Children from low-SES backgrounds have a higher probability of low birth weight, both of which independently increase the risk of NEET. The finding of additive effects implies that interventions that may reduce the probability of low birth weight have similar effects on those at risk of low birth weight across socioeconomic backgrounds.
Theoretically, the result, along with the indicative finding of stronger effects of VLBW amongst children of highly educated mothers, challenges models of compensatory advantage, which suggest that parents with high SES can shield their children from risks such as family dissolution, grade repetition or poor health (Hsin, Reference Hsin2012; Lin et al., Reference Lin, Liu and Chou2007; Bernardi, Reference Bernardi2014). Despite limited support for compensatory advantage, we also find it unlikely that our results support, given the Finnish context, Becker’s and Tomes’s (Reference Becker and Tomes1976) argument that highly resourced parents direct human capital to their ‘better endowed’ children whilst compensating the ‘less endowed’ ones with wealth transfers. Rather, our results suggest that family resources cannot always buffer the effects of biological disadvantage, such as (very) low birth weight. It is possible that for children of low-SES parents, who have the highest absolute risk of becoming NEET (see Table S6), major health shocks and other additional life course factors may have a relatively smaller influence on later life socioeconomic adversities compared with children of high-SES parents, as suggested by some previous research (Mogensen et al., Reference Mogensen, Tettamanti and Frederiksen2024).
Our work comes with limitations. Regarding generalizability, the study was conducted in Finland, a country with high infant health. Although our results point to clear individual-level relevance of (V)LBW on NEET in Finland, its population-level relevance is likely higher in countries where perinatal health is poorer. The effect of birth weight may also differ from those in other countries. For one, low infant and child mortality rates mean that (LBW) babies with the poorest health – who are also most likely to be NEET – may be more likely to survive to adolescence and adulthood. Second, strong support from pregnancy to adulthood, for example, high-quality health services and prenatal care systems that have positive effects on maternal and infant health (Corman et al., Reference Corman, Dave and Reichman2019; Yan, Reference Yan2017), can decrease the modifying role of parental SES in the impact of LBW. Moreover, whilst sibling models have a higher internal validity, they may not directly generalize to the singleton population. Further, the parents of (V)LBW infants tend to have fewer children following a preterm birth (Alenius et al., Reference Alenius, Kajantie, Sund, Näsänen-Gilmore, Vääräsmäki, Gissler and Hovi2018), which can be seen as a limitation of the – otherwise strong – SFE research design. It is also possible that some important covariates are not controlled for. Furthermore, it is beyond the scope of this study to examine the role of genes, gene–environment interplay and epigenetic processes that can partly explain the association between birth weight and NEET (Cook & Fletcher, Reference Cook and Fletcher2015).
Despite the limitations, our study offers several important contributions and valuable insights into the relationship between perinatal health and NEET status. The availability of full population registers allowed us to use data with very little missing information. Furthermore, by employing sibling fixed effects approach, we were able to control for important childhood and family characteristics that might confound the association. Further studies can aim to understand the causal mechanism between birth weight and socioeconomic outcomes and consider comparisons between countries that differ in their perinatal health and other public policies. More generally, our findings point to the importance of more comprehensive analysis of the role of early health policies as social investments into the human capital and future attainment of children.
The policy discussion stemming from the literature on the importance of early years has emphasized early interventions such as affordable and high-quality day care as a key for supporting human capital development equally between children (e.g. Heckman, Reference Heckman2006; Plavgo and Hemerijck, Reference Plavgo and Hemerijck2020). Our findings underline the role of the earliest environment – the prenatal one – and health at the starting gate of life as an important contributor to the risk being NEET and risk of social exclusion more broadly. A policy implication of our findings points to the role of perinatal health care as a policy input (Grossman, Reference Grossman, Culyer and Newhouse2000; Bütikofer et al., Reference Bütikofer, Løken and Salvanes2019) and social investment that can have long-term consequences for lessening social risks.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S0047279426101299
Data availablity statement
Confidential Finnish register data are not allowed to be shared under any circumstances according to strict rules of Statistics Finland. The data can be obtained from Statistics Finland by other researchers, provided that a research application is approved and service fees are paid.
Funding statement
Academy of Finland’s flagship programme funding (grant number 320162) and Academy of Finland’s project funding (grant number 324613).
Competing interests
The authors declared none.






 Open access
Open access