


Introduction
Ideas of mental health and well-being have taken an increasing importance in the twenty-first century, an importance which has also percolated into the archaeological discipline (Darvill et al. Reference Darvill, Heaslip, Drysdale and Barrass2019; Everill & Burnell Reference Everill and Burnell2022; Schaepe et al. Reference Schaepe, Angelbeck, Snook and Welch2017). However, there remains a discordance between positive discourses on mental health and the systemic discrimination or stigma that still surround what Western society deems more serious mental illnesses, conditions, differences, and disability. Since the nineteenth century in the Western world, and in some contexts earlier, people deemed by the state ‘mad’, ‘intellectually disabled’, or ‘mentally ill’ (all terms which today carry varying negative connotations) were often confined in psychiatric institutions and segregated from the rest of society. In this paper, we compare Portuguese and French past psychiatric hospitals to propose a new perspective on what it meant to be confined in European psychiatric institutions in the nineteenth and twentieth centuries. We take a people-centred approach to the archaeology of these institutions, going beyond simple architectural, spatial and material culture analyses to emphasize the emotions and lives of the people detained.
Archaeological studies of past psychiatric institutions have developed since the beginning of the 2000s, leading to a variety of approaches from architectural and spatial analysis to a focus on artefacts and material culture (Allmond Reference Allmond2016; Auld et al. Reference Auld, Ireland and Burke2019; Fennelly Reference Fennelly2019; Kuglitsch Reference Kuglitsch2023; Longhurst Reference Longhurst2015; Piddock Reference Piddock2007). Inspired by Mad studies, an academic discipline which originated from the social movements led by former patients and survivors of psychiatric institutions (Ben-Moshe Reference Ben-Moshe2020; Beresford & Russo Reference Beresford and Russo2022; Coleborne Reference Coleborne2020; LeBlanc & Kinsella Reference LeBlanc and Kinsella2016; LeFrançois et al. Reference LeFrançois, Menzies and Reaume2013), recent work by Michaut (Reference Michaut2024) has called for survivor-centric archaeologies of psychiatric institutions. One of this work’s contributions has been highlighting the role of sanism—that is, the systemic oppression experienced by people perceived as mad or mentally ill (Birnbaum Reference Birnbaum1960; Perlin Reference Perlin1992)—on past psychiatric institutions and lunatic asylums. Mad studies have also recently entered the heritage field with work by Rodéhn (Reference Rodéhn2024), Lanz (Reference Lanz2024) and Punzi (Reference Punzi2022) on the heritage of mental health and mad studies. By prioritizing the human stories behind the institutional walls, through the analysis of newspapers, photographs, medical records and other documents, an interview, and nonetheless not forgetting the architectural spaces and the material culture, we would like to dive into the personal narratives and emotional experiences of the individuals confined within these institutions, restoring agency and humanity to those often silenced or dismissed within asylum records. We aim to reconstruct the tangible aspects of asylum life and the intangible emotional landscapes—complex feelings of fear, anger, loneliness, and hope—that shaped the lives of those who lived and survived within these spaces. This approach aims to bridge the gap between structural analyses and personal microhistories, contributing to a more comprehensive understanding of lunatic asylums that honours the lived experiences and emotions of those who endured them. In doing so, we believe we can contribute to a more inclusive and empathetic archaeology that sees former patients and survivors not just as occupants of space but as individuals with stories worth telling.
The motivations behind this article are deeply personal. For one of the authors, these connections go beyond the ‘I’: his father, as will be described later, was once confined within the walls of a psychiatric hospital in Portugal and received medical care at the Miguel Bombarda hospital (formerly Rilhafoles hospital), one of the case studies central to this research. This hospital, which served as a key psychiatric institution until its closure, has left an indelible mark on Portuguese mental health history and is still recorded in popular culture through sayings such as ‘Ir para Rilhafoles’ (Gomes Reference Gomes2020), literally ‘Go to Rilhafoles’, used as an insult to mean that someone is ‘crazy’. In this article, the authors seek to honour the voices of those, like the author’s father, whose lives were significantly impacted by these institutions. The research was born from a desire to confront the silences surrounding patients’ lived experiences, often absent from official clinical records and institutional narratives. By re-centring the human stories (micro-histories) within these macro-histories, the authors aim to challenge the systemic silences surrounding the lives of the residents of past psychiatric institutions. The authors recognize that this personal connection necessarily impacts their perspective and the questions asked. However, rather than compromising analytical rigour, this positionality is approached reflexively, while interpretations remain grounded in archival, material and spatial evidence. This standpoint is intended to strengthen, rather than obscure, the transparency of the research process.
This paper compares two case studies: the lunatic asylum, then psychiatric hospital, of Cadillac-sur-Garonne, in southwestern France, and the Miguel Bombarda psychiatric hospital (formerly Rilhafoles hospital) in Lisbon, Portugal (Fig. 1). Besides the authors’ areas of expertise, there were ties between the two countries, with nineteenth- and early twentieth-century Portuguese psychiatrists and laws often taking inspiration from the French context (Morgado Pereira Reference Morgado Pereira2018). It is worth noting that although psychiatry followed a relatively similar course throughout the Western world, both examples are from Catholic Europe, and future comparisons with Protestant, northern or eastern European countries, and non-European countries, could shed light on unexpected differences.
Location of the Cadillac and Miguel Bombarda psychiatric hospitals in western Europe. (Map: Elias Michaut.)

Figure 1 Long description
The map of Western Europe shows the locations of Cadillac and Miguel Bombarda psychiatric hospitals. Cadillac-sur-Garonne is marked in France, while Hospital Miguel Bombarda is marked in Portugal. The map includes surrounding countries such as Germany, Belgium, Luxembourg, Switzerland, Italy, Spain, and Portugal. Key geographic features like the English Channel, Celtic Sea, Bay of Biscay, Gulf of Lion, and Ligurian Sea are labeled. The map uses a scale of 0 to 500 kilometers for distance measurement.
Our study combines site visits, archival research, architectural analysis and an interview with a former patient, father of one of the authors. Site visits allowed for direct engagement with the physical remnants of the institutions, capturing the spatial configurations, sensory atmospheres and material legacies that shaped the patients’ lived experiences. In the Miguel Bombarda case study, we had full access to the spaces (no longer in use), which contrasted with the spaces at Cadillac, to which we had no internal access (still in use). In Miguel Bombarda, the material legacies were displayed as in a museum (see Figure 6, below) outside their original places, which limited our sensorial experience. Archival research included examining institutional reports, architectural plans, newspaper articles and administrative documents, with specific attention to the few records providing insights into interned individuals’ personal stories and emotional struggles, revealing perspectives often absent from official narratives. An important source is a collection of newspaper clippings relating to news from Hospital Miguel Bombarda, currently in the library of Hospital de São José. Since access to the actual newspapers is currently unavailable, we will refer to this collection as ‘Episódios’ (followed by the newspaper name and date on which and when the news item appeared). However, it is important to note that, except for Domingos Oliveira dos Santos’s voice, we are not directly giving patients a voice. Rather, we are offering a different reading of all the materialities and archives analysed, when compared with traditional narratives.
The article begins with a historical overview of the French and Portuguese contexts of the two psychiatric institutions under study. The following section analyses the space of these institutions, exploring how architectural and administrative structures enforced segregation, isolation and strict power dynamics. By examining these spaces as sites of control, we explore the ways patients were systematically marginalized, confined and disciplined. We also critique the broad, essentialist view of ‘lunacy’, revealing how internment was often a matter of social exclusion and undesirability rather than genuine care. The next section addresses the mortality rates within these asylums and discusses the non-correspondence between the institutions’ ideals and their material reality. Building upon this, we then investigate how various actors (medical practitioners, administrators, legal authorities, and wider societal norms, etc.), voluntarily or not, collectively contributed to the systematic dehumanization of those confined. Individuals, we contend, were reduced to ‘non-persons’ through practices of social exclusion and legal erasure, and by treating them as medical curiosities, something we would like to deconstruct. We also explore how this contributed to these individuals’ symbolic and literal disappearance from collective memory. Finally, the last section discusses the emotional landscapes of psychiatric confinement, exploring, as mentioned, how fear, anger, loneliness and hope impacted the lives of those inside these institutions and how these emotions were not only responses to trauma, but also forms of survival and resistance.
Historical context
From the late nineteenth century, most of the psychiatric discourse in Portugal was inspired by the French and German schools of psychiatry, with many of the nineteenth- and twentieth-century figures of psychiatry in Portugal having been trained in France (Cintra Reference Cintra2012; Morgado Pereira Reference Morgado Pereira2018). Although in many situations, the impetus behind these laws was a desire to improve living conditions and prevent abuse in existing institutions, we argue that the final effect was the social control of the people perceived as ‘mad’. In France, the law of 30 June 1838, commonly called ‘law on the aliénés’, placed under public control all institutions dealing with those considered mad. It enforced the creation of at least one public lunatic asylum per département (a French geographical subdivision) and created a legal difference between voluntary and involuntary commitment (De Bures Reference De Bures2006). This law influenced the regulation of psychiatric institutions in Europe, and indeed, half a century later, Portugal adopted a similar law: the Sena Law of 4 July 1889. The law aimed to improve the living conditions of people confined in psychiatric institutions, reorganize at a national level the various institutions dealing with those deemed mentally ill, and enshrine in law the division between patients criminally convicted and the others. Unfortunately, the law was never fully implemented because of financial and political problems (Candeias et al. Reference Candeias, Macedo, Esteves and Sá2021).
Our first case study, the psychiatric hospital of Cadillac-sur-Garonne (France), had been receiving people for their perceived madness since at least the seventeenth or eighteenth century, but the 1838 law officially transformed it into a public departmental lunatic asylum (Bénézech Reference Bénézech2008). Located along the Garonne River, 34 kilometres south of Bordeaux, the region’s capital, Cadillac is a former medieval town. Since the early nineteenth century, it has been characterized by a carceral landscape: in addition to the psychiatric hospital of Cadillac, the nearby castle of Cadillac hosted a prison for women from 1818 to 1891 and then a youth detention centre for girls from 1891 to 1951 (Emery Reference Emery2017; Mendelsohn Reference Mendelsohn2015).
From 1844 until 1920, Cadillac housed only men, while the Saint-Jean asylum in Bordeaux housed only women (Bénézech Reference Bénézech2008). The history of Cadillac was impacted by the two world wars, receiving many traumatized soldiers during the First World War (Bénézech Reference Bénézech2015) and facing a famine during the Second World War (Bénézech 2016; Reference Bénézech2018). The psychiatric hospital is also associated with the now-famous ‘cemetery of the forgotten’ (Cimetière des Oubliés in French), a twentieth-century burial ground for patients (Ministère de la Culture 2024). Today, the psychiatric hospital of Cadillac is still a mental health facility. Since 2016, it has housed a ‘hospital prison’, a high-security mental health unit for incarcerated people (Brossard Reference Brossard2016), located next to the cemetery of the forgotten.
Our second case study is the Miguel Bombarda psychiatric hospital (initially known as Rilhafoles hospital), located in Lisbon (Portugal). Despite opening in 1848, ten years after the passing of the French 1838 law, it was the first modern psychiatric hospital in Portugal, and it would remain the only Portuguese institution of the sort for around 50 years (Cintra Reference Cintra2012). Before Miguel Bombarda hospital, the ‘insane’ were housed in the Royal Hospital of São José. The conditions in this place were described as insalubrious and incompatible with proper care, due to overcrowding. By the 1840s, several reports and medical voices denounced the crowding and degradation of the spaces, prompting the appointment of a governmental commission to evaluate the situation (Necho Reference Necho2019; Nogueira Reference Nogueira1934; Pacheco Reference Pacheco2008). During an inspection in October 1848, the Duke of Saldanha, also minister of the Kingdom’s Affairs, showed his deep discomfort with the conditions in which the patients were housed: ‘I cannot find adequate words to express the horror I felt at the state in which I found the insane (…) The wild beast cages in all the animal yards I have seen are magnificent dwellings compared to the dungeons in which the unfortunate insane suffer’ (Cintra Reference Cintra2012, 22). The first patients were moved to Rilhafoles (later Miguel Bombarda) hospital, a former religious house, on 13 December 1848. Since then, until its closure in July 2011, 163 years later, Rilhafoles has accommodated more than 66,000 patients.
Space and segregation
Walking through the sites of Cadillac and Miguel Bombarda, an attentive passer-by might be struck by the omnipresence of material traces of segregation: tall walls compartmentalizing space, and bars on windows (Fig. 2). The old psychiatric hospital of Cadillac is surrounded by a wall that isolates it from the rest of the city. It is located outside the town’s medieval walls. Miguel Bombarda Hospital is also located on one of the hills of Lisbon, which was considered out of the city at the time of the asylum’s foundation. Although some argued the fresh air and the beauty of the landscape were beneficial to patients’ mental and physical health, other official narratives emphasized that the position away from the urban centres also reflected a will to hide these institutions and their residents from the rest of society (Pulido Reference Pulido1851, 4). Societal shame was central to the treatment of people considered mentally ill throughout the nineteenth and twentieth centuries (Cascais & Medeiros Reference Cascais and Medeiros2016; Foucault Reference Foucault1988). Yet Cadillac and Miguel Bombarda were paradoxically also located not too far from large urban centres—the first in Bordeaux and the second in Lisbon. We contend that many psychiatric hospitals built in the nineteenth century in Western Europe followed a similar principle: that of being accessible but hidden. As Francisco Martins Pulido wrote, ‘the mad were conveniently isolated from (…) town, however, in sinister cases they could also be promptly rescued’ (Pulido Reference Pulido1851, 4).
Corridor in the central building with bars separating people in the Miguel Bombarda hospital. (Photograph: Antonio Sacchetti, 2024.)

Figure 2 Long description
The black and white photo captures a long, dimly lit corridor in a psychiatric hospital. The corridor is divided into sections by metal bars, creating a sense of separation and confinement. The walls are lined with windows that allow some natural light to filter in, casting shadows and highlights on the floor. The overall atmosphere is somber and reflective, emphasizing the isolation and institutional nature of the space.
The residents of psychiatric hospitals were not simply segregated from the rest of society, but also among themselves within the psychiatric institutions. Foucault (Reference Foucault1977), primarily discussing prisons but also referring to schools and psychiatric institutions, wrote about compartmentalization as a means of intensifying discipline and inculcating docility in individuals. Patients in psychiatric hospitals were, for instance, spatially separated based on their gender (see the plans of Cadillac and Miguel Bombarda in Figure 3) but also according to family wealth, behaviours and hygiene (Cintra Reference Cintra2012, 32; Pulido Reference Pulido1851, 9). The situation in asylums was often worse for women, since they were considered to be more prone to mental illnesses (Necho Reference Necho2019, 82; Pulido Reference Pulido1851, 72), with menstrual problems and pregnancy being seen by nineteenth-century Portuguese male medical staff as potential sources of mental illness (Mattos Reference Mattos1884, 18). These misogynistic scientific perspectives, together with the protocol of admission to Rilhafoles—whereby private individuals could request the admission of another individual, needing only a medical certificate (Regulamento 1851, 10)—placed women in situations of great dependence on their husbands. For example, in 1918, a 48-year-old woman from Lisbon’s high society left her home and family to live her passion with a younger man of lower status. Instead of granting her a divorce, her husband committed her to a mental institution. A doctor signed the diagnosis of insanity. Her wealthy status enabled her to fight for her freedom in court, but only in 1944, after her husband died, was she officially recognized as lucid and healthy (Diário de Notícias 2020). Probably many working-class women faced similar situations, without the possibility of legally challenging their interment. Various archaeological studies have approached psychiatric hospitals adopting a feminist lens (Atwell Reference Atwell2022; Lans Reference Lans2022), and this angle might be worth exploring further in future studies of Cadillac and Rilhafoles. The psychiatric system not only targeted women, but also persecuted those who defied sexual and gender norms more broadly. A striking example is the ballet dancer Valentim de Barros, who was detained at Rilhafoles from 1939 until his death in 1986 due to his homosexuality and non-conforming gender expression (Afonso Reference Afonso2019; Fontes Reference Fontes2016).
(a) Plan of the asylum of Cadillac-sur-Garonne in the late nineteenth century (Digital drawing: Elias Michaut following a historical plan kept in the Gironde departmental archives in Bordeaux); (b) Plan of the Rilhafoles psychiatric hospital in 1855 (Historical plan kept in the Arquivo Nacional da Torre do Tombo.)
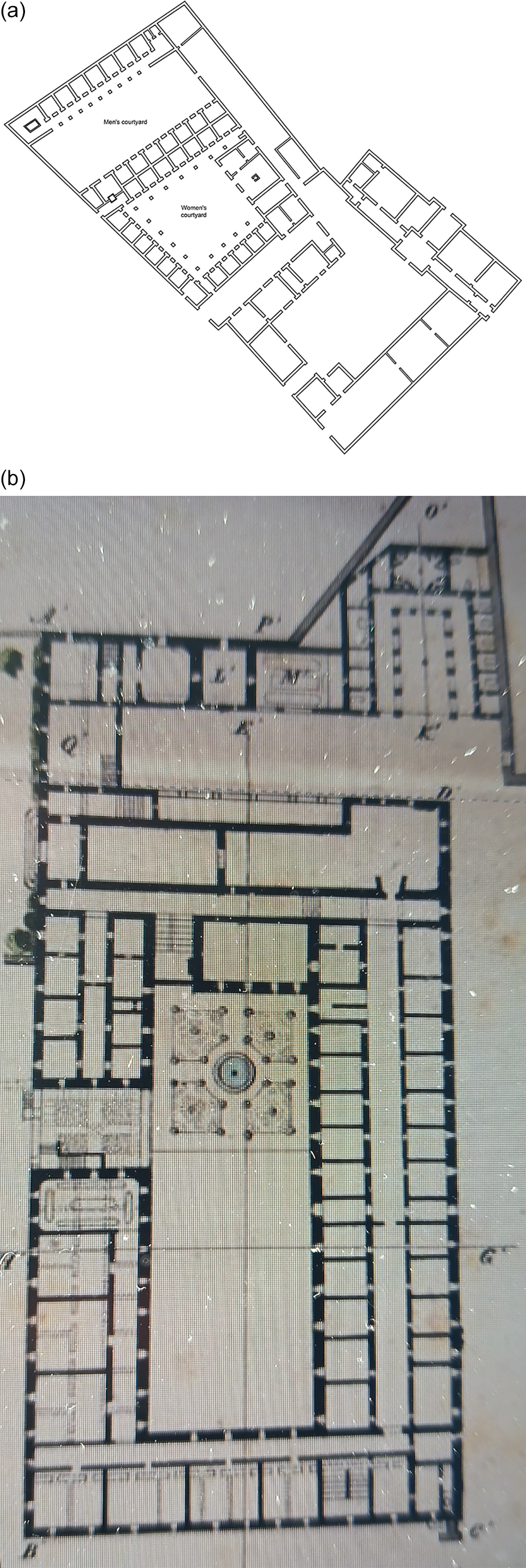
Figure 3 Long description
The image shows two architectural plans of psychiatric hospitals. The first plan, labeled (a), depicts the asylum of Cadillac-sur-Garonne from the late nineteenth century. It includes various rooms and structures, likely representing different areas of the asylum. The second plan, labeled (b), shows the Rilhafoles psychiatric hospital from 1855. This plan also includes detailed layouts of rooms and structures, providing a historical view of the hospital’s design.
Class divisions were another facet of oppression reproduced in the segregated spatial layout of the psychiatric hospitals. In Rilhafoles, like in Cadillac, there were divisions between detained individuals who paid to stay and those who did not. In 1851, Francisco Martins Pulido described how the residents of Rilhafoles were divided into four classes of paid-for pensioners and several classes of indigents who could not pay, the latter being further divided according to hygiene and ‘agitation’ (Pulido Reference Pulido1851, 8). A similar situation is reported in a 1869 report from Cadillac which describes four classes of pensioners and various classes of indigents (Icard Reference Icard1870). This rigid class structure sometimes gave rise to everyday acts of solidarity among the patients, with, for instance, wealthier patients offering some of their food to lower-class patients (Domingos Oliveira dos Santos pers. comm., Reference Santos2024). While this testimony dates to the mid twentieth century and cannot be taken as direct evidence for nineteenth-century practices, archival sources indicate that class-based segregation within the institution persisted over time, allowing this account to be read as an illustrative continuity rather than a claim of direct equivalence. Finally, a strict division also existed between patients and staff. In Rilhafoles, the Bombarda family settled on a luxurious floor of the old convent, which even had rooms for servants. On the other hand, the detained patients lived in rows of cells in the same building. These arrangements indicate how power relations were materially and spatially articulated, notably through the vertical separation of staff and patients and the compartmentalization of patient living spaces. These arrangements are characteristic of what Maguire and Costa (Reference Maguire and Costa2018) have described as ‘reverse buildings’, with the medical staff being able to move freely while the patients are compartmentalized, fixed and kept under control.
A detailed spatial analysis of Cadillac and Rilhafoles falls beyond the scope of this article which prioritizes lived experience over architectural quantification, especially as studies of power relations and spatial layout have already been conducted in archaeology. However, we would like to draw attention to one specific example from Rilhafoles: the panopticon built between 1892 and 1896 (Figs 4 & 5). Panopticons were an eighteenth-century invention of philosopher Jeremy Bentham. Bentham’s original design was a circular building lined with individual cells, with a tower in the middle from which a single staff member could simultaneously observe all the detained individuals. And even if no staff member was in the central tower, patients would not be able to know and would, theoretically, behave as if they were being watched. For Foucault (Reference Foucault1977), the panopticon epitomizes disciplinary power over the body, enforcing docility by individualizing the people detained and putting them under constant surveillance. The panopticon of Rilhafoles was a circular building lined with over 20 cells, a refectory and baths. It had been built by order of Miguel Bombarda to maximize control over the people considered ‘most dangerous’ in the establishment. Considerations were taken to adapt the structure to the asylum, rounding the edges of steps and door frames (Fig. 5) to avoid detained residents harming themselves. Although the panopticon may have seem justified to control people at risk of harming themselves or others, it also ended housing for years people like Valentim de Barros, detained simply for his homosexuality (Cascais & Medeiros Reference Cascais and Medeiros2016). Currently, the structure is disused, and there are ongoing discussions regarding its future destination. In the meantime, periodical visits to the building are organized, and artefacts from the late years of the institution are kept in the various rooms of the panopticon, such as an electroshock machine pictured in Figure 6. Unfortunately, it is not possible to know the original location of these materials, and the electroshock machine was probably moved around after the hospital’s closure.
The panopticon at Miguel Bombarda hospital. (Photograph: Antonio Sacchetti, 2024.)

Doors to the cells and benches without corners of the panopticon of the Miguel Bombarda hospital. (Photograph: Antonio Sacchetti, 2024.)

Figure 5 Long description
A series of identical doors, each with a small window and a metal handle, line a white wall. In front of each door, there is a small, round bench with a blue base. The floor is concrete, and a patch of grass is visible on the left side. The ceiling above is curved and supported by pillars, with small circular windows near the top.
Electroshock machine kept in one of the rooms of the panopticon of Miguel Bombarda hospital. (Photograph: Antonio Sacchetti, 2024.)

As discussed with the example of the women institutionalized by their husbands, or with the case of Valentim de Barros, the definition of what constituted mental illness or ‘lunacy’ fluctuated through time often to include those deemed undesirable by moral society. Political activism or homelessness were often sufficient reasons to be interned in psychiatric institutions. An 1851 report from Rilhafoles mentions alcohol abuse, prostitution, onanism, failed love passion, domestic heartbreak, jealousy, remorse, or political upheaval as causes of internment (Pulido Reference Pulido1851, 60), while an 1869 Cadillac report similarly mentions onanism, alcohol excess, jealousy, ambition, love or extreme religious feelings (Icard Reference Icard1870, 10). Intra-familial grievances were also a common reason—for instance, one individual was committed to Cadillac in 1852 by other members of his family after an inheritance dispute. Interestingly, there are also several examples of elderly men, such as Mathias Julg in 1851 and Martin Gonzalès in 1863, who had both previously been to prison for rebellious reasons (both made threats and insults towards local authorities or police officers) and were sent to Cadillac once their prison sentence ended, rather than being released (Hôpital de Cadillac Reference de Cadillac1873). It is important to keep in mind this anti-essentialist view of madness when discussing the people detained in these institutions, as internment did not necessarily correlate with mental distress and was often a socio-political tool. On the other hand, the files from Cadillac show that many of the patients were indeed individuals who had experienced mental health breakdowns, but did not benefit from strong enough familial support to keep them out of the asylum (Hôpital de Cadillac Reference de Cadillac1873). This past role of asylums in managing people with mental health conditions who did not have sufficient community support must be acknowledged, although the conditions of this management were most often appalling, imbued with paternalism (as will be discussed below), indifferent to the autonomy of the patients, and at odds with contemporary recommendations on dealing with mental distress.
Surplus of deaths
The isolation, poor living conditions and spread of diseases led to high numbers of deaths in Rilhafoles and Cadillac. The cemetery of the forgotten (cimetière des Oubliés) of Cadillac (Fig. 7), in use between 1922 and 2000, is a testimony to this high mortality. It was created after the First World War, as many former soldiers institutionalized at Cadillac for post-traumatic stress disorders died of tuberculosis. It is worth noting that at least a quarter of these soldiers were of African origin, enrolled in the French colonial troops (Bénézech Reference Bénézech2015). The cemetery is 135 m long and 35 m wide. Nearly 900 standing iron crosses are today geometrically arranged throughout the cemetery, although is estimated that over 3000 patients have been buried in that plot of land, most without grave markers and directly in the soil (Bénézech Reference Bénézech2008; Ministère de la Culture 2024).
The cemetery of the forgotten of Cadillac. (Photograph: Elias Michaut, Reference Michaut2024.)

Figure 7 Long description
The image shows a cemetery with many black crosses arranged in rows on a grassy field. The crosses are simple and uniform, indicating a memorial for a large number of individuals. The field is surrounded by trees, including a large tree on the right side. In the background, there is a wall with some buildings visible behind it. The sky is partly cloudy, suggesting a clear day. The overall scene is serene and solemn, reflecting a place of remembrance.
The cemetery of the forgotten is separated by a wall from the municipal cemetery where the free inhabitants of Cadillac are buried. The wall is tall enough that the graves of the cemetery of the forgotten are not directly visible from the municipal cemetery, despite being adjacent to it. A door in the wall connects the municipal cemetery to the cemetery of the forgotten (Fig. 8). From the nineteenth century onwards, many French psychiatric hospitals developed their own institutional cemeteries distinct from municipal cemeteries. Another famous one is the ‘cemetery of the insane’ of Navarre, near Evreux (northern France), which was built in the 1860s in woods behind the establishment, out of the view of the public (Michaut Reference Michaut2024). In Cadillac, as in Navarre, the spatial visibility of these cemeteries was different from municipal ones (Navarre was surrounded by woods, Cadillac was hidden behind a wall from the adjacent municipal cemetery), as was the treatment of the buried (few or no permanent graves, most without inscriptions). Even if pragmatic motives played a role in the creation of these distinct cemeteries (such as worries about overcrowding municipal cemeteries), the consistent differences in term of their visibility and their treatment of deceased people point to a differential treatment of institutionalized individuals, which we believe is in line with their well-documented stigmatization in nineteenth- and twentieth-century French society (see Foucault Reference Foucault1988 and Le Bras Reference Le Bras2024 for discussions of this stigmatization). In these cases, burial practices mimicked life dynamics: the patients were segregated both in life and in death, effectively remaining stigmatized.
Door in the wall separating the cemetery of the forgotten from the municipal cemetery of Cadillac. (Photograph: Elias Michaut, Reference Michaut2024.)

Figure 8 Long description
The image shows a concrete wall with an archway that separates the cemetery of the forgotten from the municipal cemetery of Cadillac. On the left side of the archway, there is a red sign with white text that reads ‘ENTREE INTERDITE AUX ANIMAUX.’ On the right side of the archway, there is a white sign with black text that provides information about the cemetery of the forgotten. Beyond the archway, rows of crosses are visible, marking graves in a well-maintained grassy area. The scene is set under a partly cloudy sky, with trees and greenery visible in the background.
Past lunatic asylums and psychiatric hospitals participated in the large-scale disappearance of people deemed by society, the state and often their own communities to be either ‘mad’ (because they were experiencing a mental health crisis or had a specific disability) or ‘undesirable’ (because of their homosexuality, political activism, sex work, etc.). This disappearance happened through confining people into closed institutions, often until their death, which frequently happened early because of poor living conditions and the fast spread of diseases in enclosed environments. Michaut (Reference Michaut2024) has used the concept of sanist death-worlds to describe the creation of these asylum landscapes characterized by very high mortality.
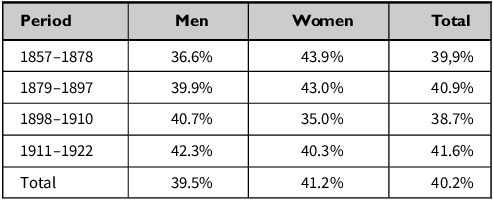
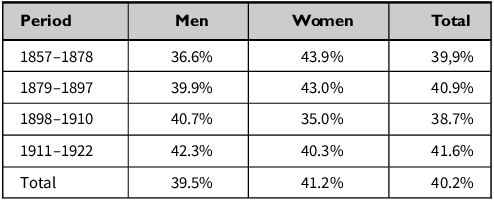
Many people who entered psychiatric institutions never left them. In Rilhafoles, between 1857 and 1922, around 40 per cent of the people who were admitted to the hospital remained there until their death. This number of 40 per cent remains constant over the whole period (see Table 1). Unfortunately, it was impossible to determine the specific causes of death, whether cholera epidemics, tuberculosis, or other. In a prior analysis of Rilhafoles, Cunha-Oliveira and Cunha-Oliveira (Reference Cunha-Oliveira, Cunha-Oliveira, Pereira and Pita2006, 89) noted very high mortality rates at the site, typical of populations experiencing health catastrophes.
Mortality rates in Rilhafoles by date of admission. The data are taken from the Men and Women entrance registers of Rilhafoles kept in the Torre do Tombo National Archive, references PT/TT/HSJ-ZHRL/004 and PT/TT/HSJ-ZHRL/005.
In Cadillac, Bénézech (Reference Bénézech2011) conducted a study on the mortality at the psychiatric hospital between 1923 and 1952. Over those three decades, at least 3453 internees died, with the two most frequent causes of death being cachexia (i.e. significant weight and muscle loss) and tuberculosis. The average age at death was around 40 years old. Between the 1920s and the Second World War, there were about 100 deaths per year on average, a number which then went down after the war. The year with most deaths was 1941, with 606 deaths due to a famine during the Second World War. According to Bénézech’s later historical research on the topic (Reference Bénézech2016; Reference Bénézech2018), this 1941 famine was worsened by staff members diverting the food intended for the patients, as demonstrated by various administrative and legal proceedings from the time. In Cadillac, as in Rilhafoles, the patients were therefore often exposed to conditions leading to high numbers of premature deaths.
Archaeologists like Piddock (Reference Piddock2007) and Longhurst (Reference Longhurst2015; Reference Longhurst2017) have discussed how what they term psychiatric ideals (such theoretical ideas surrounding care and cure) often did not correspond to the material reality of psychiatric institutions. A striking example of this non-correspondence happened at Rilhafoles in 1893. The director at the time was Miguel Bombarda, who had ceased some of the previous most brutal treatments in the institution (Cintra Reference Cintra2012). However, despite Miguel Bombarda’s apparent ideals, in 1893 an employee savagely beat a patient. Death was averted only by the intervention of other employees and patients (Episódios, Diário de Noticias 1893). Although there are no official numbers, a substantial body of historical and sociological literature has documented the routine use of physical violence within psychiatric institutions, including beatings by attendants framed as discipline, restraint, or care (Chamberlin Reference Chamberlin1979; Metzl Reference Metzl2010; Rothman Reference Rothman2002; Szasz Reference Szasz1977; Reference Szasz2010). In the case of Cadillac and in favour of this perspective of non-correspondence, one may explain some of the peaks in numbers of death by the increased pressure put on the establishment by the world wars and the influx of traumatized soldiers.
However, the discipline of Mad studies—born out of the political self-organization of psychiatric patients and former patients during the twentieth century—proposes an alternative and more complex reading of the situation. As argued by Beresford & Russo (Reference Beresford and Russo2022), the lives of institutionalized individuals were often seen as having less value than those of ‘sane’ individuals. Scholars such as LeBlanc and Kinsella (Reference LeBlanc and Kinsella2016) defend that nineteenth- and twentieth-century ideals of psychiatry were often rooted in paternalistic and top-down views of patients, denying them autonomy. In medical settings, institutional injustice towards people with experience of mental health problems still exists today and leads to failures to believe the individual and, as a result, failures or delays in responding to sometimes critical health issues (Hui et al. Reference Hui, Rennick-Egglestone and Franklin2021; LeBlanc & Kinsella Reference LeBlanc and Kinsella2016; Perry et al. Reference Perry, Lawrence and Henderson2020).
Scholars have termed sanism this systemic prejudice towards individuals with actual or perceived mental health conditions (Birnbaum Reference Birnbaum1960; Perlin Reference Perlin1992). This societal prejudice and stigma are not new and have been a constant in the treatment of people perceived as ‘mad’ over the last few centuries (see Le Bras Reference Le Bras2024 for stigma in the historical French context). Foucault (Reference Foucault1988) went further to argue that, historically, psychiatric institutionalization was as much about socially managing and controlling individuals excluded from society, creating the ever-changing category of ‘madness’, as it was about supporting or caring for them. In various movements of former psychiatric users and in Mad studies, this view led to calls for greater emphasis on the autonomy and dignity of people with mental health conditions in need of care. In the second half of the twentieth century, political consciousness gained around these issues led to the deinstitutionalization movements and the abolition of many closed-site psychiatric institutions (Ben-Moshe Reference Ben-Moshe2020).
Although issues like overcrowding, underfunding, or understaffing (or under-training of staff) definitely had dramatic consequences on the number of deaths in nineteenth- and twentieth-century institutions, insights from Mad studies force one to acknowledge that the sanism that was structural to these closed institutions provided a backdrop for these deaths to happen. Some staff may have acted with the best intentions, to their knowledge, yet the system within which they moved was a hierarchical one, inseparable from broader sanist attitudes in society and with dramatic consequences (Beresford & Russo Reference Beresford and Russo2022; LeBlanc & Kinsella Reference LeBlanc and Kinsella2016; Foucault Reference Foucault1988). Regardless of whether one ascribes more or less weight to this factor, the frequent dehumanization of patients pointed out by scholars and patients themselves must therefore be kept in mind when discussing the high mortality observed in western European psychiatric hospitals (as already pointed out in archaeology by Michaut Reference Michaut2024). In addition, for heritage specialists, being aware of these dynamics calls for a re-centring and re-humanizing of the survivors and their memories in narratives about past psychiatric institutions.
Non-persons, bare life and memory
In line with perspectives inherited from Mad studies, we contend that, throughout the nineteenth and twentieth centuries, people confined in asylums and later psychiatric institutions were subject to circumstances and processes which dehumanized them. Dehumanization, therefore, becomes a crucial analytical lens to understand the experience of people detained in psychiatric institutions and the materiality of these institutions (although we also do not pretend that this experience of dehumanization was universal to every single resident of psychiatric institutions). We also contend that exploring these processes of dehumanization is a necessary step to achieve redress in the memorial field (see McAtackney Reference McAtackney2022 on transforming confinement spaces into sites of conscience), especially as the knowledge, experience and lives of people confined in psychiatric institutions has tended to be disregarded, repressed and shunned (LeBlanc & Kinsella Reference LeBlanc and Kinsella2016; Michaut Reference Michaut2024).
Agamben (Reference Agamben1998) proposed that in extreme contexts like camps, human life was reduced to its biological existence, to a bare life, with social, political and legal relations and recognition reduced to a minimum. Building upon this idea of bare life, we examine how asylum patients were stripped of their identities and reduced to ‘non-persons’ in the eyes of the institutions and society, through paternalistic and often dehumanizing frameworks. This idea of ‘non-person’ is a parallel with Augé’s (Reference Augé1992) concept of ‘non-place’, transient places with little identity. People are made by the ‘network of personal, familial and social interactions’ within which they exist (Rovelli Reference Rovelli2018, 162). Aspects of personhood in the contemporary world may include the knowledge one has of oneself, the legal recognition of oneself as a person, the memories and knowledge others have of us, or the view society or our community has of us. We argue that the dehumanizing and paternalistic frameworks which existed in nineteenth- and twentieth-century European psychiatric institutions, and their functioning as places of disappearance, dramatically affected these aspects of personhood. The idea of non-person that we present here shares many similarities with the concepts of social death (Patterson Reference Patterson1982) or of not-quite-human or non-human (Weheliye Reference Weheliye2014). However, these two latter concepts have mostly been used to refer to racialized people in the aftermath of slavery and colonialism, and thus we did not wish to appropriate them for what in nineteenth-century Europe was a predominantly white context (although not exclusively). It is, nevertheless, worth noting that today, in many European countries such as the United Kingdom, Black people tend to be detained in psychiatric institutions in much higher proportions than white people (NHS Mental Health Services 2023), and that these concepts could in many contexts be merged.
In the nineteenth century, entering the asylum often meant going through a capitis diminutio, that is, the loss of most of one’s legal rights because of being considered incapable and irresponsible. Most asylums were completely segregated from the outside world, and the patients in the two institutions studied had little control over their time, space, activities, and to an extent, identity (Cascais & Medeiros Reference Cascais and Medeiros2016, 115). What was thus obtained was a life separated and excluded from itself, nothing more than a bare life (Agamben Reference Agamben1998). For many, and as demonstrated by the high mortality rates described above, entering an asylum was probably also a journey of no return. As shown with the cemetery of Cadillac, even after death, the existence of the former patients was hidden, quite literally, behind a wall.
However, worse than being forgotten by the state was being forgotten by one’s own family and friends. Asylums were often used by families to get rid of family members who were judged to be burdensome. Examples of this are numerous in the archives of Cadillac and Miguel Bombarda, as discussed earlier. Even when ties with the communities subsisted, the far-away location of the asylums, difficulties of access and the stigma surrounding them accelerated the oblivion process (see also the description of this in Cascais & Monteiro Reference Cascais and Medeiros2016, 139). People were made to disappear in these institutions. These processes are also evident in some archival records. For instance, after being considered cured and with no place to go, some of the patients of Miguel Bombarda hospital were sent in the 1950s to a homeless shelter in the Alcobaça monastery, more than 100 km north of Lisbon. As Catarina Gomes writes (Reference Gomes2020, 185–214), there are thousands of books in the archives of the monastery, including a description of the copper pipes of the building’s kitchens. However, no information has survived about the homeless shelter. The names and lives of the people interned were removed from written records and contemporary memory.
In addition to this disappearance, Ervin Goffman (Reference Goffman1961, 21) discusses how people in asylums were ‘stripped of one’s identity’. Cognitive science has shown that social support and relationships play a fundamental role in building and maintaining memory, and that if these are missing, people may start to lose their sense of self (Conneely et al. Reference Conneely, McNamee and Gupta2021; Kitwood Reference Kitwood1997). In asylums, Goffman (Reference Goffman1961) calls this identity erasure the ‘mortification of the self’, a process which happens as a result of taking away people’s belongings, separating them from their loved ones and imposing routines that go against individual choices, gradually erasing a person’s sense of self. Consequently, prolonged confinement within asylum environments not only jeopardizes mental health, but also disrupts the fundamental processes through which personal identity is developed and sustained (Omer & Broome Reference Omer, Broome, Monk, Lindgren, McDonald and Pasfield-Neofitou2017).
Finally, the dehumanization of asylum patients reached its extreme in nineteenth-century descriptions of patients as animals. People deemed mentally ill were often seen as curiosities (Cascais & Medeiros Reference Cascais and Medeiros2016, 134), and the medical profession interacted with them as objects of study. Theories from the beginning of the twentieth century postulated that it was possible, just from looking at patients, to recognize their madness (Cardoso Reference Cardoso2003, 58–9; Cascais & Medeiros Reference Cascais and Medeiros2016, 132). In Bordeaux, before Cadillac, in 1802, in exchange for a certain payment, the guards of the asylum let the curious visit the mad as if they were in a zoo. If they were not sufficiently excited, with the help of a stick, like wild beasts, they would agitate the madmen until they were in a rage (Lamothe Reference Lamothe1844, 8). In 1889, a Portuguese newspaper described the death of Bemvinda as follows: ‘The monkey woman, whom we have known there for many years, passed away early yesterday morning at Rilhafoles hospital It was a curious specimen, a mix of woman and monkey, with a deformed face (…) it expressed its anger or satisfaction through high-pitched squeals’ (Episódios, O Século 28 May 1889). This dehumanization of people detained in psychiatric institutions also translated into their poor treatment in the institution. The psychiatrist António Maria da Sena, who visited Rilhafoles around the same period as the newspaper article was published, described seeing people naked inside their rooms, with a total lack of hygiene, urinating and defecating all over the room and sleeping in their faeces (Primaz Reference Primaz2020, 78).
This understanding of the dehumanization processes at play in past psychiatric institutions does not diminish the agency of past patients, their real humanity, which never disappeared. Many survived by helping each other, made friends in the institutions, or later organized politically outside them (Michaut Reference Michaut2024). Yet understanding nineteenth- and twentieth-century asylums as participating in the process of constructing non-persons is a crucial step to understanding the necessity to re-centre, honour and re-humanize the experience of past patients and survivors in archaeological narratives about psychiatric institutions.
Emotional landscapes of psychiatric confinement
In one of the interviews with Domingos Oliveira dos Santos, father of one of the authors, he still remembers, 50 years after his internment, how painful his insulin and electroshock treatments were. A decade after the appearance of psycho-pharmaceuticals in the 1960s, Domingos was still, like most of the other patients in Portugal, treated in the old way:
I remember I fainted during the shocks.
– How often were you given this treatment?
– I don’t remember, but it seemed to me that I was getting shocks every day. I remember that during a certain time that seemed eternal, I did not know where I was.
Methodologically, this section adopts a reflexive and interpretive approach to past emotions, drawing on the archaeology of emotion (Tarlow Reference Tarlow2000; Reference Tarlow2012). Rather than claiming direct access to patients’ inner experiences, emotions are approached as historically situated responses inferred through the oral testimony, archival sources and material settings. Given the relative temporal proximity of the case studies (nineteenth to mid-twentieth century) and the absence of opportunities to engage directly with past patients, this approach necessarily involves interpretive risk. These interpretations are therefore presented as cautious, evidence-based propositions rather than substitutions for patients’ own voices.
What may a nineteenth- or early twentieth-century individual have felt on entering a lunatic asylum? Fear? Anger? Loneliness? Hope? What would be the thoughts of a patient in the moment of being tied to the electroshock machine? Inside the walls of psychiatric hospitals, emotions were not just personal experiences but tools of control, resistance and survival. Fear, anger, hope and loneliness shaped the daily realities of those confined within, often defining their very existence. For many, institutionalization was not just a medical process, but a complete severance from the outside world. This exile stripped them of identity, autonomy and, in many cases, even their memory. In the last 25 years, much has been written about emotions in archaeology (Fleisher & Norman Reference Fleisher, Norman, Fleisher and Norman2016; Hamilakis Reference Hamilakis2013; Harris & Sørensen Reference Harris and Sørensen2010; Meskell Reference Meskell2002; Sonik & Steinert Reference Sonik and Steinert2023; Tarlow Reference Tarlow2000; Reference Tarlow2012), although the field still has a long way to go before being fully accepted within the discipline (Santos Reference Santos2024). As Gosden writes (Reference Gosden, DeMarrais, Gosden and Renfrew2004, 39), ‘emotions are materially constituted, and material culture is emotionally constituted’. Archaeology has a lot to offer to our understanding of past emotions, and emotions can be ‘extrapolated not only from artefacts but also architectural structures, landscapes, interviews, (sensorial experiences) and historical sources and documents’ (Santos Reference Santos2024, 93). This final section, therefore, explores the emotional landscapes of psychiatric patients.
Fear was probably the first and last feeling many patients experienced. From the moment they arrived, stripped of their belongings, subjected to cold institutional routines and surrounded by unfamiliar voices, a deep sense of terror settled in. The clang of iron gates closing after the last warden made the round or the sound of the wickets closing after verifying that all the patients were in their cell, the rhythmic footsteps of wardens, the sharp echo of keys turning in locks—all of these sounds became part of the daily fabric of asylum life, reinforcing the helplessness of those inside. It is still possible nowadays to feel what could be the impact of certain sounds on the patients’ emotions when closing the iron gates (Fig. 2), and it is not hard to imagine how anxious some patients may have felt.
There were many triggers causing fear and anxiety. Entering a place that was not your home, the despair of not knowing for how long, the apprehension of waiting for a familiar face that may never come. However, fear was not just about physical control, but also about unpredictability. The accounts of Domingos Oliveira dos Santos, who endured repeated electroshock sessions without understanding why, illustrate how fear was tied to confusion and powerlessness. Many patients lived in a state of permanent anxiety, unsure of whether they were being treated, punished, or forgotten. Newspapers tell us many stories about suicides in Miguel Bombarda. One of them is the story of Georgina Pereira. She entered Rilhafoles on 11 May 1888 while pregnant. Her child was born on 23 July 1888. She asked to be allowed to raise her daughter, but doctors did not let her, and from then on, she fell into a deep sadness. One day, after dinner, she no longer appeared. She hanged herself. It was 5 August 1888 (Episódios, O Dia 1888). We did not find the medical records of Georgina Pereira and therefore cannot tell whether this decision was made out of concerns for the safety of the child; however, this case illustrates the tragic powerlessness patients may have felt, and the sadness and despair that may have resulted from it.
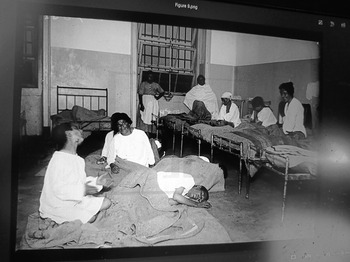
Loneliness was also a strong force Psychiatric hospitals did not just make individuals feel displaced from the places and the people they loved (Santos Reference Santos2024); they also ensured they were forgotten by the outside world. Although isolation is proven to be correlated with loneliness, people will also suffer from loneliness just by the perception that they are alone (Cacioppo et al. Reference Cacioppo, Fowler and Christakis2009). Both situations occurred in asylums. Some patients were alone and isolated in their cells, and others felt alone because, despite being surrounded by people (Figs 9 & 10), they were displaced from all that they knew, like Georgina Pereira (see above) separated from her daughter.
A dormitory for women in Miguel Bombarda hospital in 1926. (Empresa Pública Jornal O Século, Álbuns Gerais n.º 15, doc. PT/TT/EPJS/SF/001-001/0015/1746D in ANTT.)
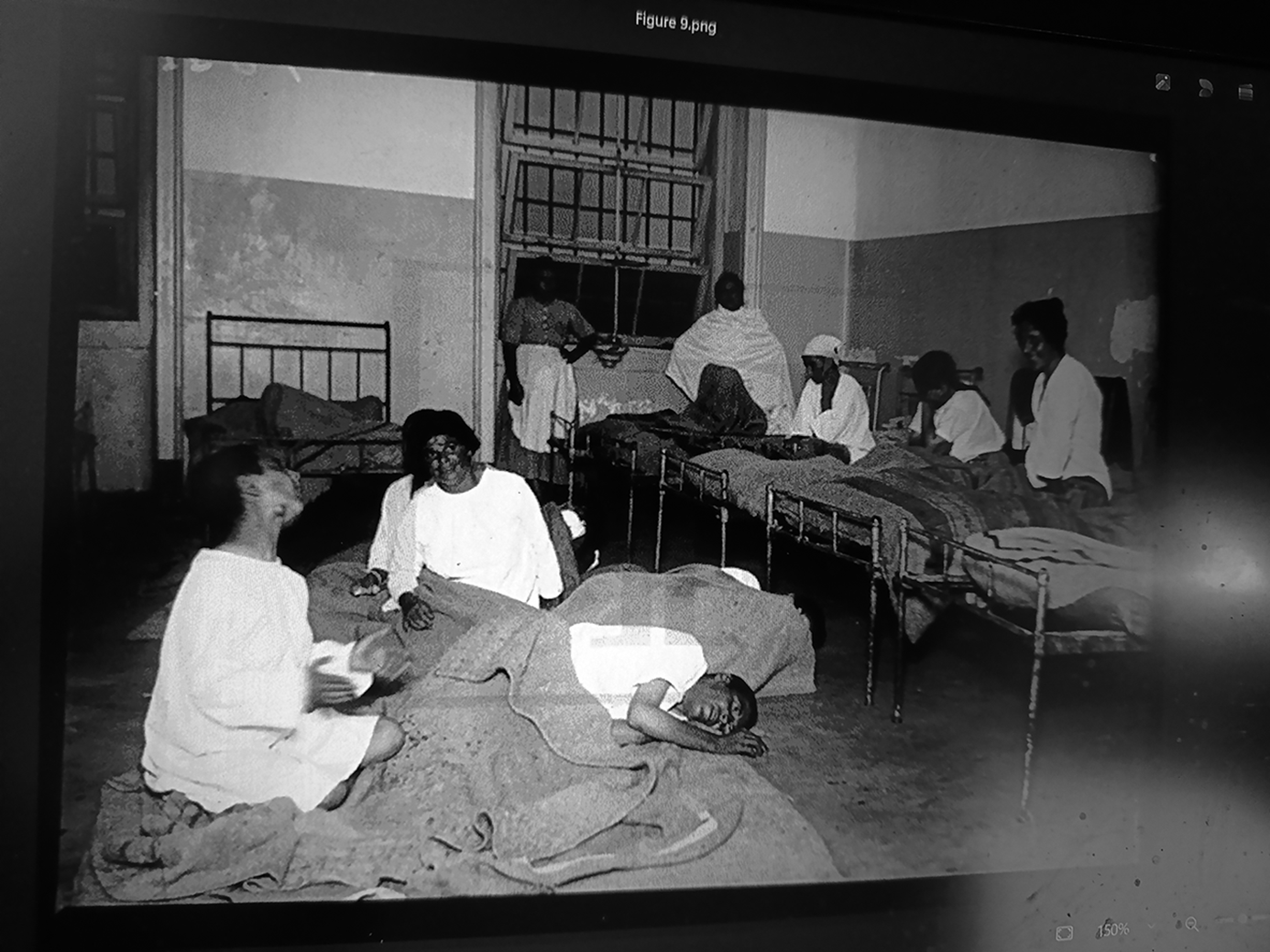
Figure 9 Long description
A black and white photograph of a dormitory for women in Miguel Bombarda hospital in 1926. The room contains several beds lined up against the walls. Some women are sitting on the beds, while others are lying down. The room has a window with bars and a door in the background. The women are dressed in white garments, and the room appears to be quite sparse and utilitarian.
A dormitory for men in Miguel Bombarda hospital in 1926. (Empresa Pública Jornal O Século, Álbuns Gerais n.º 15, doc. PT/TT/EPJS/SF/001-001/0015/1746D in ANTT.)
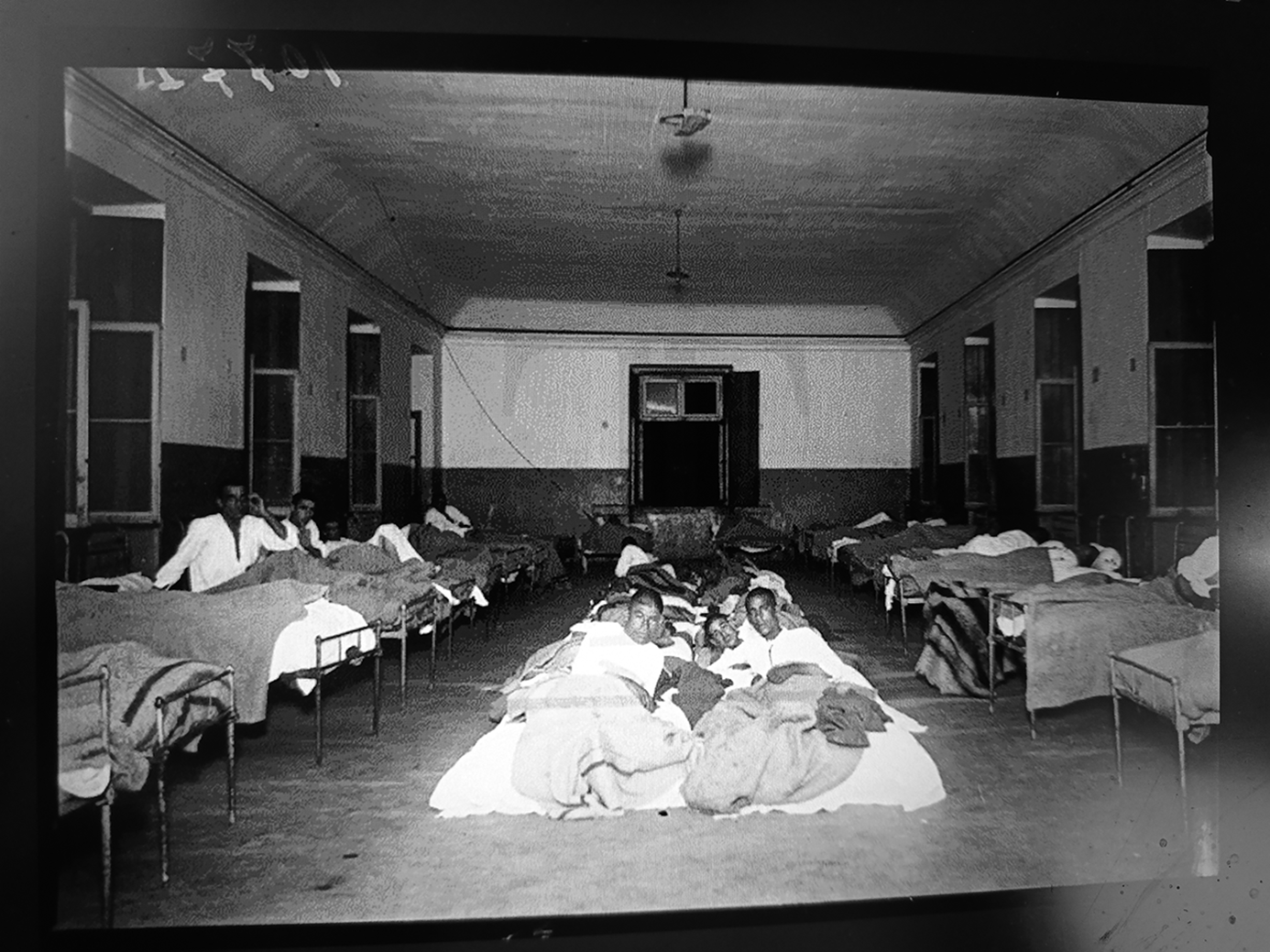
Figure 10 Long description
A dormitory for men in Miguel Bombarda hospital in 1926. The room features multiple beds arranged in rows, with patients lying on them. The beds are covered with blankets and pillows. The room has high ceilings and large windows, allowing natural light to enter. The walls are plain, and the floor appears to be made of a simple material. The overall atmosphere suggests a historical medical setting, reflecting the conditions of the time.
Despite this isolation (physical or emotional), some of the patients remained hopeful. In 1942, Ricardo Vinte-e-um entered Miguel Bombarda. Until his death 41 years later, in 1983, he wrote 50 letters to several people stating that he was not ill, that there was some mistake. On 22 July 1965, a medical report concluded: ‘We do not know why he was arrested.’ However, Ricardo never left Miguel Bombarda. Ricardo’s letters are signs of a desperate hope to be freed, although his letters were never sent by the staff members, contrary to what he believed (Gomes Reference Gomes2020). Hope was also evident in the attempted escapes of the patients of Rilhafoles and Cadillac. Newspapers from the time report numerous escapes (Episódios, Diário de Noticias 22 November 1893; O Século 25 October 1904; 12 November 1904; 4 November 1908; 1 October 1910; 25 September 1920; 12 October 1920). Whether through physical attempts to flee or through imagination and art (Gomes Reference Gomes2020), the need to break free—if only in thought—was often present. The asylum walls could confine bodies, but not always minds.
In the end, the emotions of psychiatric patients were testaments to survival. Fear controlled them, anger gave them strength, loneliness attempted to erase them and hope kept them alive. By retelling their stories—through testimonies, historical records and visual evidence—we ensure they do not remain invisible. The cemetery of the forgotten of Cadillac may have been designed to hide the dead from memory, but the very act of remembering restores dignity to those who lived and suffered within these walls.
Conclusion
We have explored the human experiences within the walls of two historic psychiatric institutions, Cadillac-sur-Garonne in France and Miguel Bombarda hospital in Portugal. Through a people-centred approach, using archival research, spatial analyses, site visits and an oral testimony, we have shown the way these institutions functioned not only as sites of psychiatric care, but also as sanist spaces of control, segregation and emotional struggles. These asylums were often instruments of social exclusion and disappearance for people in precarious situations or experiencing mental health crises, with their experiences being shaped along classist, racist, sexist and ableist lines.
The study has shown how materiality, spatial organization and administrative protocols worked together to enforce isolation and dehumanization. Patients were classified, confined, and, in many cases, reduced to legal and social invisibility (what we have termed ‘non-persons’). Mortality data from both institutions support the argument that these hospitals often functioned as spaces of disappearance rather than spaces of recovery. Patients experienced a wide range of emotions in reaction to this environment, from fear and anger to loneliness and hope, but these emotions were also testimonies to their struggle to survive and their resistance to the structures in which they had found themselves. Emotions are often overlooked in traditional archaeology. However, these emotional landscapes are fundamental to understanding the lives of people in these institutions and to re-centre their humanity and personhood.
The 1960s and ’70s saw the growth of the deinstitutionalization movement, which led to the closure of many psychiatric institutions across the western world. However, the story does not end here. Our study focuses on western European psychiatric institutions in France and Portugal, but future work could expand the geographical and cultural scope of the comparison to include psychiatric institutions in Protestant countries, eastern Europe, or non-European countries. Psychiatric institutions were imported in the nineteenth century by colonial powers into their empires, forming the basis of modern psychiatry in many colonized countries. Comparative views on psychiatric institutions in colonized and colonizer countries would therefore be of chief importance and no doubt reveal the deep historical intricacies of race and psychiatric treatment (Kanani Reference Kanani2011; Metzl Reference Metzl2010; Sadowsky Reference Sadowsky1999). How did histories and differences shape these spaces’ architecture, daily routines and treatment practices? Comparative studies may reveal unexpected nuances or continuities across these contexts and enrich our understanding of the broader historical treatment of people deemed mentally ill. However, only by rehumanizing and recentring the people who inhabited these spaces, who never stopped being human, can we move towards a more just, reflexive and compassionate archaeology that does not shy away from pain, but instead chooses to remember, reckon and give voice to those long silenced.










 Open access
Open access