

Impact Statement
This study provides formative evidence for implementing non-specialist-administered mental health interventions in Senegal, revealing complex cultural dynamics to inform intervention design and implementation. Significant barriers include strong preferences for resolving mental health conditions within the family, various stigmatizing beliefs and attitudes and substantial financial constraints. However, the research also identifies facilitators such as widespread recognition of the value of interpersonal dialog, empathy and community enthusiasm for mental health interventions. The findings demonstrate that successful implementation requires navigating nuanced cultural norms while leveraging existing community strengths in social support. The coexistence of stigma and empathy, alongside both resistance and openness to non-specialist services, highlights a dynamic tension that not only challenges implementation but also presents an opportunity for change. These insights provide critical foundations for designing culturally tailored, sustainable interventions to reduce the mental health treatment gap in Senegal.
Introduction
Mental health conditions pose a significant global challenge. Nine of the 20 leading causes of disability-adjusted life years worldwide are mental, neurological or substance use conditions (Grelotti et al., 2016; Collier and Valentin, Reference Collier and Valentin2018). According to the Mental Health Atlas, over one billion people globally are living with mental health conditions, comprising 17.2% of global years lived with disability (Institute for Health Metrics and Evaluation, 2024; World Health Organization, 2025). Depression and anxiety account for the greatest percentage of the burden. A critical issue is the substantial treatment gap for mental health conditions: in low-income countries, fewer than 10% of affected individuals receive care, compared to over 50% in higher-income nations (World Health Organization, 2025). This disparity is projected to worsen due to growing at-risk populations and expanding drivers of poor mental health, including climate impacts and social inequality (Charlson et al., Reference Charlson, Ali, Augustinavicius, Benmarhnia, Birch, Clayton, Fielding, Jones, Juma, Snider, Ugo, Zeitz, Jayawardana, La Nauze and Massazza2022). Low- and middle-income countries (LMICs) experience severe shortages of mental health specialists, resulting in significant treatment gaps. Low-income countries have a median of 0.1 psychiatrists per 100,000 population, compared to 7 per 100,000 in high-income countries (World Health Organization, 2025). Over 70% of mental health staff in LMICs remain concentrated in urban-based hospitals, further limiting access in rural areas (Shan et al., Reference Shan, Liu, Wang, Yu, Liu, Zheng, He, Li, Li and Yu2025).
To address this workforce shortage, task-sharing models have emerged as optimal solutions for scaling psychological interventions in these settings. A 2017 review demonstrated that psychological treatments – primarily individual, face-to-face sessions with 10 or fewer visits – delivered by non-specialist providers in LMICs are effective in reducing symptoms of depression and anxiety (Singla et al., Reference Singla, Kohrt, Murray, Anand, Chorpita and Patel2017). Cochrane review evidence supports the effectiveness of task-sharing mental health interventions delivered by non-specialists (e.g., lay health workers, primary care professionals, community workers), as these providers enhance accessibility and affordability while leveraging their cultural knowledge, often with minimal training and supervision (van Ginneken et al., Reference van Ginneken, Tharyan, Lewin, Rao, Meera, Pian, Chandrashekar, Patel and van Ginneken2013, Reference van Ginneken, Chin, Lim, Ussif, Singh, Shahmalak, Purgato, Rojas-García, Uphoff, McMullen, Foss, Thapa Pachya, Rashidian, Borghesani, Henschke, L-Y and Lewin2021).
Sub-Saharan African countries such as Senegal consistently experience substantial challenges in mental health service access (Kaminer et al., Reference Kaminer, Owen and Schwartz2018). In 2017, Senegal had prevalence rates of 3.9% for depressive disorders and 2.7% for anxiety, although these estimates may be underestimations (World Health Organization, 2017; Millen et al., Reference Millen, Daniels and Baijnath2024). The country faces systemic challenges including mental health professional shortages, limited policies and pervasive stigma (Abd Rahim et al., Reference Abd Rahim, Abdul Manaf, Juni and Ibrahim2021). Geographic disparities are particularly pronounced: the urban centers of Dakar and Thiès, representing 36% of Senegal’s population, house an overwhelming 93% of specialized mental health personnel (Petit, Reference Petit, Petit, Qureshi, Charbit and Kreager2020), leaving the remaining 64% of the nation with limited access to specialized support.
Implementation gaps compound these challenges despite Senegal approving an official mental health policy in 2006 and again in 2019 (Monteiro et al., Reference Monteiro, Ndiaye, Blanas and Ba2014; WHO, 2020). Most primary care providers lack formal mental health training, official manuals for managing mental health conditions are unavailable in most clinics and no centralized mental health database exists (Monteiro et al., Reference Monteiro, Ndiaye, Blanas and Ba2014). The WHO Mental Health Atlas reveals additional barriers: mental health conditions are not covered by national health insurance or reimbursement schemes, and the integration of mental health into primary care is essentially non-existent (WHO, 2020). While these health system challenges need to be tackled, addressing the burden of mental health conditions in Senegal may also benefit from diversified approaches that leverage existing social program infrastructure (e.g., education, social protection delivery systems) to deliver culturally congruent mental health services using task-sharing strategies.
Understanding contextual determinants – social norms, cultural beliefs and socio-economic factors – is essential for successful intervention adaptation and implementation (Sangraula et al., Reference Sangraula, Kohrt, Ghimire, Shrestha, Luitel, Van’t Hof, Dawson and Jordans2021). Systematic reviews of non-specialist psychological interventions identify common barriers: low acceptability of talking treatments, mental health stigma and competing social problems that demand attention beyond counseling interventions (Chowdhary et al., Reference Chowdhary, Sikander, Atif, Singh, Ahmad, Fuhr, Rahman and Patel2014). Formative qualitative research can identify contextual barriers and facilitators essential for designing culturally appropriate and effective mental health interventions – particularly crucial in LMIC settings such as Senegal where cultural adaptation and community acceptability are fundamental to implementation success (Heim and Kohrt, Reference Heim and Kohrt2019; Ottman et al., Reference Ottman, Wahid, Flynn, Momodu, Fisher, Kieling, Mondelli, Adewuya and Kohrt2022).
Given the complex interplay of cultural, structural and social factors influencing mental health in Senegal, the current study aimed to understand facilitators and barriers to implementing non-specialist mental health interventions that can be integrated into existing social policy programming using open-ended qualitative research. By identifying specific barriers requiring attention and facilitators available for leverage, this study contributes to the growing evidence base for task-sharing strategies in sub-Saharan Africa and offers practical insights for successful non-specialist mental health intervention implementation in Senegal.
Methods
Study design and setting
This formative qualitative study is part of the RElief from STress via SOcial PRotEction (RESTORE) project (Lufumpa et al., Reference Lufumpa, Hilger, Shaw, Rudiman, Moscoe, Experton, Kohrt, Ng and Wahid2026), a broader effort to identify and test appropriate community-based mental health interventions that can be delivered using a task-sharing model with non-specialists, and integrated alongside existing social protection programming implemented by the Senegalese government and supported by the World Bank, the PNBSF (Programme National de Bourses de Sécurité Familiale; National Family Security Grants Program in English). PNBSF provides cash transfers to the poorest households and accompanying social and behavioral change activities to support improvements in human capital development and productive capacity. This approach aligns with recent advances in understanding and responding to the social determinants of mental health, particularly poverty, as a critical component of responding to the mental health burden holistically (Lund, Reference Lund2023). Poverty and mental health interact in a vicious cycle comprising social causation, that is, poverty leading to poor mental health, and social drift, whereby poor mental health makes people more likely to drift into poverty (Jin et al., Reference Jin, Zhu and He2020). Combined delivery of mental health and poverty reduction interventions may help address the necessary preventative and curative aspects within this cycle.
Study setting
The study was conducted across four districts in Senegal – Parcelles Assainies, Sébikotane, Thiès Nord and Chérif Lô – chosen to reflect a mix of urban and rural environments and to ensure accessibility. These regions were selected due to their active participation in social protection programs, making them ideal for piloting community-based mental health interventions. The population targeted included beneficiaries of these programs, many of whom face compounded vulnerabilities due to poverty, climate shocks and displacement.
Participants
In-depth interviews were conducted with 53 participants: social protection program facilitators (n = 11), social protection program beneficiaries (n = 34) and community members (n = 8). Purposive sampling was used to gather diverse perspectives relevant to mental health in Senegal (Patton, Reference Patton2014). Facilitators of the social protection program hold deep insider knowledge of the communities they serve, salient contextual and cultural factors surrounding mental health and experience of social protection program delivery mechanisms. As a future mental health intervention would serve beneficiaries of the social protection program, existing beneficiaries were included to get perspectives about their lives and experiences. Finally, understanding social and cultural norms and attitudes toward mental health within the broader community was considered essential for understanding stigma mechanisms, attitudes toward service use and overall community acceptability. Beneficiaries themselves are also community members, so communal attitudes are drawn from their experience as well.
Sampling and recruitment
Sample size determination was guided by best-practice standards in methodological literature, which endorses 16 interviews to achieve “meaning saturation,” to inform successful identification and richly textured understanding of themes (Hennink et al., Reference Hennink, Kaiser and Marconi2017). We included a larger sample of beneficiaries, as their perspectives were considered to be most essential in informing the feasibility, cultural acceptability and design of a future mental health program.
Beneficiaries were identified from existing social registries containing contact information. Local researchers contacted several randomly selected beneficiaries to obtain permission to visit and explain the study. Facilitators of the social protection program were identified and approached with the assistance of social protection program staff. Community members were recruited through informal community engagement, followed by snowball sampling to identify additional, potentially less-represented community members.
Data collection
Interview guides were informed by Kleinman’s explanatory model of illness (Kleinman, Reference Kleinman1980), and theoretical literature on stigma in LMIC settings (Gronholm et al., Reference Gronholm, Bakolis, Cherian, Davies, Evans-Lacko, Girma, Gurung, Hanlon, Hanna, Henderson, Kohrt, Lempp, Li, Loganathan, Maulik, Ma, Ouali, Romeo, Rüsch, Semrau, Taylor Salisbury, Votruba, Wahid, Zhang and Thornicroft2023). Interviews explored explanatory models of mental illness, symptom recognition, commonly used terminology, community perceptions and beliefs about mental illness, coping strategies, help-seeking behaviors, stigma experiences and perceived barriers and facilitators to implementing non-specialist mental health interventions. Interviews (45 min, approximately) were conducted in the community by a team of one female (MD) and three male (PNSS, CID, MF) Senegalese researchers, with Masters in Sociology (MD, CID), Masters in Sociology and Anthropology (MF) and PhD in Socio-Anthropology (PNSS). Interviews were audio-recorded in the local language, Wolof and transcribed in French. Data transcribed in French were translated into English for analysis. The entire translation process was conducted and verified by trilingual and bilingual (Wolof-French and French-English) research team members.
Data analysis
Data were analyzed using a six-phase process of thematic analysis for psychological research (Braun and Clarke, Reference Braun and Clarke2006). An a priori theory-informed codebook was initially developed and subsequently modified to include inductive codes identified from the data. Data were coded by a team of three researchers: two female coders with graduate degrees in public health (AS and GR), who were mentored by a male professor of global health, an experienced global mental health qualitative researcher (SW). Coder inter-rater reliability was established during an initial coding phase with a Cohen’s kappa of 0.71, representing substantial agreement (McHugh, Reference McHugh2012). Afterward, researchers coded individually with weekly debrief meetings to discuss emerging issues, patterns, etc. A constant comparison approach was followed, systematically comparing newly coded segments with previously coded data to ensure consistent code application across the dataset (Glaser, Reference Glaser and Strauss1968). Dedoose software (Version 9.0.107, 2023) was utilized for coding and data management (Dedoose Version 10.0.59, 2026). After coding, each code was summarized following a standard template, capturing common and deviant narratives and retaining salient quotes.
The study adhered to the Consolidated Criteria for Reporting Qualitative Research (COREQ) guidelines (Tong et al., Reference Tong, Sainsbury and Craig2007; see Supplementary Material).
Results
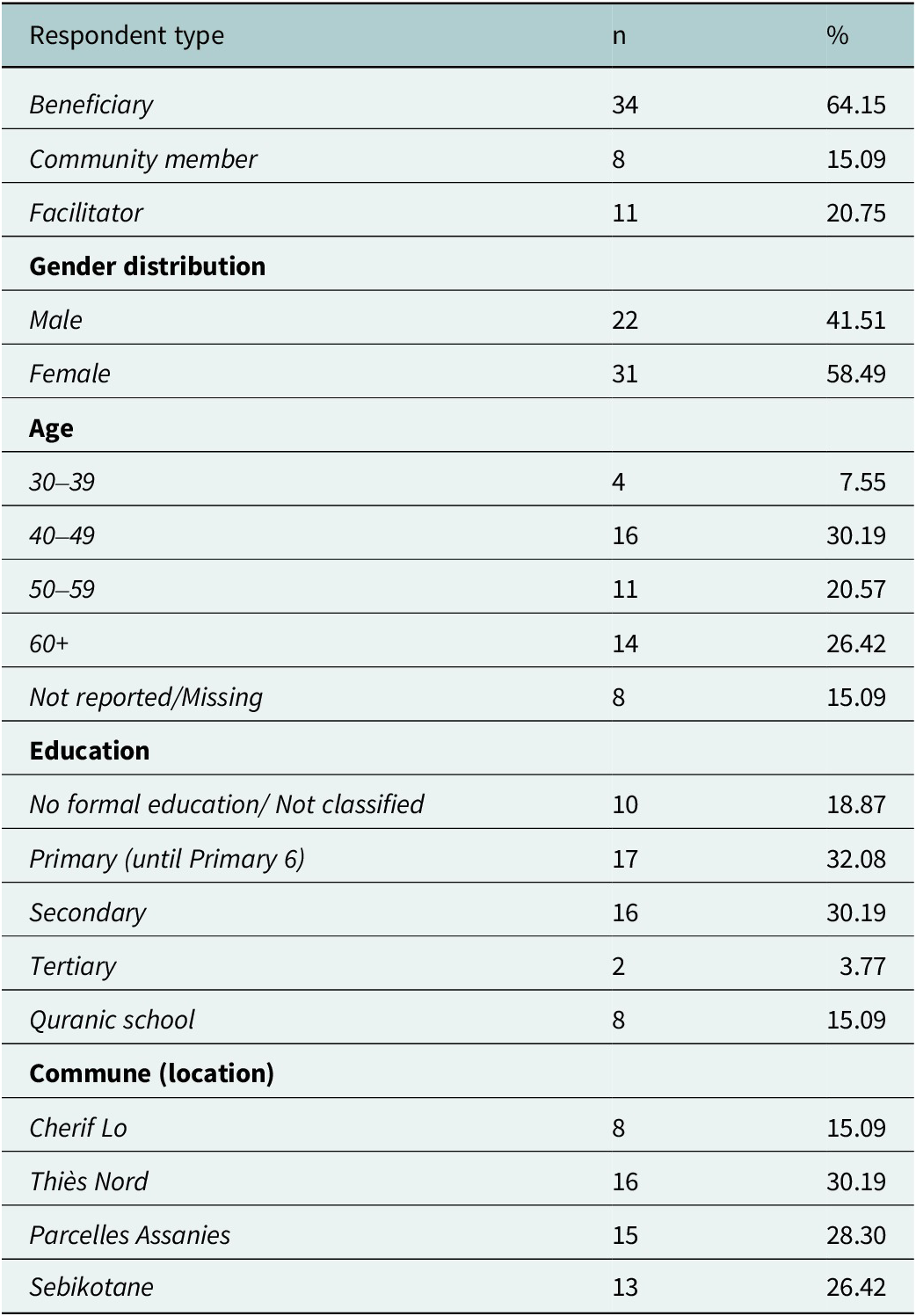
Demographic characteristics of the participants are presented in Table 1. Approximately 60% of respondents were female. Around 63% had at least primary level education, and the majority were aged between 30 and 60 years. The analysis revealed a complex set of factors influencing the potential implementation of non-specialist mental health interventions in Senegal. Four primary themes were constructed: (1) implementation barriers, (2) facilitating factors, (3) help-seeking beliefs and practices and (4) community recommendations.
Respondent characteristics (n = 53)

Table 1. Long description
The table presents characteristics of 53 respondents, organized into five sections. Respondent type: Beneficiary 34 (64.15 percent), Community member 8 (15.09 percent), Facilitator 11 (20.75 percent). Gender: Male 22 (41.51 percent), Female 31 (58.49 percent). Age: 30 to 39 years 4 (7.55 percent), 40 to 49 years 16 (30.19 percent), 50 to 59 years 11 (20.57 percent), 60 plus years 14 (26.42 percent), Not reported or missing 8 (15.09 percent). Education: No formal education or not classified 10 (18.87 percent), Primary (until Primary 6) 17 (32.08 percent), Secondary 16 (30.19 percent), Tertiary 2 (3.77 percent), Quranic school 8 (15.09 percent). Commune: Cherif Lo 8 (15.09 percent), Thiès Nord 16 (30.19 percent), Parcelles Assanies 15 (28.30 percent), Sebikotane 13 (24.53 percent).
Theme-1: Implementation barriers
Sub-Theme 1.1: Concealment of psychological distress, self-stigma and family-related stigma
A primary barrier centered on deeply embedded cultural preferences for keeping mental health concerns within family networks, while avoiding disclosure to outsiders. This pattern reflects both protective family dynamics and pervasive concerns about fear of social repercussions, positioning mental health conditions as sensitive, and oftentimes shameful, secrets that must be concealed.
Participants consistently emphasized that resolving mental health conditions is primarily the family’s responsibility. One older female beneficiary exemplified this preference: “go to a doctor to talk about [having trouble sleeping], no! I prefer to discuss it with my daughter; no one else outside of my family will know anything about me” (IDI 302, Female, 66, Beneficiary).
This sentiment was echoed across participant groups, reflecting profound concerns about confidentiality, social judgment and appropriateness of seeking external help. The fear of community judgment was captured by one respondent who described sharing mental health conditions as “like going out and vilifying myself outside” (IDI 215, Female, over 60, Beneficiary). Another participant expanded on this reluctance:
No, I don’t think so! I stay in my room; I cry and I leave it at that. You can’t open up to anyone; you talk about it to someone who doesn’t resolve it and also vilifies you among others. I don’t want that. (IDI 312, Female, 66, Beneficiary)
Facing stigma was also a concern for those family or community members affiliated with people with mental health conditions. One participant explained avoiding seeking religious counsel for their husband’s mental health difficulties:
No, I haven’t talked to an imam because it’s quite shameful to talk about this, it’s something very ugly and sensitive. At that time, he [her husband] was still living in the house and I couldn’t afford to tell anyone else about it because you never know what might happen. I preferred to talk to the family so that they would pay attention to him and keep an eye on him. I was really ashamed to talk about it to someone outside because it’s really ugly. Even if someone else hears it, it’s not good for the reputation because I was married to him. (IDI 307, Female, 59, Beneficiary)
Family members of those with mental health conditions worried about harming the family’s reputation, reinforcing tendencies toward non-disclosure. As one respondent noted about group support: “I would agree but it won’t be easy for me because I don’t want to go out there and say things and have my kids tell me I shouldn’t have talked about it” (IDI 215, Female, over 60, Beneficiary). This highlights a community norm of actively maintaining privacy and isolating relatives with mental health conditions due to a fear of negative consequences for the family’s reputation.
Alongside these concerns, many participants emphasized self-reliance and the belief that individuals should resolve difficulties independently or within the family. Seeking outside support could be perceived as a sign of personal failure or insufficient religious faith.
Sub-Theme 1.2: Community perceptions of mental health conditions – stigma and social exclusion
The preference for confidential family-centered care was closely intertwined with widespread community perceptions about mental health stigma. Mental health conditions were often seen as shameful and disgraceful, demanding secrecy. Among participants, the majority (60%) described stigmatizing attitudes or reported first-hand experiences of discrimination.
People with mental health conditions were frequently described as lacking self-control, being improper, or socially unacceptable. The label “crazy” (“dof”) or “weakness of mind or faith” was sometimes used, reinforcing negative stereotypes. Stigma was also reported to manifest in exclusionary practices: individuals were prevented from sharing meals, disinvited from homes or subjected to public ridicule. One community member explained a community norm, “It’s the same thing, we isolate them [people with mental health conditions]. For meals, we put them aside with their dish. They do not share meals with other members of the family” (IDI 101, Male, 59, Community member).
Stigma was particularly intense around concerns of physical violence and unpredictable behavior (38%). As one beneficiary described, “There are risks associated with being around a mentally ill person. He may hit you if he’s on his bad days. He can be violent at any time” (IDI 68, Male, 48, Beneficiary). Yet, this fear was not universal; participants distinguished between familiar and unfamiliar individuals, and between those who seemed “harmless” and those perceived as “violent.” One facilitator explained, “For me, there are no risks. She is not a dangerous person. If, on the other hand, it’s someone you don’t know, you should be wary. Sometimes they are people who are very aggressive. So, you have to stay away from them” (IDI 244, Female, over 60, Facilitator). Nevertheless, the prevailing climate of negative perceptions and social exclusion often led people to conceal their struggles, feeding a cycle of self-stigma, isolation and worsening symptoms.
Sub-Theme 1.3: Financial and structural barriers to accessing care
Economic hardship arose as a major obstacle to accessing both traditional and modern healthcare support for mental health conditions, involving both direct and indirect costs. Participants described significant out-of-pocket expenses that rendered services unattainable for many and that treatment related financial strain could lead to discouragement, causing people to give up on treatment. Barriers included transportation expenses, hospitalization fees, diagnostic and medication costs and ongoing treatment needs. These proved especially prohibitive for social protection beneficiaries, among the community’s most vulnerable. One facilitator explained:
The beneficiaries are sensitive targets. They have no means to support themselves. There are some among them who are very vulnerable even though the family grant [cash transfer] is granted every three months. This means that there will be families who will not have the means to care for their mentally ill. So, this is problematic. (IDI 118, Female, 48, Facilitator)
In addition to financial obstacles, structural issues – such as lack of access to free public healthcare – were cited. Some participants described being denied promised services, even with official documentation: “We were given notebooks as Imams to get free health care,” one man reported, but care was still inaccessible (IDI 305, Male, 60, Beneficiary). Beyond these immediate barriers, poverty and financial stress were themselves seen as drivers of mental distress, creating a self-perpetuating cycle.
Theme-2: Facilitating factors
Sub-Theme 2.1: Compassionate and supportive community attitudes
Although stigmatization and discrimination occur, respondents also articulated strong beliefs that discrimination is harmful. They advocated for the use of respectful language and stressed that stigma stems from ignorance that could be reversed with education. Many emphasized the need to treat people with mental health conditions with dignity, compassion and the assurance that recovery was possible (71%). One beneficiary drew a parallel to physical illness: “She has to treat him like a normal person because he’s just a person like you who has a disease. It’s like someone who has breast cancer and has it amputated. He’s just a sick person and should be treated as such” (IDI 309, Female, 54, Beneficiary). Another facilitator elaborated:
Some people manage their patients well, while others don’t. Here, the community takes proper care of its mentally ill people. Those who see him in the streets don’t live there. To me, the stigmatization of the mentally ill is not a good thing. Those who do so have been completely mistaken. We have to take care of these patients and treat them well because they are part of our community. They need to be brought to the treatment centers so that they can find peace and quiet. If the person relapses, the center may hospitalize them to help them recover. Afterwards, we can take him home and take care of him. (IDI 115, Female, 44, Facilitator)
Others stressed a moral imperative: “It’s a bad thing because if it was them or a member of their family, they wouldn’t like it. We must have compassion on them and pray for their healing. You have to cover it when you see them without clothes” (IDI 317, Female, 60, Beneficiary). When asked what the desired attitude should be toward those with mental health conditions, one respondent said, “It’s very simple, the community must know that these people are part of the community, she must not reject or sideline them…we must help them because they are part of us, they are our brothers and sisters” (IDI 196, Male, 44, Beneficiary). Many participants recognized that mental health conditions are not contagious (n = 43%). As one beneficiary stated: “No, this disease [mental health condition] is not communicable. Perhaps there is a risk if he is violent, but I have not yet seen a mental illness that is transmitted” (IDI 133, Male, 63, Beneficiary). A few, however, associated particular symptoms – such as seizures – with possible contagion, reflecting symptom-specific rather than general fear. Despite these compassionate impulses, some attitudes still marked mental health conditions as “other” – emphasizing the need for careful, gentle handling. As a facilitator put it: “We say Nit kou weredi (a person who does not have good mental health), Nit kou xelam matoul (someone who has a mental disability)….It’s not good to call a mentally ill person ‘Dof’ (crazy). One can use ‘kou xelam matoul’ so as not to frustrate the person… This is the way to behave with a mentally ill person” (IDI 183, Female, 40–50, Facilitator).
Sub-Theme 2.2: Intervention acceptability
Participants across all groups expressed enthusiasm for a proposed community-based mental health intervention, seeing it as addressing urgent community needs. When asked if they would be willing to participate in the program, the overwhelming response was affirmation. Motivation came from both a desire to help others and a recognition that current options were inadequate. One participant explained: This is a very important intervention… We must assist them by talking to them constantly. By speaking to them, they will be able to change. We must go to them and share moments with them (IDI 46, Female, 63, Community member). Many respondents saw an intervention as potentially benefiting the entire community, not just individuals in distress: “It’s a big advantage because it’s going to fix the mentally ill, it’s going to fix his family, his neighborhood and it’s even going to fix the whole country because the person can heal and be part of those who move society and the country forward. That’s a real advantage” (IDI 73, Male, 57, Beneficiary).
Theme 3: Help-seeking beliefs and practices – facilitators and barriers
Sub-Theme 3.1: Modern medicine is effective for treating mental health conditions
Attitudes toward professional healthcare for bringing about recovery from mental health conditions were largely positive, demonstrating considerable trust in the formal medical system, especially for more severe symptoms. Some participants consistently advocated for early intervention by doctors and psychologists, seeing it as a more reliable and effective approach than traditional remedies. The importance of medical stabilization – often with medication – was strongly endorsed. As one woman put it: “Of course, these people [those with mental health conditions] need to see doctors and psychologists… when it reaches a certain level it becomes very difficult to manage” (IDI 216, Female, 48, Beneficiary). Still, some participants worried that psychiatric medications change a person’s language and behavior, making patients appear like “robots,” and cause other side effects like weight gain without fully curing the condition.
Sub-Theme 3.2: Traditional and religious healing
Some respondents reported that traditional medicine and spiritual healing play an important role in help-seeking, primarily for problems attributed to supernatural or spiritual causes, such as spirits known as the Djinn (“Rab” or “Rapp”) or curses said to be cast by marabouts (N.B.: holy men who often function as traditional healers). For example, a respondent noted: “It’s stress. In certain families also, we talk about demons (“raap”). It’s culture and we can’t exclude it. There are individuals who are under the influence of the demon and do things that they do not realize” (IDI 320, Male, 33, Facilitator).
When symptoms are attributed to spiritual causes, individuals and families often first seek care from traditional healers, marabouts or religious leaders. Some stated that those afflicted by a “curse” had sometimes engaged in taboo behaviors, such as substance abuse or inappropriate dress. For those who hold these beliefs about the causes of mental health conditions it strongly shapes treatment preferences. Some participants viewed psychological distress as a test from God, believing that faith and prayer could provide healing or resilience:
There was a year when I was really in great difficulty. It is the Lord who tests his disciples. There was a year that I will never forget, my big brother and my little brother both got sick, they had mental illnesses…Until now they are sick, there are things that are of divine order, we must endure them and pray to God so that he takes these trials away from us. (IDI 196, Male, 44, Beneficiary)
Others drew distinctions based on faith, contrasting approaches from the West versus local traditions:
…the example of Westerners that you gave earlier, perhaps they have a weakness of mind and a faith that does not allow them to overcome certain challenges without seeking medical assistance. On the other hand, we don’t need it. If you see and experience certain things, nothing can affect you. If you know who you are, you won’t need medical assistance. (IDI 133, Male, 63, Beneficiary)
At the same time, many respondents pursued pragmatic, multi-modal treatment – combining modern and traditional medicine with family and social support. As one participant highlighted:
It was after she started doing [traditional] treatments and sometimes it works, sometimes it doesn’t. But as we are Africans we are obliged to diversify the treatments. (IDI 194, Male, 58, Beneficiary)
Theme 4: Recommendations for intervention design
Sub-Theme 4.1: Intervention delivery format
Preferences for intervention delivery modalities varied. Many participants favored private home visits (26%), appreciating the privacy, comfort and opportunity for tailored support. However, others valued group approaches (36%), noting that they could encourage learning, shared experience and reduced social isolation, though privacy also remained a top concern for this group.
Some recommended involving community leaders in program implementation, reasoning that they have the best sense of who is in need. As one respondent suggested, “You have to make a selection by getting closer to the community because there may be people who have mental illnesses and who cannot seek treatment. This program would allow them to get treatment” (IDI 29, Female, 63, Beneficiary).
A recurring theme was the need for ongoing, comprehensive support. Respondents advocated strongly for improved access – including more facilities, better affordability and especially consistent follow-up: “The first recommendation is to facilitate health care for mentally ill people. There must be free care for these patients. This is already the start of treatment. Second, we must reintegrate these people into society… We should not treat a person and abandon them. For me, follow-up is very important.” (IDI 118, Female, 48, Facilitator).
Sub-Theme 4.2: Facilitator characteristics and program topics
Respondents outlined both the personal qualities and skills required of program facilitators. Above all, they emphasized compassion, open communication and strong listening skills: facilitators should “listen to people,” “soothe their hearts” and possess a “good heart,” being “open, attentive, understanding” and full of “passion.”
First the person must have a good heart because that is the basis. She must know how to communicate well, be open, attentive, understanding. (IDI 133, Male, 63, Beneficiary)
Confidentiality was a key concern. While familiarity with the community was seen as important, participants worried that local facilitators might compromise privacy or contribute to gossip. Several expressed preferences for facilitators who were from outside the community. One participant noted:
This initiative is good, but we must carefully choose the people who will be trained so that these people are attentive, caring people, who will have the sense of listening to help people get out of their problem, and that it’s not a political structure, but really something to help the population. (IDI 42, Male, 66, Beneficiary)
Psychoeducation and mental health awareness were viewed as essential for the broader community. As one facilitator noted, “the advantages are numerous: we can note the reduction in stress, the strengthening of knowledge among people who had negative ideas about these people. They can know the approach to use to direct these patients to competent structure” (IDI 118, Female, 48, Facilitator). Across responses, priority was placed on helping community members with both practical skills and the confidence to engage in mental health promotion and support, while also tackling stigma through awareness and education.
Discussion
While literature traditionally emphasizes stigma as the central barrier to mental health care in Senegal, our findings suggest a more complex picture of ambivalence, in which discriminatory perceptions coexist with empathy and resistance to stigma, thereby highlighting an opportunity for change. Participants described a pronounced reluctance to share personal information, reflecting broader cultural patterns. This hesitancy is further reinforced by both community – and provider-level stigma, as well as limited knowledge of mental health conditions – factors widely documented as barriers to care (Saxena et al., Reference Saxena, Thornicroft, Knapp and Whiteford2007; Monteiro et al., Reference Monteiro, Ndiaye, Blanas and Ba2014). Importantly, however, participants also expressed strong moral and social obligations to care for family members and support their communities, highlighting a dynamic process in which interest in stigma reduction and engagement with mental health care may be possible despite prevailing negative beliefs, which are addressed in our recommendations below. This mix of supportive and stigmatizing attitudes is consistent with findings from a recent study across seven countries demonstrating that people with mental health conditions and service providers perpetuate stigma while also engaging in support and care (Koschorke et al., Reference Koschorke, Oexle, Ouali, Cherian, Deepika, Mendon, Gurung, Kondratova, Muller, Lanfredi, Lasalvia, Bodrogi, Nyulászi, Tomasini, Chammay, Hana, Zgueb, Nacef, Heim, Aeschlimann, Souraya, Milenova, van Ginneken, Thornicroft and Kohrt2021).
Participants placed significant value on interpersonal dialog, often describing it as a “form of therapy,” highlighting promising entry points for community-based interventions. However, confidentiality remains a substantial concern. Respondents emphasized the importance of privacy in one-on-one sessions to avoid gossip, shame or exposure. Supporting this approach, Bernard et al. (Reference Bernard, Font, Ziadeh, Tine, Diaw, Ndiaye, Samba, Bottai, Jacquesy, Verdeli, Ngom, Dabis, Seydi and de Rekeneire2023) found high completion rates for group interpersonal psychotherapy among people living with HIV in Senegal when confidentiality safeguards and psychoeducation were in place, alleviating participants’ fears. These findings suggest that robust training and supervision of facilitators are necessary to maintain trust and ensure program fidelity.
Participants emphasized that facilitators should possess qualities, such as empathy, active listening, rapport building and strong communication skills – attributes aligned with common factors underpinning effective psychotherapy, namely therapist qualities, the therapeutic alliance and collaborative goal-setting (Wampold, Reference Wampold2015). Endorsement of these essential skills supports the use of tools such as ENACT (Enhancing Assessment of Common Therapeutic factors), a rating scale designed to assess helpers’ competence in delivering core therapeutic skills, specifically intended for training and supervising non-specialists in diverse, resource-limited settings (Saxena et al., Reference Saxena, Thornicroft, Knapp and Whiteford2007; Monteiro et al., Reference Monteiro, Ndiaye, Blanas and Ba2014; Kohrt et al., Reference Kohrt, Ramaiya, Rai, Bhardwaj and Jordans2015). Additionally, the EQUIP project (Ensuring Quality in Psychosocial and Mental Health Care) – a WHO and UNICEF initiative – provides free, standardized resources for competency assessment, training and ongoing supervision (Kohrt et al., Reference Kohrt, Pedersen, Schafer, Carswell, Rupp, Jordans, West, Akellot, Collins, Contreras, Galea, Gebrekristos, Mathai, Metz, Morina, Mwenge, Steen, Willhoite, Ommeren, Underhill, Akhtar, Bryant, Concepcion, Marsi, Elnasseh, Hemmo, Kasujja, Manolova, Maslovskiy, Mbwayo, Moran, Munthali-Mulemba, Mutamba, Mutavi, Raji, Rangel, Sangraula, Sepulveda, Tol, t’Hof and Yurtaev2025). These resources could provide culturally congruent guidance for developing and implementing mental health interventions in Senegal.
Structural barriers were also noted, particularly regarding financial constraints. Participants cited costs associated with transportation, hospitalization, medication and treatment as major challenges to accessing and maintaining continuity of care – challenges that mirror widespread resource limitations documented across sub-Saharan Africa (Petersen et al., Reference Petersen, Hanass Hancock, Bhana and Govender2014; Meffert et al., Reference Meffert, Neylan, McCulloch, Blum, Cohen, Bukusi, Verdeli, Markowitz, Kahn, Bukusi, Thirumurthy, Rota, Rota, Oketch, Opiyo and Ongeri2021). Transportation was consistently recognized as a common impediment for individuals in LMICs seeking mental health support.
Limitations
Several limitations warrant consideration. This study was conducted in a specific geographic and cultural context in Senegal, limiting transferability of findings elsewhere. The sample composition may have introduced selection bias due to overrepresentation of individuals already engaged with the National Family Security Grants Program. Responses may have reflected social desirability, particularly on stigmatizing attitudes. Some recommendations from participants, while important, may not be feasible in practice, namely home visits for mental health care. Additionally, the expressed need for confidentiality cannot be guaranteed, but proper cultural adaptation should minimize confidentiality concerns if stigmatizing aspects are addressed and the mental health status of individuals are not disclosed. The interviews were conducted in Wolof, then subsequently transcribed into French, and then translated into English. Although trilingual and bilingual researchers conducted and verified the process, a degree of nuance in meaning may not have carried over due to this multi-step process.
Recommendations
Our findings hold important implications for designing and adapting mental health interventions in Senegal. Interventions should build on existing cultural emphases on interpersonal dialogue, using local metaphors and communication styles to position talking as therapy. Anti-stigma efforts could highlight participants’ existing belief that “man is man’s medicine,” framing mental health care as a moral and religious obligation, which reflects what-matters-most in that cultural context (Yang et al., Reference Yang, Chen, Sia, Lam, Lam, Ngo, Lee, Kleinman and Good2014; Kohrt et al., Reference Kohrt, Turner, Rai, Bhardwaj, Sikkema, Adelekun, Dhakal, Luitel, Lund, Patel and Jordans2020). This approach can ensure that all interventions materials and procedures are culturally adapted to reflect local, non-stigmatizing idioms of distress and well-being. Importantly, mental health interventions may need to consider financing mechanisms to offset transportation and treatment costs.
Conclusion
This study offers insights into the complex interplay of cultural values, community strengths and structural barriers shaping mental health intervention delivery in Senegal. These findings underscore the importance of tailored, context-sensitive approaches that leverage community strengths while addressing barriers.
Open peer review
To view the open peer review materials for this article, please visit http://doi.org/10.1017/gmh.2026.10217.
Supplementary material
The supplementary material for this article can be found at http://doi.org/10.1017/gmh.2026.10217.
Data availability statement
Code summaries from this qualitative dataset are available upon reasonable request.
Acknowledgments
We acknowledge the support from the Programme National de Bourses de Sécurité Familiale, National Family Security Grants Program in Senegal.
Author contribution
Conceptualization: E.M., B.A.K., A.H., S.S.W.; Data Collection: P.N.S.S., M.D., C.I.D., M.F.; Formal Analysis: A.M.S., G.R., S.B., C.P., S.S.W.; Funding Acquisition: A.H.; Investigation: E.M., L.E., A.H.; Methodology: E.M., L.E., A.H., S.S.W.; Project Administration: N.L., E.M., O.N.; Supervision: E.M., O.N., A.H., S.S.W.; Translation: P.N.S.S., M.D., C.I.D., M.F., L.E.; Writing – Original Draft Preparation: A.M.S., S.S.W.; Writing – Review & Editing: A.M.S., G.R., N.L., E.M., L.E., B.A.K., A.H., S.S.W.
Financial support
This study was funded by the World Bank Group through the Sahel Adaptive Social Protection Program (SASPP) multi-donor trust fund. SASPP is a multi-donor trust fund managed by the World Bank that supports the strengthening of adaptive social protection systems in the Sahel (Burkina Faso, Chad, Mali, Mauritania, Niger and Senegal) to enhance the resilience of poor and vulnerable households and communities to the impacts of climate change. The program is supported by Denmark, France, Germany and the United Kingdom. The pilot received additional support from the Early Learning Partnership multi-donor trust fund at the World Bank. The views expressed in this research do not necessarily represent the views of the World Bank, its Executive Board or World Bank management. The funders had no role in study design, data collection and analysis, decision to publish or preparation of the manuscript.
Competing interests
The authors have no conflict of interest to disclose.
Ethics statement
The study (IRB number 2575) was approved by HML IRB, an international independent review board and ethics review board. All study activities were conducted in compliance with HML IRB guidelines, including the collection of informed consent prior to interviews.



 Open access
Open access