


For most students, entering university is a highly desirable experience, but can also represent a transition from a previously traditional way of life that can be particularly stressful for many individuals. Reference Duffy, Saunders, Malhi, Patten, Cipriani and McNevin1 This experience can be challenging as many students are living away from their homes for the first time, often facing academic challenges, financial difficulties, relationship problems and challenges with career choices. Reference Kronfol, Khalifa, Khoury, Omar, Daouk and deWitt2 Therefore, university students are susceptible to a range of mental health issues that may not exist to the same extent in the general population. Reference Brown3 Eisenberg et al Reference Eisenberg, Hunt, Speer and Zivin4 reported that approximately 32% of university students in the USA reported mental health problems with surveys among these students, indicating high rates of depression, suicidal ideation, anxiety and other psychiatric disorders. Reference Eisenberg, Hunt and Speer5
Although well-recognised efforts are underway to deal with these mental health issues in college students in Western countries (e.g. the USA, Europe), there is less information available from Arabic-speaking countries, where the topic of university students mental health does not seem to be as adequately reported in the literature. Reference Kronfol, Khalifa, Khoury, Omar, Daouk and deWitt2 This includes the United Arab Emirates (UAE), where most studies investigating mental health in university students have restricted their focus to a single disorder, and where the tools used in these studies have not been explicitly designed to cater to student populations, limiting their utility in detecting broader and more generalised mental health issues and how these issues relate to the student’s experience of university life.
The Healthy Minds Study (HMS) Questionnaire is an assessment tool that examines mental health, service awareness and help-seeking behaviour among university students, allowing for substantial detail in this area and is particularly suitable as it is based on the incorporation of academic stressors that typically accompany university life. This allows for a holistic understanding of trends related to mental health among university-aged populations. It has been used to document mental health issues among university students in multiple studies, and since 2007, has involved over 850 000 responses from students at more than 600 colleges and universities in the USA, helping to predict academic outcomes. 6 The tool is updated yearly with more recent versions including additional modules. For example, during the pandemic, a module was included on COVID-19. 6
No previous studies have been published using the HMS Questionnaire in university students in the UAE. Only one previous study has reported on its use in the Middle East in Qatar and Lebanon, Reference Kronfol, Khalifa, Khoury, Omar, Daouk and deWitt2 although it has also been used with university students of Arab/Middle Eastern origin in the USA. Reference Abuelezam, Lipson, Abelson, Awad, Eisenberg and Galea7 Therefore, the objective of our study was to describe the prevalence of mental health symptoms, service awareness, stigma and help-seeking attitudes among medical students at the United Arab Emirates University (UAEU), using the HMS Questionnaire. We hypothesised that UAEU medical students participating in the HMS Questionnaire would report comparable rates in these domains as in other studies. As the data for this study were collected in 2016–2017, before the COVID-19 pandemic and subsequent national mental health initiatives in the UAE, the findings provide a valuable pre-pandemic baseline for understanding mental health, stigma and help-seeking behaviours among medical students.
Method
Study site
The study was conducted at the College of Medicine & Health Sciences (CMHS) at the UAEU, which is located in the city of Al Ain in the Eastern region of the Emirate of Abu Dhabi (the largest of the seven Emirates in the UAE). It was established in 1984 and is the oldest and highest ranked national medical school in the UAE. 8 Its undergraduate medical programme is comprised of 6 years, consisting of premedical (2 years), preclinical (2 years) and clinical (2 years) courses. English is the language of instruction and, upon graduation, a Bachelor of Medicine and Surgery degree is awarded. Graduates must then complete a 1-year internship programme before obtaining their licence to practice as physicians. Reference Abdel Aziz, Okasha, Bhugra, Molodynski, AlKhyeli and AlNeyadi9 The CMHS accepts students from all seven Emirates of the UAE and, at the time the study was conducted, had an undergraduate student population of 533 students that included 123 men (23.1%) and 410 women (76.9%).
Study tool
For our study, we used the 2015–2016 version of the HMS Questionnaire (https://healthymindsnetwork.org/wp-content/uploads/2019/04/HMN-Questionnaire-Modules-and-Survey-Endings-4.13.2016_Final.pdf), which included the original three standard and 12 elective modules. 10 This version consists of up to 468 questions that are contained in three standard modules (demographics, mental health status, mental health service awareness/help-seeking behaviour), and 12 elective modules (substance use, sleep, eating and body image, sexual assault, overall health, knowledge and attitude about mental health, upstander behaviour, campus climate, competition, resilience and coping, persistence and retention and financial stress). 10
For our study, we obtained permission from the original author to use and culturally adapt the HMS Questionnaire for the student population in the UAE. Several adaptations were made from the original version of the tool to suit the cultural and social context of the UAE. Each item of the HMS Questionnaire was surveyed to examine which items were culturally suitable and which items had to be adapted. In the demographics module, questions about sexual orientation, gender identity, ethnicity and military experience were removed. Questions about citizenship were modified. In the mental health status module, questions about violence and sexual assault were removed. In the eating and body image module, the statement ‘I am worried about gaining the freshman fifteen’ was removed. The module on sexual assault was removed in its entirety. In the module on overall health, questions about sexual health and behaviour were removed. In the module on financial stress, questions that mentioned US dollars were modified to Emirati dirhams. In addition, questions that were repeated more than once throughout the tool were removed. For example, questions about sleep were mentioned as part of the module on overall health and so were removed as they had already been asked as part of the sleep module. This was to make the questionnaire more user-friendly and shorten the time needed for completion.
To screen for the presence of symptoms of different psychiatric disorders, the HMS Questionnaire uses previously validated tools, including the Patient Health Questionnaire-9 (PHQ-9), Reference Kroenke, Spitzer and Williams11 for depression; the Generalised Anxiety Disorder-7 (GAD-7), Reference Spitzer, Kroenke, Williams and Löwe12 for anxiety; the Sick, Control, One stone, Fat, Food (SCOFF) questionnaire, Reference Morgan, Reid and Lacey13 for eating disorders; the Alcohol Use Disorders Identification Test (AUDIT), Reference Saunders, Aasland, Babor, de la Fuente and Grant14 for alcohol use; and the Insomnia Severity Index (ISI), Reference Morin, Belleville, Bélanger and Ivers15 for sleep disorders. In our study, these were kept unchanged.
Study design and participants
We conducted a quantitative, cross-sectional survey at the CMHS between September 2016 and June 2017. Participants were included if they were male or female, were medical students from across the six undergraduate years of the CMHS and consented to participate. Data were collected electronically by participants completing an online link, using Google Forms and entering their responses anonymously. A message accompanied the link that explained the topic and benefits of the research, obtained consent and ensured confidentiality and anonymity. The survey included questions of the three standard and 11 adapted elective modules of the HMS Questionnaire 2015–2016, and took between 45 and 60 min to complete. A total of 87 people agreed to participate and completed the entire survey. Based on an eligible undergraduate medical student population of 533 students at the time of data collection, this corresponds to a response rate of 16.3%.
Statistical analysis
Data were analysed using IBM SPSS for Windows, version 29.0 (2022) (IBM Corp., Armonk, NY, USA; from: https://www.ibm.com/products/spss-statistics). The results were tabulated, grouped and statistically analysed using the following tests: mean and standard deviation for quantitative data; and frequency and percentage for non-numerical (qualitative) data.
Results
Demographic characteristics
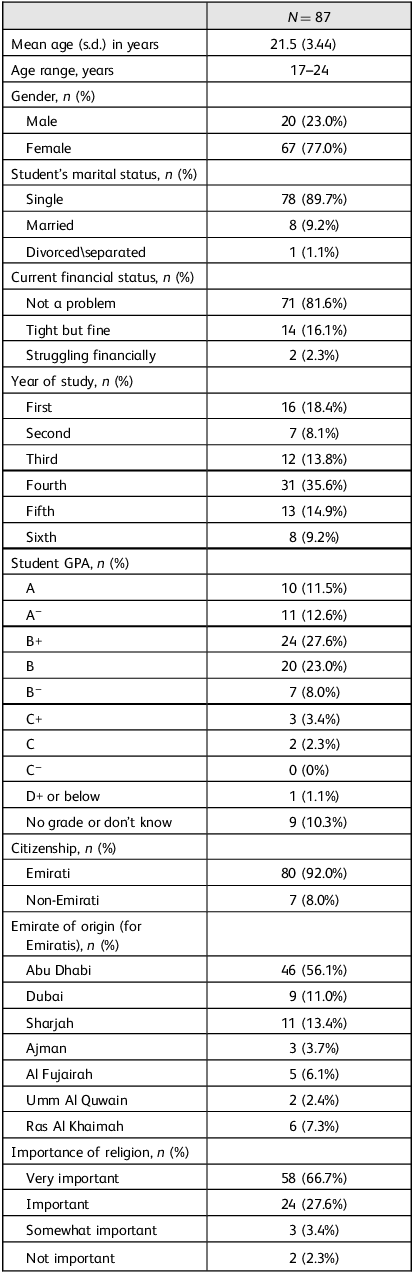
Table 1 summarises the main demographic data of the sample. A total of 87 participants from all six years of the CMHS participated in the study. Of these, 80 (92.0%) were UAE nationals. No students had registered as disabled. As regards accommodation, 84 (96.6%) students lived either in the university hostel or with their parents (n = 42 each).
Main demographic characteristics of participants

GPA, grade point average.
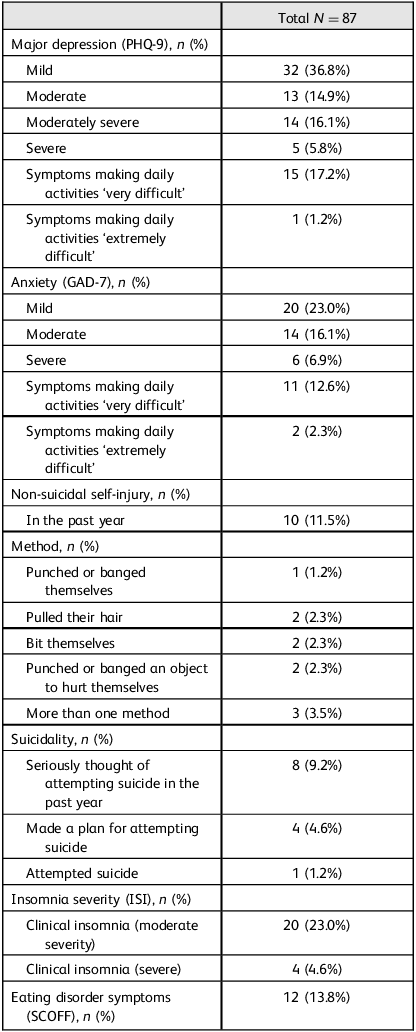
Depression, non-suicidal self-injury and suicidality
A total of 64 students (73.6%) reported at least mild depressive symptoms (PHQ-9 ≥ 5). Of these, 31 students (35.8%) met the threshold for probable major depression (PHQ-9 ≥ 10), comprising the moderate, moderately severe and severe categories (Table 2), of whom 16 (18.4%) reported that their daily functioning (doing their work, taking care of things at home or getting along with other people) was ‘very difficult’ or ‘extremely difficult’ (Table 2). A total of 10 students (11.5%) reported non-suicidal self-injury, eight (9.2%) reported seriously thinking of attempting suicide, four (4.6%) reported making a plan and one (1.2%) reported attempting suicide (Table 2). Twenty-four students (27.6%) reported that depression/suicidality had affected their academic performance in the past year. It is important to note that the HMS Questionnaire item on suicidal ideation asked whether students had ‘seriously thought about attempting suicide’ in the past year, without assessing the duration, persistence or contextual factors surrounding these thoughts. Therefore, the reported prevalence reflects screening-level suicidal ideation and does not differentiate between transient thoughts and more sustained or clinically severe ideation.
Depression, anxiety, non-suicidal self-injury, suicidality, insomnia and eating disorders
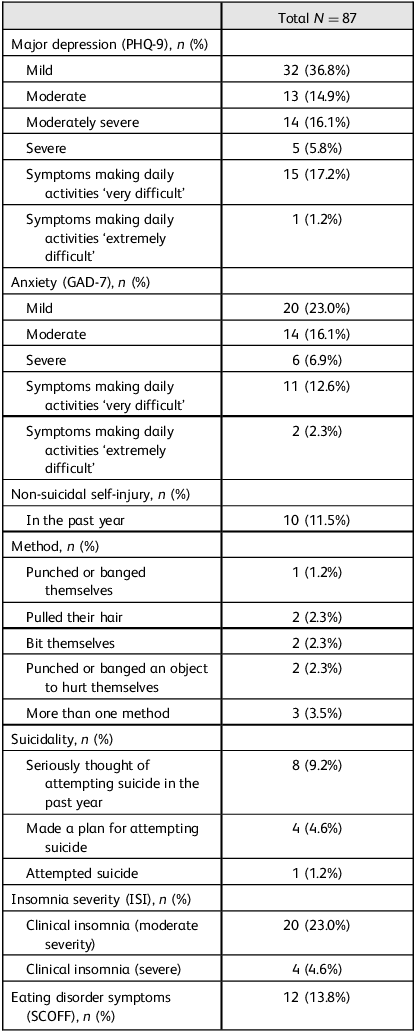
PHQ-9, Patient Health Questionnaire-9; GAD-7, Generalised Anxiety Disorder-7; ISI, Insomnia Severity Insomnia; SCOFF, Sick, Control, One stone, Fat, Food Questionnaire.
Anxiety
A total of 40 students (46.0%) scored positive for anxiety on the GAD-7 (Table 2), of whom 13 (14.9%) reported that their daily functioning (doing their work, taking care of things at home or getting along with other people) was ‘very difficult’ or ‘extremely difficult’ (Table 2). Forty-seven students (54.0%) reported that anxiety/stress had affected their academic performance in the past year.
Substance use, sleep and eating disorders
No students (0%) met the criteria for an alcohol or substance use disorder based on validated screening thresholds. However, five students (5.8%) reported using alcohol or drugs at least occasionally, as a way of coping with stress. A total of 24 students (27.6%) had moderate or severe clinical insomnia on the ISI. A total of 12 students (13.8%) reported two or more symptoms of an eating disorder on the SCOFF, although none of these students had a body mass index of <17.5 kg/m2 (Table 2). Eleven students (12.6%) reported that their eating/body image concerns had affected their academic performance in the past year.
Knowledge and attitudes about mental health and its services
A total of 29 students (33.3%) identified themselves as suffering from a mental illness, with 23 students (26.4%) reporting that they sometimes felt ashamed of having a mental illness and 37 students (42.5%) reporting that they sometimes kept their mental illness a secret. Only 25 students (28.7%) agreed that if they needed professional help for their mental health issue, they would know where to go on campus. The majority of students (n = 73, 83.9%) were not aware of mental health outreach efforts on campus, and only 24 students (27.6%) agreed that there was a good support system on campus for students going through difficult times.
Perceived and personal stigma toward mental health issues
Regarding perceived stigma, 48 students (55.2%) agreed that most people would willingly accept someone who has received mental health treatment as a close friend, whereas 46 students (52.9%) agreed that most people feel that receiving mental health treatment is a sign of personal failure. Sixty students (69.0%) agreed that most people would think less of a person who has received mental health treatment. Regarding personal stigma, 81 students (93.1%) agreed that they would willingly accept someone who has received mental health treatment as a close friend, whereas only ten students (11.5%) agreed that they feel that receiving mental health treatment is a sign of personal failure. Only seven students (8.1%) agreed that they would think less of a person who has received mental health treatment.
Academic experience, perceptions of campus climate and coping with stress
Eighty-one students (93.1%) felt confident that they would be able to finish their degree despite any challenges, with academic challenges (e.g. struggling to pass) being identified as the most likely challenge to prevent students from finishing their degree (n = 35, 40.2%), followed by mental health problems (n = 27, 31.0%) and then lack of motivation or desire (n = 15, 17.2%). Almost three-quarters (n = 64, 73.6%) of students felt that the campus environment had a negative impact on students’ mental and emotional health, with just over half (n = 145, 51.7%) of students reporting that they felt that students’ mental and emotional well-being was a priority at the college, and under half (n = 39, 44.8%) reporting that they felt that the campus climate encouraged free and open discussion about mental and emotional health. Regarding strategies to cope with stress, 46 students (52.8%) reported coping by getting emotional support from family and friends, 76 students (87.3%) reported that they coped with stress by finding comfort in religion and 80 students (92.0%) reported that they coped with stress by praying or meditating. Only five students (5.8%) reported using alcohol or drugs to cope with stress.
Discussion
The aim of this study was to describe the prevalence of mental health symptoms, service awareness, stigma and help-seeking attitudes among medical students at the UAEU.
Mental health issues
A key finding of our study was that 73.6% of students reported at least mild depressive symptoms (PHQ-9 ≥ 5). Importantly, 35.8% met the threshold for probable major depression (PHQ-9 ≥ 10), representing moderate-to-severe symptoms and reflecting the clinically meaningful burden of depression in this population, with 18.4% reporting major difficulties in functioning. This finding was consistent with a previous study in medical students in the UAEU by Abdel Aziz et al, Reference Abdel Aziz, Okasha, Bhugra, Molodynski, AlKhyeli and AlNeyadi9 which reported rates of 74.5% for depressive symptoms measured with the General Health Questionnaire-12 in a sample of 385 participants.
When focusing on clinically significant symptoms, the prevalence of probable major depression in our sample (35.8%) was comparable to the 2023–2024 HMS Questionnaire estimate of 38% for moderate-to-severe depression, 6 which indicates a similar trend in UAE students as USA students. These comparisons should be interpreted with caution, as our data represent a pre-pandemic period (2016–2017), whereas the 2023–2024 HMS Questionnaire findings were collected in a distinctly different global and regional mental health context. Our data was also similar to the trend of Qatari and Lebanese university students who had a combined prevalence of 34.6%, also using the PHQ-9. Reference Kronfol, Khalifa, Khoury, Omar, Daouk and deWitt2 Rates of moderate or severe anxiety symptoms in our study were 23%, which was somewhat lower than both the HMS Questionnaire (2023–2024), which reported a rate of 34%, 6 and Kronfol et al Reference Kronfol, Khalifa, Khoury, Omar, Daouk and deWitt2 in Qatari and Lebanese students, which was 36.1%. In our sample, rates of non-suicidal self-injury, suicidal ideation, suicidal plans and suicidal attempts in the past year were 11.5%, 9.2%, 4.6% and 1.2%, respectively, which were lower than the HMS Questionnaire (2023–2024), which was 26%, 13%, 6% and 2%, respectively. 6 This difference might be explained by a very large proportion (87.3%) reporting finding comfort in religion to cope with difficulties (which in the case of the UAE is Islam, which considers suicide a major sin), Reference Shoib, Armiya’u, Nahidi, Arif and Saeed16 and where religious affiliation has the potential to counter impulsivity and facilitate greater self-control. Reference McCullough, Carter, Pargament, Exline and Jones17 Interpretation of suicidal ideation in this study must be made with caution, as the survey did not assess whether these thoughts were short-lived or persistent, nor did it evaluate contextual factors such as adjustment to the early years of medical training. Clinically, suicidal ideation without a formulated plan may not necessarily indicate imminent risk; however, our tool allowed only for reporting of prevalence rather than assessment of severity. Consequently, findings should be viewed as indicative of the presence of suicidal thoughts rather than a determination of clinical seriousness.
Rates of students scoring positive for eating disorder symptoms on the SCOFF in our sample was 13.8%, which was similar to the HMS Questionnaire (2023–2024), which was 13%. 6 Rates of moderate or severe insomnia on the ISI were 27.6%. Data from the various HMS Questionnaire reports have not commented on rates of insomnia, but a previous study in UAE university students found that almost 22% reported bad quality of sleep, which was somewhat comparable to our study. Reference Ahmed, Shawky and Al Sarraf18
There may be a number of reasons why university students (including those in our sample) are especially vulnerable to mental health problems. First, these students frequently have high personal standards, which may be an advantage in a highly competitive field, but may also lead to excessive preoccupation with academic performance and maladaptive perfectionism. These are significantly associated with baseline neuroticism and can predict hopelessness and depression. Reference Hays, Cheever and Patel19 Also, most university students around the world are between the ages of 17 and 24 years, which is already a high-risk age for developing mental health problems. Reference El-Gabry, Okasha, Shaker, Elserafy, Yehia and Abdel Aziz20 Furthermore, university students experience high levels of distress because of the quantity of their studies, examination stress, the competitive nature of the university environment and the anxiety that may be associated with new experiences. Reference Dyrbye, Thomas and Shanafelt21 These students are also expected to adapt to new social and academic demands, including changes in the methods of teaching between high school and university, dealing with financial difficulties, having limited leisure time, facing accommodation issues, dealing with personal relationships and having to make career choices. Reference Ishak, Nikravesh, Lederer, Perry, Ogunyemi and Bernstein22
Knowledge and attitudes about mental health and its services
Our findings reflect students’ awareness and perceptions of available mental health services rather than actual utilisation rates. Despite the high occurrence of mental health issues in our sample, only 33.3% of students identified themselves as suffering from a mental illness. Only 28.7% of students agreed that if they needed professional help for their mental health issue, they would know where to go on campus. This was markedly lower than the HMS Questionnaire (2023–2024), where 76% of participants agreed that if they needed professional help for their mental health issue, they would know where to go on campus. 6 In addition, 83.9% of students were not aware of mental health outreach efforts on campus, and only 27.6% agreed that there was a good support system on campus for students going through difficult times. One possible reason for these rates might be underlying beliefs and the level of knowledge about mental health conditions among students. Reference Aluh, Okonta and Odili23 Mental health literacy is intricately linked with factors like age, culture and socioeconomic background, Reference Sampaio, Gonçalves and Sequeira24 and enhancing mental health literacy is one of the most important factors in reducing stigma and improving early recognition of mental health conditions. Reference Javaid, Bennett and Goodall25 Although there have been efforts to improve mental health literacy within the Middle East, Reference Elyamani, Naja, Al-Dahshan, Hamoud, Bougmiza and Alkubaisi26 much more is needed to achieve satisfactory levels of health literacy among the population. Reference Pedersen and Paves27 The importance of this cannot be overstated, especially as mental health problems were identified in our study as the second most likely challenge to prevent students from finishing their degree (31%), with nearly three-quarters of students (73.6%) feeling that the campus environment had a negative impact on their mental and emotional health, and only half of students (51.7%) reporting that they felt that their mental and emotional well-being was a priority at the college, and less than half (44.8%) reporting that they felt that the campus climate encouraged free and open discussion about mental and emotional health.
Perceived and personal stigma toward mental health issues
Perceived mental health stigma is defined as how a person believes others would view and treat those who sought out treatment for mental illness. Reference Knaak, Mantler and Szeto28 In our study, we found that 69% of participants agreed that most people would think less of a person who has received mental health treatment, while for personal stigma, only 8.1% agreed that they would think less of a person who has received mental health treatment. Compared to the HMS Questionnaire (2023–2024), this was much higher than the rate of 41% for perceived stigma, but was comparable to the rate of 7% for personal stigma. 6 Both our study and the HMS Questionnaire (2023–2024) highlight the discrepant rates between perceptions of personal and public stigma, with a negative trend toward the perception of public stigma. Furthermore, our study found that 26.4% reported that they sometimes felt ashamed of having a mental illness, with 42.5% reporting that they sometimes kept their mental illness a secret. This reinforces the role of stigma (especially public stigma) as a possible reason for reluctance in seeking help for mental health issues among students. Although efforts have been made to increase the visibility of mental health, mental health stigma remains a major concern. Reference Shalbafan, El Hayek and de Filippis29 The relationship between stigma and reluctance to seek help has been investigated in the general population, Reference Corrigan, Druss and Perlick30 and has also been studied among medical students. Reference Wilkinson31 A study involving medical students in nine medical schools across the UK found that nearly half of the participants experienced significant mental health-related symptoms, and stigma was a major impediment to getting appropriate help. Reference Wilkinson31 Studies from the Middle East also acknowledge stigma as a major factor behind the underreporting of mental health problems and a reluctance to seek professional help. Reference Elyamani, Naja, Al-Dahshan, Hamoud, Bougmiza and Alkubaisi26,Reference Amiri, Voracek, Yousef, Galadari, Yammahi and Sadeghi32
Coping with stress
Regarding strategies to cope with stress, around half of participants (52.8%) reported coping by getting emotional support from family and friends, 87.3% reported that they coped with stress by finding comfort in religion, 92% reported that they coped with stress by praying or meditating and >95% denied use of alcohol or drugs to cope with stress. Previous literature associated with coping mechanisms used by students has shown that alongside religion, peer and family support are commonly utilised as positive coping mechanisms against stress, Reference Lipson, Zhou, Abelson, Heinze, Jirsa and Morigney33 with informal social support identified as a buffer against mental health conditions among students from Middle Eastern backgrounds. Reference Samari, McNall, Lee, Perlstadt and Nawyn34 Although no participants met screening criteria for a substance use disorder, a small proportion of students (5.8%) reported using alcohol or drugs as a coping strategy, indicating occasional or situational use rather than clinically significant misuse. The finding of low drug and alcohol use in Emirati medical students is consistent with the previous study by Abdel Aziz et al, Reference Abdel Aziz, Okasha, Bhugra, Molodynski, AlKhyeli and AlNeyadi9 which reported that <1% of students screened positive on the Cut down drinking, Annoyed by criticism, Guilty feelings, Eye-opener (CAGE) questionnaire for alcohol misuse and ≤1% reported using illicit substances (cannabis, opiates and amphetamines). Previous studies have reported on the role of religious affiliation as a positive protective factor against the use of drugs and alcohol, where religious affiliation has the potential to counter impulsivity and facilitate greater self-control. Reference McCullough, Carter, Pargament, Exline and Jones17 Although the present study did not directly assess protective strategies among students who experienced suicidal ideation but did not engage in self-harm or suicide attempts, the high prevalence of adaptive coping strategies reported, particularly reliance on family support and religious or spiritual practices, may represent potential protective influences. These strategies may help mitigate distress and reduce the likelihood of acting on suicidal thoughts, although this cannot be confirmed within the scope of the current data.
Overall, our findings provide an important historical benchmark for medical student mental health in the UAE before the COVID-19 pandemic, offering a reference point for future post-pandemic research and for evaluating the impact of evolving mental health initiatives.
Limitations
There were several limitations to our study. First, the sample size was relatively small, with a response rate of 16.3%, which may introduce selection bias, as students experiencing greater mental health concerns may have been more likely to participate. However, the gender distribution of the sample (77.0% female) closely mirrored that of the overall undergraduate medical student population at the time (76.9% female), suggesting reasonable demographic representativeness with respect to gender. Additionally, the length of the survey and the sensitive nature of mental health topics may have further limited participation.
Another limitation is that the assessment of suicidality was restricted by the structure of the HMS Questionnaire, which included only a single screening question on suicidal thoughts and did not capture duration, frequency or severity of ideation. The tool also did not distinguish between ideation with or without a plan, nor did it assess whether suicidal thoughts varied across academic years. This limits the ability to interpret the clinical significance of suicidal ideation or identify developmental or contextual patterns.
A further limitation relates to the self-administered nature of the questionnaire. As the survey was completed independently, there remains the possibility that some students may have misinterpreted individual items (as with all self-administered questionnaires). Although investigator contact details were provided for clarification, misunderstandings may still have occurred and could have contributed to under- or overreporting of symptoms.
Another limitation is that the HMS Questionnaire version used in this study did not include questions assessing personal psychiatric history or family history of mental illness. Although students were asked whether they identified themselves as having a mental illness, the absence of detailed lifetime or family mental health information limited our ability to determine whether university-related stressors may have precipitated symptoms or whether findings may reflect pre-existing vulnerabilities. Future studies would benefit from incorporating these variables to better contextualize mental health outcomes.
In addition, the questionnaire assessed mental health symptoms within the past year, but did not distinguish between current and resolved symptoms, nor did it include items exploring factors that may have contributed to symptom improvement or recovery. As a result, we were unable to examine temporal trajectories of mental health difficulties or identify protective strategies that may have facilitated symptom resolution. Future studies incorporating longitudinal designs or retrospective symptom assessment could help identify preventive factors applicable to newer cohorts of medical students.
Furthermore, there may have been a reluctance on the part of students to participate in a mental health survey given the negative perceived public stigma associated with mental health issues. Another limitation was that participants were from one college (the College of Medicine), where academic stress tends to be high, Reference Farrell, Moir, Molodynski and Bhugra35 which may limit the generalisability of our findings with other colleges. Future studies using the HMS Questionnaire should aim to include a broader range of colleges and universities to reflect the experience of the broader UAE university student population.
In conclusion, our study revealed a high prevalence of mental health difficulties in medical students in the UAEU. We also found a reluctance to report and seek help for mental health difficulties, which may be associated with a negative perceived public stigma. These findings highlight the need for targeted preventive interventions, including structured mental health literacy programmes to improve recognition of symptoms, stigma-reduction initiatives addressing negative perceptions of mental health treatment, and improved visibility and accessibility of on-campus mental health services. Early screening initiatives, particularly during transitional phases of medical training, alongside culturally sensitive support strategies that acknowledge the role of family and religious coping, may serve as protective measures to reduce psychological distress and promote help-seeking among medical students.
Data availability
The data that support the findings of this study are available from the corresponding author, K.A.A., on reasonable request.
Acknowledgements
The authors wish to thank Professor Sami Shaban, Professor of Medical Education, CMHS, for his valuable support in providing data related to student numbers used in this study; and Mr Rashed Khalid Alsuwaidi, for his valuable support in designing the electronic version of the survey used in this study.
Author contributions
All authors contributed to the concept and design of the study. K.A.A. and S.O. contributed to coordinating and facilitating investigators’ roles and revising the article. M. Aldobaee, S. Alshehhi, S. Alsuwaidi, M. Alyammahi and S.K. were involved in the acquisition of the data and revising of the article. S.F.J. wrote the first draft of the article and contributed to the statistical analysis. E.S. and F.A.M. revised the write-up and contributed to editing the article. All authors approved the final version of the paper.
Funding
This project received a grant from the Summer Undergraduate Research Experiences (SURE) Program at the College of Medicine and Health Sciences, United Arab Emirates University (grant number: 31M285).
Declaration of interest
K.A.A. is an Editorial Board member for BJPsych International. All other authors having nothing to disclose.
Ethical standards
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2013. All procedures involving human participants were approved by the Social Sciences Research Ethics Committee at the United Arab Emirates University (approval number ERS_2016_4326).

 Open access
Open access
eLetters
No eLetters have been published for this article.