


Introduction
Paranoia, or ideas of social self-reference and persecution, is predominantly perceived to exist within the general population on a continuum ranging from a nonclinical phenomenon through paranoid ideation to persecutory delusions (e.g. Freeman et al., Reference Freeman, Lambe, Waite, Rosebrock, Morrison, Chapman, Dudley, Common, Jones, Kabir, Beckley, Westgate, Rouse and Loe2025). Delusions are highly individual and complex, emerging from interactions among multiple factors, including internal psychological processes as well as social and cultural influences (Ritunnano et al., Reference Ritunnano, Kleinman, Whyte Oshodi, Michail, Nelson, Humpston and Broome2022). Although delusions occur transdiagnostically (Pappa et al., Reference Pappa, Baah, Lynch, Shiel, Blackman, Raihani and Bell2025; Rootes-Murdy et al., Reference Rootes-Murdy, Goldsmith and Turner2022), they are frequent, often persistent, and associated with poorer long-term recovery in schizophrenia spectrum disorders (SSDs) (Feyaerts et al., Reference Feyaerts, Henriksen, Vanheule, Myin-Germeys and Sass2021; Grunfeld et al., Reference Grunfeld, Lemonde, Gold, Paquin, Iyer, Lepage, Joober, Malla and Shah2024; Harrow & Jobe, Reference Harrow and Jobe2010; Rosen et al., Reference Rosen, Harrow, Humpston, Tong, Jobe and Harrow2022). While recovery is possible in SSD, outcomes remain suboptimal for many individuals, highlighting the need for more effective interventions (Molstrom et al., Reference Molstrom, Nordgaard, Urfer-Parnas, Handest, Berge and Henriksen2022).
Pharmacological treatment can be effective in managing positive symptoms in SSD, such as delusions (Leucht et al., Reference Leucht, Siafis, McGrath, McGorry, Howes, Tamminga, Carr, Bighelli, Schneider-Thoma, Priller and Davis2025). However, issues with adverse effects (Huhn et al., Reference Huhn, Nikolakopoulou, Schneider-Thoma, Krause, Samara, Peter, Arndt, Bäckers, Rothe, Cipriani, Davis, Salanti and Leucht2019), discontinuation (Brandt et al., Reference Brandt, Schneider-Thoma, Siafis, Efthimiou, Bermpohl, Loncar, Neumann, Hasan, Heinz, Leucht and Gutwinski2022), nonadherence (Kishimoto et al., Reference Kishimoto, Hagi, Kurokawa, Kane and Correll2021), suboptimal response (O’Donoghue et al., Reference O’Donoghue, Piacenza, Plapp, Siskind and Lyne2024), and residual symptoms (Schennach et al., Reference Schennach, Riedel, Obermeier, Spellmann, Musil, Jäger, Schmauss, Laux, Pfeiffer, Naber, Schmidt, Gaebel, Klosterkötter, Heuser, Maier, Lemke, Rüther, Klingberg, Gastpar and Möller2015) remain. Together with ongoing debate regarding long-term antipsychotic use relative to short-term benefits (Bjornestad et al., Reference Bjornestad, Lavik, Davidson, Hjeltnes, Moltu and Veseth2020; Schlier et al., Reference Schlier, Buck, Müller, Lincoln, Bott and Pillny2023), this highlights the need to expand access to effective nonpharmacological interventions.
Cognitive behavioral therapy for psychosis (CBTp) is a recommended first-line psychological treatment, yet rates of receipt remain low (Burgess-Barr et al., Reference Burgess-Barr, Nicholas, Venus, Singh, Nethercott, Taylor and Jacobsen2023). Meta-analytic evidence from an umbrella review suggests small-to-moderate effects of CBTp on delusions (Berendsen et al., Reference Berendsen, Berendse, van der Torren, Vermeulen and de Haan2024). While the effectiveness seems to have improved over time (Sitko et al., Reference Sitko, Bewick, Owens and Masterson2020), CBTp neither consistently outperforms other psychological treatments (Varese et al., Reference Varese, Sudell, Morrison, Longden and Tudur Smith2025), nor demonstrates sustained treatment effects (Berendsen et al., Reference Berendsen, Berendse, van der Torren, Vermeulen and de Haan2024; Mehl et al., Reference Mehl, Werner and Lincoln2015). CBTp targeting specific symptoms (e.g. delusions) may be more effective than generic approaches addressing psychosis broadly (Freeman et al., Reference Freeman, Taylor, Molodynski and Waite2019; Lincoln & Peters, Reference Lincoln and Peters2019). Emerging evidence, such as from the Feeling Safe Programme (Freeman et al., Reference Freeman, Emsley, Diamond, Collett, Bold, Chadwick, Isham, Bird, Edwards, Kingdon, Fitzpatrick, Kabir, Waite, Carr, Causier, Černis, Kirkham, Lambe, Lister and Twivy2021), supports its benefits in treating persecutory delusions. These approaches are grounded in interventionist causal models (Kendler & Campbell, Reference Kendler and Campbell2009), aiming to identify and modify mechanisms that maintain distressing symptoms (Freeman Reference Freeman2024a, Reference Freeman2024b).
Virtual reality-assisted CBTp (VR-CBTp) enables more targeted interventions for paranoia (Bird et al., Reference Bird, O’Neill and Riches2024), with promising results (Freeman et al., Reference Freeman2016; Pot-Kolder et al., Reference Pot-Kolder, Geraets, Veling, van Beilen, Staring, Gijsman, Delespaul and van der Gaag2018). Compared to traditional therapies, VR-CBTp has the potential to be more engaging, with immersive VR eliciting cognitions, emotions, and behaviors in a safe environment, potentially increasing motivation and treatment adherence (Bell et al., Reference Bell, Pot-Kolder, Rizzo, Rus-Calafell, Cardi, Cella, Ward, Riches, Reinoso, Thompson, Alvarez-Jimenez and Valmaggia2024). In the recent FaceYourFears trial, 10 sessions of CBTp or VR-CBTp targeting paranoia in individuals with SSD produced large within-group reductions in paranoia (Jeppesen et al., Reference Jeppesen, Vernal, Due, Mariegaard, Pinkham, Austin, Vos, Christensen, Hansen, Smith, Hjorthøi, Veling, Nordentoft and Glenthøj2025). However, no between-group superiority was found, mirroring results from a similar trial (van der Stouwe et al., Reference van der Stouwe, Geraets, Berkhof, Hidding, van Amstel, van den Berg, van Grunsven, de Jager, Kooijmans, Sageot, Staring, Vos, Zandee and Veling2025). Moreover, efficacy remains uncertain in the absence of an inactive control group. Combined with the additional implementation barriers of digital interventions like VR (Bin et al., Reference Bin, Alrashdi, Whitehead, Riches and Drini2025), identifying treatment effect modifiers is crucial to clarify who benefits and assess VR’s added value.
In CBTp, a systematic review suggested that female gender, older age, greater clinical insight, shorter illness duration, and higher educational attainment were associated with better outcomes (O’Keeffe et al., Reference O’Keeffe, Conway and McGuire2017). In contrast, higher baseline negative symptoms have been associated with poorer treatment response (e.g. Lincoln et al., Reference Lincoln, Rief, Westermann, Ziegler, Kesting, Heibach and Mehl2014; Thomas et al., Reference Thomas, Rossell, Farhall, Shawyer and Castle2011), with avolition identified as a key factor (Allott et al., Reference Allott, Alvarez-Jimenez, Killackey, Bendall, McGorry and Jackson2011; Strauss et al., Reference Strauss, Bartolomeo and Harvey2021). Moreover, greater delusion severity may interfere with treatment response (Brabban et al., Reference Brabban, Tai and Turkington2009), although findings remain mixed (Lincoln et al., Reference Lincoln, Rief, Westermann, Ziegler, Kesting, Heibach and Mehl2014). Especially, high conviction may delay therapy response and reduce the likelihood of a positive response (Jenner et al., Reference Jenner, Payne, Waite, Beckwith, Diamond, Isham, Collett, Emsley and Freeman2024). Relatedly, cognitive biases have been linked to delusions (De Rossi & Georgiades, Reference De Rossi and Georgiades2022) and may maintain paranoia by limiting consideration of alternative interpretations (Freeman, Reference Freeman2016; Mehl et al., Reference Mehl, Landsberg, Schmidt, Cabanis, Bechdolf, Herrlich, Loos-Jankowiak, Kircher, Kiszkenow, Klingberg, Kommescher, Moritz, Muller, Sartory, Wiedemann, Wittorf, Wölwer and Wagner2014). However, meta-analytic evidence indicates no consistent effect of treatment modification by demographic or clinical variables (Turner et al., Reference Turner, Reijnders, van der Gaag, Karyotaki, Valmaggia, Moritz, Lecomte, Turkington, Penadés, Elkis, Cather, Shawyer, O’Connor, Li, de Paiva Barretto and Cuijpers2020; Varese et al., Reference Varese, Sudell, Morrison, Longden and Tudur Smith2025). Most studies evaluated generic CBTp rather than symptom-specific approaches, and few examined specific symptoms – such as paranoia – as variables associated with outcomes, limiting understanding of factors influencing targeted CBTp response (Thomas, Reference Thomas2015). In VR interventions, higher baseline safety behaviors have been associated with improved outcomes in VR-CBTp for paranoia (Berkhof et al., Reference Berkhof, van der Stouwe, Pot-Kolder, van der Gaag, Veling and Geraets2024) and in automated VR therapy for agoraphobia (Freeman et al., Reference Freeman, Lambe, Kabir, Petit, Rosebrock, Yu, Dudley, Chapman, Morrison, O’Regan, Aynsworth, Jones, Murphy, Powling, Galal, Grabey, Rovira, Martin, Hollis and West2022). These findings warrant replication and further investigation, ideally through direct comparisons between CBTp and VR-CBTp.
Identifying treatment effect modifiers can inform the selection of interventions based on individual symptom profiles (Hofmann & Hayes, Reference Hofmann and Hayes2019). An important next step is therefore to determine whether CBTp and VR-CBTp share similar modifiers of paranoia outcomes or differ in meaningful ways. To guide this investigation, we propose three categories of baseline variables, namely those (1) previously examined in CBTp-studies (O’Keeffe et al., Reference O’Keeffe, Conway and McGuire2017; Turner et al., Reference Turner, Reijnders, van der Gaag, Karyotaki, Valmaggia, Moritz, Lecomte, Turkington, Penadés, Elkis, Cather, Shawyer, O’Connor, Li, de Paiva Barretto and Cuijpers2020; Varese et al., Reference Varese, Sudell, Morrison, Longden and Tudur Smith2025); (2) involved in the formation and maintenance of paranoia (Freeman, Reference Freeman2016; Freeman & Loe, Reference Freeman and Loe2023; Freeman et al., Reference Freeman, Emsley, Diamond, Collett, Bold, Chadwick, Isham, Bird, Edwards, Kingdon, Fitzpatrick, Kabir, Waite, Carr, Causier, Černis, Kirkham, Lambe, Lister and Twivy2021; Valmaggia, Day, & Rus-Calafell, Reference Valmaggia, Day and Rus-Calafell2016); and (3) clinically or theoretically relevant explored more tentatively, reflecting VR-CBTp’s early stage (Bell et al., Reference Bell, Pot-Kolder, Rizzo, Rus-Calafell, Cardi, Cella, Ward, Riches, Reinoso, Thompson, Alvarez-Jimenez and Valmaggia2024), particularly in domains where VR shows promise (Freeman et al., Reference Freeman, Freeman, Ahmed, Haynes, Beckwith, Rovira, Miguel, Ward, Bousfield, Riffiod, Kabir, Waite and Rosebrock2024, Reference Freeman, Lambe, Kabir, Petit, Rosebrock, Yu, Dudley, Chapman, Morrison, O’Regan, Aynsworth, Jones, Murphy, Powling, Galal, Grabey, Rovira, Martin, Hollis and West2022; Jongeneel et al., Reference Jongeneel, Pot-Kolder, Counotte, van der Gaag and Veling2018; Novo et al., Reference Novo, Fonsêca, Barroso, Guimarães, Louro, Fernandes, Lopes and Leitão2021; Pot-Kolder et al., Reference Pot-Kolder, Veling, Counotte and Van Der Gaag2018; Schröder et al., Reference Schröder, Wrona, Müller, Heinemann, Fischer and Dockweiler2023; Schroeder et al., Reference Schroeder, Bogie, Rahman, Thérond, Matheson and Guimond2022; Veling et al., Reference Veling, Counotte, Pot-Kolder, Van Os and Van Der Gaag2016).
Accordingly, this exploratory study investigated whether baseline characteristics were associated with post-treatment paranoia and whether they interacted with treatment allocation among individuals with SSD following 10 sessions of CBTp or VR-CBTp in the FaceYourFears trial.
Methods
Study design and source of data
This exploratory moderator study used baseline data collected before randomization and outcome data at treatment cessation (3 months) from FaceYourFears, a two-site, assessor-masked, randomized, parallel-group superiority trial comparing VR-CBTp (n = 126) with CBTp (n = 128) for paranoia in SSD. Elsewhere, more details are provided on FaceYourFears’ methodology (Jeppesen et al., Reference Jeppesen, Due, Mariegaard, Pinkham, Vos, Veling, Nordentoft and Glenthøj2022), outcomes (Jeppesen et al., Reference Jeppesen, Vernal, Due, Mariegaard, Pinkham, Austin, Vos, Christensen, Hansen, Smith, Hjorthøi, Veling, Nordentoft and Glenthøj2025), and secondary analyses of mechanisms of change (Jeppesen et al., Reference Jeppesen, Vernal, Christensen, Pinkham, Veling, Hidding, Jensen, Austin, Nordentoft and Glenthøjn.d.).
Participants
The target population was individuals diagnosed with SSD experiencing paranoia. Inclusion criteria were age ≥ 18 years, SSD diagnosis (ICD-10, F20–29), ability to provide informed consent, and scoring ≥40 on the Green Paranoid Thought Scale (GPTS) (Green et al., Reference Green, Freeman, Kuipers, Bebbington, Fowler, Dunn and Garety2008). Exclusion criteria were organic brain disease, IQ ≤ 70, inability to tolerate assessment, or insufficient Danish proficiency (Jeppesen et al., Reference Jeppesen, Due, Mariegaard, Pinkham, Vos, Veling, Nordentoft and Glenthøj2022). The trial was conducted across two Danish sites. Enrolment started March 26, 2021; follow-up ended August 10, 2024.
Sample size
The sample comprised all 270 randomized participants in the FaceYourFears trial. Because the trial was powered for its primary hypotheses rather than the secondary analyses reported here, and because power calculations are hypothesis- and dataset-specific, post hoc power calculations were not conducted.
Interventions
The FaceYourFears trial adapted therapy manuals from previous research (Pot-Kolder et al., Reference Pot-Kolder, Geraets, Veling, van Beilen, Staring, Gijsman, Delespaul and van der Gaag2018), delivering 10 individual sessions focused on paranoia. Trained psychologists provided both treatments (Jeppesen et al., Reference Jeppesen, Vernal, Due, Mariegaard, Pinkham, Austin, Vos, Christensen, Hansen, Smith, Hjorthøi, Veling, Nordentoft and Glenthøj2025).
CBTp targeted paranoia using a cognitive model emphasizing aberrant salience, reasoning biases, and consolidation processes. Sessions included cognitive worksheets, psychoeducation, cognitive restructuring, core belief work, and self-worth enhancement, with guided homework and in vivo experiments where feasible.
VR-CBTp integrated CBTp principles with in-session exposure and behavioral experiments in immersive VR using CleVR Social Worlds. Participants confronted paranoia triggers in realistic, customizable virtual settings, enabling therapists to intervene in real time during ‘hot’ cognitions.
Candidate baseline variables
In the current study, all candidate baseline variables, whether previously tested in CBTp or newly examined in VR-CBTp, were theoretical in nature, grounded in cognitive-behavioral models of psychosis. Consistent with the conceptual framework outlined in the Introduction, variables were organized into three overarching categories: (1) established CBTp moderators, (2) variables related to mechanisms underlying paranoia, and (3) exploratory VR-CBTp-relevant variables. For conceptual coherence, the variables were organized hierarchically as follows: Established CBTp variables, theoretically relevant but untested VR variables, trauma-related variables, and supplementary psychosocial factors.
The established CBTp variables included age, gender, positive symptoms, negative symptoms, anxiety, and depression (Varese et al., Reference Varese, Sudell, Morrison, Longden and Tudur Smith2025). These were supplemented by education, diagnosis, paranoid ideation, social anxiety, safety behavior, core beliefs, and social functioning, which had been examined in a VR-CBTp versus TAU moderator study (Berkhof et al., Reference Berkhof, van der Stouwe, Pot-Kolder, van der Gaag, Veling and Geraets2024). Variables tested in CBTp but not yet in VR-CBTp were added, including avolition and anhedonia (Allott et al., Reference Allott, Alvarez-Jimenez, Killackey, Bendall, McGorry and Jackson2011), cognitive biases (Lincoln et al., Reference Lincoln, Rief, Westermann, Ziegler, Kesting, Heibach and Mehl2014), and symptom severity (Allott et al., Reference Allott, Alvarez-Jimenez, Killackey, Bendall, McGorry and Jackson2011; Lincoln et al., Reference Lincoln, Rief, Westermann, Ziegler, Kesting, Heibach and Mehl2014; Naeem et al., Reference Naeem, Kingdon and Turkington2008; Tarrier et al., Reference Tarrier, Beckett, Harwood, Baker, Yusupoff and Ugarteburu1993, Reference Tarrier, Yusupoff, Kinney, McCarthy, Gledhill, Haddock and Morris1998) conceptualized as delusion severity. Interpersonal trauma was included due to its established association with paranoia (Frost et al., Reference Frost, Collier and Hardy2024; Grady et al., Reference Grady, Twomey, Cullen and Gaynor2024; Jorovat et al., Reference Jorovat, Twumasi, Mechelli and Georgiades2025), and prior studies examining the moderation of post-traumatic stress symptoms (de Haan et al., Reference de Haan, Meiser-Stedman, Landolt, Kuhn, Black, Klaus, Patel, Fisher, Haag, Ukoumunne, Jones, Flaiyah, Catani, Dawson, Bryant, de Roos, Ertl, Foa, Ford and Dalgleish2024) and childhood trauma (Spidel et al., Reference Spidel, Daigneault, Kealy and Lecomte2019) on therapy outcomes. Finally, given VR-CBTp’s early stage, supplementary analyses included psychosocial functioning (Schroeder et al., Reference Schroeder, Bogie, Rahman, Thérond, Matheson and Guimond2022), self-esteem (Jongeneel et al., Reference Jongeneel, Pot-Kolder, Counotte, van der Gaag and Veling2018), personality traits (Katifori et al., Reference Katifori, Lougiakis and Roussou2022), social cognition (Pinkham et al., Reference Pinkham, Harvey and Penn2018), basic symptoms (Schultze-Lutter, Reference Schultze-Lutter2009), and additional demographics to inform the field and future research (Supplementary Appendix A).
Measures
Paranoia ideation was assessed using the Revised Green Paranoid Thoughts Scale (R-GPTS) (Freeman et al., Reference Freeman, Loe, Kingdon, Startup, Molodynski, Rosebrock, Brown, Sheaves, Waite and Bird2021) as a candidate baseline variable, due to its strong psychometric properties, while the original GPTS (Green et al., Reference Green, Freeman, Kuipers, Bebbington, Fowler, Dunn and Garety2008) was retained as the outcome variable to align with the primary study (Jeppesen et al., Reference Jeppesen, Vernal, Due, Mariegaard, Pinkham, Austin, Vos, Christensen, Hansen, Smith, Hjorthøi, Veling, Nordentoft and Glenthøj2025).
Safety behavior was assessed by the Safety Behaviour Questionnaire (Freeman et al., Reference Freeman, Garety and Kuipers2001) with the addition of close-ended questions for in-situation behaviors in FaceYourFears (Jeppesen et al., Reference Jeppesen, Vernal, Due, Mariegaard, Pinkham, Austin, Vos, Christensen, Hansen, Smith, Hjorthøi, Veling, Nordentoft and Glenthøj2025).
Delusion severity was assessed by the Scale for the Assessment of Positive Symptoms (SAPS; Andreasen, Reference Andreasen1984) subscale global delusion severity.
Negative symptoms were assessed by the Brief Negative Symptom Scale’s (BNSS; Kirkpatrick et al., Reference Kirkpatrick, Strauss, Nguyen, Fischer, Daniel, Cienfuegos and Marder2011; Strauss et al., Reference Strauss, Hong, Gold, Buchanan, McMahon, Keller, Fischer, Catalano, Culbreth, Carpenter and Kirkpatrick2012) total score, and the subscales anhedonia and avolition.
Social anxiety was assessed by the Social Interaction Anxiety Scale (SIAS; Mattick & Clarke, Reference Mattick and Clarke1998).
Depression was assessed by the Calgary Depression Scale for Schizophrenia (CDS; Addington et al., Reference Addington, Addington and Maticka-tyndale1993).
Cognitive biases were assessed by the Davos Assessment of Cognitive Biases Scale (DACOBS; Van der Gaag et al., Reference Van der Gaag, Schütz, ten Napel, Landa, Delespaul, Bak, Tschacher and De Hert2013).
Core beliefs were assessed by the Brief Core Schema Scale (BCSS; Fowler et al., Reference Fowler, Freeman, Smith, Kuipers, Bebbington, Bashforth, Coker, Hodgekins, Gracie, Dunn and Garety2006).
Level of function was assessed by the Personal and Social Performance scale (PSP; Morosini et al., Reference Morosini, Magliano, Brambilla, Ugolini and Pioli2000).
Interpersonal trauma was assessed by the Trauma and Life Events Checklist (TALE; Carr et al., Reference Carr, Hardy and Fornells-Ambrojo2018) using a composite score of interpersonal trauma types.
Education was self-reported and categorized according to the highest level achieved: primary education, vocational education, secondary/high school education, post-secondary education, or other.
Statistical analyses
Using Stata 18.0, separate general linear models (continuous variables) and logistic regression models (categorical variables) examined whether baseline demographic and clinical variables (Table 1) were associated with paranoia reduction at treatment cessation (GPTS total score at 3 months) in VR-CBTp and/or CBTp. Following the intention-to-treat principle, all randomized participants were included in the analyses.
Baseline participant demographics and clinical characteristics

Note: * = unless otherwise specified. Measures: BCSS: Brief Core Schema Scale; BNSS: Brief Negative Symptom Scale; CDSS: Calgary Depression Scale for Schizophrenia; DACOBS: Davos Assessment of Cognitive Biases Scale; PSP: Personal and Social Performance Scale; R-GPTS: Revised Green Paranoid Thoughts Scale; Safety Behavior Questionnaire; SAPS: Scale for the Assessment of Positive Symptoms; SIAS: Social Interaction Anxiety Scale; TALE: Trauma and Life Events Checklist.
Analysis of covariance (ANCOVA), adjusting for baseline scores as a covariate, was used to estimate treatment effects at post-treatment. ANCOVA focusing on the end-point score was selected in accordance with recommendations for RCTs (Clifton & Clifton, Reference Clifton and Clifton2019; Fu et al., Reference Fu, Haley and Holmer2015; Van Breukelen, Reference Van Breukelen2006), as it accounts for baseline group differences and avoids potential bias associated with change scores, including regression to the mean. Each candidate’s baseline variable was analyzed in a separate model. The significance level was set to p < 0.05 with a two-sided 95% confidence interval (CI). Post hoc analyses were conducted to examine subscale scores for measures that showed statistically significant overall effects.
Missing data were addressed as in the primary study (Jeppesen et al., Reference Jeppesen, Vernal, Due, Mariegaard, Pinkham, Austin, Vos, Christensen, Hansen, Smith, Hjorthøi, Veling, Nordentoft and Glenthøj2025) using multiple imputations and incorporating variables associated with attrition at post-treatment into the statistical model. For each variable, 100 Markov Chain Monte Carlo imputations were performed.
The FaceYourFears trial was not powered for moderation analyses, underscoring the current study’s exploratory nature. Given the exploratory design, multiplicity adjustments were not applied (Bender & Lange, Reference Bender and Lange2001).
Covariate analyses (variables associated with outcome irrespective of intervention)
In these analyses, associations between candidate demographic (age, gender, education, and occupation) and clinical (diagnosis, paranoia, social anxiety, depression, safety behavior, core beliefs, level of functioning, delusion severity, negative symptoms, anhedonia, avolition, cognitive biases, and interpersonal trauma) variables and post-treatment paranoia (GPTS) were examined. The regression coefficient (b-value) represents the relationship between the candidate baseline variable and post-treatment paranoia. Positive b-values indicate that a 1-point increase in the candidate baseline variable is associated with an increase in post-treatment GPTS, suggesting a poorer treatment response. Conversely, negative b-values indicate that a 1-point increase in the candidate baseline variable is associated with a decrease in post-treatment GPTS, suggesting a greater treatment response.
Moderator analyses (variables potentially modifying the effect of the intervention)
In these analyses, treatment group (VR-CBTp or CBTp) was the input variable, post-treatment paranoia (GPTS) was the output variable, and baseline demographic (age, gender, education, and occupation) and clinical (diagnosis, paranoia, social anxiety, depression, safety behavior, core beliefs, level of functioning, delusion severity, negative symptoms, anhedonia, avolition, cognitive biases, and interpersonal trauma) variables were candidate moderators. Moderators are factors that allow estimation of an effect for a specific intervention for a group of patients with specific factors (Van Hoorn et al., Reference Van Hoorn, Tummers, Booth, Gerhardus, Rehfuess, Hind, Bossuyt, Welch, Debray, Underwood, Cuijpers, Kraemer, Van Der Wilt and Kievit2017, p. 2). The values of b represent the regression coefficients for the treatment group (VR-CBTp or CBT). CBTp served as the reference group; positive b-values indicate stronger associations in CBTp, while negative b-values indicate stronger associations in VR-CBTp.
Interaction analyses examined the relationship between treatment group allocation (randomization) and each moderator variable (randomization × moderator). For continuous variables, estimates of the outcome’s effect were conditioned at the 25th, 50th, and 75th percentile splits, representing ‘low’, ‘moderate’, and ‘high’ levels in the distribution of the candidate variables at baseline. These variables were analyzed as continuous moderators to assess linear associations across the full range of values. Separate analyses for each quartile were conducted, but results were only inspected in detail when interactions were significant.
Results
In total, 254 participants were included in the analyses (Table 1), with no significant baseline demographic or clinical differences between the VR-CBTp and CBTp groups, as reported elsewhere (Jeppesen et al., Reference Jeppesen, Vernal, Due, Mariegaard, Pinkham, Austin, Vos, Christensen, Hansen, Smith, Hjorthøi, Veling, Nordentoft and Glenthøj2025).
Baseline variables associated with outcome
All outcomes for candidate baseline variables associated with the outcome are provided in Table 2a, with post hoc analyses in Table 2b. Below, the results of variables with statistically significant associations with post-treatment paranoia are summarized.
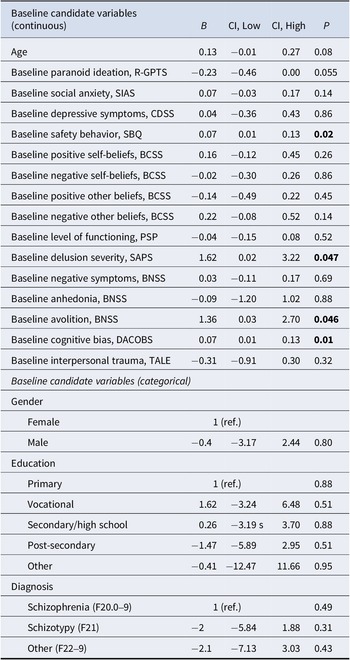
Results of covariate analyses (baseline variables associated with outcome irrespective of intervention).

Significance level: p < 0.05 (highlighted). All confidence intervals (CI) set at 95%. Measures: BCSS: Brief Core Schema Scale; BNSS: Brief Negative Symptom Scale; CDSS: Calgary Depression Scale for Schizophrenia; DACOBS: Davos Assessment of Cognitive Biases Scale; R-GPTS: Revised Green Paranoid Thoughts Scale; PSP: Personal and Social Performance Scale; Safety Behavior Questionnaire; SAPS: Scale for the Assessment of Positive Symptoms; SIAS: Social Interaction Anxiety Scale; TALE: Trauma and Life Events Checklist.
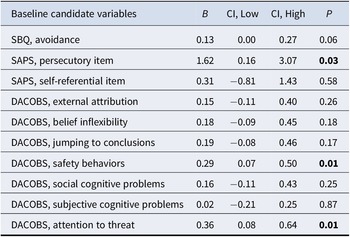
Post hoc covariate analyses (baseline variables associated with outcome irrespective of intervention).

Significance level: p < 0.05 (highlighted). All confidence intervals (CI) set at 95%. Measures: DACOBS: Davos Assessment of Cognitive Biases Scale; SAPS: Scale for the Assessment of Positive Symptoms; SBQ: Safety Behavior Questionnaire.
Avolition, delusion severity, safety behavior, and cognitive biases were associated with outcome, with higher baseline levels being associated with higher post-treatment paranoia, indicating less treatment response. With associations in the same direction, post-hoc analyses showed that SAPS delusion subscale item persecutory delusions and DACOBS subscales attention to threat and safety behavior were associated with outcome.
Moderation
Interactions
Results of interaction analyses for candidate moderators by treatment allocation are presented in Tables 3a and 3b.
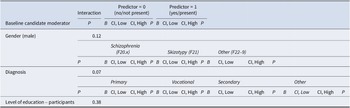
Results of moderator analyses (baseline variables interacting with randomization), continuous variables.

Significance level: p < 0.05 (highlighted). All confidence intervals (CI) set at 95%. Abbreviations: Cont = continuous; DNC = ‘Does not compute’ (software unable to conduct analysis); Hi/H = high; Lo/L = low; M = median split; 25% = 25 percentile split; 75% = 75 percentile split. Measures: BCSS: Brief Core Schema Scale; BNSS: Brief Negative Symptom Scale; CDSS: Calgary Depression Scale for Schizophrenia; DACOBS: Davos Assessment of Cognitive Biases Scale; R-GPTS: Revised Green Paranoid Thoughts Scale; PSP: Personal and Social Performance Scale; Safety Behavior Questionnaire; SAPS: Scale for the Assessment of Positive Symptoms; SIAS: Social Interaction Anxiety Scale; TALE: Trauma and Life Events Checklist.
Results of moderator analyses (baseline variables interacting with randomization), categorical variables.

Significance level: p < 0.05 (highlighted). All confidence intervals (CI) set at 95%.
Post hoc moderator analyses (baseline variables interacting with randomization), continuous variables.

Significance level: p < 0.05 (highlighted). All confidence intervals (CI) set at 95%. Abbreviations: Cont = continuous; DNC = Does not compute’ (software unable to conduct analysis); Hi/H = high; Lo/L = low; M = Median split; 25% = 25 percentile split; 75% = 75 percentile split. Measures: SAPS: Scale for the Assessment of Positive Symptoms.
Interactions were observed for avolition, negative other beliefs, delusion severity, and post hoc persecutory delusions, indicating that these baseline variables were differentially associated with outcome when comparing VR-CBTp and CBTp.
Moderators of outcome following either CBTp or VR-CBT
All outcomes of candidate moderators stratified by percentiles are provided in Tables 3a and 3b, with post hoc analyses in Table 3c. Below, statistically significant interactions are summarized, some showing stronger associations in either VR-CBTp or CBTp.
Avolition significantly moderated the association between group and paranoia at treatment cessation at the 75th percentile. Avolition at the sample’s highest level was more strongly positively associated with outcomes in the VR-CBTp group than the CBTp group, indicating greater improvement following VR-CBTp for participants with high baseline avolition.
Delusion severity significantly moderated the association between group and paranoia at treatment cessation when analyzed at the 25th percentile. Delusions at the sample’s lowest level (<25th percentile) were more strongly positively associated with outcomes following CBTp compared to VR-CBTp, suggesting that participants with low delusion severity improved more in CBTp. However, delusions above the sample’s lowest level (≥25th percentile) were more strongly positively associated with outcomes in the VR-CBTp group, suggesting that participants with moderate-to-high levels improved more in VR-CBTp.
Supplemental analyses
Supplemental analyses showed that SAPS global positive symptoms, BNSS asociality, alcohol intake, and parental education were associated with outcome (Supplementary Appendices B and C), and that SAPS global positive symptoms, BNSS asociality, DACOBS external attribution bias, and trustworthiness interacted with randomization (Supplementary Appendices D and E).
Discussion
This exploratory study examined whether baseline demographic and clinical variables were associated with post-treatment paranoia and whether they interacted with treatment allocation following 10 sessions of VR-CBTp or standard CBTp in a sample diagnosed with SSD. Across treatments, baseline avolition, safety behaviors, cognitive biases, and delusion severity were associated with poorer outcomes. Separately, high baseline avolition was associated with better outcomes in VR-CBTp than CBTp, and, while low-to-moderate delusion severity was linked to better outcomes in VR-CBTp, lower delusion severity was linked to better response to CBTp. Post hoc analyses suggested that the severity of persecutory delusions was the primary contributor to this effect. Demographic (age, gender, and education) and other clinical variables (diagnosis, paranoia, social anxiety, depression, functioning, total negative symptoms, anhedonia, core beliefs, and interpersonal trauma) were unrelated to outcome.
Baseline variables associated with outcome irrespective of treatment allocation
A novel finding was that higher baseline safety behavior was associated with poorer treatment outcomes across both CBTp and VR-CBTp but demonstrated no moderating effect. This contrasts previous findings suggesting it to be a moderator associated with better outcomes in VR-based interventions (Berkhof et al., Reference Berkhof, van der Stouwe, Pot-Kolder, van der Gaag, Veling and Geraets2024; Freeman et al., Reference Freeman, Lambe, Kabir, Petit, Rosebrock, Yu, Dudley, Chapman, Morrison, O’Regan, Aynsworth, Jones, Murphy, Powling, Galal, Grabey, Rovira, Martin, Hollis and West2022). Compared with prior studies, the present study differed with respect to analytic strategy, number of sessions, measures of baseline paranoia, and administration of safety behavior subscales. Differences in primary symptom targets, such as agoraphobia versus paranoia, may also contribute. Safety behaviors related specifically to paranoia may constitute a distinct construct, and a dedicated self-report measure has recently been developed (Lambe et al., Reference Lambe, Mulhall, Bird, Williams, Mitchell, Roddan, Sokunle, Rosebrock, Freeman and Waite2025). Given heterogeneity across studies, these findings should be interpreted cautiously. Further research is warranted to clarify how safety behaviors are associated with CBTp and VR-CBTp.
The negative effect of avolition mirrors prior findings linking higher baseline avolition to greater negative symptom severity at follow-up (Allott et al., Reference Allott, Alvarez-Jimenez, Killackey, Bendall, McGorry and Jackson2011). Extending this to paranoia at treatment cessation, the present findings support the view that avolition represents a central domain within the negative symptom construct (Strauss et al., Reference Strauss, Bartolomeo and Harvey2021). Taken together with the null findings for total negative symptoms, which contrast with earlier studies (Lincoln et al., Reference Lincoln, Rief, Westermann, Ziegler, Kesting, Heibach and Mehl2014; Tarrier et al., Reference Tarrier, Beckett, Harwood, Baker, Yusupoff and Ugarteburu1993; Thomas et al., Reference Thomas, Rossell, Farhall, Shawyer and Castle2011), the results underscore the importance of assessing negative symptoms at the domain level (Galderisi et al., Reference Galderisi, Mucci, Dollfus, Nordentoft, Falkai, Kaiser, Giordano, Vandevelde, Nielsen, Glenthøj, Sabé, Pezzella, Bitter and Gaebel2021), rather than relying solely on total scores or global ratings.
Consistent with prior findings (e.g. Brabban et al., Reference Brabban, Tai and Turkington2009; Jenner et al., Reference Jenner, Payne, Waite, Beckwith, Diamond, Isham, Collett, Emsley and Freeman2024), delusion severity was associated with outcome, with post hoc analyses suggesting the strength of perceived persecution to be involved. This is in line with cognitive models of persecutory delusions, which highlight their strong links with maintenance processes (e.g. Freeman, Reference Freeman2016). Future research could further examine how different components of persecutory delusion severity relate to outcome, with recent findings suggesting that conviction may be particularly prognostically informative (Jenner et al., Reference Jenner, Payne, Waite, Beckwith, Diamond, Isham, Collett, Emsley and Freeman2024).
Cognitive biases were associated with outcome, consistent with their established role in the development and maintenance of delusions (De Rossi & Georgiades, Reference De Rossi and Georgiades2022), but contrasting with previous findings suggesting that they do not constitute a barrier to improvement during CBTp (Lincoln et al., Reference Lincoln, Rief, Westermann, Ziegler, Kesting, Heibach and Mehl2014). Post hoc analyses of DACOBS subscales indicated that ‘attention to threat’ and ‘safety behavior’ biases were particularly implicated. These subscales have previously shown strong correlations with clinician-rated safety behavior and self-reported paranoia (Pot-Kolder et al., Reference Pot-Kolder, Geraets, Veling, van Beilen, Staring, Gijsman, Delespaul and van der Gaag2018; Van der Gaag et al., Reference Van der Gaag, Schütz, ten Napel, Landa, Delespaul, Bak, Tschacher and De Hert2013). Methodologically, this raises whether DACOBS provides incremental value when the GPTS and SBQ are already included, given that the GPTS is a preferred self-report measure of paranoia (Statham et al., Reference Statham, Emerson and Rowse2019). Clinically and theoretically, these results highlight the importance of targeting specific threats to maintain cognitive processes in the treatment of paranoia (Moritz et al., Reference Moritz, Balzan, Menon, Rojahn, Schlechte, Veckenstedt, Schöttle and Meinhart2025; Sauve et al., Reference Sauve, Lavigne, Pochiet, Brodeur and Lepage2020), consistent with modular approaches aimed at strengthening a sense of safety as a counterbalance to heightened threat sensitivity (Freeman et al., Reference Freeman, Emsley, Diamond, Collett, Bold, Chadwick, Isham, Bird, Edwards, Kingdon, Fitzpatrick, Kabir, Waite, Carr, Causier, Černis, Kirkham, Lambe, Lister and Twivy2021).
Moderation of outcome following VR-CBTp or CBTp
The differential moderation by baseline avolition represents a novel contribution to CBTp research, as it suggests that VR-CBTp may mitigate the otherwise negative association between avolition and treatment outcome when compared directly with CBTp. This might reflect the greater in-session exposure time observed in VR-CBTp (Jeppesen et al., Reference Jeppesen, Vernal, Due, Mariegaard, Pinkham, Austin, Vos, Christensen, Hansen, Smith, Hjorthøi, Veling, Nordentoft and Glenthøj2025), as well as its immersive, behavior-focused format, which can facilitate engagement in and accessibility to therapeutic tasks (Bell et al., Reference Bell, Pot-Kolder, Rizzo, Rus-Calafell, Cardi, Cella, Ward, Riches, Reinoso, Thompson, Alvarez-Jimenez and Valmaggia2024). In the FaceYourFears trial, VR-CBTp enabled real-time exposure and cognitive work during sessions, while CBTp relied more on between-session tasks such as homework and symptom monitoring (Jeppesen et al., Reference Jeppesen, Due, Mariegaard, Pinkham, Vos, Veling, Nordentoft and Glenthøj2022). Together with the cognitive restructuring demands typically required during CBTp sessions (e.g. Beck & Rector, Reference Beck and Rector2005), these between-session requirements may pose barriers for individuals with motivational impairments, potentially limiting treatment outcomes (Kazantzis et al., Reference Kazantzis, Whittington, Zelencich, Kyrios, Norton and Hofmann2016; Thai et al., Reference Thai, Audet, Koestner, Lepage and O’Driscoll2024). This aligns with emerging evidence suggesting that immersive VR-interventions may help alleviate negative symptoms and the associated challenges (Novo et al., Reference Novo, Fonsêca, Barroso, Guimarães, Louro, Fernandes, Lopes and Leitão2021). Given evidence linking therapeutic alliance with improvements in negative symptoms (Browne et al., Reference Browne, Wright, Berry, Mueser, Cather, Penn and Kurtz2021), and suggestions that VR may facilitate collaborative therapeutic experiences (e.g. Christensen et al., Reference Christensen, Rydborg, Jørgensen, Nielsen, Mainz, Bell, Thomas, Smith, Mariegaard, Ward, Nordentoft, Glenthøj and Vernal2025), the attenuated negative impact of avolition in VR-CBTp relative to CBTp may partly reflect VR-specific affordances for strengthening alliance and engagement.
The differential moderation by baseline delusion severity also represents a novel finding, indicating a nuanced pattern of treatment responsiveness. This might reflect individuals with lower delusion severity having a stronger cognitive foundation, including greater cognitive flexibility, better insight, and lower conviction in their beliefs, which may facilitate engagement with the cognitive demands of CBTp (Brabban et al., Reference Brabban, Tai and Turkington2009; Garety et al., Reference Garety, Fowler, Kuipers, Freeman, Dunn, Bebbington, Hadley and Jones1997; Jenner et al., Reference Jenner, Payne, Waite, Beckwith, Diamond, Isham, Collett, Emsley and Freeman2024; Naeem et al., Reference Naeem, Kingdon and Turkington2008; Waltz, Reference Waltz2017). In contrast, individuals with more pronounced delusion symptoms may benefit more from the enhanced experiential learning offered by VR-CBTp, which can present safer, more immediate alternative experiences to challenge inflexible paranoid beliefs (Bell et al., Reference Bell, Pot-Kolder, Rizzo, Rus-Calafell, Cardi, Cella, Ward, Riches, Reinoso, Thompson, Alvarez-Jimenez and Valmaggia2024; Freeman et al., Reference Freeman, Garety, Kuipers, Bebbington, Fowler and Dunn2004). Thus, the present results hold promise for implementing precision medicine approaches in which either CBTp or VR-CBTp could be prescribed pending the initial level of paranoia severity.
Nonsignificant treatment effect modification
Overall, most candidate baseline variables were unrelated to treatment outcome, aligning with meta-analytic evidence suggesting no consistent treatment effect modification of CBTp (Turner et al., Reference Turner, Reijnders, van der Gaag, Karyotaki, Valmaggia, Moritz, Lecomte, Turkington, Penadés, Elkis, Cather, Shawyer, O’Connor, Li, de Paiva Barretto and Cuijpers2020; Varese et al., Reference Varese, Sudell, Morrison, Longden and Tudur Smith2025). However, the significant effects identified here suggest that the question remains open and highlight limitations in comparing CBTp protocols across studies. Differences in outcome measures, symptom targets, and conceptualization of symptoms may contribute to inconsistent findings. Furthermore, the integration of VR within CBTp has enabled examination of moderators less commonly assessed in traditional trials, such as safety behaviors (Berkhof et al., Reference Berkhof, van der Stouwe, Pot-Kolder, van der Gaag, Veling and Geraets2024), not explored in previous reviews or meta-analyses.
Notably, self-reported paranoia, which was a part of the inclusion criteria in the FaceYourFears trial (Jeppesen et al., Reference Jeppesen, Vernal, Due, Mariegaard, Pinkham, Austin, Vos, Christensen, Hansen, Smith, Hjorthøi, Veling, Nordentoft and Glenthøj2025), was unrelated to outcome. This indicates that alternative cutoff thresholds of self-reported paranoia would most likely not have altered the conclusion that VR-CBTp was not superior to standard CBTp. These findings suggest that future VR-CBTp trials may consider alternatives to self-reported paranoia as eligibility criteria. Clinician-rated delusional severity may represent a more informative candidate, given its association with outcome, and may further enhance external validity by better aligning trial inclusion criteria with routine clinical assessment practices.
Given that the relatively weak moderation signals between VR-CBTp and CBTp provide little guidance for treatment selection in routine care, future research should also consider patient preference as a potential determinant of outcomes. Patient preference has been associated with improved treatment satisfaction, treatment completion, and clinical response (Bennett et al., Reference Bennett, Toevs, Angus, Krawczak, Trentacosta, Jagadeesh, Tomlinson and Lindhiem2025). Greater patient involvement in therapy processes, shared decision-making approaches, and allowing patients to select preferred treatment modalities may therefore enhance engagement and improve outcomes (Gerger et al., Reference Gerger, Nascimento, Locher, Gaab and Trachsel2020; Stovell et al., Reference Stovell, Morrison, Panayiotou and Hutton2016; Swift et al., Reference Swift, Callahan, Cooper and Parkin2018).
Strengths and limitations
The study’s strengths include the clinical relevance, sample size, use of a broad range of candidate baseline variables, and data from the high-quality FaceYourFears trial, which enrolled 254 participants broadly representative of the psychiatric clinic population, enhancing generalizability.
Limitations should, however, be noted. First, the study was not powered to detect subgroup effects, as FaceYourFears employed a fixed sample size and was not designed for moderator analyses. No individual subgroup reached the required size for adequate statistical power, increasing the risk of type I and II errors. Moreover, interaction tests typically require larger sample sizes than those available. Additionally, the randomization has technically been compromised due to subgroup and interaction analyses, except when the subgroups were defined by a variable used for stratification during the original randomization procedure. Consequently, these exploratory subgroup analyses should be considered hypothesis-generating and require replication in adequately powered trials specifically designed to test subgroup effects. Furthermore, the statistical models used in the study could not differentiate between a lack of treatment response and clinical deterioration. Although baseline paranoia was controlled for and changes were interpreted as treatment effects, deterioration cannot be entirely excluded. However, given the large overall effect size in the primary trial (Jeppesen et al., Reference Jeppesen, Vernal, Due, Mariegaard, Pinkham, Austin, Vos, Christensen, Hansen, Smith, Hjorthøi, Veling, Nordentoft and Glenthøj2025), substantial deterioration appears unlikely. All participants were included in the analyses, consistent with the intention-to-treat approach in the primary trial. While this preserves randomization benefits, minimizes bias, and enhances generalizability, it limits our ability to determine whether participants with certain moderating characteristics may have received suboptimal treatment or dropped out prematurely, potentially masking moderator effects. Moreover, the strength of the identified associations with the outcome seems modest. Although statistically significant, the clinical significance of identified associations between treatment outcome and baseline safety behavior, avolition, cognitive biases, and delusion severity appears modest. Finally, the analyses focused on baseline variables and treatment cessation outcome, preventing the assessment of in-session variables and long-term effects of candidate variables. Future studies should investigate in-session variables and whether baseline variables have sustained effects beyond the immediate post-treatment period.
Conclusion
This exploratory study found that higher baseline avolition, safety behavior, delusion severity, and cognitive biases were associated with poorer paranoia outcomes across participants receiving 10 sessions of either CBTp or VR-CBTp. Moderator analyses revealed a more nuanced pattern: individuals with elevated avolition benefited more from VR-CBTp, and, while moderate-to-high delusion severity was linked to better outcomes in VR-CBTp, lower delusion severity was linked to better response to CBTp. The seemingly contradictory findings suggest that although higher avolition and delusion severity are generally linked to poorer outcomes overall, individuals with elevated levels may benefit relatively more from VR-CBTp than from CBTp in direct comparisons. Demographic and most clinical variables were unrelated to outcome, with significant associations being statistically or clinically modest. This tentatively suggests both therapies may be broadly applicable across diverse clinical profiles in individuals with paranoia. However, given the exploratory design, findings should be interpreted with caution and considered hypothesis-generating rather than conclusive.
Supplementary material
The supplementary material for this article can be found at http://doi.org/10.1017/S0033291726103870.
Data availability statement
Data from the FaceYourFears trial will, after initial publications, be made publicly available through the Danish National Archives.
Acknowledgments
The authors extend their gratitude to all participants in the FaceYourFears trial. Details regarding compliance with ethical standards can be found in the primary study (Jeppesen et al., Reference Jeppesen, Vernal, Due, Mariegaard, Pinkham, Austin, Vos, Christensen, Hansen, Smith, Hjorthøi, Veling, Nordentoft and Glenthøj2025).
Author contribution
The first, second, and last author designed the study. The fourth author conducted the statistical analyses as an external consultant. The first author drafted the manuscript with contributions from the second author. The third, fourth, and last author critically revised the manuscript before forwarding to co-authors. All authors provided feedback during rounds of revision, with the first author incorporating suggestions in collaboration with the second author and with inputs from the third, fourth, and last author. All authors contributed to and approved the final manuscript.
Funding statement
This work was supported by the same grants as in the FaceYourFears trial: Tryg foundation (ID: 148727), Independent Research Fund Denmark (0134-00066B), Research Fund of the Mental Health Services – Capital Region of Denmark, Research and Fund for Health Research 2019 – Capital Region of Denmark (A6622), Innovation Fund North Denmark Region (2022–0010), Psychiatry Research Fund North Denmark Region (1–45-72-3778-24), The M. L. Jørgensen and Gunnar Hansen Fund (2022–0019), and The A.P. Moller Foundation (L-2021-00244). None of the funders had a role in the study design, data collection, analysis, or interpretation, and no role in writing the article.
Competing interests
The second and last authors are involved in other funded studies investigating VR-therapy. Furthermore, they have received funding to teach a VR-assisted form of avatar therapy by the Danish VR-firm Khora. Otherwise, the authors declare no conflicts of interest.
Ethical standard
Ethical approval for the FaceYourFears trial was granted by the Regional Ethics Committee (H-20048806) and Data Protection Agency (P-2020-823). Written informed consent was obtained from all FaceYourFears participants, who were informed of their right to withdraw at any time. The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008.
Clinical trial registration
The FaceYourFears trial was registered with ClinicalTrials.gov identifier NCT04902066.
Declaration of generative AI and AI-assisted technologies in the writing process
During the preparation of this work, the authors used ChatGPT to limit word count, redundancy, and improve the readability of the description of statistics. After using this tool/service, the authors reviewed and edited the content as needed and take full responsibility for the content of the publication.






 Open access
Open access