

1. Introduction
Mental healthcare in the Netherlands is experiencing a crisis in terms of accessibility for people who urgently need support. Each year, around one in five people experiences a mental health problem, often presenting patterns of comorbidity (Reference Steel, Marnane, Iranpour, Chey, Jackson, Patel and SiloveSteel et al., 2014). Treatment access rates for major depressive disorder range from 51% in high-income regions to 20% in lower-middle- and low-income countries (Reference Moitra, Santomauro, Collins, Vos, Whiteford, Saxena and FerrariMoitra et al., 2022). The long waiting times are a symptom of this complex problem. Waiting lists for the Dutch Association of Mental Health Providers are considered unacceptably long, and only 33% of patients meet the standard set by the governmental health authorities of 4 weeks of waiting until receiving a first intake interview (Nederlandse Zorgautoriteit, 2024). In parallel, general practitioners (GPs), municipalities, and secondary-care mental health providers have been observing a rise in mental health complaints (Ministerie van Volksgezondheid, Welzijn en Sport et al., 2022).
To tackle this challenge, innovations in Dutch mental healthcare should strive to alleviate the healthcare professionals’ workload and improve caregivers’ experience. According to current care demand, in 2040 1 in 4 workers in the Netherlands will have to work in healthcare (Ministerie van Volksgezondheid, Welzijn en Sport et al., 2022), and therefore hiring more healthcare professionals is not a sustainable solution. Healthcare providers should aim to reduce resource burden while safeguarding a motivated and efficient workforce and a positive caregiving experience (Reference Sikka, Morath and LeapeSikka et al., 2015). Previous literature has shown the benefits of implementing well-being interventions at the individual level to assist healthcare professionals in managing stress and boosting their resilience, but fewer interventions have been successfully developed and implemented to reduce stress and workload at an organisational level (Reference Cohen, Pignata, Bezak, Tie and ChildsCohen et al., 2023; Reference Fox, Johnson, Berkman, Sianoja, Soh, Kubzansky and KellyFox et al., 2022).
To ease resource burden at an organisational level, we highlight the potential of artificial intelligence (AI) in (semi-)automating processes related to triage, therapy planning, and treatment delivery (Reference Gutierrez, Stephenson, Eadie, Asadpour and AlaviGutierrez et al., 2024). By AI solutions, we refer to all technological developments and services that emulate human intelligence and decision-making processes, encompassing various types of machine learning algorithms (Reference MichMich, 2020). AI solutions demonstrate value in analysing patterns within behavioural data and monitoring chronic mental health conditions, but they also pose risks of excessive patient surveillance (Reference Babu and JosephBabu & Joseph, 2024). AI-integration programs in healthcare may represent time reductions in administrative workload between 33% and 66%, liberating time that can be used on caregiving tasks (MIT Technology Review & GE Healthcare, 2019). Online triage tools and symptom checkers are some examples of health services enabled by data technologies that assess patients’ symptoms and provide advice and guidance to patients around the appropriate health pathway (Reference Chambers, Cantrell, Johnson, Preston, Baxter, Booth and TurnerChambers et al., 2019; Reference Wallace, Chan, Chidambaram, Hanna, Iqbal, Acharya, Normahani, Ashrafian, Markar, Sounderajah and DarziWallace et al., 2022). In this paper, we focus on AI-supported triage and signposting for patients with mental health issues because of the potential gains in care efficiency through the reduction of waiting times and optimising referral of patients to appropriate services in either mental, primary, or social care domains (Reference Ni and JiaNi & Jia, 2025).
Despite their potential to support higher efficiency and accessibility to mental health services, the adoption of digital triage tools in the healthcare system is very limited. A recent survey on the Dutch GPs’ digital means showed that only 3% of practices have integrated digital triage systems (Vliegweld and Patiëntenfederatie Nederland, 2024). A study conducted in Australia on digital triage identified that only one out of 500,000 patients met the eligibility criteria for participation in a digital triage and monitoring program for mental health (Reference Allison, Bastiampillai, Kisely and LooiAllison et al., 2024). Two barriers for deploying machine learning models in mental health services are the lack of co-creation with clinicians and the misalignment of these models with each specialist’s capabilities in psychiatric care and treatment pathways available (Reference Chekroud, Bondar, Delgadillo, Doherty, Wasil, Fokkema, Cohen, Belgrave, DeRubeis, Iniesta, Dwyer and ChoiChekroud et al., 2021). Moreover, in high-risk contexts such as psychiatric care, the literature on AI highlights that AI solutions’ agency and capabilities should follow the values and objectives of the humans who use them (Reference Ji, Qiu, Chen, Zhang, Lou, Wang, Duan, He, Zhou and ZhangJi et al., 2023).
To explore how AI solutions such as digital triage tools can be effectively adopted in mental health pathways, this study drew on the concept of integrated care pathways (ICPs). ICPs mainly consist of patients’ journey maps that inform a multidisciplinary care management team on how to improve efficiency and quality in care delivery and ensure that treatment protocols are followed (Reference Allen, Gillen and RixsonAllen et al., 2009). They represent a tool to orchestrate roles and responsibilities from a multi-stakeholder perspective (Reference Rees, Huby, McDade and McKechnieRees et al., 2004), enhance continuity of care, and support the implementation of multi-disciplinary guidelines and protocols (Reference Schrijvers, van Hoorn and HuiskesSchrijvers et al., 2012). Similarly, service blueprinting represents a type of journey mapping that has been utilised to examine AI technology as an organisational resource within clinical settings, highlighting its role in key stages of the care journey (Reference Magyari and SecomandiMagyari & Secomandi, 2023). Service design approaches also demonstrated potential to ensure human-centredness in the development of digital services and foster institutional change (Reference Patrício, Grenha Teixeira and VinkPatrício et al., 2019).
Therefore, this study used a service design approach focused on care pathways to provide an initial understanding of the opportunities of AI technologies to improve triaging and signposting into secondary-care mental health services and, ultimately, overall quality of care. We zoomed in on the context of a Dutch mental health organisation that provides secondary-care generalist mental health services for moderate or medium-complexity patients. Recognising the importance of aligning AI solutions with the values and objectives of the actors within a service system, this study explores the following questions: Q1- What are the current bottlenecks to efficiently access secondary-care generalist mental health services? Q2- What challenges can we investigate through prototypes of AI-supported service processes, and what design questions do they pose?
2. Research design
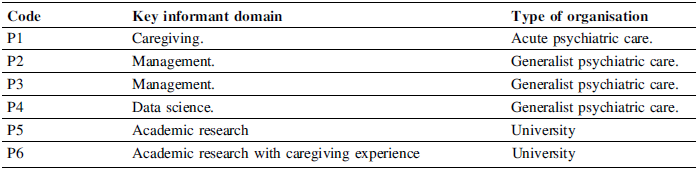
To investigate where in the care pathway AI technologies could provide the highest value, we conducted a descriptive study through semi-structured interviews (Reference Blessing and ChakrabartiBlessing & Chakrabarti, 2009). We selected participants who held substantial knowledge about the context of interest and could be considered key informants (Reference PattonPatton, 2014). As shown in Table 1, we interviewed 6 domain experts; two of them were interviewed in one session (P5 & P6). Three of the six participants (P2, P3 & P4) were key decision-makers in the R&D and management of a generalist mental health organisation, and three others (P1, P5 & P6) were experts outside of the Dutch mental health organization who had experience in providing or researching generalist or specialist mental health services in the Netherlands and could complement the input of the other three decision-makers.
Key informants interviewed

2.1. Data collection
The interview plan was guided by the research questions and followed the ‘path of expression’ from generative design research (Reference Sanders and StappersSanders & Stappers, 2012). The participants first reflected on the patient journey, discussing stages such as GP referral, screening, treatment, and further referrals. Then, they provided insights into labour-intensive processes and current bottlenecks in the care pathway. Finally, we discussed their aspirations and perspectives on how AI solutions could be adopted to tackle these challenges.
During the interviews, a service blueprint was used to stimulate a discussion on the current care journey and explore opportunities for AI-supported interventions. A first version of the blueprint was created before the interviews based on open-access information from the mental health organisation and governmental websites, and was iteratively refined with the interview participants’ input. Apart from allowing the experts to correct the care journey phases, key stakeholders and communication channels, the service blueprint allowed participants to point and annotate bottlenecks and challenges across different stages of the care pathway and at diverse triage or patient stratification moments. This is based on the role of design artefacts, in this case the service blueprint, as a generative tool to imagine and expand the design space (Reference Stappers and GiaccardiStappers & Giaccardi, 2014). The blueprinting materials, as shown in Figure 1, consisted of four types of cards: care stages (orange) to map key patient journey moments, stakeholder cards (blue) to identify responsible institutions and professionals, data sources (brown) used to screen, diagnose and monitor patients, and touchpoint cards (green) to represent technologies supporting communication and coordination. During the interview, the participants had access to an online project board with the service blueprint so that they could interact and propose changes.
2.2. Data extraction and analysis
To analyse the interviews, the recorded audios were transcribed and inductively coded by selecting quotes that represented either modifications in the service blueprint (care journey stages, sources of evidence, stakeholders involved, and communication channels) or challenges/bottlenecks in the current processes. The coding process was mainly generative (Reference Sanders and StappersSanders & Stappers, 2012), instead of focusing on code frequency. The insights on challenges and bottlenecks from the coding process were iteratively mapped along the service blueprint as shown in Figure 1.
After all interviews had been finalised, we clustered the bottlenecks and challenges described by the key informants. In Figure 1, the areas coloured in different shades of purple represent the clusters of challenges and bottlenecks. From the emerging clusters of challenges and bottlenecks, we could derive ‘design requirements’ which form the intervention directions described in the results section. As shown in Figure 2, these intervention directions were added to a copy of the service blueprint to visualise in which stage of the care journey they address. This process of transforming and combining stakeholders’ challenges and aspirations into possible design interventions can be thought of as ‘creative leaps’ (Reference CrossCross, 2006). The challenges and design requirements that define each intervention direction are listed in Table 3 in the next section.
Finally, the intervention directions were presented in a multidisciplinary session with stakeholders from a regional insurance company and the secondary-care generalist mental health provider involved in this project to share the findings and incorporate their feedback. This multidisciplinary session also guided the discussion of our results.
Section of the service blueprint with bottlenecks and challenges along the care journey

3. Results
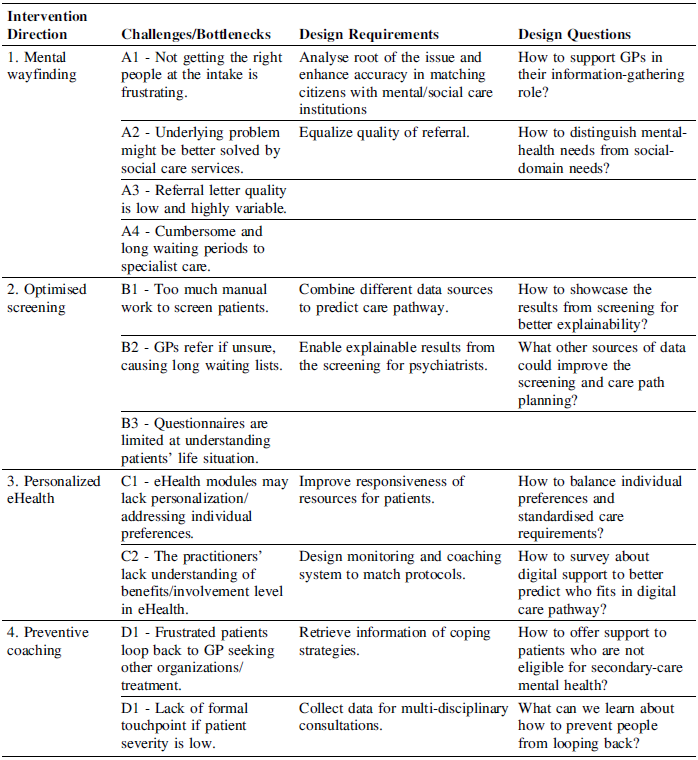
The interviews with key informants yielded 11 challenges/bottlenecks, which were clustered into four intervention directions. Figure 2 shows two of the intervention directions added to the service blueprint. Table 2 presents the challenges/bottlenecks illustrated with representative quotes. Table 3 presents the four intervention directions through three categories of information: the challenges and bottlenecks extracted from the semi-structured interviews, the inferred design requirements, and design questions to guide future design activities and research. Despite two clusters having more challenges and bottlenecks, we decided to keep two design requirements per intervention direction to allow easier comparison among the four directions.
Section of the service blueprint with the intervention directions

Figure 2 Long description
The flowchart illustrates the process of mental healthcare service intervention in the Netherlands. The process begins with a referral and registration step. From there, patients are placed on a waiting list. The next step involves optimized screening, which combines different data sources to predict care paths and is explainable and scrutable for therapists. Following the screening, patients are referred back to their general practitioner (GP). There is a decision point asking how to showcase the results from screening for better explainability. The final step is preventive coaching, which involves information retrieval of coping strategies and data collection for an exploratory consultation.
The first intervention direction in Table 3, “Mental wayfinding”, draws on challenges in the referral and intake processes. These include poor quality and variability in referral letters and inefficiencies in identifying exclusion criteria, leading to long waiting times and frustration among patients, GPs, and mental health practitioners. Additionally, after long waiting and screening periods, some patients may require social care or more specialised mental health services instead of generalist psychiatry. Participants recognised lengthy and cumbersome waiting times for specialist psychiatric care, too. Interventions in this area should aim to standardise referral quality, identify underlying issues, or provide feedback to screening specialists on appropriate referrals. By prototyping this intervention, researchers can explore ways to support GPs in gathering information for secondary-care psychiatry. For instance, investigating the characteristics of a service system that uses a natural language processing model to synthesise and classify GP consultation notes that point towards a need for social care or psychiatric treatment, which can be used as input for a GP follow-up meeting or a multidisciplinary meeting.
The second direction, “Optimised screening”, highlights the burden of manual administrative work to screen patients in secondary-care mental health services and the tendency of GPs to refer patients despite uncertainty, due to time constraints. Moreover, some participants highlighted that standardised screening questionnaires do not comprehensively capture patients’ life situations and they could be more effectively combined with other data sources, such as the GP referral letter, to make appropriate decisions. To address these issues, future research could explore the use of machine learning methods that combine several existing data sources, such as the GP referral letter and mental health questionnaires, and provide recommendations for appropriate care pathways. This direction aligns with the potential of machine learning models to use routinely-collected data to predict treatment outcomes and support practitioners in making treatment decisions (Reference Chekroud, Bondar, Delgadillo, Doherty, Wasil, Fokkema, Cohen, Belgrave, DeRubeis, Iniesta, Dwyer and ChoiChekroud et al., 2021), but also raises questions on how to ensure the explainability of machine learning models’ suggestions to healthcare professionals.
The third intervention, “Personalised eHealth”, s gaps in stratifying patients in eHealth modules, with participants highlighting the need for personalised digital care that aligns with patient preferences. Additionally, some participants highlighted that practitioners require support in understanding the value and necessary engagement in eHealth systems. Researchers could investigate this direction by exploring how to provide responsive and adaptive eHealth modules to individual patient profiles while adhering to established protocols, and co-designing digital monitoring that aligns with practitioners’ values and objectives. A possibility would be to investigate the integration of AI agents supported by a retrieval augmented generation architecture (Reference Stryker and ScapicchioStryker & Scapicchio, 2026) to adapt the content of eHealth modules to the diverse contexts and needs of patients or, for instance, suggest extra modules that patients may need, such as a sleep-specific module when patients frequently report sleep deprivation. However, this direction raises questions regarding the balance between personalisation and standardised care (Reference Jerjes and HardingJerjes & Harding, 2024), as well as how to determine patient eligibility for digital care pathways.
The fourth direction, “Preventive coaching”, addresses challenges in communication and referral back to GP care, particularly the lack of formal touchpoints for patients with lower-severity conditions. As a result, these patients often return to the overburdened GPs seeking referrals to other generalist psychiatric institutions. Therefore, further research could explore how to provide relevant coping strategies to patients who were deemed not eligible for secondary-care mental health services and gather additional patient data when the origin of the patient’s issue remains unclear. Regarding this direction, researchers could investigate the use of ML-based recommender systems due to their potential to suggest tailored content recommendations and allow individuals to control the data they are feeding to the system (Reference Figueroa, Torkamaan, Bhattacharjee, Hauptmann, Guan and SedrakyanFigueroa et al., 2025). A recommender system could then use data related to individual preferences and lifestyle, and retrieve mild coping strategies to try before going back to GPs.
Insights from the semi-structured interviews and illustrative quotes

Description of the four intervention directions

4. Discussion
In this study, service blueprinting effectively supported the involvement of diverse domain experts to define unmet opportunities for quality improvement, resulting in four intervention directions for using AI technologies to support patient triage and signposting processes in mental health services. The insights are preliminary and exploratory in nature, intending to inform future research and development, but we must acknowledge that the generalizability of these results is limited by a small sample of participants. The results may be generalizable to other generalist secondary-care psychiatry in the Netherlands, but not to specialised psychiatric services. Moreover, they should not be interpreted as standalone solutions to the systemic challenges discussed. Especially, since service inefficiencies cannot be solved only by standardising or automating processes (Reference Fließ and KleinaltenkampFließ & Kleinaltenkamp, 2004).
These intervention directions were presented in a multidisciplinary meeting with decision-makers from a regional insurance company and the secondary-care generalist mental health provider involved in this project. The stakeholders agreed that AI algorithms should aim to support providing more care with fewer resources through evidence-based eHealth programmes. The third intervention direction sparked great interest, and participants in this meeting suggested that providing personalised eHealth modules should aim to enhance patient engagement and adherence to therapy and, in turn, reduce the need for check-ups and unnecessary involvement of psychologists and therapists. Previous literature has proposed utilising digital tools for data collection to enhance precision mental health care, leading to improved decision-making about effective care pathways and individual treatment outcomes (Reference Bickman, Lyon and WolpertBickman et al., 2016; Reference Moggia, Lutz, Brakemeier and BickmanMoggia et al., 2024). Furthermore, there is a growing interest in the development of digital twins to provide more personalised treatment and coaching in healthcare services (Reference Kamel Boulos and ZhangKamel Boulos & Zhang, 2021).
Despite the initial focus on digital triage, taking a greater service-level perspective, we found that a promising direction for AI technologies was to adapt therapy content according to engagement preferences and patients’ personal contexts. This may be seen as signposting patients into specific treatment content. Similarly, previous research has shown that engagement patterns can influence treatment outcomes (Reference Chien, Enrique, Palacios, Regan, Keegan, Carter, Tschiatschek, Nori, Thieme, Richards, Doherty and BelgraveChien et al., 2020), and personalising digital therapy may lead to better treatment adherence and outcomes (Reference Hornstein, Zantvoort, Lueken, Funk and HilbertHornstein et al., 2023). Moreover, multinational technology companies highlight the value of generative AI tools to efficiently personalise communications and content suggestions to improve engagement (Reference Hayes and DownieHayes & Downie), but the direct evidence that these technologies will benefit service efficiency in healthcare remains limited (Reference GoodingGooding, 2024). Therefore, we pose that future work on digitalisation of mental health services should further investigate whether (1) AI systems to personalize eHealth modules can lead to reducing delays in recovery and accelerating patient flow, and if (2) the integration of AI technologies in online therapy modules to enhance patient’s self-management can also facilitate that more patients can be treated with the same human resources.
However, the use of AI techniques in mental treatment pathways raises concerns about risks of bias, transparency, and accountability (Reference Thakkar, Gupta and De SousaThakkar et al., 2024). There is a danger that AI tools are built on inaccurate and biased data, which leads to inequalities in diagnosis, risk detection and reproducing demographic biases (Reference Thakkar, Gupta and De SousaThakkar et al., 2024). For example, adapting therapy content based on unproven stereotypes could lead to worsened treatment outcomes for specific groups of people. In the face of these challenges, the design of AI-supported digital mental health care pathways should be framed within standardised protocols (Reference Jerjes and HardingJerjes & Harding, 2024), ensure clinician oversight as the practitioners are more aware of contextual factors (Reference Chekroud, Bondar, Delgadillo, Doherty, Wasil, Fokkema, Cohen, Belgrave, DeRubeis, Iniesta, Dwyer and ChoiChekroud et al., 2021) and incorporate a health equity lens to ensure that personalisation mechanisms serve marginalised populations (Reference Figueroa, Torkamaan, Bhattacharjee, Hauptmann, Guan and SedrakyanFigueroa et al., 2025). In this regard, future research should continue to explore design processes and frameworks to develop triage, screening and therapy content personalisation strategies that consider algorithmic bias and health equity.
5. Conclusion
In this descriptive study, we used semi-structured expert interviews supported by service blueprinting to provide a first overview of how AI technologies can innovate the service journey from general practices to secondary-care generalist psychiatry services in the Netherlands, while considering existing institutional arrangements and service processes. Starting from the idea of AI-supported triage and signposting, we mapped bottlenecks and challenges along a service blueprint, and proposed four intervention directions for design researchers interested in AI-supported mental health services and developers of AI tools for mental health clinical practice. We found that promising directions in AI technology include improving the classification of patient cases that require support from either mental or social care, combining different data sources to accelerate screening processes, investigating how to provide personalised therapy modules, and supporting processes for referring patients back to primary care. AI developers and design researchers investigating these directions should explore, in parallel with their development, how to preserve human oversight, a necessary degree of standardisation, and equity in health outcomes.
Acknowledgement
The authors wish to thank all the interview participants for their time and invaluable insights. We also thank Fredrik K. Bodell and Juliana Silva Barbosa for their ideas and feedback on this paper.




 Open access
Open access