


Introduction
PCOS is a complex endocrine condition impacting patients’ health across the lifespan. It is defined by a combination of ovulatory dysfunction, hyperandrogenism and polycystic ovary morphology (Ref. Reference Goodarzi, Dumesic, Chazenbalk and Azziz1). PCOS affects an estimated 4%–21% of women worldwide, a wide range that largely reflects differences in the clinical criteria applied for diagnosis (Ref. Reference Lizneva, Suturina, Walker, Brakta, Gavrilova-Jordan and Azziz2). Over the past 10 years, its prevalence in China has similarly exhibited a marked upward trend (Ref. Reference Yang, Li, Zhou, Qian, Zhang, Wu, Jin, Wu, Zhang, Zheng, Tan, Hao, Li, Tian, Hao, Zheng, Wang, Norman, Li, Liu and Qiao3). The pathogenesis of PCOS is currently unknown, the genetic factors, insulin resistance and obesity may play roles in its development (Ref. 4). The 2003 Rotterdam criteria, which include oligomenorrhea, hyperandrogenism and polycystic ovary morphology (PCOM) has been mostly used as diagnostic criteria in clinical practice (Ref. Reference Kumariya, Ubba, Jha and Gayen5). For women of childbearing age, there is growing concern that PCOS leads to female infertility.
PCOS causes ovulation disorders, leading to menstrual cycle irregularities and infertility. According to a meta-analysis, roughly 15% of women diagnosed with PCOS experience oligoovulation (Ref. Reference Bozdag, Mumusoglu, Zengin, Karabulut and Yildiz6). Infertility resulting from PCOS can be addressed through lifestyle improvement, ovulation-stimulating therapy and assisted reproductive technology (ART). The outcome of assisted ART is, however, adversely impacted by the endocrine and reproductive system dysfunction associated with PCOS. A common IVF complication, ovarian hyperstimulation syndrome (OHSS) (Ref. Reference Sun, Ma, Li, Hu, Wang, Zhang, Dai and Sun7), is a known cause of unsuccessful embryo transfer procedures. PCOS patients are also at increased risk for a range of poor pregnancy outcomes versus those without PCOS (Ref. Reference Alenezi, Khan and Amer8).
Recently, the significance of acupuncture within assisted reproductive technology has become increasingly prominent. Several studies have reported that acupuncture can enhance live birth and pregnancy rate in infertile women (Ref. Reference Manheimer, Zhang, Udoff, Haramati, Langenberg, Berman and Bouter9). Clinical studies have investigated acupuncture for treating various types of infertility, such as infertility due to POR, recurrent implantation failure (RIF) and PCOS (Refs Reference Guo, Wei and Song10, Reference Zegers-Hochschild, Adamson, Dyer, Racowsky, de Mouzon, Sokol, Rienzi, Sunde, Schmidt, Cooke, Simpson and van der Poel11, Reference Li15–Reference Xing, Liu and Dong27). In 2002, Paulus and colleagues reported in an RCT (Ref. Reference Paulus, Zhang, Strehler, El-Danasouri and Sterzik12) that acupuncture applied during the IVF-ET process resulted in a significant improvement in the clinical pregnancy rate. However, a 2018 study by Smith et al. (Ref. Reference Smith, de Lacey, Chapman, Ratcliffe, Norman, Johnson, Boothroyd and Fahey13) concluded that acupuncture provided no significant increase in live birth rates in treatment cycles of fresh embryo transfers. In 2022, Chinese academician Jisheng Han discovered that acupuncture may improve endometrial receptivity, thereby improving pregnancy outcomes in IVF-ET patients, particularly in patients of older reproductive age (Ref. Reference Feng, Zhu, Yang, Wang, Sun, Li, Gong, Han, Zhang and Han14). These studies indicate that while acupuncture is increasingly used in ART, its efficacy remains uncertain and controversial.
However, these studies often suffer from insufficient numbers of participants, suboptimal study designs and unclear long-term efficacy due to short follow-up periods. Currently, in the field of traditional Chinese medicine, robust statistical evaluations remain scarce. This study, therefore, seeks to conduct a systematic assessment of all accessible RCTs to evaluate both the safety profile and effectiveness of acupuncture for PCOS management, thereby contributing pertinent evidence to the field.
Method
Information sources and search methods
We systematically searched in The Cochrane, Web of Science, Embase, PubMed, VIP database, CNKI database, WanFang database and CBM database from their establishment until April 1, 2024. A hand-search was also conducted through the reference sections of key articles to locate any other eligible RCTs. Publications in Chinese and English were both eligible for inclusion. The search strategy combined subject terms and free terms such as (‘ovary syndrome, polycystic’ or ‘polycystic ovarian syndrome’ or PCOS), (‘Acupuncture Therapy’ or acupunct or acupuncture) and (‘fertilization in vitro’ or ‘in vitro fertilization’ or IVF). The specific vocabulary and syntax used for searching were adapted to align with the unique requirements and search field structures of each individual database. The review was prospectively registered on PROSPERO (registration number CRD42024539293). The detailed search methodology is available in Supplementary Material 1.
Eligibility criteria
All studies that evaluated the therapeutic effects and safety characteristics of acupuncture treatment for PCOS were considered eligible for inclusion. Animal studies were excluded. Several studies (Refs Reference Li15–Reference Xiang, Xia, Song, Liu and Lian21) used the Rotterdam criteria for diagnosing PCOS (Ref. 22); however, studies based on clinical symptoms or corresponding criteria were included if the Rotterdam criteria were not explicitly mentioned. The intervention considered was acupuncture therapy, including hand acupuncture and electroacupuncture. Comparators included no intervention or sham acupuncture. There were no limits on the duration of intervention. The following outcomes were included:
Primary outcome: Clinical pregnancy rate (number of cycles achieving clinical pregnancy/number of embryo transfers).
Secondary outcomes: Live birth rate (number of deliveries resulting in live births/number of transferred cycles×100%), fertilization rate (numbers of 2PN zygotes/numbers of MII oocytes inseminated), number of retrieved oocytes (numbers of retrieved oocytes /count of ≥ 14 mm follicles on the day of trigger), high-quality embryo rate (numbers of high-quality embryos/total numbers of embryos, Embryo quality was classified on a grade of I– IV, as previously described and level I embryos considered high-quality), thickness of endometrium, dose and duration of Gn used, level of progesterone (P), luteinizing hormone (LH) and oestradiol (E2) on the hCG day.
Adverse effects: Number of OHSS cases, the miscarriage rate (the number of spontaneous intrauterine pregnancy losses before 20 completed weeks of gestation/the number of transplantation cycles×100%) and cycle cancellation rate.
All definitions herein adhere to The International Glossary on Infertility and Fertility Care (2017) (Ref. 22).
Data collection and selection process
Two authors independently screened the publications after removing duplicates using the EndNote21 reference manager programme. The selection process began with a review of titles and abstracts. Potentially relevant studies identified in this phase were subsequently retrieved for a detailed full-text evaluation to determine if they met the study’s eligibility requirements. For this purpose, a uniform data extraction form was designed to ensure systematic collection of information. The following data were extracted into a predefined data extraction sheet: title, first author, publication year, the design of the study, main study results, the criteria for including and excluding participants, details regarding the PICO (patient population, intervention, comparator and outcomes) and the outcome measurement.
When outcomes were shown as continuous variables, the corresponding mean and standard deviation (SD) were extracted. For dichotomous data, we recorded the number of occurrences in the patients. Data presented only in the form of charts were extracted using professional software (Automeris).
Study risk of bias assessment
To appraise the risk of bias within the selected trials, the Cochrane risk-of-bias assessment tool (Ref. Reference Cumpston, Li, Page, Chandler, Welch, Higgins and Thomas23) specific for RCTs was applied. Two independent reviewers (Z.H.L and Y.L.N) performed quality assessments, and a third reviewer (Y.R) consulted to resolve any disagreements. We created a risk of bias graph and summaries using the Review Manager (RevMan, version 5.4). The risk of bias assessment targeted several core methodological areas: procedures for randomization and concealment of allocation; blinding of personnel, participants and outcome assessors; approaches to managing incomplete data; potential for selective outcome reporting and consideration of any other biases. Each study was categorized into three levels for each criterion: ‘low risk’, ‘unclear’ or ‘high risk’.
Data analysis
The effect of acupuncture for women with PCOS during IVF was analysed using RevMan version 5.4 to perform the Meta-analysis.
-
1) Study Heterogeneity: Heterogeneity was assessed using the Cochrane Chi-square test and I square (I 2) statistic. An I 2 statistic less than 50% or a P-value greater than 0.01 indicated low heterogeneity. When these criteria were met, we used a fixed effects model. Otherwise, significant heterogeneity was indicated, and a random-effects model was applied to account for heterogeneity across studies.
-
2) Statistical Significance: For all analyses in this review, statistical significance was set at P < 0.05.
-
3) Outcome Measure: Risk ratios (RR) expressed dichotomous outcomes, while mean differences (MD) were calculated for continuous variables, both reported with 95% Confidence Intervals (CIs). When the measurement method or unit is the same, outcomes were extracted using the weighted mean difference (WMD); otherwise, the standardized mean difference (SMD) were applied.
The small total number of included studies and concerns regarding their quality precluded the planned subgroup analyses. Similarly, due to the insufficient number of RCTs, we only created the funnel plot for the clinical pregnancy rate. We used forest plots to graphically display the results.
Results
Search results
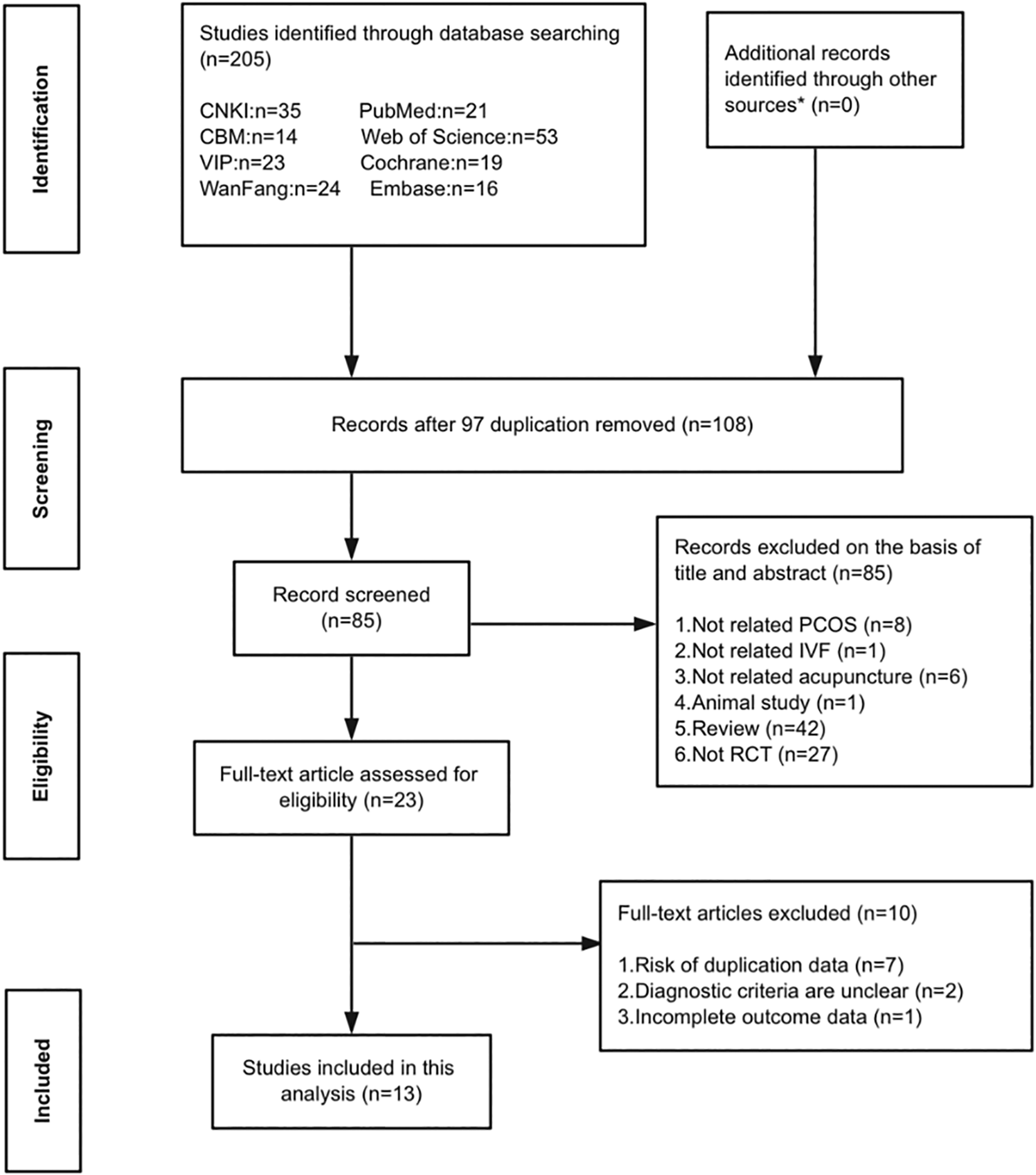
We imported 205 relevant records into EndNote after searching across eight databases. After removing duplicates, 108 articles remained. Upon screening the titles and abstracts, we excluded 85 articles for the following reasons: not related to PCOS (n = 8), not related to IVF (n = 1), not related to acupuncture (n = 6), animal study (n = 1), and not RCTs (n = 69). Twenty-three papers were deemed eligible, and their full text articles were obtained for review. A final set of 13 RCTs (Refs Reference Li15–Reference Xiang, Xia, Song, Liu and Lian21, Reference Rashidi, Tehrani, Hamedani and Pirzadeh24–Reference Wu, Ning, Ye, Liu, Tang, Hu and Zhuo29) met all inclusion criteria and were analysed. The flow of literature through the different stages of screening and selection is detailed in Figure 1.
Flow diagram of the study selection process. *Other sources included the reference list of the studies and a Google search.

Study characteristics
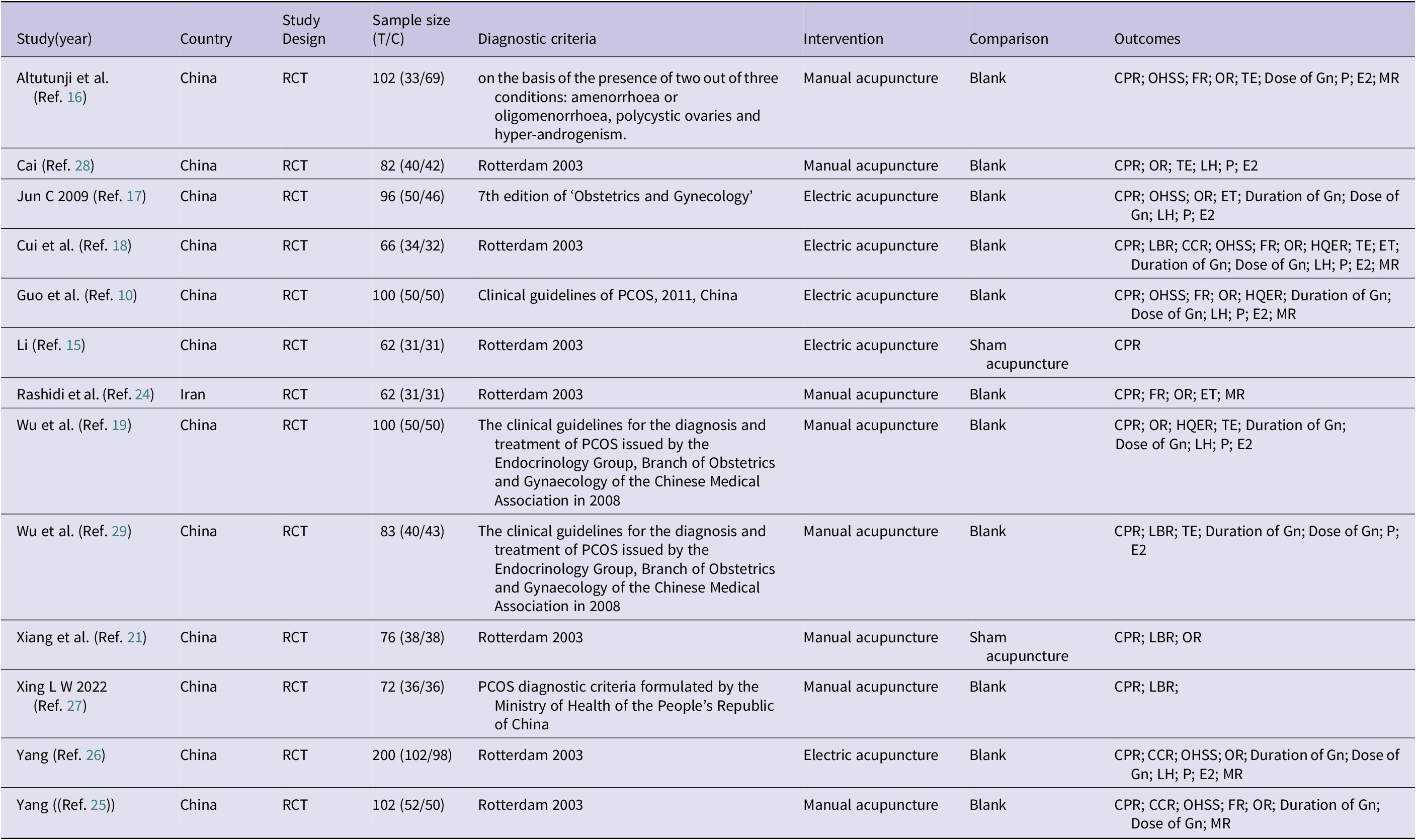
Table 1 summarizes the main characteristics of the eligible RCTs. A total of 1,203 patients were enrolled across the 13 RCTs, which were published between 2009 and 2022. Twelve studies were conducted in China and one in Iran (Ref. Reference Rashidi, Tehrani, Hamedani and Pirzadeh24). Two studies (Refs Reference Li15, Reference Yang25) were master’s dissertations, and the remaining 11 were journal articles (Refs Reference Li15, Reference Altutunji, Liu, Cai, Wang and Gao16, Reference Cui, Li, Sun and Wen18–Reference Ajeena, Al-Haris and Al-Kefae20, Reference Rashidi, Tehrani, Hamedani and Pirzadeh24–Reference Wu, Ning, Ye, Liu, Tang, Hu and Zhuo29). Four articles (Refs Reference Cui, Li, Sun and Wen18, Reference Wu, Zhuo and Tang19, Reference Rashidi, Tehrani, Hamedani and Pirzadeh24, Reference Cai, Li, Zhao, Liu, Yan and Tong28) were published in English, and the other nine (Refs Reference Li15–Reference Jun, Wei and Jing17, Reference Ajeena, Al-Haris and Al-Kefae20, Reference Xiang, Xia, Song, Liu and Lian21, Reference Yang25–Reference Xing, Liu and Dong27, Reference Wu, Ning, Ye, Liu, Tang, Hu and Zhuo29) were published in Chinese. Regarding diagnostic criteria, seven studies utilized the 2003 Rotterdam criteria (Refs Reference Li15–Reference Xiang, Xia, Song, Liu and Lian21), one study diagnosed PCOS based on clinical symptoms (Ref. Reference Altutunji, Liu, Cai, Wang and Gao16) and the other five articles provided a clear PCOS diagnostic consensus. Therapy included manual acupuncture (Refs Reference Li15, Reference Cui, Li, Sun and Wen18, Reference Xiang, Xia, Song, Liu and Lian21, Reference Rashidi, Tehrani, Hamedani and Pirzadeh24, Reference Xing, Liu and Dong27–Reference Wu, Ning, Ye, Liu, Tang, Hu and Zhuo29) and electric acupuncture (Refs Reference Altutunji, Liu, Cai, Wang and Gao16, Reference Jun, Wei and Jing17, Reference Wu, Zhuo and Tang19, Reference Ajeena, Al-Haris and Al-Kefae20, Reference Yang25, Reference Yang, Cui and Li26). Among the 13 studies, two compared acupuncture therapy with placebo (sham acupuncture) (Refs Reference Jun, Wei and Jing17, Reference Wu, Zhuo and Tang19), while the control group in the other studies did not receive any intervention. The outcomes included: clinical pregnancy rate (Refs Reference Li15–Reference Xiang, Xia, Song, Liu and Lian21, Reference Rashidi, Tehrani, Hamedani and Pirzadeh24–Reference Wu, Ning, Ye, Liu, Tang, Hu and Zhuo29), live birth rate (Refs Reference Altutunji, Liu, Cai, Wang and Gao16, Reference Wu, Zhuo and Tang19, Reference Cai, Li, Zhao, Liu, Yan and Tong28, Reference Wu, Ning, Ye, Liu, Tang, Hu and Zhuo29), fertilization rate (Refs Reference Altutunji, Liu, Cai, Wang and Gao16, Reference Jun, Wei and Jing17, Reference Rashidi, Tehrani, Hamedani and Pirzadeh24–Reference Yang, Cui and Li26), number of oocytes retrieved (Refs Reference Li15, Reference Altutunji, Liu, Cai, Wang and Gao16, Reference Cui, Li, Sun and Wen18–Reference Xiang, Xia, Song, Liu and Lian21, Reference Rashidi, Tehrani, Hamedani and Pirzadeh24–Reference Xing, Liu and Dong27) high-quality embryo rate (Refs Reference Altutunji, Liu, Cai, Wang and Gao16, Reference Yang, Cui and Li26, Reference Xing, Liu and Dong27), thickness of endometrium (Refs Reference Li15, Reference Altutunji, Liu, Cai, Wang and Gao16, Reference Rashidi, Tehrani, Hamedani and Pirzadeh24, Reference Xing, Liu and Dong27, Reference Cai, Li, Zhao, Liu, Yan and Tong28) number of embryo transferred (Refs Reference Altutunji, Liu, Cai, Wang and Gao16, Reference Cui, Li, Sun and Wen18, Reference Yang25), dose of Gn (Refs Reference Altutunji, Liu, Cai, Wang and Gao16, Reference Ajeena, Al-Haris and Al-Kefae20, Reference Xiang, Xia, Song, Liu and Lian21, Reference Rashidi, Tehrani, Hamedani and Pirzadeh24–Reference Cai, Li, Zhao, Liu, Yan and Tong28), duration of Gn (Refs Reference Altutunji, Liu, Cai, Wang and Gao16, Reference Ajeena, Al-Haris and Al-Kefae20, Reference Xiang, Xia, Song, Liu and Lian21, Reference Yang25–Reference Cai, Li, Zhao, Liu, Yan and Tong28), levels of P (Refs Reference Li15, Reference Altutunji, Liu, Cai, Wang and Gao16, Reference Ajeena, Al-Haris and Al-Kefae20, Reference Rashidi, Tehrani, Hamedani and Pirzadeh24–Reference Cai, Li, Zhao, Liu, Yan and Tong28), LH (Refs Reference Li15, Reference Altutunji, Liu, Cai, Wang and Gao16, Reference Yang25–Reference Xing, Liu and Dong27) and E2 (Refs Reference Altutunji, Liu, Cai, Wang and Gao16, Reference Ajeena, Al-Haris and Al-Kefae20, Reference Rashidi, Tehrani, Hamedani and Pirzadeh24–Reference Cai, Li, Zhao, Liu, Yan and Tong28), cycle cancellation rate (Refs Reference Altutunji, Liu, Cai, Wang and Gao16, Reference Ajeena, Al-Haris and Al-Kefae20, Reference Xiang, Xia, Song, Liu and Lian21), number of OHSS cases (Refs Reference Altutunji, Liu, Cai, Wang and Gao16, Reference Ajeena, Al-Haris and Al-Kefae20, Reference Xiang, Xia, Song, Liu and Lian21, Reference Rashidi, Tehrani, Hamedani and Pirzadeh24–Reference Yang, Cui and Li26) and the miscarriage rate (Refs Reference Altutunji, Liu, Cai, Wang and Gao16, Reference Cui, Li, Sun and Wen18, Reference Ajeena, Al-Haris and Al-Kefae20, Reference Xiang, Xia, Song, Liu and Lian21, Reference Rashidi, Tehrani, Hamedani and Pirzadeh24, Reference Yang, Cui and Li26).
Basic information on RCTs included

Blank means no treatment; CPR: Clinical pregnancy rate; CCR: Cycle cancellation rate; E2: the level of oestrogen; ET: number of embryo transferred; FR: fertilization rate; HQER: high-quality embryo rate; LBR: live birth rate; LH: the level of luteinizing hormone; MR: miscarriage rate; OHSS: number of Ovarian hyperstimulation syndrome; OR: number of oocytes retrieved; P: the level of progesterone; TE: thickness of endometrium.
Risk-of-bias assessment
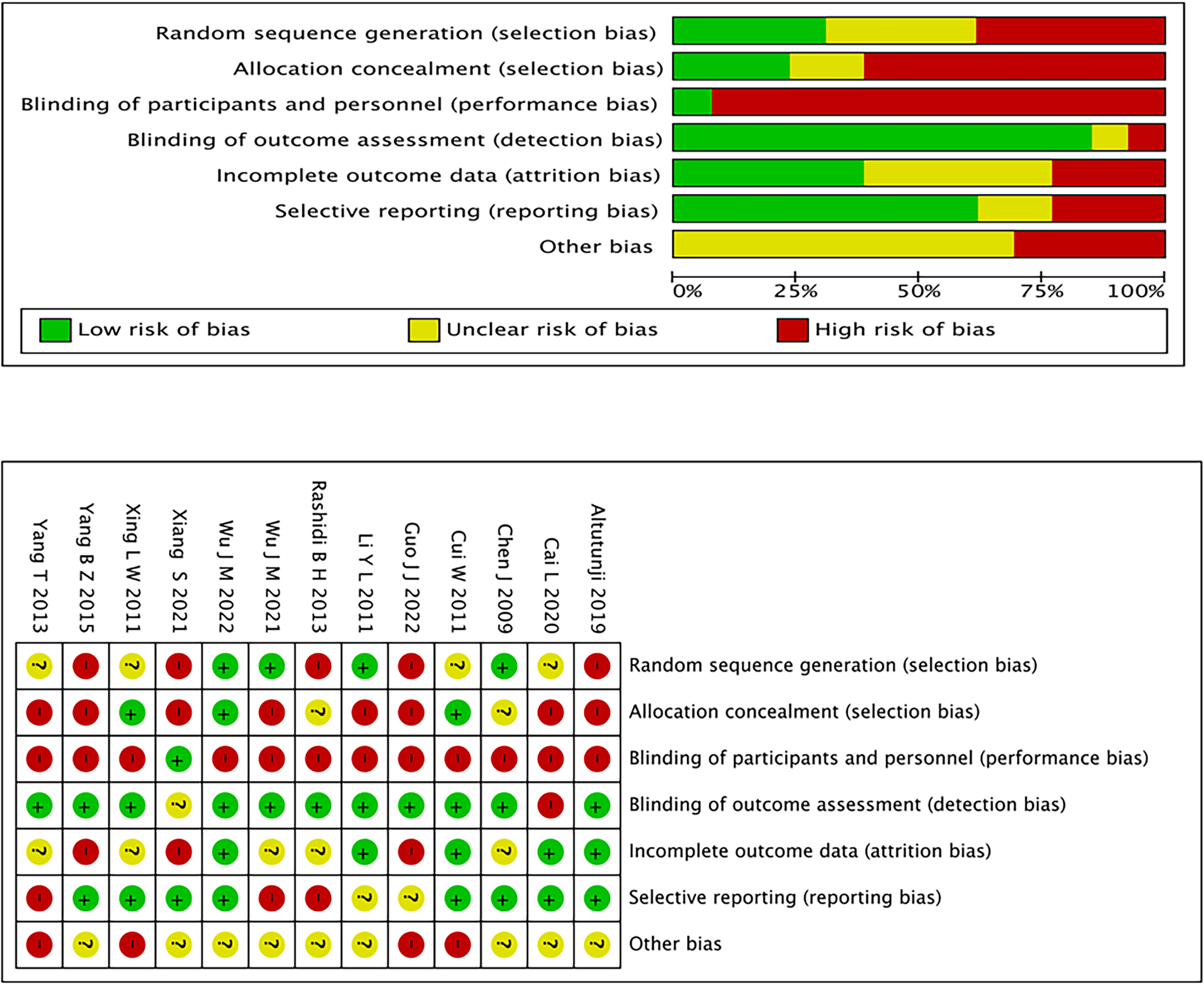
Figure 2 shows the risk of bias assessment for the included studies. The Cochrane Handbook’s predefined criteria guided our assessment of study quality. All 13 studies mentioned the randomized sequence generation. Two studies (Refs Reference Jun, Wei and Jing17, Reference Yang25) did not mention whether allocation was concealed, and seven studies were judged to be at high risk of bias in the randomization process (Refs Reference Li15, Reference Jun, Wei and Jing17, Reference Wu, Zhuo and Tang19–Reference Xiang, Xia, Song, Liu and Lian21, Reference Yang, Cui and Li26, Reference Xing, Liu and Dong27). Only two studies reported the blinding of participants and researchers (Refs Reference Jun, Wei and Jing17, Reference Wu, Zhuo and Tang19). Across the included trials, the risk of bias related to the blinding of outcome assessment was judged to be low. It was unclear whether complete outcome data were reported in one study (Ref. Reference Jun, Wei and Jing17). None of the 13 trials selectively reported outcomes. Four included RCTs were rated as carrying a high risk of other bias for various reasons: one did not mentions the basic information of participants (Ref. Reference Altutunji, Liu, Cai, Wang and Gao16), one included a specific type among PCOS patients (Ref. Reference Cui, Li, Sun and Wen18), one did not compare the BMI of two groups (Ref. Reference Xing, Liu and Dong27) and one included patients diagnosed only with PCO (Ref. Reference Yang25). Funnel plots for all outcomes can be found in Supplementary Material 2.
Risk of bias.

Associations between acupuncture therapy and IVF outcomes
Clinical pregnancy rate
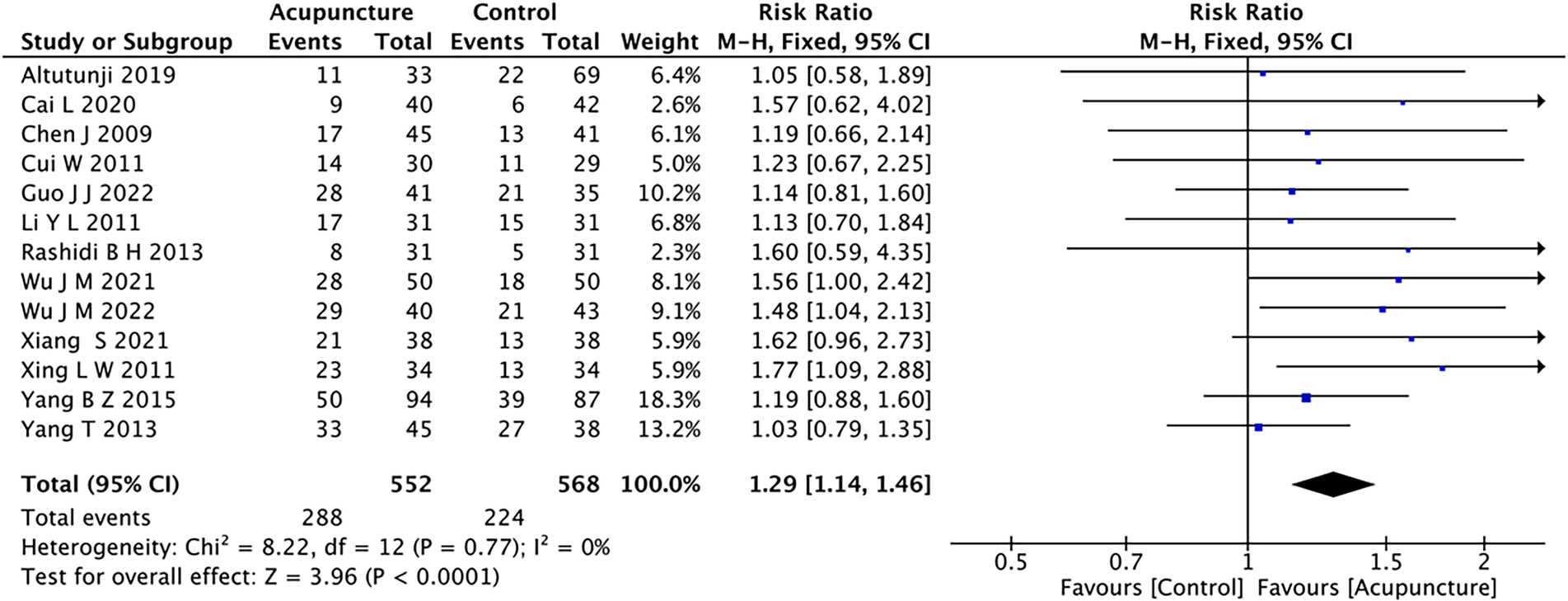
CPR was evaluated in all 13 studies. In every study, the CPR was greater among patients receiving acupuncture compared to those in the control group. Acupuncture therapy significantly improved CPR, as revealed by the meta-analysis, showing a notable enhancement in CPR for women with PCOS undergoing IVF-ET (RR 1.29; 95%CI: 1.14 to 1.46; P < 0.01; I 2 = 0%, Figure 3). No indication of publication bias was detected for the clinical pregnancy rate based on the funnel plot.
Forest plot of CPR for meta-analysis of acupuncture among women with PCOS undergoing IVF-ET.

Live birth rate
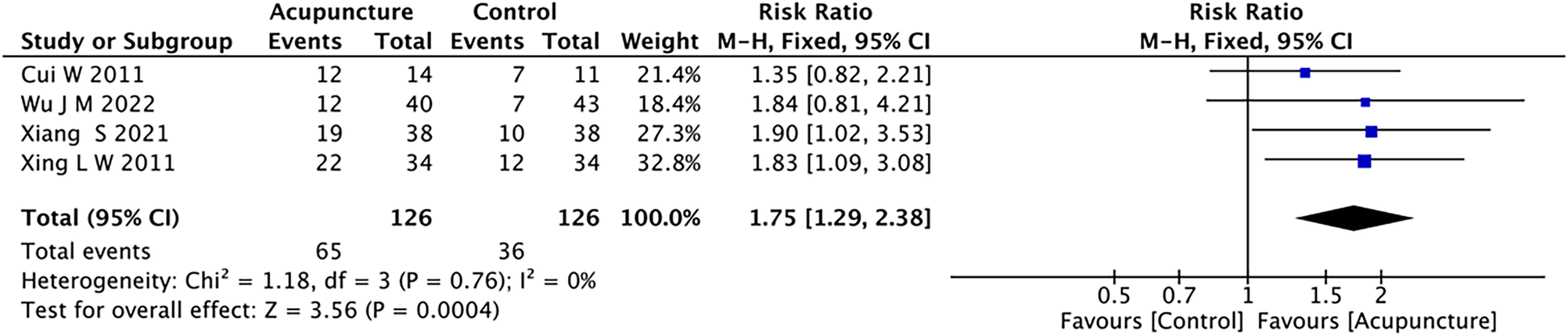
Four studies (Refs Reference Altutunji, Liu, Cai, Wang and Gao16, Reference Wu, Zhuo and Tang19, Reference Cai, Li, Zhao, Liu, Yan and Tong28, Reference Wu, Ning, Ye, Liu, Tang, Hu and Zhuo29) evaluated the live birth rate among 252 registered participants. As a long-term prognostic index, our study demonstrated a higher live birth rate in PCOS women receiving acupuncture compared to those not receiving it(RR 1.75; 95%CI: 1.29 to 2.38; P < 0.001; I 2 = 0%, Figure 4). This indicates that acupuncture therapy can improve pregnancy outcomes.
Forest plot of LBR for meta-analysis of acupuncture among women with PCOS undergoing IVF-ET.

Dose and duration of Gn
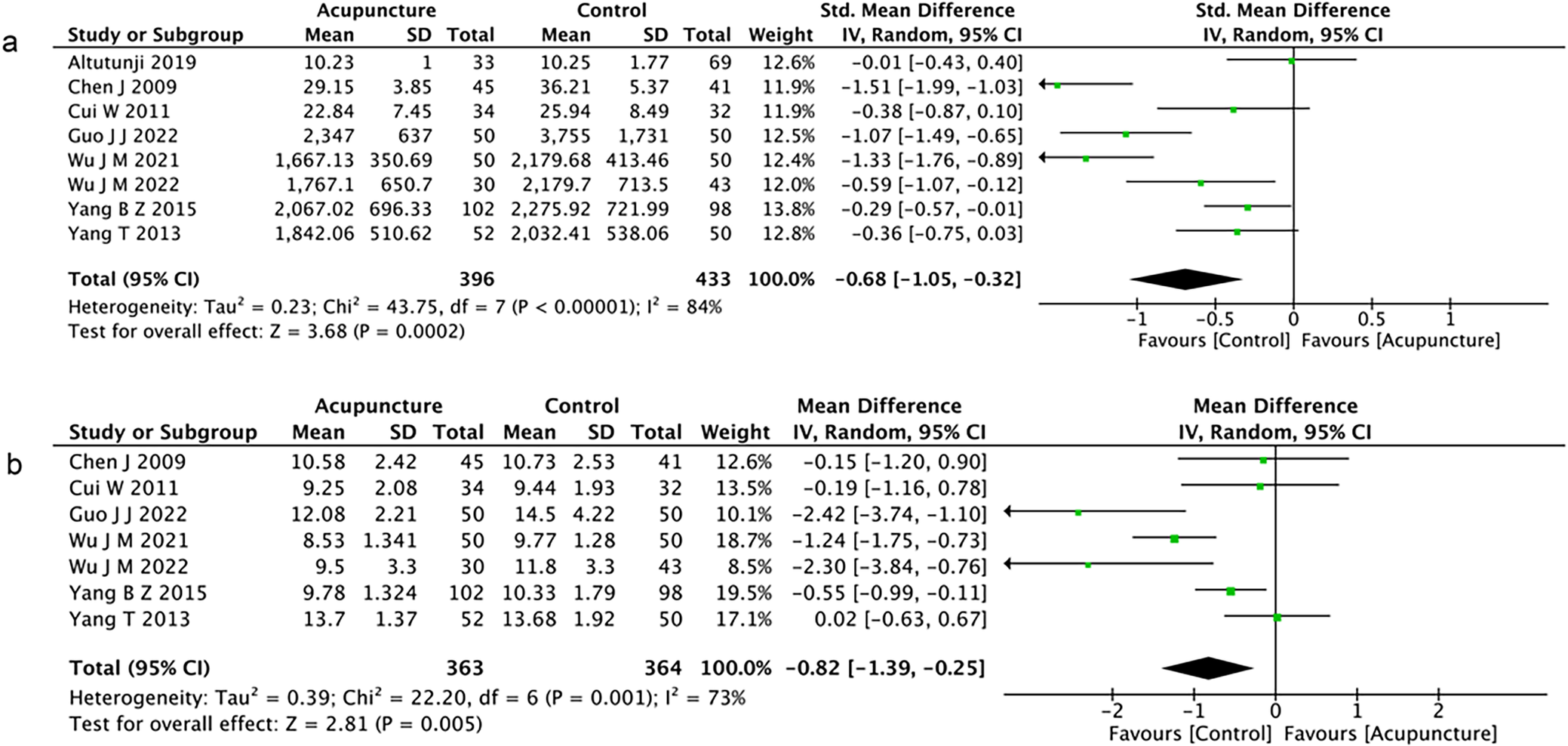
Eight studies (Refs Reference Altutunji, Liu, Cai, Wang and Gao16, Reference Ajeena, Al-Haris and Al-Kefae20, Reference Xiang, Xia, Song, Liu and Lian21, Reference Rashidi, Tehrani, Hamedani and Pirzadeh24–Reference Cai, Li, Zhao, Liu, Yan and Tong28)compared the Gn dose used in the acupuncture and control groups. Among these, five studies showed a significant difference (Refs Reference Ajeena, Al-Haris and Al-Kefae20, Reference Yang25–Reference Cai, Li, Zhao, Liu, Yan and Tong28). A significantly lower Gn dose was observed with acupuncture in the random-effects model analysis(SMD −0.68; 95%CI: −1.05 to −0.32; P = 0.0002; I 2 = 84%; Figure 5A).
Forest plots for meta-analysis of acupuncture among women with PCOS undergoing IVF-ET. Forest plot for (A) dose of Gn and (B) duration of Gn.

The duration of Gn was reported in seven RCTs (Refs Reference Altutunji, Liu, Cai, Wang and Gao16, Reference Ajeena, Al-Haris and Al-Kefae20, Reference Xiang, Xia, Song, Liu and Lian21, Reference Yang25–Reference Cai, Li, Zhao, Liu, Yan and Tong28). In four studies (Refs Reference Ajeena, Al-Haris and Al-Kefae20, Reference Yang, Cui and Li26–Reference Cai, Li, Zhao, Liu, Yan and Tong28), the duration of Gn in the acupuncture group was shorter than that in the control group. Fewer days of Gn use were associated with acupuncture.(WMD -0.82; 95%CI: −1.39 to −0.25; P = 0.005; I 2 = 73%, Figure 5B).
Number of oocytes retrieved
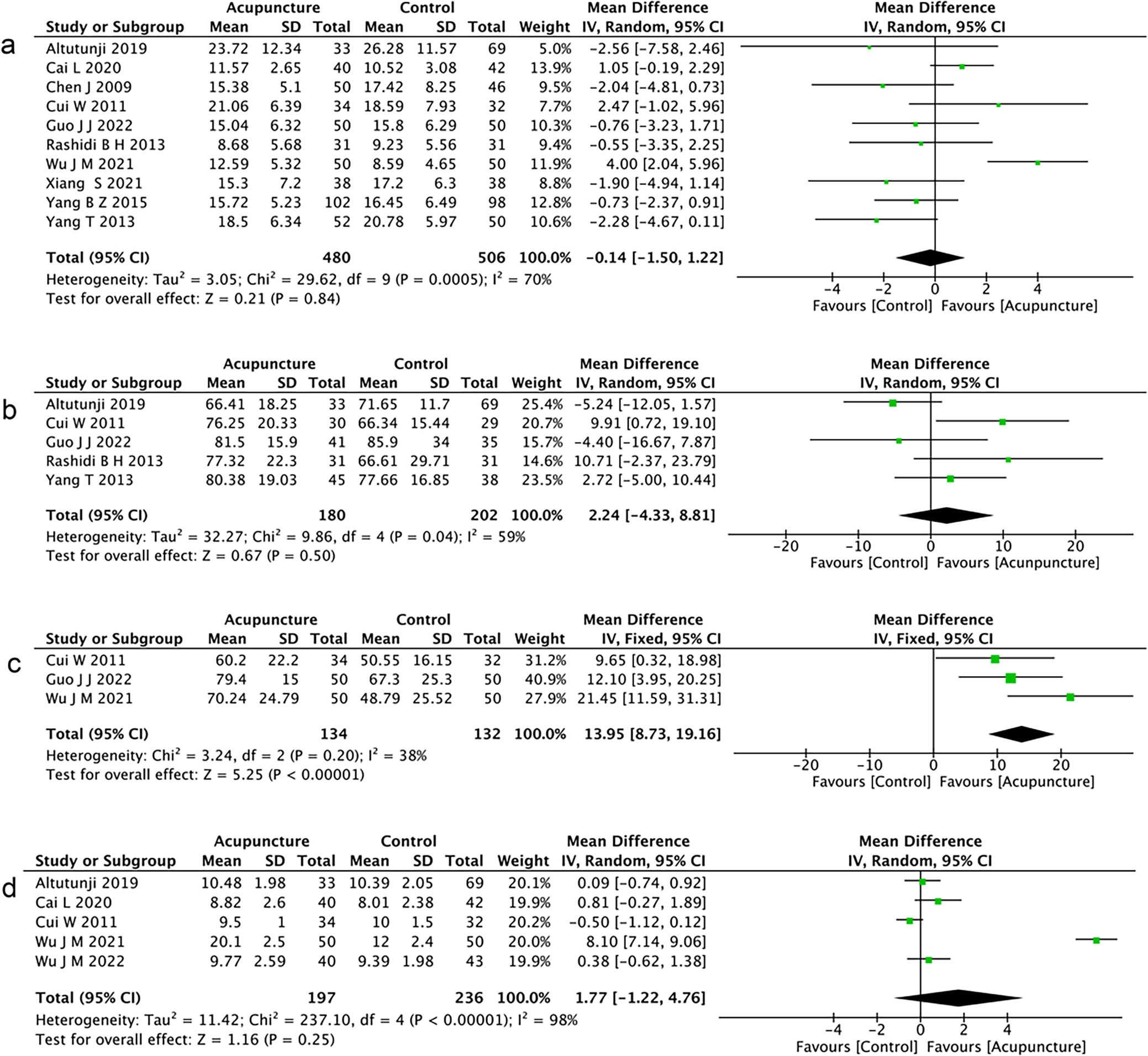
The data from these three studies (Refs Reference Li15, Reference Altutunji, Liu, Cai, Wang and Gao16, Reference Xing, Liu and Dong27) showed a higher oocyte yield with acupuncture, the remaining seven (Refs Reference Cui, Li, Sun and Wen18–Reference Xiang, Xia, Song, Liu and Lian21, Reference Rashidi, Tehrani, Hamedani and Pirzadeh24–Reference Yang, Cui and Li26) indicated no intergroup difference, resulting in no overall effect in our meta-analysis. (WMD -0.14; 95%CI: −1.50 to 1.22; P = 0.84; I 2 = 70%, Figure 6A).
Forest plots for meta-analysis of acupuncture among women with PCOS undergoing IVF-ET. Forest plot for (A) number of oocytes retrieved; (B) fertilization rate; (C) high-quality embryo rate; and (D) number of thickness of endometrium.

Fertilization rate
Five studies (Refs Reference Altutunji, Liu, Cai, Wang and Gao16, Reference Cui, Li, Sun and Wen18, Reference Xiang, Xia, Song, Liu and Lian21, Reference Rashidi, Tehrani, Hamedani and Pirzadeh24, Reference Yang, Cui and Li26) reported fertilization rate. The two groups showed comparable fertilization rates, with no significant difference (WMD 2.24; 95%CI: −4.33 to 8.81; P = 0.50; I 2 = 59%, Figure 6B).
High-quality embryo rate
Three included studies (Refs Reference Altutunji, Liu, Cai, Wang and Gao16, Reference Yang, Cui and Li26, Reference Xing, Liu and Dong27) provided data on the rates of high-quality embryos for both the acupuncture group and the control group. Our study showed a significant increase in the high-quality embryo rate favouring the acupuncture group (WMD 13.95; 95%CI: 8.73 to 19.16; P < 0.001; I 2 = 38%, Figure 6C).
Thickness of endometrium
According to our analysis, only one study (Ref. Reference Yang25) showed a significant difference in endometrial thickness between the acupuncture group and the control group. No statistically significant difference in endometrial thickness was found in our study of five RCTs (Refs Reference Altutunji, Liu, Cai, Wang and Gao16, Reference Cui, Li, Sun and Wen18, Reference Wu, Zhuo and Tang19, Reference Cai, Li, Zhao, Liu, Yan and Tong28, Reference Wu, Ning, Ye, Liu, Tang, Hu and Zhuo29) (WMD 1.77; 95%CI: −1.22 to 4.76; P = 0.25; I 2 = 98%, Figure 6D). Significant heterogeneity was detected among the study data.
Levels of P, LH and E2
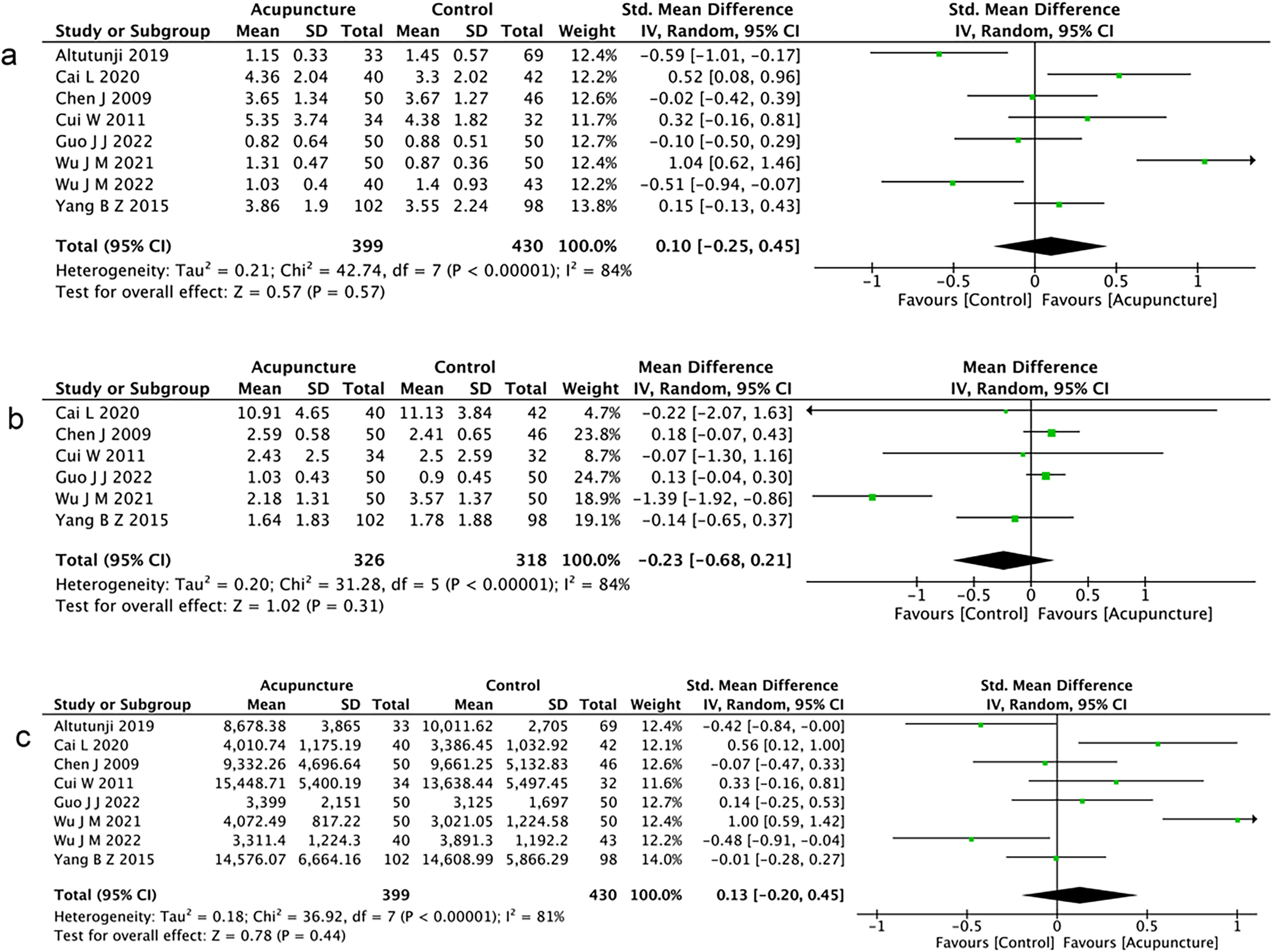
We analysed the effect of acupuncture on hormone parameters on the trigger day of HCG administration. Eight RCTs (Refs Reference Li15, Reference Altutunji, Liu, Cai, Wang and Gao16, Reference Ajeena, Al-Haris and Al-Kefae20, Reference Rashidi, Tehrani, Hamedani and Pirzadeh24–Reference Cai, Li, Zhao, Liu, Yan and Tong28) were included in our analysis for P levels, indicating no significant difference between the two groups (WMD 0.10; 95%CI: −0.25 to 0.45; P = 0.57; I 2 = 84%, Figure 7A).
Forest plots for meta-analysis of acupuncture among women with PCOS undergoing IVF-ET. Forest plot for (A) P level, (B) LH level, and (C) E2 level.

Six studies (Refs Reference Li15, Reference Altutunji, Liu, Cai, Wang and Gao16, Reference Ajeena, Al-Haris and Al-Kefae20, Reference Yang25–Reference Xing, Liu and Dong27) reported LH level, and no significant differences were found between the acupuncture and control groups (WMD −0.23; 95%CI: −0.68 to 0.21; P = 0.31; I 2 = 84%, Figure 7B).
Eight studies (Refs Reference Li15, Reference Altutunji, Liu, Cai, Wang and Gao16, Reference Ajeena, Al-Haris and Al-Kefae20, Reference Rashidi, Tehrani, Hamedani and Pirzadeh24–Reference Cai, Li, Zhao, Liu, Yan and Tong28) compared E2 levels among women with PCOS undergoing IVF-ET treatment between the acupuncture group and control groups. Acupuncture therapy showed similar results to no-acupuncture therapy (WMD 0.13; 95%CI: −0.20 to 0.45; P = 0.44; I 2 = 81%, Figure 7C).
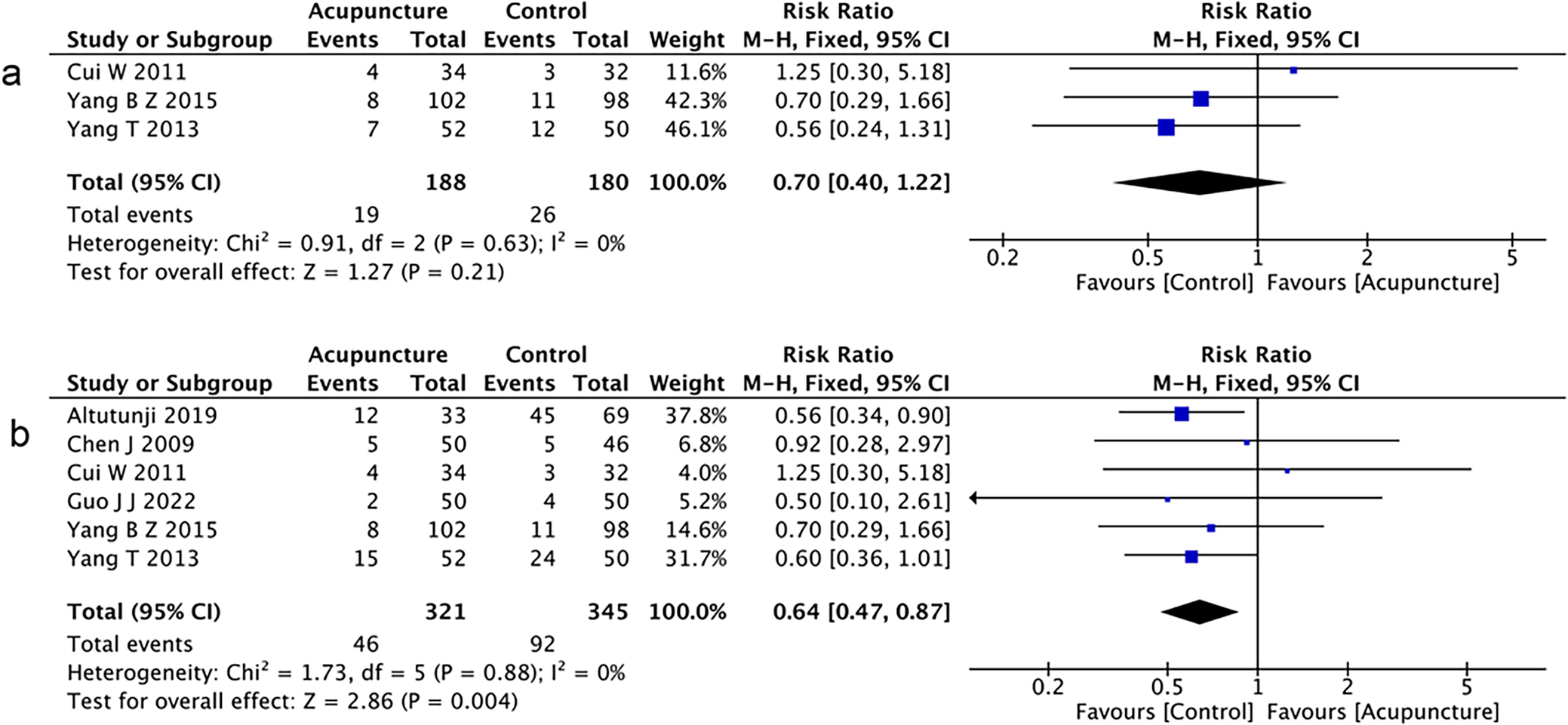
Cycle cancellation rate
As an index of adverse effects, three RCTs (Refs Reference Altutunji, Liu, Cai, Wang and Gao16, Reference Ajeena, Al-Haris and Al-Kefae20, Reference Xiang, Xia, Song, Liu and Lian21) reported the cycle cancellation rate. The analysis revealed no difference in cycle cancellation rate between the two groups of women with PCOS (RR 0.7; 95% CI: 0.4 to 1.22; P = 0.21; I 2 = 0%, Figure 8A).
Forest plots for meta-analysis of acupuncture among women with PCOS undergoing IVF-ET. Forest plot for (A) cycle cancellation rate and (B) OHSS.

Number of OHSS
Six studies (Refs Reference Altutunji, Liu, Cai, Wang and Gao16, Reference Ajeena, Al-Haris and Al-Kefae20, Reference Xiang, Xia, Song, Liu and Lian21, Reference Rashidi, Tehrani, Hamedani and Pirzadeh24–Reference Yang, Cui and Li26) involving 666 patients were included in the analysis. It showed a significant trend for acupuncture to decrease the occurrence of OHSS in PCOS women (RR 0.64; 95%CI: 0.47 to 0.87; P = 0.004; I 2 = 0%, Figure 8B).
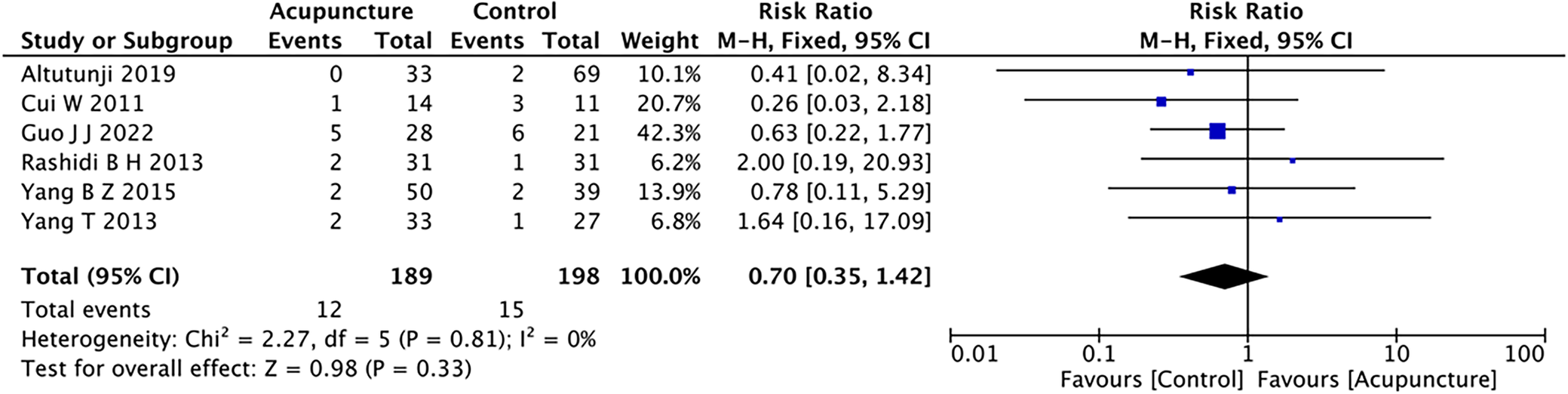
Miscarriage rate
Six studies (Refs Reference Altutunji, Liu, Cai, Wang and Gao16, Reference Cui, Li, Sun and Wen18, Reference Ajeena, Al-Haris and Al-Kefae20, Reference Xiang, Xia, Song, Liu and Lian21, Reference Rashidi, Tehrani, Hamedani and Pirzadeh24, Reference Yang, Cui and Li26) reported miscarriage rates, with one study (Ref. Reference Altutunji, Liu, Cai, Wang and Gao16) including both spontaneous miscarriage and ectopic pregnancy rates. Our meta-analysis demonstrated a lower miscarriage rate in the acupuncture group compared to controls, though this difference did not reach statistical significance (RR 0.7; 95%CI: 0.35 to 1.42; P = 0.33; I 2 = 0%, Figure 9).
Forest plot of the miscarriage rate for meta-analysis of acupuncture among women with PCOS undergoing IVF-ET.

Discussion
Our study included a total of 1,023 participants from 13 RCTs. We investigated the effectiveness of acupuncture therapy for PCOS patients receiving IVF-ET. Our study showed that acupuncture therapy could increase both the live birth rate and clinical pregnancy rate. Additionally, a statistically significant increase in good-quality embryo rate was observed with acupuncture compared with the control intervention. Acupuncture also reduced the dose and duration of Gn used during stimulation. Furthermore, it indicated that acupuncture decreased the occurrence of OHSS in PCOS patients undergoing IVF-ET.
Traditional Chinese medicine has a long history of application in the field of reproduction. Acupuncture, as one of the traditional therapies, has been applied in the treatment of infertility for thousands of years. Acupuncture may improve pregnancy outcome by regulating the hypothalamic–pituitary-ovary axis, improving endometrial and ovarian blood flow and changing the endometrial environment and so on (Refs Reference Chen, Tang, Liang, Wu, Xie, Ding, Yang, Long and Lin30–Reference Ouyang, Gao and Che35).
An RCT was conducted to assess whether transcutaneous electrical nerve stimulation (TENS) affects endometrial thickness, with results indicating a positive effect in a cohort of healthy women (Ref. Reference Ajeena, Al-Haris and Al-Kefae20). Xiang Shan et al. found that electroacupuncture in patients with insulin-resistant PCOS could improve oocyte and embryo quality, potentially through upregulation of the IRS-1/PI3K/GLUT4 pathway (Ref. Reference Xiang, Xia, Song, Liu and Lian21).Chen et al. performed an experimental study by rat models, and found that acupuncture treatment could downregulate LncMEG3, inhibit PI3K/AKT/mTOR signalling, and thereby attenuate granulosa cell autophagy while promoting proliferation (Ref. Reference Chen, Tang, Liang, Wu, Xie, Ding, Yang, Long and Lin30).A miRNA sequencing analysis of endometrial samples from infertile women revealed that acupuncture treatment potentially enhanced endometrial receptivity by modulating ADCY2 gene activity, thereby activating downstream cAMP signalling cascades (Ref. Reference Mu, Li, Cheng, Shen, Jin, Xie, Gao, Zhang, Hua, Xia, Gao and Xia31).Collectively, these findings indicate that acupuncture may enhance the endometrial and ovarian microenvironment, promoting smoother ovulation and ultimately improving live birth and clinical pregnancy outcomes.
In 2023, Xu et al. conducted low-frequency electro-acupuncture at PCOS rats’ Guan Yuan acupoint (CV4), revealed that intervention lowered serum levels of testosterone and LH, while also reducing GnRH, kisspeptin and dynorphin levels in the hypothalamic arcuate nucleus (Ref. Reference Xu, Zhao, Li, Hu, Li, Li and Chen32). Ma et al. found that Low-frequency electro-acupuncture performed at the ‘Sanyinjiao’ (ST29) and ‘Guilai’ (SP6) acupoints can promoted angiogenesis in ovarian and neovascularization around antral follicles, it indicated that acupuncture may affect ovulation by affecting ovarian angiogenesis (Ref. Reference Ma, Cui, Tong, Hu, Shao, Zhang, Li and Feng33). This suggests that acupuncture may improve the ovarian microenvironment and enhance ovarian sensitivity to Gn, thereby reducing the dose and duration of Gn used during stimulation.
Our results showed that acupuncture significantly decreased OHSS occurrence in ART cycles. OHSS clinical symptoms are caused by vascular hyperpermeability, primarily mediated by vascular endothelial growth factor (VEGF) (Ref. Reference Palomba, Costanzi, Nelson, Caserta and Humaidan34). Research evidence indicates that acupuncture intervention effectively decreases VEGF concentrations in peripheral circulation and synovial membranes among rheumatoid arthritis patients (Ref. Reference Ouyang, Gao and Che35). Therefore, this may be the reason for the lower OHSS incidence in the acupuncture group.
Our results are inspiring and provide strong evidence supporting the benefits of acupuncture for PCOS patients receiving IVF-ET. Currently, there is limited evidence from both individual studies and meta-analyses on the efficacy of acupuncture in improving assisted reproductive outcomes in PCOS patients. Our study, however, provided a comprehensive and up-to-date summary of acupuncture’s clinical application in this context. Notably, among the included studies, nine were published in the Chinese language. Given that the majority of acupuncture interventions for PCOS are conducted in China, the incorporation of these studies enhances the reliability and clinical relevance of our findings. Our study compiled clinical research on acupuncture for PCOS patients from multiple databases, providing statistical analysis on various outcomes, including clinical pregnancy rate, live birth rate and high-quality embryo rate.
However, our study has limitations concerning statistical and clinical heterogeneity. The criteria for diagnosing PCOS varied between studies, the participants were not identical and the application of acupuncture therapy was not uniform. Studies also lack subgroup analysis due to the heterogeneity of each study. Additionally, the eligible RCTs were conducted in Asian countries, and the relevance of our results to other populations requires further investigation.
Conclusion
Based on this meta-analysis, traditional Chinese acupuncture therapy appears to be an effective supportive treatment for women with PCOS undergoing IVF-ET. It can increase both live birth rate and clinical pregnancy rate, improve embryo quality and simultaneously reduce the dosage and duration of Gn. Additionally, acupuncture therapy may decrease the incidence of OHSS, with a similar cancellation rate compared to the non-acupuncture group. However, due to limitations in the current evidence, there is an urgent need for extensive, well-designed, high-quality randomized clinical trials to provide more reliable evidence supporting the application of traditional Chinese medicine in ART.
Supplementary material
The supplementary material for this article can be found at http://doi.org/10.1017/erm.2026.10048.
Funding statement
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Competing interests
None.



 Open access
Open access