


Introduction
Health technology assessment (HTA) is defined as “a multidisciplinary process that uses explicit methods to determine the value of a health technology at different points in its lifecycle. The purpose of HTA is to inform decision making in order to promote an equitable, efficient, and high-quality health system” (Reference O’Rourke, Oortwijn and Schuller1). In January 2025, the European Union HTA Regulation (EU HTAR) entered into force, which aims to create a harmonized HTA framework, foster member state cooperation, and enhance equal patient access to innovative health technologies (2). However, implementation of the EU HTAR increases pressure on EU HTA organizations to perform joint clinical assessments of innovative health technologies (Reference Desmet, Brijs and Vanderdonck3).
Many HTA organizations in the EU have concerns about the lack of capacity in their organizations to perform joint assessments. Capacity building is seen as one of the primary barriers to actively implementing the EU HTAR by different stakeholders involved in HTA (Reference Desmet, Brijs and Vanderdonck3). Capacity building for HTA includes a process by which individuals and organizations develop or strengthen competencies, such as understanding, providing input to, conducting, or utilizing HTA for health policy and decision making via education and training, as well as developing awareness and support in the environment within which HTA is used (Reference Pichler, Oortwijn, Ruether and Trowman4).
To guide capacity building, the use of a competency framework might be valuable as it describes competencies, which are the ability of a person to integrate knowledge, skills, and attitudes in their performance of tasks (Reference Mills, Middleton and Schafer5;Reference Gwaza, Chemwolo, Musonda, Kuwana and Dube6). A competency framework can provide guidance in workforce development, training and learning, credentialing, and assessment. In this way, it can provide an effective way to assess, monitor, and increase the knowledge and skills of professionals, which emphasizes the importance of updating competency frameworks regularly (Reference Green, Forssman and Marcil7).
Currently, competencies for HTA professionals are described in the validated, comprehensive competency framework developed by Mueller et al. (Reference Mueller, Gutierrez-Ibarluzea, Chiumente and Oortwijn8). It contains an overview of competencies grouped in the main HTA domains, based on the HTA Core Model. These are health problem and current use of the technology, description and technical characteristics, safety, clinical effectiveness, costs and economic evaluation, ethical analysis, organizational aspects, patient and social aspects, and legal aspects (Reference Mueller, Gutierrez-Ibarluzea, Chiumente and Oortwijn8). The existing framework also includes competencies related to the HTA process, which are introduction to HTA, prioritization, scoping, synthesis of evidence, dissemination, stakeholder engagement, and communication and others. This competency framework is used in practice, for instance, in developing HTA training materials (Reference Migliore, Mueller and Oortwijn9) and context-specific HTA competency frameworks (Reference Dixon, Tyagi and Singh10;Reference Refolo, Bond and Bloemen11).
However, the current competency framework was published in 2020, and as mentioned by Mueller et al. (Reference Mueller, Gutierrez-Ibarluzea, Chiumente and Oortwijn8) themselves, new competencies emerge quickly in the HTA field. For example, a competency related to the assessment of environmental aspects may be added to the competency framework (Reference Mueller, Gutierrez-Ibarluzea, Chiumente and Oortwijn8). Other competencies may also have become more important or emerged in the years after developing the original framework. Therefore, this study aimed to identify new competencies and competency domains described in the literature and to update and verify the competency framework of Mueller et al. (Reference Mueller, Gutierrez-Ibarluzea, Chiumente and Oortwijn8).
The research described in this article is part of the Support Utilization of Sustainable and TAilored INnovative methods for HTA (SUSTAIN-HTA) coordination and support action, which is a European initiative aimed to support the pan-European HTA workforce and align HTA expertise via a robust education and training framework. SUSTAIN-HTA encourages the uptake of new methodologies that address important HTA needs. By doing so, it aims to build HTA capacity to address the needs of EU HTA organizations (12).
Methods
Scoping review
Scientific literature search
We followed the Arksey & O’Malley framework (Reference Arksey and O’Malley13) and PRISMA-ScR guidelines (Reference Tricco, Lillie and Zarin14) for executing and reporting the scoping review. The PRISMA-ScR checklist is provided in Supplementary Table S1. The protocol of the scoping review was registered prospectively on OpenScienceFramework: https://doi.org/10.17605/OSF.IO/S5Q7K and executed accordingly.
The search strategy was developed together with an information specialist of Radboud University and was inspired by the search terms used in Mueller et al. (Reference Mueller, Gutierrez-Ibarluzea, Chiumente and Oortwijn8). The search was performed in the databases PubMed, Embase, PsycINFO, ERIC, CINAHL, and Web of Science. Supplementary Table S2 presents the search strategies for the respective databases. The search date was from 1 January 2018 to 13 May 2024, with 1 year overlap with the search period of Mueller et al. (Reference Mueller, Gutierrez-Ibarluzea, Chiumente and Oortwijn8) from 2016 to 2019, to identify new documents.
Records were uploaded in Rayyan for screening (Reference Ouzzani, Hammady, Fedorowicz and Elmagarmid15). Table 1 presents the inclusion and exclusion criteria that were used for title/abstract and full-text screening, based on key articles (Reference Mueller, Gutierrez-Ibarluzea, Chiumente and Oortwijn8;Reference Refolo, Bond and Bloemen11;Reference Pizzi, Onukwugha, Corey, Albarmawi and Murray16;Reference Bidonde, Meneses-Echavez and Asare17).
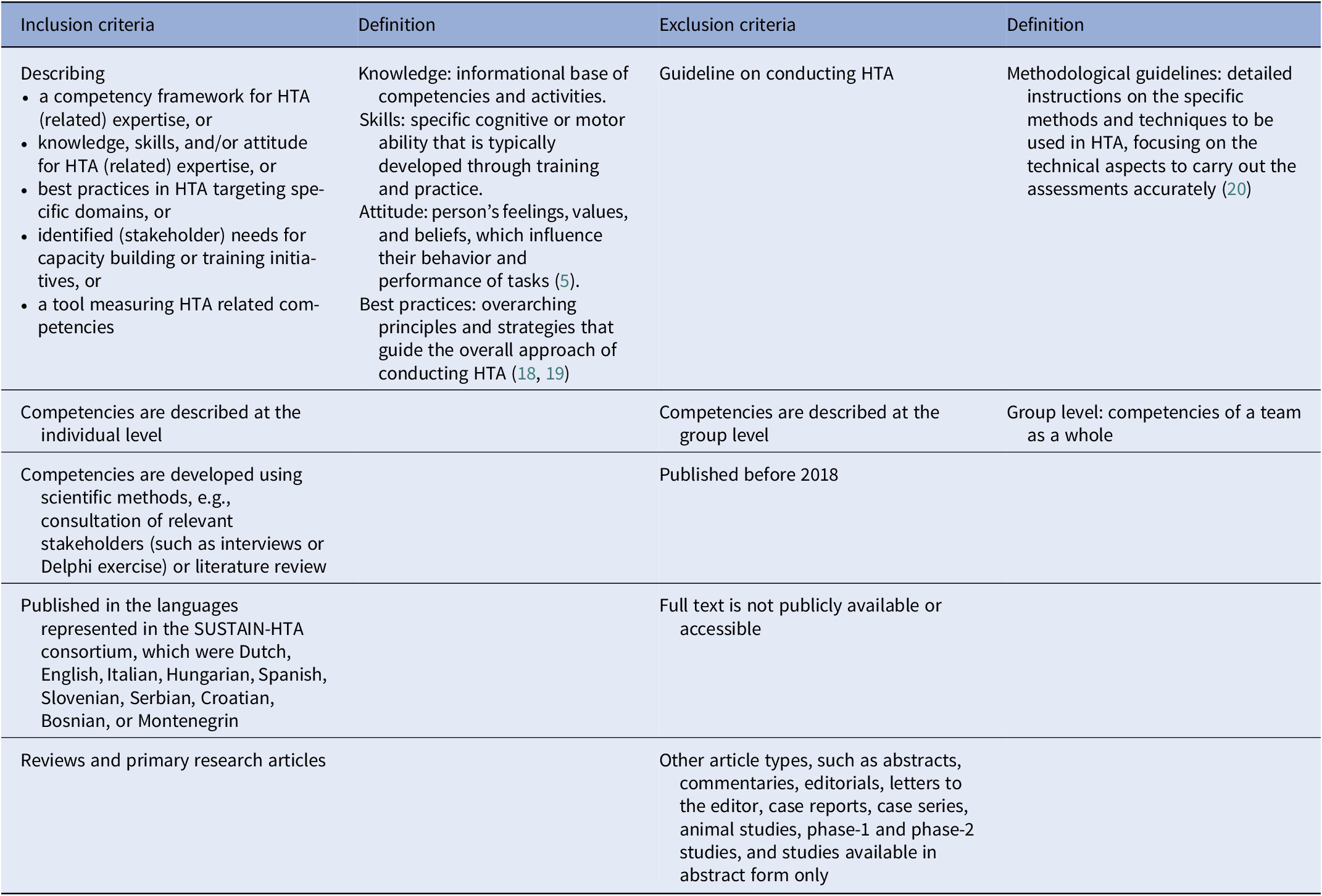
Inclusion and exclusion criteria, including definitions based on (Reference Mills, Middleton and Schafer5, Reference Bertram, Dhaene and Tan-Torres Edejer18–Reference Brinkhuis, Julian and van den Ham20), for the title/abstract and full text screening

Table 1. Long description
The table has four columns: Inclusion criteria, Definition, Exclusion criteria, and Definition. The first row lists inclusion criteria as describing a competency framework for H T A expertise, knowledge, skills, attitude, best practices, stakeholder needs, or tools measuring H T A competencies. The definition column explains knowledge as the informational base, skills as abilities developed through training, attitude as values and beliefs, and best practices as overarching principles. The corresponding exclusion criterion is guideline on conducting H T A, defined as methodological guidelines with detailed instructions on technical aspects. The second row includes individual-level competencies as inclusion and group-level competencies as exclusion, with group level defined as competencies of a team. The third row includes competencies developed using scientific methods as inclusion and studies published before 2018 as exclusion. The fourth row includes publications in SUSTAIN-H T A consortium languages as inclusion and inaccessible full texts as exclusion. The fifth row includes reviews and primary research articles as inclusion and other article types, such as abstracts, commentaries, editorials, letters, case reports, case series, animal studies, phase-1 and phase-2 studies, and studies available in abstract form only as exclusion. Abbreviations are defined below the table: H T A is health technology assessment, SUSTAIN-H T A is support utilization of sustainable and tailored innovative methods for H T A.
HTA, health technology assessment; SUSTAIN-HTA, Support Utilization of Sustainable and TAilored INnovative methods for HTA.
Two authors (LvM and WK or WO) independently performed title/abstract and full text screening. Conflicts in decisions were resolved by consensus, with reconciliation by a third reviewer (WK or WO) when necessary. One reviewer (LvM) checked the references of articles included in this scoping review and checked citations of the article by Mueller et al. (Reference Mueller, Gutierrez-Ibarluzea, Chiumente and Oortwijn8).
Gray literature search
One reviewer (LvM) searched websites of HTA-related societies, which were HTA International (HTAi), Drug Information Association (DIA), International Society for Priority Setting in Health (ISPH), Society for Medical Decision Making (SMDM), International Health Economics Association (IHEA), International Society for Quality of Life Research (ISOQoL), International Society for Pharmacoeconomics and Outcomes Research (ISPOR), European Health Economics Association (EUHEA), International Society for Pharmaceutical Engineering (ISPE), International Society of Pharmacoepidemiology (ISPE), and European Public Health Association (EUPHA), using the terms “health technology assessment”, “competencies”, and “competences”. Additionally, webpages related to resources and education, as well as special interest group webpages and their reports, were searched for HTA competency frameworks and HTA core courses. Furthermore, Google was searched using the society name, in combination with the terms “core courses”, “competencies”, and “capacity building”, and the first ten results for each combination were reviewed. One reviewer (LvM) checked the documents and website pages using the inclusion and exclusion criteria described in Table 1 on 22 April 2024.
Data extraction
Data extraction were performed using a standardized Microsoft Excel spreadsheet. Two authors (LvM and WO) performed a pilot test using three included documents (Reference Low, André-Vert, Fanelli and Galbraith21–Reference Wu, Chen, Wang, Jian and Ko23) to improve extractor reliability and ensure accuracy of the data extraction form and extracted data. One author (LvM) completed data extraction of the following items: author(s), year of publication, title, country of origin, organizations involved, population (doers or users of HTA and which role they have in the HTA process), stages of the HTA process based on Mueller et al. (Reference Mueller, Gutierrez-Ibarluzea, Chiumente and Oortwijn8), methods used to develop the framework or tool, if and how competencies were described, HTA Core Model domains covered, conflicts of interest, and funding source. Any doubts regarding data extraction were discussed within the research team.
Content analysis
One author (LvM) mapped the competencies identified in the scoping review against those from the original competency framework to verify the original competencies, using deductive content analysis in Atlas.ti 24.0.0 for Windows (ATLAS.ti Scientific Software Development GmbH) (Reference Braun and Clarke24). When a competency did not match one of the competencies of Mueller et al. (Reference Mueller, Gutierrez-Ibarluzea, Chiumente and Oortwijn8), this was marked with a new code (Reference Elo and Kyngäs25), which was used to identify potential new competencies. The mapping and coding outcomes were discussed between the authors (LvM, WO, WK) and potential new HTA competencies and competency domains were determined after several rounds of discussion.
Results
Scoping review
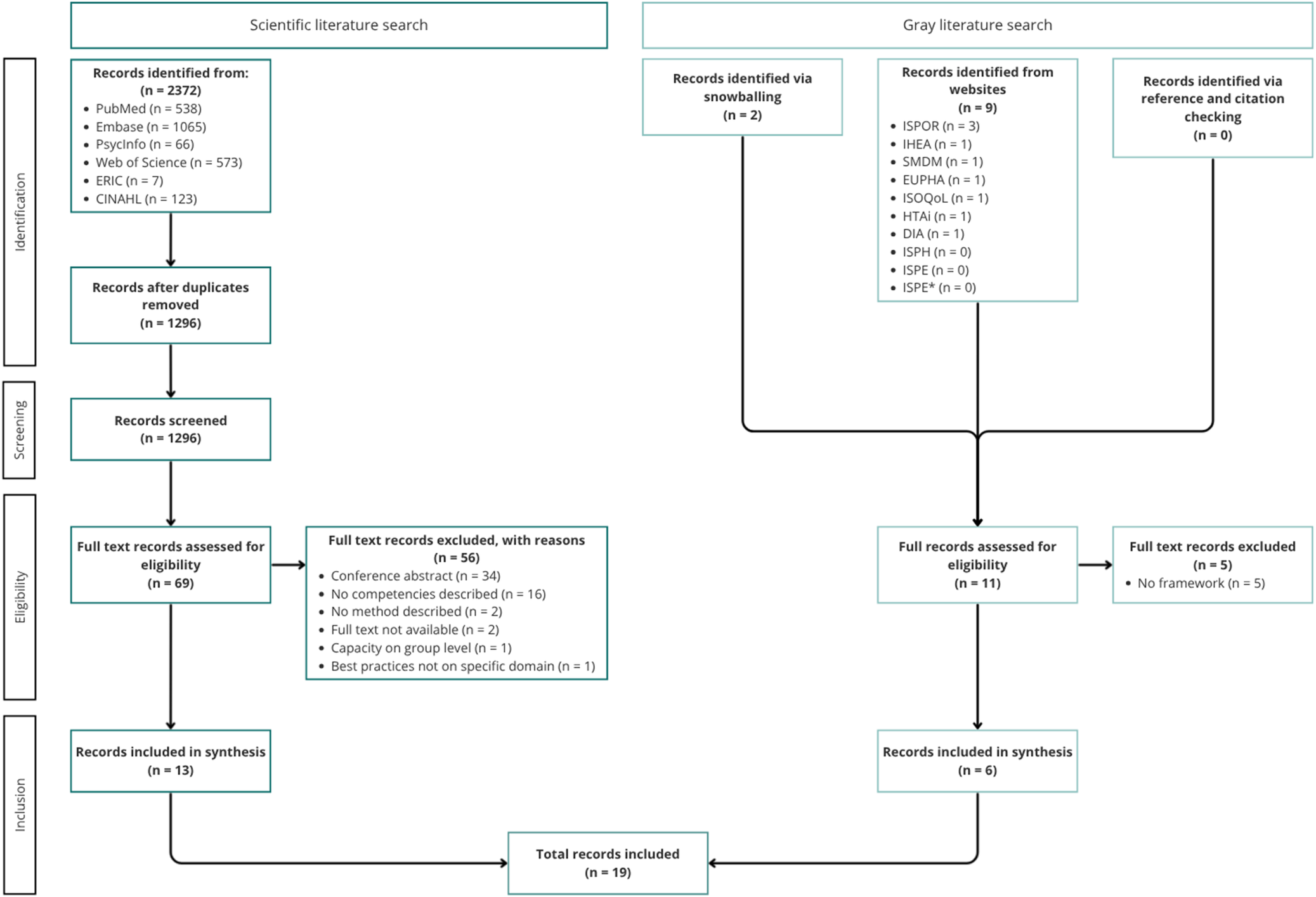
In our scoping review, we identified scientific and gray literature describing competencies for HTA expertise. Figure 1 presents the PRISMA flowchart of the search. The systematic literature search resulted in 1296 articles after removing duplicates, of which 69 articles were initially selected based on title and abstract screening. After reading the full text, thirteen articles were included and fifty-six articles were excluded; see Supplementary Table S3 for exclusion reasons. One author was contacted to retrieve the full text of an article, but no response was received, which resulted in exclusion of the article. Another author was contacted to retrieve the methods used for the competency framework development, which were sent by email. The gray literature search resulted in the initial identification of eleven documents, of which nine were identified using the search and two were identified via snowballing. After reading the full documents, six documents were included and five were excluded; see Supplementary Table S3 for exclusion reasons. Reference and citation checking of Mueller et al. (Reference Mueller, Gutierrez-Ibarluzea, Chiumente and Oortwijn8) resulted in no additional articles. A total of nineteen documents (Reference Dixon, Tyagi and Singh10;Reference Refolo, Bond and Bloemen11;Reference Pizzi, Onukwugha, Corey, Albarmawi and Murray16;Reference Bidonde, Meneses-Echavez and Asare17;Reference Low, André-Vert, Fanelli and Galbraith21–Reference Wu, Chen, Wang, Jian and Ko23;Reference Abraham, Kvamme and Magrin Sammut26–Reference Zemplényi, Tachkov and Balkanyi37) describing competencies for HTA expertise were included.
PRISMA flowchart of the scoping review. ISPOR: International Society for Pharmacoeconomics and Outcomes Research, IHEA: International Health Economics Association, SMDM: Society for Medical Decision Making, EUPHA: European Public Health Association, ISOQoL: International Society for Quality of Life Research, HTAi: Health Technology Assessment International, DIA: Drug Information Association, ISPH: International Society for Priority Setting in Health, ISPE: International Society for Pharmaceutical Engineering, ISPE*: International Society of Pharmacoepidemiology.

Figure 1. Long description
At the top, two main branches represent scientific literature search and graey literature search. The scientific literature search starts with records identified from six sources: PubMed 538, Embase 1065, PsycInfo 66, Web of Science 573, E R I C 7, and C I N A H L 123, totaling 2372. After removing duplicates, 1296 records remain. These are screened, with 69 full text records assessed for eligibility. Of these, 56 are excluded for reasons: conference abstract 34, no competencies described 16, no method described 2, full text not available 2, capacity on group level 1, best practices not on specific domain 1. Thirteen records are included in synthesis. The gray literature search includes records identified via snowballing 2, from websites 9 (I S P O R 3, I H E A 1, S M D M 1, E U P H A 1, I S O Q O L 1, H T A I 1, D I A 1, I S P H 0, I S P E 0, I S P E star 0), and via reference and citation checking 0. Eleven full records are assessed for eligibility, with five excluded for no framework. Six records are included in synthesis. Both branches converge at the bottom, showing a total of 19 records included.
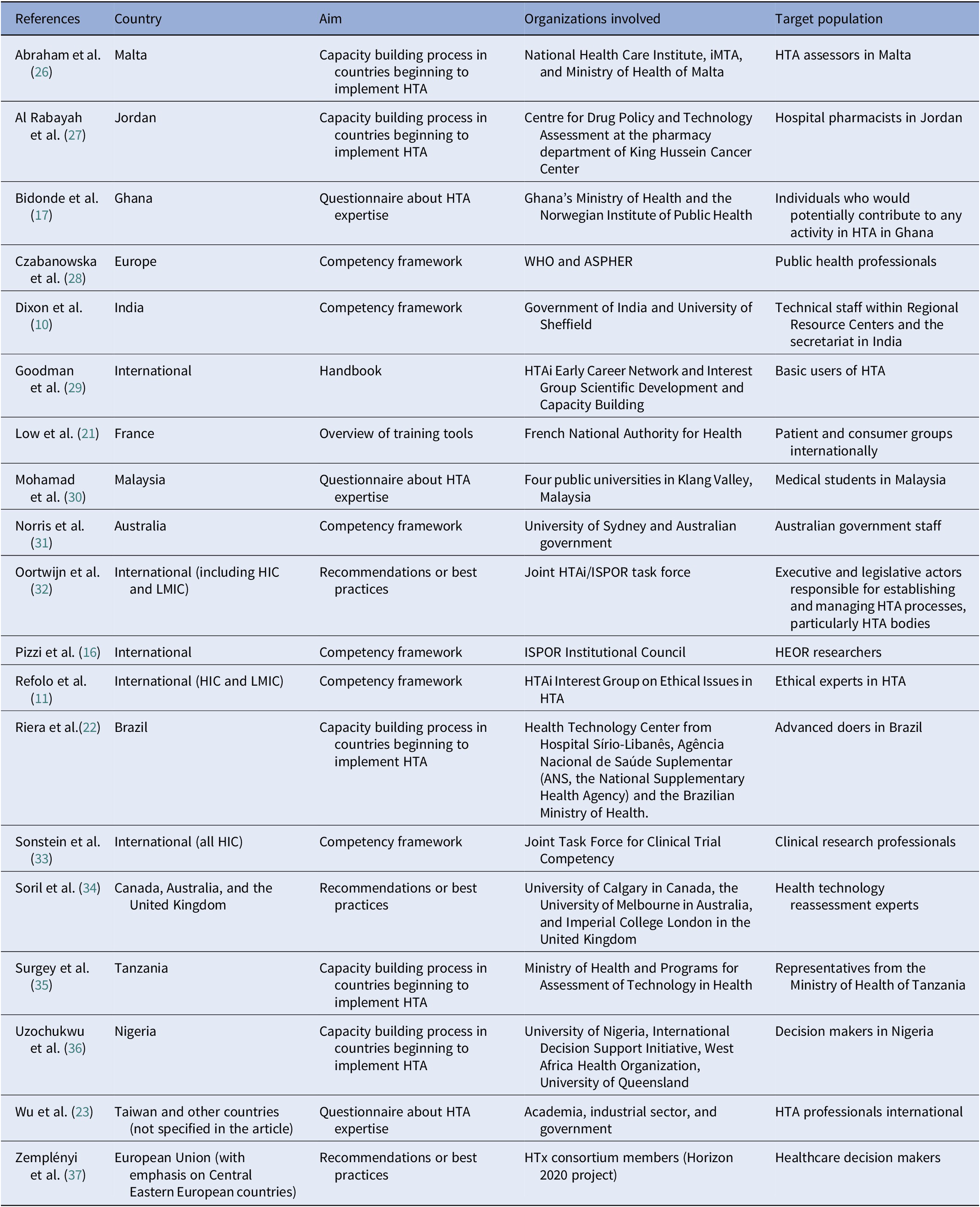
Six competency frameworks, one handbook, and twelve scientific articles describing knowledge, skills, and attitudes for HTA expertise were identified. Table 2 presents the main characteristics of the documents and a detailed overview is provided in Supplementary Table S4. Most documents were developed with representatives from countries across several continents (n = 6) or from Europe (n = 4). Academia (n = 10) and national government organizations (n = 8) were the most frequently involved organizations, and target populations mostly included HTA professionals (n = 5) or decision makers (n = 5).
Main characteristics of the identified documents describing competencies for HTA expertise

Table 2. Long description
The table contains 18 rows, each representing a document on HTA competencies. Columns are References, Country, Aim, Organizations involved, and Target population. From the top row: Abraham et al. 26, Malta, capacity building process in countries beginning to implement HTA, National Health Care Institute, i M T A, and Ministry of Health of Malta, HTA assessors in Malta. Al Rabayah et al. 27, Jordan, capacity building process in countries beginning to implement HTA, Centre for Drug Policy and Technology Assessment at the pharmacy department of King Hussein Cancer Center, hospital pharmacists in Jordan. Bidonde et al. 17, Ghana, questionnaire about HTA expertise, Ghana's Ministry of Health and the Norwegian Institute of Public Health, individuals who would potentially contribute to any activity in HTA in Ghana. Czabanowska et al. 28, Europe, competency framework, W H O and A S P H E R, public health professionals. Dixon et al. 10, India, competency framework, Government of India and University of Sheffield, technical staff within Regional Resource Centers and the secretariat in India. Goodman et al. 29, International, handbook, HTAi Early Career Network and Interest Group Scientific Development and Capacity Building, basic users of HTA. Low et al. 21, France, overview of training tools, French National Authority for Health, patient and consumer groups internationally. Mohamad et al. 30, Malaysia, questionnaire about HTA expertise, four public universities in Klang Valley, Malaysia, medical students in Malaysia. Norris et al. 31, Australia, competency framework, University of Sydney and Australian government, Australian government staff. Oortwijn et al. 32, International including H I C and L M I C, recommendations or best practices, Joint HTAi forward slash I S P O R task force, executive and legislative actors responsible for establishing and managing HTA processes, particularly HTA bodies. Pizzi et al. 16, International, competency framework, I S P O R Institutional Council, H E O R researchers. Refolo et al. 11, International H I C and L M I C, competency framework, HTAi Interest Group on Ethical Issues in HTA, ethical experts in HTA. Riera et al. 22, Brazil, capacity building process in countries beginning to implement HTA, Health Technology Center from Hospital Sirio-Libanes, A N S the National Supplementary Health Agency and the Brazilian Ministry of Health, advanced doers in Brazil. Sonstein et al. 33, International all H I C, competency framework, Joint Task Force for Clinical Trial Competency, clinical research professionals. Soril et al. 34, Canada, Australia, and the United Kingdom, recommendations or best practices, University of Calgary in Canada, the University of Melbourne in Australia, and Imperial College London in the United Kingdom, health technology reassessment experts. Surgey et al. 35, Tanzania, capacity building process in countries beginning to implement HTA, Ministry of Health and Programs for Assessment of Technology in Health, representatives from the Ministry of Health of Tanzania. Uzochukwu et al. 36, Nigeria, capacity building process in countries beginning to implement HTA, University of Nigeria, International Decision Support Initiative, West Africa Health Organization, University of Queensland, decision makers in Nigeria. Wu et al. 23, Taiwan and other countries not specified in the article, questionnaire about HTA expertise, academia, industrial sector, and government, HTA professionals international. Zemplenyi et al. 37, European Union with emphasis on Central Eastern European countries, recommendations or best practices, HTx consortium members Horizon 2020 project, healthcare decision makers. Table footnotes define abbreviations: A N S, Ag ê ncia Nacional de Sa ú de Suplementar the National Supplementary Health Agency; A S P H E R, Association of Schools of Public Health in the European Region; H E O R, Health Economics and Outcomes Research; H I C, high-income country; HTA, health technology assessment; HTAi, health technology assessment international; i M T A, Institute for Medical Technology Assessment; I S P O R, Professional Society for Health Economics and Outcomes Research; L M I C, low-and middle-income country; W H O, World Health Organization.
ANS, Agência Nacional de Saúde Suplementar (the National Supplementary Health Agency); ASPHER, Association of Schools of Public Health in the European Region; HEOR, Health Economics and Outcomes Research; HIC, high-income country; HTA, health technology assessment; HTAi, health technology assessment international; iMTA, Institute for Medical Technology Assessment; ISPOR, Professional Society for Health Economics and Outcomes Research; LMIC, low-and middle-income country; WHO, World Health Organization.
Content analysis
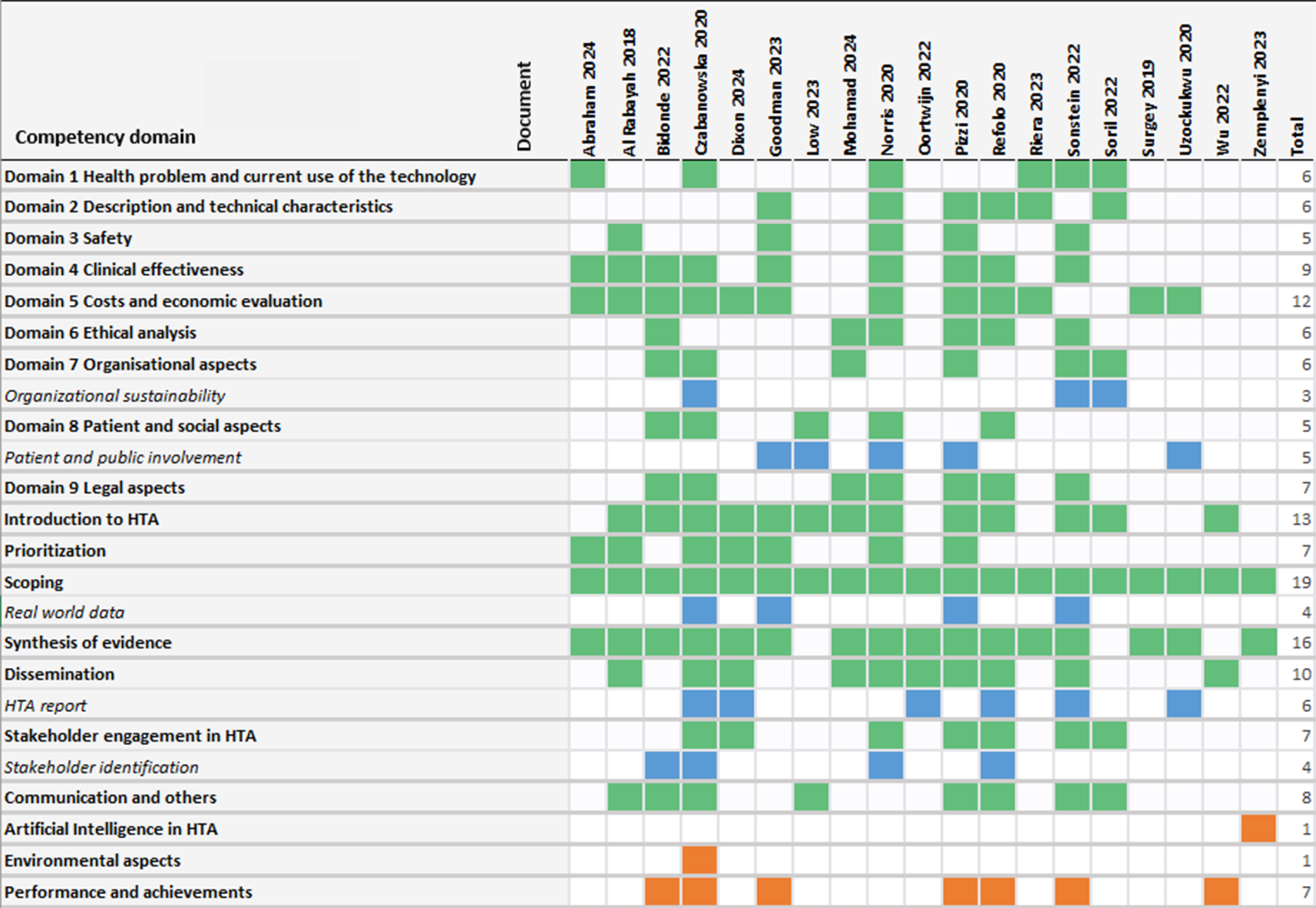
Using deductive content analysis, we compared the competencies for HTA expertise identified in the literature to those listed in the original competency framework of Mueller et al. (Reference Mueller, Gutierrez-Ibarluzea, Chiumente and Oortwijn8). Figure 2 shows the results of the content analysis. The process domain Scoping was represented in all the documents and the domains Synthesis of evidence and Introduction into HTA were also represented in most documents. The domains Safety and Patient and Social aspects were mentioned in the least number of documents. Overall, we found that all original competencies described in the framework by Mueller et al. (Reference Mueller, Gutierrez-Ibarluzea, Chiumente and Oortwijn8) were represented in at least five of the included documents, suggesting a verification that the existing HTA competencies are supported by the current literature.
Mapping results of the competencies described in the identified literature with the domains of the original competency framework. Green sections represent that competencies within this domain are represented in the document. Blue sections indicate the new competencies in the existing domains and orange the new competency domains. HTA: Health Technology Assessment.

Figure 2. Long description
Starting from the top-left, the table lists competency domains vertically and documents horizontally. Each row represents a domain such as Health problem and current use of the technology, Description and technical characteristics, Safety, Clinical effectiveness, Costs and economic evaluation, Ethical analysis, Organisational aspects, Patient and social aspects, Legal aspects, Introduction to H T A, Prioritization, Scoping, Real world data, Synthesis of evidence, Dissemination, H T A report, Stakeholder engagement in H T A, Stakeholder identification, Communication and others, Artificial Intelligence in H T A, Environmental aspects, and Performance and achievements. Each column from left to right is labeled with a document name and year, including Abraham 2024, Al Ibrah 2018, Bidonde 2020, Dabrowska 2020, Dioxon 2024, Goodman 2023, Low 2023, Mohamad 2024, Norris 2024, Oortwijn 2022, Pizzi 2020, Rehbo 2020, Riee 2023, Soinne 2023, Sun 2021, Uzochukwu 2020, Iwu 2022, and Zemplenyi 2023. Green cells indicate a domain is covered in a document, blue cells indicate subdomains or specific aspects, and orange cells at the bottom highlight unique or less common competencies. The rightmost column totals the number of documents covering each domain, with Synthesis of evidence and Scoping being the most frequently mapped. The table visually demonstrates the distribution and overlap of competencies across the literature.
We identified new competencies that can be included in an existing domain in the original framework. First, we identified the competencies required for interpreting and developing HTA reports, such as full, rapid, and mini HTA reports (Reference Merlin, Tamblyn and Ellery38). It is important that HTA professionals have expertise in this competency because they need to be able to interpret and communicate the results of HTA effectively to different stakeholders. This facilitates the appropriate use of HTA results and effective translation into policy (Reference Dixon, Tyagi and Singh10;Reference Refolo, Bond and Bloemen11;Reference Czabanowska, Shickle and Burazeri28;Reference Oortwijn, Husereau and Abelson32;Reference Sonstein, Namenek Brouwer and Gluck33;Reference Uzochukwu, Okeke and O’Brien36). Second, the competency patient and public involvement were identified, which include considering patient and public views in HTA as well as assessing patient-reported outcomes. This competency is important for HTA professionals as these aspects are increasingly integrated into HTA processes to support decision making (Reference Pizzi, Onukwugha, Corey, Albarmawi and Murray16;Reference Low, André-Vert, Fanelli and Galbraith21;Reference Goodman29;Reference Norris, Huckel Schneider, Howard, Merlin and Elshaug31;Reference Uzochukwu, Okeke and O’Brien36). Furthermore, we identified real-world data as a source of evidence for HTA (Reference Pizzi, Onukwugha, Corey, Albarmawi and Murray16;Reference Czabanowska, Shickle and Burazeri28;Reference Goodman29;Reference Sonstein, Namenek Brouwer and Gluck33) and identification of relevant stakeholders in HTA (Reference Refolo, Bond and Bloemen11;Reference Bidonde, Meneses-Echavez and Asare17;Reference Czabanowska, Shickle and Burazeri28;Reference Norris, Huckel Schneider, Howard, Merlin and Elshaug31) as new competencies. Real-world data (RWD) as a source of evidence for HTA is emerging globally, because an increasing number of health technologies enter the market via pathways with limited or no evidence from randomized clinical trials (RCTs). This requires additional evidence collected, for example, via postmarketing surveillance or RWD sources, to determine its value. There is also an increased interest from HTA organizations in complementing RCTs with RWD, for example, to better understand patient outcomes in practice and how it can inform outcome-based managed entry agreements (Reference Oortwijn, Sampietro-Colom and Trowman39). As the use of RWD comes with its own methodological challenges, such as confounding and missing data, expertise on whether and how this evidence should be considered in HTA is essential. Lastly, the competency of organizational sustainability was identified, which includes affordability, effective use of resources, and especially workforce management. It is important for HTA professionals to interpret and analyze organizational sustainability, as scarcity of resources is increasingly used to guide decisions. For example, policy makers as well as healthcare managers worldwide are requesting evidence on the impact of health technologies on the scarce healthcare workforce performance and workload (Reference Czabanowska, Shickle and Burazeri28;Reference Sonstein, Namenek Brouwer and Gluck33;Reference Soril, Elshaug and Esmail34).
In addition, we identified three new competency domains that are not yet part of the original competency framework. These were artificial intelligence (AI) use in HTA, environmental aspects of health technologies, and performance and achievements of HTA professionals. Competencies related to AI use in HTA involve how to use AI in different parts of the assessment, such as assisting in literature reviews or analyzing data (Reference Zemplényi, Tachkov and Balkanyi37). Competencies on environmental aspects include, for example, describing the importance of identifying environmental determinants in health and the main features of the climate change process (Reference Czabanowska, Shickle and Burazeri28). Lastly, competencies related to performance and achievements enable HTA professionals to successfully perform their jobs and achieve desired results. These include business management, career and personal development, networking, mentoring and teaching, dealing with stress and uncertainty, as well as adhering to scientific principles (Reference Refolo, Bond and Bloemen11;Reference Pizzi, Onukwugha, Corey, Albarmawi and Murray16;Reference Bidonde, Meneses-Echavez and Asare17;Reference Wu, Chen, Wang, Jian and Ko23;Reference Czabanowska, Shickle and Burazeri28;Reference Goodman29;Reference Sonstein, Namenek Brouwer and Gluck33).
Discussion
In this scoping review, we identified competencies of HTA professionals described in the literature, which were used to verify and update the original competency framework of Mueller et al. (Reference Mueller, Gutierrez-Ibarluzea, Chiumente and Oortwijn8). Most competencies identified in the current literature mapped appropriately to the original framework. We identified five new competencies that should be included in existing domains. These competencies include interpreting and developing HTA reports, patient and public involvement, real-world data as a source of evidence for HTA, stakeholder identification, and organizational sustainability. We also identified three new domains, which were AI use for HTA, environmental aspects of health technologies, and performance and achievements of professionals, although the latter is not specifically for HTA.
The newly identified competencies and competency domains highlight emerging areas of expertise, which are increasingly gaining interest in the HTA community. For example, several HTA organizations around the globe are starting to incorporate environmental aspects into their HTA process, including those in the Netherlands (40), the United Kingdom (41), and Canada (Reference Bénard, Gatovo and Guertin42). Furthermore, the global society of HTA, HTA International (HTAi), recently started a working group on environmental sustainability in HTA, which aims to define the scope for environmental sustainability in HTA and proposes approaches to incorporate environmental sustainability in HTA recommendations (43).
The use of generative AI is also gaining more attention in HTA. It has the potential to assist in, for example, automating aspects of literature reviews, analyzing large collections of real-world data, and developing and adapting health economic models (Reference Fleurence, Bian and Wang44;45). Appropriate use of generative AI might optimize resource and personnel use, shorten assessment timelines, and improve alignment between evidence generation and decision making. However, there are also some drawbacks to the use of AI, such as issues of scientific validity and reliability, impact on equity, and regulatory considerations. These limitations could influence generative AI’s outcomes and interpretations, for example, resulting in incorrect conclusions in literature reviews or model development, a lack of transparency on methods, limited generalizability, and privacy issues (Reference Fleurence, Bian and Wang44). Therefore, several HTA organizations, including the National Institute for Health and Care Excellence (NICE) in England (United Kingdom) and Canada’s Drug Agency, published position statements on the use of AI in evidence identification, generation, extraction, and reporting for HTA (46;47). Additionally, the Global Policy Forum of HTAi, in which HTA organizations, industry, patients, and other stakeholders discuss hot topics related to HTA policy, recently published overarching principles for appropriate use of generative AI (45). It is essential that HTA professionals develop their competencies within the domains of AI use in HTA and environmental aspects, as well as the newly identified competencies, such as real-world data, stakeholder identification, and organizational sustainability. In this way, they remain responsive to the developments in their field. Therefore, the original competency framework of Mueller et al. (Reference Mueller, Gutierrez-Ibarluzea, Chiumente and Oortwijn8) needs to be updated with the newly identified competencies and domains. We have performed this update and international consensus building of the competency framework with HTA professionals, which will be described separately.
Strengths and limitations
The broad search strategy enabled a comprehensive scoping review, which identified new competencies and domains for HTA professionals in scientific and gray literature. However, a few limitations also have to be mentioned. First, heterogeneity in the use of terminology related to competencies in the literature made it difficult to assess whether a competency was described in the article, which challenged our screening and data extraction process. However, the authors, who are all HTA professionals, discussed the findings extensively, and as one author (WO) was involved in developing the original framework (Reference Mueller, Gutierrez-Ibarluzea, Chiumente and Oortwijn8), the interpretation of existing competencies was ensured. Second, the gray literature search was performed by one author only, which may have resulted in selection bias. However, the outcomes of the search were discussed with the SUSTAIN-HTA consortium members several times, who are all HTA professionals, to ensure that no relevant records were missed. Finally, although we only included records developed using scientific methods, no formal quality assessment was performed. This was also not possible because, due to the nature of the included studies, no standardized tool is available.
Conclusion
This study demonstrated that the competency framework of Mueller et al. (Reference Mueller, Gutierrez-Ibarluzea, Chiumente and Oortwijn8) can be verified, because competencies in the identified literature are mapped appropriately to the original competencies. We suggest adding new competencies related to interpreting and developing HTA reports, patient and public involvement, real-world data as a source of evidence for HTA, stakeholder identification, and organizational sustainability, and new domains comprising competencies related to AI use for HTA, environmental aspects of health technologies, and performance and achievements in HTA. Next steps include updating the competency framework of Mueller et al. (Reference Mueller, Gutierrez-Ibarluzea, Chiumente and Oortwijn8) with the newly identified competencies and domains and building international consensus using a Delphi exercise. The updated competency framework will be described separately and can support capacity building efforts and development of HTA training programs within the SUSTAIN-HTA project and beyond.
Supplementary material
The supplementary material for this article can be found at http://doi.org/10.1017/S0266462326103808.
Acknowledgments
We would especially like to thank Alessandra Lo Scalzo, Antonini Debora, Silvia Vainieri, and Marco Marchetti for their work on checking the included and excluded articles. We would also like to thank Marloes IJff, information specialist of Radboud University, for her help with developing the search strategy and Debjani Mueller for her input during the study. We would like to extend our gratitude to all the members of the SUSTAIN-HTA consortium for their input and critical review of the draft deliverables of the work presented in this manuscript, and especially Mariam Bibi, Shane Collins, Saif Elayan, and Femke Schuitmaker for providing editorial suggestions on the draft of this manuscript.
Funding statement
The SUSTAIN-HTA project is funded by the European Union’s Horizon Europe programme under grant agreement No 101136318. The UK participant is supported by UKRI grant No 10106859 (National Institute for Health and Care Excellence). Views and opinions expressed are, however, those of the author(s) only and do not necessarily reflect those of the European Union, the United Kingdom, HaDEA, or UKRI. Neither the European Union, the United Kingdom, nor the granting authorities can be held responsible for them. Open access funding provided by Radboud University Medical Center.
Competing interests
The Radboud University Medical Center received funding from Horizon Europe because of the SUSTAIN-HTA project. The funder had no role in the design, execution, and reporting of this study.
Disclosure of AI use
No text was generated using ChatGPT or any other Artificial Intelligence tool. ChatGPT was used in order to improve a few sentences and to gain inspiration for the structure of the discussion. After using this tool, the authors reviewed and edited the content as needed.



 Open access
Open access