


Introduction
Patients in post-acute care hospitals (PACH) experience high rates of colonization with multidrug-resistant organisms (MDRO). Reference McKinnell, Singh and Miller1 MDRO colonization in PACH likely reflects two scenarios: 1) importation by patients already colonized with MDRO who are admitted to PACH from acute care hospitals (ACH) and 2) acquisition via transmission within the PACH. Indeed, a previous longitudinal study in PACH found a high prevalence of MDRO carriage (57%), including vancomycin-resistant enterococci (VRE), methicillin-resistant Staphylococcus aureus (MRSA), and resistant gram-negative bacilli, upon admission, as well as new acquisitions during the patients’ stay (ranging from 13% to 36% of at-risk patients). Reference Mody, Foxman and Bradley2
The epidemiology of carbapenem-resistant Acinetobacter baumannii (CRAB) is multifaceted, involving clonal dissemination within and between healthcare institutions, frequent introduction of new clones, and horizontal gene transfer between A. baumannii clones. Reference Agodi, Voulgari and Barchitta3,Reference Doughty, Liu and Moran4 Clonal transmission between ACH and affiliated long-term care facilities (LTCF) has also been documented. Reference Kon, Temkin and Elmalih5–Reference Mortensen, Trivedi and Rosenberg7 Although CRAB is highly prevalent in PACH, Reference Harris, Pineles and Johnson8 its epidemiology in these settings is not well explored. In our previous study of PACH in Israel, we reported a high prevalence of CRAB carriage, particularly in mechanical ventilation wards (48%) and skilled nursing wards (28%). Reference Schechner, Masarwa and Levi9 However, the relative contributions of importation versus in-facility transmission in PACH remain unclear.
Here we aimed to study within-PACH CRAB transmission, and estimate the proportion of carriage related to it, by using Fourier-transform infrared (FTIR) spectroscopy to identify CRAB clusters. FTIR groups strains according to similarities in their physical properties and has been shown to correlate well with genetic relatedness, with higher discriminative power than multilocus sequence typing (MLST) and somewhat lower resolution than whole-genome single-nucleotide polymorphism (SNP) analysis. Reference Uribe, Salipante and Curtis10–Reference Teng, Habermehl and van Houdt13 Thus, isolates belonging to the same chain of transmission will fall into the same FTIR cluster, while those unrelated by transmission are less likely to do so. In this study, we hypothesized that patients with isolates belonging to the same cluster are more likely to represent within-PACH transmission than those who belong to different clusters. Spatial proximity facilitates microbial spread, thus, patients who are closer to one another are more likely to have CRAB isolates belonging to the same cluster. We therefore analyzed the association between patients’ spatial proximity—both within the same PACH and across different PACHs—and the likelihood of sharing the same CRAB cluster.
Methods
Setting and study design
The data for this study came from a one-day point-prevalence survey (PPS) conducted across all 18 PACH in Israel from June to December 2021. Information on the PPS and on infection prevention practices in PACHs in Israel, including hand hygiene audits, bathing practices, room cleaning protocols, and other standards, is available in detail in Schechner et al. Reference Schechner, Masarwa and Levi9 No outbreaks of clinical CRAB infections were reported in any of the PACHs during the study period. Patient transfers between PACHs are uncommon. PACHs are not linked to a specific acute care hospital for receiving or transferring patients.
The survey took place on four ward types: prolonged mechanical ventilation, skilled nursing, sub-acute care, and rehabilitation. These wards are considered “acute beds” in PACH and primarily serve elderly patients with complex medical needs. We selected them because they represent populations at particularly high risk for carriage of MDRO, including CRAB. The average length of stay varies by ward type: sub-acute wards typically accommodate patients for several weeks, rehabilitation wards for weeks to months, and skilled nursing and mechanical ventilation wards for months to years. Reference Ben-David, Masarwa and Fallach14 We randomly selected one ward of each type per facility (n = 55) and screened all patients in the selected wards for CRAB.
Study sample
The study sample comprised all patients who screened positive for CRAB during the PPS and whose isolates were saved for analysis.
CRAB screening and microbiological methods
Samples for CRAB were collected from the skin using sterile pre-moistened sponges and from the rectum using swabs. Skin samples were collected from patients’ arms (from the axilla downward) and legs (from the groin downward). Patients with tracheostomies also provided tracheal aspirate samples. Samples were processed at the national reference laboratory on the same day that they were collected. (For details, see Nutman et al.Reference Nutman, Levi and Keren-Paz 15 )
FTIR spectroscopy and spectrum analysis
We assessed the phenotypic similarity of CRAB isolates using FTIR spectroscopy (IR Biotyper, Bruker, Leipzig, Germany), as previously described. Reference Rakovitsky, Frenk and Kon16 We prepared samples according to the Biotyper manufacturer’s protocol. Isolates were grown on blood agar plates (HyLabs, Rehovot, Israel) at 35 ± 2°C for 24 hours. Each sample was tested in at least three replicates using the Biotyper’s default settings. Spectral data were processed with OPUS 7.5 software (Bruker) to generate a hierarchical cluster analysis, visualized as a dendrogram using the Pearson correlation coefficient. The cut-off value used to define dendrogram clusters was chosen based on visual inspection; we chose a cut-off of 0.4, which is within the manufacturer’s recommended range for Acinetobacter spp. We assigned a letter to each cluster defined by FTIR; even singletons are referred to here as clusters.
Data collection
During the PPS we collected the following data: institution, ward type, sample site, and room number. Each ward was classified as either one area or two separate areas based on floor plans and interviews with the PACH infection control (IC) nurse or head nurse. Wards were defined as two separate areas when they were both physically and functionally distinct, that is, separate wings or hallways, dedicated nursing staff assigned per shift, and designated equipment for each area.
Statistical analysis
We summarized the distribution of CRAB FTIR clusters by institution, by ward type, and by sample site. To explore the relationship between cluster sameness and proximity, the unit of analysis was patient pairs: we assigned each patient isolate to its cluster and paired each patient-cluster combination with every other patient-cluster combination. Patients who carried two distinct CRAB strains (belonging to more than one cluster) were counted separately for each of their clusters. We excluded pairs made up of the same patient and their two different clusters. We defined six patient proximity categories on an ordinal scale: same room, adjacent rooms, same ward (same area), same ward (different areas), different ward types (same institution), and different institutions. We calculated the odds of pairs having the same cluster for each proximity category and displayed this as a graph.
We performed a generalized estimating equation (GEE) logistic regression using cluster sameness (yes/no) as the outcome and patient proximity category as the predictor variable. This model accounted for patients who had 2 distinct CRAB strains and applied an exchangeable working correlation structure. We performed two regressions: in the first, all proximity categories were compared to the reference category of “different institutions”; in the second, we used staircase coding for dummy variables. The resulting odds ratios compared cluster sameness at each proximity level to the previous level rather than to a single reference category.
To estimate the extent of within-ward CRAB transmission, we compared the proportion of patient pairs with CRAB belonging to the same cluster in different institutions (serving as a baseline level of cluster similarity unrelated to transmission within the PACH) to the proportion of such pairs within the same ward. The difference between these proportions was used to approximate the fraction of same-cluster patient pairs attributable to transmission within the wards.
We created a radar graph to display the proportion of patient pairs with the same CRAB cluster for each proximity category, stratified by ward type.
Ethics
The study was approved by the jurisdictional institutional review board. The requirement for written informed consent was waived. Patients were informed of the screening verbally and in writing and had the option to refuse.
Results
Patients and clusters
A total of 3,909 samples were collected from 1,725 patients. Overall, 514 samples were positive for CRAB: 368 of 1,723 (21.4%) skin swabs, 69 of 1,683 (4.1%) rectal swabs, and 77 of 503 (15.3%) tracheal aspirates. We analyzed 461 CRAB samples isolated from 357 patients across 36 wards in 16 institutions. There were 15 wards with no CRAB carriers detected and 4 wards (in 2 PACH) for which the isolates were not saved. The strains were isolated from the skin (n = 338), tracheostomy (n = 63), and rectum (n = 60). FTIR analysis revealed 23 distinct clusters; two of them were singletons and one contained only 2 isolates from the same patient (dendogram in Figure S1).
Figure 1 displays the frequency and cumulative percentage of the 23 CRAB clusters detected by FTIR (N = 388 patient-cluster combinations). Cluster sizes ranged from 1 to 90, with a median of 7.0 and an interquartile range (IQR) of 2.5 to 23.0. Notably, 7 clusters accounted for 78% of all observations. As shown in Figure S2, the seven dominant clusters were not confined to a single facility but were distributed across multiple PACH.
Frequency and cumulative percentage of CRAB clusters detected by FTIR (N = 388 patient-cluster combinations).

Figure 2 illustrates the distribution of clusters by institution and ward type. Three findings are evident in the figure. First, most clusters appeared in multiple institutions, not necessarily in the same geographic area; the most common cluster (in black) was present in 11/16 PACH. Second, within the same institution, cluster composition differed between the various wards. Third, in wards with high CRAB frequency, multiple clusters were present, with or without a dominant cluster. There were only 3 wards (in PACH L and P) with more than one CRAB case and only a single cluster.
CRAB clusters by institution and ward type. Each panel represents one PACH (coded 1-16). Geographic areas: Jerusalem (1, 11); Central Israel (2, 5, 6, 9, 10, 12, 13, 15, 16); Northern Israel (3, 7, 8); Southern Israel (4, 14).

Cluster frequency of the 461 isolates by ward type and by anatomic site is presented in Figures S3 and S4.
Association between patient proximity and cluster sameness
A total of 326 patients were part of a single CRAB cluster, while 31 patients were part of two different clusters, resulting in 388 unique patient-clusters. Each patient-cluster was paired with every other patient-cluster, resulting in 75,047 pairs.
Figure 3 shows the odds of pairs having the same cluster versus a different cluster for each proximity category. Three steps are evident: the odds were similarly low (0.1) for pairs of patients in different institutions and in different wards within the same institution. The odds were highest (and similar) for pairs of patients in the same room or in adjacent rooms. Pairs of patients sharing the same ward, regardless of whether they were in the same area of the ward, comprised the middle step.
Odds of patient pairs having the same CRAB cluster, by proximity category.

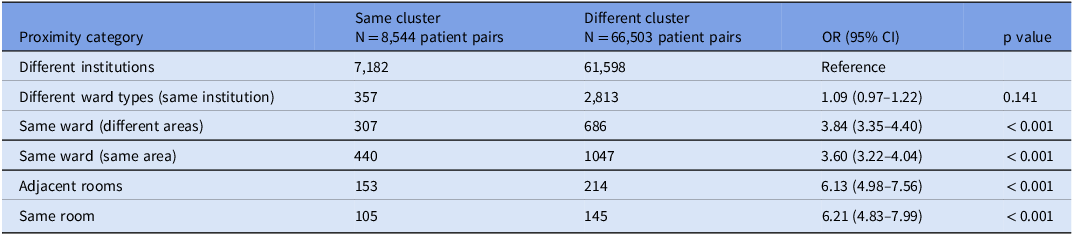
Table 1 shows the results of the logistic regression that corresponds to Figure 3. Compared to the reference category of “different institutions,” being in different wards within the same institution only led to a minor non-significant increase in the odds of cluster sameness (OR = 1.09; 95% CI = 0.97–1.22). Being in the same ward (different areas) or the same ward (same area) increased the odds by factors of 3.8 and 3.6, respectively (p < 0.001). Patients in adjacent rooms or in the same room had approximately 6 times higher odds of having the same cluster than the reference category. The model that compared each category to the previous category confirmed that there was no significant difference in the odds of having the same cluster between patients in the same area versus different areas of the ward (OR = 0.94; 95% CI = 0.79–1.12), or between those in the same room versus adjacent rooms (OR = 1.01; 95% CI = 0.73–1.40).
Generalized estimating equation (GEE) logistic regression of the association between patient proximity and CRAB cluster sameness

The proportion of patient pairs from different institutions who shared the same CRAB cluster was 10% (7,182 out of 68,780, Table 1). Thus, 10% represents cluster sameness that is not because of within-PACH transmission. In contrast, 32% of patient pairs within the same ward shared the same cluster (1,005 out of 3,097). Using these data, we estimated that approximately 70% of same-cluster pairs within wards (32% – 10%)/32%) were attributable to within-ward transmission.
The radar chart in Figure 4 shows that the association between proximity category and cluster sameness differed across ward type. In total, 19,683 pairs from ventilation wards and 12,868 pairs from skilled nursing wards were analyzed. Rehabilitation and sub-acute wards were excluded from this analysis due to the limited number of patient pairs (<10) in some proximity categories. As shown in the graph, the proportion of patient pairs in the same room with the same cluster was similar in both ventilation and skilled nursing wards, at approximately 40%. However, differences emerged for adjacent rooms: 56% of patient pairs in skilled nursing wards shared the same cluster, compared to only 35% in ventilation wards. A similar trend was observed for pairs within the same area of the ward, with cluster similarity rates of 39% in skilled nursing wards and 22% in ventilation wards. In both ward types, the percentage of pairs from different institutions with the same cluster was very low: 9% in ventilation wards and 12% in skilled nursing wards.
Association between proximity category and cluster sameness in ventilation and skilled nursing wards.

Discussion
Our analysis of CRAB isolates from 16 PACH revealed substantial cluster diversity, with 23 distinct clusters identified among 461 isolates. Seven dominant clusters accounted for 78% of cases. Cluster distribution varied both between institutions and between wards within the same institution. Having the same cluster may indicate cross-transmission within the PACH, either sporadic or in an outbreak, but it may also indicate importation of common strains acquired in other healthcare settings. In such cases, patients may share a cluster not due to transmission within the PACH but because certain strains are more prevalent. Our finding that sameness of CRAB clusters increased with patient proximity is evidence of cross-transmission within the PACH. Based on same-cluster pairs we estimated that 70% of prevalent CRAB cases resulted from within-ward transmission. Notably, the proportion of cluster sameness in some proximity categories (e.g., adjacent rooms) varied by ward type, suggesting that ward-specific factors, such as use of shared equipment or differences in cleaning practices, may influence the likelihood of CRAB transmission.
Compared to our findings, the cross-sectional study by Thom et al. demonstrated considerably greater A. baumannii clonal diversity. Reference Thom, Maragakis and Richards17 Among 128 isolates collected from ventilated patients in 10 LTCF in Maryland USA, they identified 68 unique PFGE groups. The higher diversity in that study compared to ours may reflect a difference in categorization between PFGE and FTIR or it may reflect true epidemiological differences in A. baumannii distribution related to geography and time. As in our study, Thom et al. found that small PFGE-defined clusters were shared both within individual facilities and across institutions, illustrating the potential for both importation and cross-transmission.
Imported versus nosocomially-acquired CRAB cases require different infection control strategies. Imported cases can be addressed through active screening upon admission, whereas nosocomial acquisition requires a combination of vertical interventions (screening and isolation) and horizontal infection control measures, including hand hygiene, environmental cleaning, and antimicrobial stewardship. In our study, the majority (70%) of within-ward cluster sameness reflected ward-level CRAB transmission, underscoring the importance of infection control efforts within PACH. To validate this estimate, universal CRAB screening upon admission would help determine the proportion of cases that are imported. Repeated follow-up screening of patients, combined with FTIR or whole-genome sequencing (WGS), would further clarify the dynamics of nosocomial transmission.
In our study, CRAB carriers sharing the same room had the highest odds of having the same cluster, which is not surprising. Suetens et al. previously identified room sharing as a risk factor for MRSA carriage. Reference Suetens, Niclaes and Jans18 However, we found that patients in adjacent rooms and even in the same ward also had high odds of strain sameness, especially in skilled nursing wards. This suggests that isolating CRAB carriers together in the same room may not be sufficient to prevent transmission. There are several explanations for these findings. First, we have previously shown that environmental contamination by CRAB carriers is high, and that nearly all CRAB carriers contribute to environmental contamination. Reference Schechner, Lerner, Temkin and Carmeli19 Second, in skilled nursing wards, the routine use of shared equipment, such as mobile trolleys, may facilitate transmission between rooms. Moreover, low nurse-to-patient ratios and the presence of patients with complex medical needs requiring frequent close contact with nursing staff may further increase the risk of transmission. Therefore, creating a physically separate CRAB cohort territory, along with enhanced environmental cleaning and infection control measures, may be necessary to prevent transmission in high-risk wards.
This study has several strengths. First, it was based on a large cross-sectional survey encompassing all PACH in Israel; the high prevalence of CRAB enabled a robust analysis of cluster diversity and transmission dynamics. Second, the use of FTIR allowed high-resolution differentiation of CRAB clusters. Third, we examined six levels of proximity, rather than simply room sharing.
The main weakness of our study was its cross-sectional design, which cannot determine precisely where CRAB was acquired and is inferior to longitudinal studies in distinguishing between imported cases and in-facility transmission. Second, we did not have whole-genome sequencing data to detect transmission events. Third, we lacked individual-level data on patients’ daily activities and movements, which could have helped to identify opportunities for spread. For these reasons, we avoided implying certainty that one patient directly infected another. Instead, we interpreted our findings in terms of the likelihood of potential transmission within the PACH compared with the likelihood of importation. Finally, our findings may not be generalizable to other settings with different CRAB prevalence, PACH design and patient mix, and infection control measures.
In conclusion, we found that the greater the proximity between CRAB carriers in PACH, the more likely they were to carry CRAB belonging to the same FTIR cluster. This strongly suggests that transmission is occurring within the PACH and is not limited to patients sharing a room. Screening upon admission to detect CRAB carriers, isolation (preferably in a cohort area), and compliance with horizontal infection control measures are important to limit the spread of CRAB in PACH.
The Israel PACH CRAB Working Group
Jacob Haviv, Emilia Anis, Esther-Lee Marcus, Hana Yosef (Herzog Medical Center); Ari Lauden (Reut Rehabilitation Hospital); Debby Ben-David, Angela Shimonov (Beit Rivka Geriatric Medical Center); Jochanan Stessman, Esther Ben Hamo, Moria Atun (Hod Amal Ma’ale Adumim Geriatric Hospital); Maya Shkolnik Gazit, Oshra Tirosh, Yana Vishnevski, Irena Uzlianer (Beit Hadar Medical Rehabilitation and Nursing Center); Nadya Kagansky, Yochai Levy (Shmuel Harofe Geriatric Medical Center); Tanya Bogoslavsky, Tammy Porat-Packer, Orna Eluk (Shoham Geriatric Medical Center); Ramzi Kurd (Bayit Balev Rishon Le’zion Geriatric Rehabilitation Center); Galia Rahav (Bayit Balev Geriatric & Rehabilitation Healthcare Services); Margalit Ben Shimol (Dorot Geriatric Rehabilitation Center); Mohamed Nassar, Tatiana Nagulevich, Osnat Kimchi (Golden Care Ness Ziona Geriatric Rehabilitation Center); Boris Svirsky, Mariana Habiballa, Rabea Ramlawe, Ibrahim Saffuri, Subhi Azzam (Golden Care Dushi Nazareth Geriatric Rehabilitation Center); Tatiana Hutzistov (Golden Care Tel Aviv Geriatric Rehabilitation Center); Pnina Ciobotaro, Pasha Gur (Herzfeld Geriatric Rehabilitation Medical Center); Ilana Or, Nurit Ben Aroya (Loewenstein Rehabilitation Hospital); Olga Druker (Neve Amit Geriatric Center); Inna Kaganovich Zafrany (Neve Shva Geriatric Center); Inna Shugaev, Eduard Zalyesov, Svetlana Zheleznyak, Alona Paz (Fliman Geriatric Rehabilitation Hospital); Ariel Yakim (Geriatrics Branch, Ministry of Health).
Supplementary material
For supplementary material accompanying this paper visit https://doi.org/10.1017/ice.2025.10337
Author contribution
Conceptualization: YC and VS; Methodology: YC and VS; Investigation: SM, REE, MB, AKP, and ET; Formal analysis: AC; Writing of the first draft: VS; Data collection: Study group members; Critical review and approval of the final draft: All authors and study group members.
Financial support
None.
Competing interests
Yehuda Carmeli has received grants and personal fees from Basilea, Enlivex Therapeutics, Omnix Medical, Pfizer, and Roche. All other authors have no conflicts of interest.







 Open access
Open access