


Introduction
The co-occurrence of substance use disorder (SUD) and mental health disorder (MHD) is a complex condition requiring tailored and effective care approaches from healthcare system. The overlap between substance use and MHDs have been described as dual diagnosis, psychiatric comorbidity, or concurrent/comorbid disorders. However, in 2022, Szerman with colleagues recommended adopting the standardised term ‘dual disorder’ (Szerman et al. Reference Szerman, Torrens, Maldonado, Balhara, Salom, Maremmani, Sher, Didia-Attas, Chen and Baler2022).
The complexity of dual disorder has been widely documented in the scientific literature (EMCDDA 2015; NIDA 2020) underscoring a worse clinical prognosis for people with dual disorder than for those with a diagnosis of either substance use or psychiatric illness. Dual disorder patients experience more severe symptoms, are at a greater risk of suicidal behaviour, more often visit emergency services or are hospitalised, and are more likely to have comorbid physical disorders. Additionally, they have lower retention rates in treatment and are at a higher risk of recurrence of substance use or other mental disorders. From a social perspective, people with dual disorder are characterised by higher rates of unemployment, poverty, and homelessness, and experience a higher incidence of social exclusion, violent or criminal behaviour (Bahji Reference Bahji2024; EMCDDA 2015; Volkow et al. Reference Volkow, Torrens, Poznyak, Sáenz, Busse, Kashino, Krupchanka, Kestel, Campello and Gerra2020; Volkow and Blanco Reference Volkow and Blanco2023).
Treatment for dual disorder varies across countries, ranging from fragmented care delivered across different settings and services to fully integrated approaches. Historically, treatment of dual disorder was shaped by prevailing policies and available resources (Fantuzzi and Mezzina Reference Fantuzzi and Mezzina2020; Staiger et al. Reference Staiger, Long and Baker2010), with MHD and SUD being managed separately within either the mental health or substance use services. This fragmented care model has been criticised for not acknowledging the interaction between MHD and SUD, which may lead to suboptimal interventions for people requiring comprehensive care. Several studies highlighted complex needs of patients with dual disorder (Cantwell Reference Cantwell2003; Weaver et al. Reference Weaver, Rutter, Madden, Ward, Stimson and Renton2001), which led to the development of interdependent approaches for both conditions: sequential, parallel, coordinated and integrated care models (Hemphill Reference Hemphill2021).
The sequential model addresses disorders one after the other, treating MHD first and SUD subsequently or vice versa; treatment for the latter disorder is only initiated once the former has been stabilised. The sequential approach can be useful in uncertain diagnoses, but it can also lead to fragmented care, information loss or treatment interruption due to the absence of a unified strategy (EMCDDA 2015). The parallel model addresses disorders at the same time but in different settings, and there may be no coordination between treatment services. The parallel approach can result in the duplication of efforts, leading to inefficiency and increased treatment costs (Torrens et al. Reference Torrens, Rossi, Martinez-Riera, Martinez-Sanvisens and Bulbena2012). The coordinated model addresses the limitations of the parallel approach by fostering communication between treatment teams and enhancing continuity of care (Balhara et al. Reference Balhara, Lev-Ran, Martínez-Raga, Benyamina, Singh, Blecha and Szerman2016). In this approach, mental health and addiction professionals work in parallel but coordinated manner, adjusting their interventions according to patient needs. The coordinated approach also has limitations, including potential information loss during treatment (Barba et al. Reference Barba, León, Calderón, López, García, Batanero, Barreno, López, Marín and Rojas2021; McGovern et al. Reference McGovern, Lambert-Harris, Gotham, Claus and Xie2014) and possibility of patients refusing some services, especially if they are isolated or not easily accessible. Today, the integrated treatment model is the most comprehensive approach for patients with dual disorder. In integrated care, both MHD and SUD are addressed simultaneously by the same treatment team providing holistic care (Brewer et al. Reference Brewer, Godley and Hulvershorn2017; Buckner et al. Reference Buckner, Zvolensky, Ecker, Schmidt, Lewis, Paulus, Lopez-Gamundi, Crapanzano and Bakhshaie2019). The integration of mental health and addiction specialists within an interdisciplinary team fosters a collaborative approach to treatment planning, ensuring that patients receive tailored response to their needs. This approach has been shown to reduce the risk of information loss, improve adherence to treatment and enhance clinical outcomes (Brooner et al. Reference Brooner, Kidorf, King, Peirce, Neufeld, Stoller and Kolodner2013; Watkins et al. Reference Watkins, Patton, Drexler, Rauch and Rothbaum2023).
While integrated care is the recommended approach to comorbidity of MHD and SUD (EMCDDA 2015), usually local policies, organisational structures and available resources define which care model is most prevailing for dual disorder across health systems. This has been shown in a recent survey of the REITOX National Focal Points (NFP) in Europe, where dual disorder has been addressed by varied treatment approaches (Montanari et al. 2025). The same survey identified 14 services across 10 European countries reporting the provision of integrated care for dual disorder. A further ad-hoc survey has been developed for the representatives of these services to scope characteristics of their organisation and treatment provision, barriers and facilitators for implementing integrated care for people with dual disorder. This paper summarises findings of the latest survey and aims to identify gaps and potential solutions to better address needs of people with dual disorder in Europe.
Methods
Since 2020, the European Union Drugs Agency (EUDA) and its Advisory Board on psychiatric comorbidity, which promotes a common treatment approach for dual disorder patients, have worked on mapping interventions for comorbid MHD and SUD across European countries. With this aim, an online survey was conducted through the EUDA REITOX NFP network in 2022, where country representatives were asked to describe the type of dual disorder treatment model that best fits the situation in their country and provide descriptions of services for people with dual disorder. Ten surveyed countries reported services providing integrated care, and an ad-hoc survey was designed to further scope the details of these services.
The survey was developed following literature and recommendations on assessment and treatment of dual disorder (Todd Reference Todd2010; UNODC 2022), and was finalised after incorporating feedback from members of the EUDA Advisory Board on psychiatric comorbidity. Participants were asked to complete the survey on EU survey platform. The survey included questions about:
-
• Service description, including location, setting, service type and waiting lists.
-
• Offered treatments and their characteristics.
-
• Treatment process, including admission, diagnosis, staff responsibilities and termination.
-
• Treatment outcomes: how they are measured and collected.
-
• Treatment implementation characteristics, including funding, costs, training, barriers and facilitators.
The full survey is included in the supplementary materials.
Study sample included dual disorder treatment services from European countries that were identified by REITOX NFPs. Since there is no comprehensive registry of services in Europe offering integrated dual disorder treatment, the respondents for the survey were selected based on the recommendations from NFPs as those representing best practices in dual disorder care. A unique link to the survey was shared with respondents explaining the objectives of the survey and inviting them to complete the survey. Representatives could also share their login details with anyone who could contribute accurate information about the service characteristics.
In October 2022, invitations to participate in the survey were sent to 32 services providing integrated dual disorder treatment in 16 European countries with a follow-up reminder sent in November 2022. Final study sample included responses from 14 treatment services from 10 European countries. Data were analysed using thematic qualitative analysis, grouping responses by commonalities and differences between the services.
Results
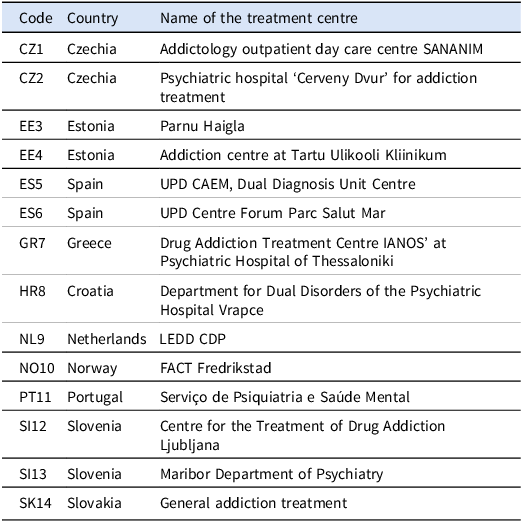
Fourteen treatment centres from 10 European countries were included to the analysis (Table 1).
Treatment centres included in the analysis

Characteristics of treatment centres
Nearly all treatment centres were set in urban areas except for CZ2 which was in a rural area. All services offered integrated care for dual disorder but their setting type varied: five were drug treatment centres (CZ1, CZ2, NL9, SI12, SK14), four were mental health centres (EE3, ES5, GR7, SI13), three were situated in a hospital (EE4, ES6, PT11), and a service in Norway was a community care centre for outpatients only (NO10). Most services provided both inpatient and outpatient treatment (EE3, EE4, GR7, NL9, PT11, SI12, SI13, SK14), with a few focusing on inpatients (CZ2, ES5, ES6) or outpatients only (CZ1, NO10). Four services did not have waiting lists (ES5, ES6, NO10, SK14), while six services with waiting lists specified that patients had to wait from 14 days (SI12) to three months (CZ2) for treatment. Average treatment length ranged from 14 (ES5), 18 (ES6) or 21 days (GR7) up to six months (CZ2, SI12). Some services offered longer treatment for outpatients lasting up to 12 months (SK14) or without closing time (NO10, SI12).
Services offered
Out of 14 services, most offered treatment for multiple addictions: mostly cited were alcohol (13 services), cocaine (13) and other psychostimulants (13), opioids (13), and new psychoactive drugs (13). Services also offered treatment for other drugs (10) and various behavioural addictions (8), of which gambling was mentioned most often (5). Treatment for compulsive internet use (3), gaming (2), or shopping (1) were also mentioned. Only three centres (ES6, GR7, SK14) offered treatment for cannabis use, and half of the surveyed services (7) addressed tobacco addiction.
All services addressed an array of MHD, including psychotic or bipolar disorder conditions (13 out of 14), affective disorders (14), posttraumatic stress disorder (14), and treatment-resistant personality disorders (14). Seven out of 14 services offered suicide prevention programmes. Various psychological treatment approaches were used, including 12 services mentioning individual and/or group psychological counselling, and 10 services providing family counselling. Nearly all services (13) used Motivational Interviewing, eight services provided Cognitive Behavioural Therapy, one offered contingency management (SK14), and one used integrative psychotherapeutic approach (CZ2).
Regarding specific treatment options, all services offered multiple interventions for both drug and mental health problems. The only exception was Opioid Agonist Treatment (OAT), as none of the analysed centres provided integrated treatment for patients with dual disorder and who were still participating in OAT. Also, recovery management/social reintegration services was the least mentioned support option offered by eight out of 14 surveyed service providers. Regarding additional integrated support, 13 treatment centres offered pregnancy testing, 12 screened for infections, and 10 provided various vaccination. Centres also offered consultations with specialists in infectious medicine (13 out of 14), hepatology (9), dentistry (9), or gynaecology (8). Support with intimate partner violence detection or legal advice were offered by five services, four reported supporting adolescents and youth (CZ2, PT11, SI12, SK14). Regarding cooperation with external agencies, most services supported patients with social security (11 out of 14), employment (10) and housing (8), or provided educational programmes (7). Fewer services offered legal support with the criminal justice system (5).
Treatment process
Majority of services had inclusion and exclusion criteria (10 out of 14 for each), with some excluding people with cognitive impairment (ES5, ES6) or antisocial personality disorder (NL9). Some services reported excluding patients if they exhibited violent behaviour (SI12, SI13) or sexual harassment (SI13) during the treatment episode in the centre.
All services established dual disorder diagnosis following clinical evaluation by a psychiatrist. In eight services, dual disorder diagnosis was also established by psychologists. Half of the services used standardised diagnostic tools that varied considerably between services (e.g., MINI, MINI 7, MINI PLUS, COWS, CIWA-AR, DIVA 5, MMSE, MOCA, AUDIT, DUDIT, TRAPS, PANS, CAGE, SAD-Q). In most services, all staff members, including psychiatrists, psychologists, social workers and nurses, shared responsibilities for individual patients’ care and clinical records.
Patients accessed the integrated dual disorder treatment in multiple ways, including being referred from primary care or general hospital, community or other drug treatment centres, harm reduction, social or criminal justice services, but access through mental health service was mentioned by all surveyed centres. Eleven out of 14 services emphasised the importance of continuity of care plan after the integrated treatment ends. Ten services reported that patients were referred to other service providers post-treatment, with community (7 out of 10) or other drug treatment centres (6), and mental health services (7) mentioned most often. Some services noted coordinating post-treatment options when transferring patients to community mental health or drug services (ES6, HR8, PT11), outpatient care (GR7), or retaining the contact with former patients even if they become incarcerated (NO10).
Evaluation of treatment
Treatment outcomes were collected at eight out of 14 surveyed services, and the collected outcome measures differed. Services collected data on treatment completion or continuation (CZ2), treatment length (GR7), patients’ abstinence (CZ2, PT11, SK14) or relapses (GR7). Other services were evaluating outcomes every few months (NO10) or used validated scales for measuring treatment outcomes (ES6, NL9). Eight services collected data on patients’ satisfaction, three (CZ1, SI12, SK14) conducted cost-benefit evaluations, and one (CZ1) assessed the outcomes of cross-referrals.
Barriers for integrated dual disorder treatment
Several challenges have been recognised when operating a multidisciplinary dual disorder treatment service. Respondents mentioned insufficient professional knowledge regarding both addiction and MHDs (NL9) and a lack of adequate staff that would meet the needs of patients with dual disorder (PT11). In some instances, the difficulty arises from the need to coordinate different professions involved in the management of dual disorders, which may lead to divergent objectives and a lack of a unified response to the patient’s needs (CZ1). Other difficulties appear when collaborating with services that are less familiar with dual disorder, for instance, the criminal justice system (EE4). Maintaining continuity of care after the integrative treatment period was identified as an obstacle to patients’ recovery, specifically in places where community services for dual disorder treatment are not available (ES6).
Facilitators for integrated dual disorder treatment
Services noted that effectively addressing the above-mentioned barriers strongly facilitates overall dual disorder treatment. For instance, continued staff training, expertise and knowledge in treating dual disorder were stressed as crucial factors for successfully running an integrative treatment service (CZ1, NL9). Some noted that maintaining staff motivation and providing continued education (NO10, SI12) are important for improving dual disorder treatment.
Respondents mostly stressed the importance of collaboration with other services that attend patients with dual disorder. For success of integrative care, respondents stressed the importance of cooperation between SUD and MHD services (CZ1), clear communication with acute mental health staff about patients’ issues with substance use (ES6), maintaining communication with services that support patients after treatment – health and social services, therapeutic communities, criminal justice system, and non-governmental organisations (HR8). Several respondents emphasised raising awareness of the need for integrated dual disorder treatment, involving medical staff and public advocacy representatives (SI12), hospitals, municipalities (NO10), and the Ministry of Health (SK14).
Personalised support for both conditions was noted crucial for treatment success (CZ1). Tailored services are convenient, enhance therapeutic alliance, patients’ compliance and adherence to treatment process that lead to treatment success and recovery (EE4, GR7). Strong therapeutic alliance helps educate patients about the links between their substance use and mental health conditions, which in turn increases tolerance for relapses and reduces odds of re-hospitalisation (GR7).
Discussion
Survey of 14 treatment centres from 10 European countries providing integrated treatment for people with addiction and mental health diagnoses showed that integrated care services are exceptions among available support options for this patient group in European healthcare systems. Although scientific publications and clinical guidelines recommend integrated treatment approaches addressing the needs of people with dual disorders, services that effectively implement these recommendations remain the exception rather than the rule. As collected data show, the organisation of treatment programmes and the available service portfolios in most countries still do not provide such integrated care. Survey results indicated that while comprehensive support for dual disorder patients can be implemented through various approaches, many services reported challenges in sustaining continuity of care following integrated treatment.
Dual disorder treatment was implemented across diverse settings, including hospitals, drug treatment and mental health centres, showing that integrated support can be tailored to varied healthcare systems and national SUD and/or MHD treatment strategies. Mostly a combination of inpatient and outpatient treatment options of different lengths were offered, and an array of adjustable treatment modalities for addiction and mental health problems were provided. Most respondents highlighted the input of all staff members to organisation of integrated care; for instance, in many services all staff, including psychiatrists, psychologists, social workers, and nurses, shared the responsibility of monitoring patients and updating clinical records. Nevertheless, predominantly psychiatrists diagnosed dual disorder across most services, which underscores the importance of specialised psychiatric knowledge in these settings. While the dual disorder diagnosis was mostly confirmed by a clinician (psychiatrist or psychologist), use of diagnostic tools for establishing the diagnosis or its severity was less common. This is likely due to lengthy administration times that screening and diagnostic interviews conducted by clinicians require, which makes them unfeasible for use in clinical practice (EMCDDA 2015). This underscores the inherent challenges when identifying people with dual disorder, and highlights the need for a standardised instrument that could reliably identify the diagnosis without lengthy screening process or specialised expertise.
Apart from standard addiction treatments, 13 out of 14 services offered treatment for people using novel psychoactive substances (NPS), likely focusing on detoxification and psychological support (Scherbaum et al. Reference Scherbaum, Schifano and Bonnet2017; Specka et al. Reference Specka, Kuhlmann, Sawazki, Bonnet, Steinert, Cybulska-Rycicki, Eich, Zeiske, Niedersteberg, Schaaf and Scherbaum2020). In contrast, only half services treated tobacco addiction, and just three centres addressed cannabis use. Both tobacco and cannabis use are common among people in treatment of using other drugs (Simonavicius et al. Reference Simonavicius, Singh, Calder, Hines, Lynskey and Morley2019), and both substances have been linked to acute or longer-term physical and mental health issues (Lowe et al. Reference Lowe, Sasiadek, Coles and George2019; Taylor et al. Reference Taylor, Taylor, McNeill, Girling, Farley, Lindson-Hawley and Aveyard2014). Smoking-related health conditions cause around a quarter of deaths among people using illicit drugs (Callaghan et al. Reference Callaghan, Gatley, Sykes and Taylor2018; Lewer et al. Reference Lewer, Tattan-Birch and Cox2025), which highlights a need for integrated care services to address smoking among patients. Additionally, cannabis is the most frequently cited primary drug reported by 42% of all first-time treatment clients in Europe in 2023 (EUDA 2025), which underscores the need to increase integrated dual disorder treatment provisions for those with primary cannabis use disorder.
None of the reviewed services offered integrated care for people in OAT, which meant that people with a mental health diagnosis in OAT would need to undergo detoxification before receiving integrated care for their dual disorder. A recent study in Spain found that nearly two-thirds (63.5%) of surveyed OAT outpatients had a lifetime dual disorder, illustrating a substantial need for integrated care among this population (Barbaglia et al. Reference Barbaglia, Molero-Calafell, Angulo-Brunet, Alcaraz, Bartroli and Mestre-Pintó2025). While nearly all dual disorder treatment services offered pharmacological detoxification as part of integrated care, this gap restricts treatment access to opioid users who might be reluctant to give up their OAT.
Only half of integrated care services offered suicide prevention programmes. SUDs are closely linked with suicidal ideation and suicide death (Poorolajal et al. Reference Poorolajal, Haghtalab, Farhadi and Darvishi2016), and the link is strengthened by comorbid MHDs. In a Danish cohort study which followed up dual disorder patients for up to 21 years after integrated care, nearly 8% died from suicide, which could be prevented by better-tailored treatment (Düring et al. Reference Düring, Jobe, Balleby and Mårtensson2025). Recent data from the European Drug report (EUDA 2025) also indicate that approximately one in eight overdose deaths were attributed to suicidal intent in certain countries, with notably higher rates among women compared to men. Despite the clear need to address suicidal intent among those with dual disorder during and after treatment, the limited availability of prevention programmes remains a major gap hinting that responsibility for managing suicidal ideation largely remains with mental health services.
Most services addressed intimate partner violence, but there were no gender-responsive treatments offered as part of the integrated dual disorder care. Women with SUDs are disproportionately affected by adverse environmental and familial conditions compared to men – they are more likely to grow up in households with a history of substance use, marked by family disruption and increased environmental stressors, that later lead to relationships with partners who also use substances. Around 70% of women who inject drugs experience intimate partner violence in their current or most recent relationship, which is often associated with women being pressured into unsafe drug use, unprotected sex or trading sex for drug or money (Tirado-Muñoz et al. Reference Tirado-Muñoz, Gilchrist, Fischer, Taylor, Moskalewicz, Giammarchi, Köchl, Munro, Dąbrowska, Shaw, Di Furia, Leeb, Hopf and Torrens2018). Gender-responsive interventions have been developed for women with dual disorder and experiencing intimate partner violence. In general, these interventions focus on social support, interpersonal relationships, psychoeducation, self-efficacy, and coping skills for mood disturbances (Epstein et al. Reference Epstein, McCrady, Hallgren, Cook, Jensen and Hildebrandt2018). For instance, Female-Specific Cognitive Behavioural Therapy has shown efficacy in reducing alcohol use, alleviating internalising symptoms and improving interpersonal functioning in women with SUD (Epstein et al. Reference Epstein, McCrady, Hallgren, Gaba, Cook, Jensen, Hildebrandt, Holzhauer and Litt2018). Similar gender-responsive treatment components should be integrated into dual disorder treatment programmes.
Fewer than half of services collected treatment outcomes or measured patients’ satisfaction, cross-referral effectiveness or cost–benefit of interventions provided. The evaluation of patients’ satisfaction in dual disorder treatment is necessary for assessing the quality of care and for providing more person-centred interventions. Research shows that higher patients’ satisfaction is associated with greater treatment adherence, better clinical outcomes and reduced dropout rates. Satisfaction is related to perceived quality of the therapeutic relationship, individualised attention, and active user participation in treatment planning (Bador et al. Reference Bador, Johansson, Axelsson, Nilsson and Kerekes2025; Sanghani and Moler Reference Sanghani and Moler2015). Therefore, patients’ satisfaction could be enhanced by the presence of engaged, knowledgeable staff, opportunities for collaborative decision-making, and a trusting therapeutic alliance. Patients’ satisfaction is an indirect marker of the quality and effectiveness of treatment programmes, making its systematic evaluation a priority in research and clinical practice for integrated care in dual disorder (Ferreira et al. Reference Ferreira, Vieira, Pedro, Caldas and Varela2023). Despite persisting challenges in standardisation, data collection, and the interpretation of patient-reported measures across clinical contexts (Migchels et al. Reference Migchels, Zerrouk, Crunelle, Matthys, Gremeaux, Fernandez, Jérôme, van den Brink and Vanderplasschen2023), using comprehensive treatment evaluation methods could enhance dual disorder care and identify most effective interventions.
Despite some limitations in provision, the surveyed integrated care services were well-established in their respective countries and served as examples of dual disorder treatment. Several services noted discrepancies in how needs of people with dual disorder were addressed during and following discharge from integrated care. To facilitate patients’ reintegration after treatment, services addressed their social, employment, housing needs, and some offered legal support. Nevertheless, the lack of continuity of care post-discharge was reported frequently and was mostly attributed to divergent viewpoints and challenges in communication with services supporting patients afterwards. Continuity of care, including uninterrupted therapeutic relationships, seamless transitions between services, and prompt responsiveness to emerging needs, is critical for sustained recovery in dual disorder treatment (McCallum et al. Reference McCallum, Mikocka-Walus, Turnbull and Andrews2015). Continued engagement with coordinated services ensures that patients receive consistent support across different phases of treatment, thus facilitating adherence, reducing risk of relapse and improving psychosocial functioning. Continuity of care is particularly crucial for individuals transitioning from incarceration to community. Upon release, people with dual disorder face an elevated risk of relapse and reincarceration, partly due to the disruption of care. To mitigate the risks, establishing a discharge plan with individuals, linking them to community mental health and addiction services, and ensuring uninterrupted provision of medication and planned follow-up appointments can support successful reintegration (Turu et al. Reference Turu, Barnés and Marco2019; Young et al. Reference Young, Heffernan, Borschmann, Ogloff, Spittal, Kouyoumdjian, Preen, Butler, Brophy, Crilly and Kinner2018).
Integrated care is the most effective treatment for people with dual disorder, and the identified diversity of approaches across Europe suggests that effective care can be implemented in various forms. On the other hand, different integrated care approaches might hinder the continuity of dual disorder treatment. One potential solution is to adopt a nationally endorsed model of care for dual disorder throughout the healthcare system, as currently being implemented in Ireland (National Working Group for Dual Diagnosis 2023). This would provide a framework that enables the implementation of integrated care in various settings and supports the provision of tailored care for people with dual disorder beyond a single treatment episode. Moreover, evaluation of treatment outcomes and longer follow-up of integrated care patients could strengthen evidence base and improve integrated treatment provision. A coordinated work by European integrated care services towards screening and evaluation of dual disorder patients could further support the development of harmonised approach towards dual disorder treatment, which is a recognised priority in the European Union (Council of the EU 2023).
This study has several limitations. Firstly, only services from 10 out of 16 invited European countries replied to the survey, therefore findings do not represent fully the European context. Secondly, the selection of integrated care services that were approached were identified by the European National Focal Points, based on the expert opinion rather than on specific selection criteria. Thirdly, the described services are heterogeneous regarding setting, programmes, objectives and other characteristics and cannot be compared directly. Despite these limitations, this is the first analysis of best practice examples in how dual disorder is treated in multiple integrated care services across Europe.
Conclusion
This is a first description of integrated care for patients with comorbid MHD and SUD in Europe. The analysed services offer comprehensive treatment for dual disorder, but further improvements could be introduced by broadening treatment options for tobacco and cannabis use, tailoring for sex/gender-specific problems, and establishing treatment outcome measures. Improving continuity of care after a dual disorder treatment episode is currently the top priority. The current analysis could be followed by the comparable assessment of integrated care outcomes in other European countries.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/ipm.2026.10174.
Acknowledgements
We thank members of the EUDA Advisory Board on psychiatric comorbidity for their guidance on the integrated care centre survey, and the representatives of European National Focal Points for their expertise and support in mapping integrated care services across Europe. We also are grateful to all respondents from surveyed integrated care centres for their valuable time and insights, which are crucial to advancing dual diagnosis treatment in Europe.
Funding statement
This study was funded by MCDDA Contract CT.HEA.0116.10 and RIAPAd RD24/0003/0001 funded by Instituto de Salud Carlos III (ISCIII) and co-funded by the European Union.
Competing interests
The authors declare none.
Ethical standards
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committee on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008.



 Open access
Open access