


Purpose in life is the feeling that one’s life is goal-oriented and has direction (Ryff, Reference Ryff1995). There is a substantial literature that links purpose in life, and the related construct of meaning in life, to healthier behaviors and better health outcomes (Czekierda, Banik, Park, & Luszczynska, Reference Czekierda, Banik, Park and Luszczynska2017; Ribeiro, Yassuda, & Neri, Reference Ribeiro, Yassuda and Neri2020). Individuals higher in purpose in life, for example, tend to engage in more physical activity (Sutin et al., Reference Sutin, Stephan, Kekäläinen, Luchetti and Terracciano2025), are less likely to smoke (Weston, Hill, & Mroczek, Reference Weston, Hill and Mroczek2024) or use other substances (Kim et al., Reference Kim, Ryff, Hassett, Brummett, Yeh and Strecher2020), and more likely to get preventative cancer screenings (Kim, Strecher, & Ryff, Reference Kim, Strecher and Ryff2014). Perhaps as a result, such individuals are also less likely to have chronic disease (Musich et al., Reference Musich, Wang, Kraemer, Hawkins and Wicker2018), including cardiovascular disease (Kim et al., Reference Kim, Sun, Park, Kubzansky and Peterson2013), diabetes (Hafez et al., Reference Hafez, Heisler, Choi, Ankuda, Winkelman and Kullgren2018), Parkinson’s disease (Sutin, Luchetti, Stephan, & Terracciano, Reference Sutin, Luchetti, Stephan and Terracciano2024), or dementia (Sutin et al., Reference Sutin, Luchetti, Aschwanden, Stephan, Sesker and Terracciano2023). And, ultimately, individuals higher in purpose in life have longer health spans (Boyle et al., Reference Boyle, Wang, Yu, Barnes, Wilson and Bennett2022) and lower risk of mortality (Hill & Turiano, Reference Hill and Turiano2014).
A landmark meta-analysis published in 2016 demonstrated that purpose and meaning in life had a consistent association with lower risk of mortality (Cohen, Bavishi, & Rozanski, Reference Cohen, Bavishi and Rozanski2016). The present research seeks to update and extend this seminal meta-analysis. With 10 years since publication, there have been additional studies that can be added to the meta-analysis (e.g. Ironson, Verhagen, da Rosa, & Hylton, Reference Ironson, Verhagen, da Rosa and Hylton2021; Lamar et al., Reference Lamar, James, Glover, Capuano, McSorley, Wilson and Barnes2022). Further, even studies included in the previous meta-analysis now have a longer follow-up, particularly large cohort studies that are ongoing and tracking vital status (e.g. the Midlife in the United States study). As such, the length of participant follow-up is extended by at least a decade. There are also several additional large, ongoing cohort studies that measured purpose or meaning and track vital status that were not included in the previous meta-analysis. The first goal of this research is thus to update the previous meta-analysis with additional published studies and a coordinated analysis of publicly available datasets that includes the most updated vital status available to have the longest survival time possible and the largest sample size to date.
In addition to an update, the present research expands on the previous meta-analysis in several ways. In particular, we take a systematic approach to evaluate whether the association between purpose and mortality generalizes across sociodemographic populations. There is some evidence that the association may be moderated by sex (Shiba et al., Reference Shiba, Kubzansky, Williams, VanderWeele and Kim2022) or socioeconomic status (Shiba et al., Reference Shiba, Kubzansky, Williams, VanderWeele and Kim2021), although not all find these differences (Boyle, Barnes, Buchman, & Bennett, Reference Boyle, Barnes, Buchman and Bennett2009). Interactions can be difficult to detect and replicate (Sherman & Pashler, Reference Sherman and Pashler2019), and thus the use of multiple samples is essential to identify the most robust, replicable differences across populations. The second goal of this research is thus to test whether the association between purpose and mortality varies by individual-level factors: age, sex, race, Hispanic ethnicity, or education. Moreover, meta-regressions offer the opportunity to test potential study-level moderators, such as the content of the scale (e.g. purpose versus meaning), length of the scale (i.e. number of items), and the location (e.g. United States versus other).
Another expansion on the previous meta-analysis is to systematically evaluate whether the association between purpose and mortality is accounted for by common behavioral and clinical risk factors. There is a consistent association between purpose in life and greater engagement in physical activity, measured either with self-report (Yemiscigil & Vlaev, Reference Yemiscigil and Vlaev2021) or accelerometry (Sutin et al., Reference Sutin, Stephan, Kekäläinen, Luchetti and Terracciano2025), and lower likelihood of smoking (Weston et al., Reference Weston, Hill and Mroczek2024). Physical (in)activity and smoking are well-replicated behavioral risk factors for earlier mortality (Ekelund et al., Reference Ekelund, Tarp, Steene-Johannessen, Hansen, Jefferis, Fagerland and Lee2019; Magnussen et al., Reference Magnussen, Ojeda, Leong, Alegre-Diaz, Amouyel, Aviles-Santa and Consortium2023). Likewise, hypertension, diabetes, and obesity are associated with mortality risk (Magnussen et al., Reference Magnussen, Ojeda, Leong, Alegre-Diaz, Amouyel, Aviles-Santa and Consortium2023), and individuals higher in purpose are less likely to have these conditions (Hafez et al., Reference Hafez, Heisler, Choi, Ankuda, Winkelman and Kullgren2018; Kim, Delaney, & Kubansky, Reference Kim, Delaney and Kubansky2019). As such, these behavioral (physical activity, smoking) and clinical (hypertension, diabetes, obesity) factors may account for the association between purpose and meaning in life and mortality. These factors may also serve as mediators rather than confounders, as models of purpose and health suggest that the healthier behavioral patterns and clinical profiles associated with purpose are mechanisms of maintaining better health (Kim et al., Reference Kim, Delaney and Kubansky2019; Sutin, Luchetti, & Terracciano, Reference Sutin, Luchetti and Terracciano2021). The third goal of this research is thus to evaluate how much of the association between purpose and mortality is accounted for by behavioral and clinical risk factors.
Finally, purpose and meaning in life and depression are consistently related (Boreham & Schutte, Reference Boreham and Schutte2023). Individuals with greater purpose tend to have fewer depressive symptoms (meta-analytic association = −.32, p < .001; Sutin, Luchetti, Stephan, Karakose, et al., 2026) and a lower risk of developing depression over time (HR = .74, 95% CI = .68, .81, p < .001; Sutin, Luchetti, Stephan, & Terracciano, Reference Sutin, Luchetti, Stephan and Terracciano2026; Wood & Joseph, Reference Wood and Joseph2010). Although conceptually distinct constructs, there is often the question of whether the association between purpose and better health outcomes is observed because individuals with more purpose tend to have less depression. As such, the fourth goal of this research is to systematically address whether the association between purpose and mortality is accounted for by depression.
To address these four questions, the present research undertook a systematic review of the published literature and combined the results with new results from a coordinated analysis of individual-participant data from publicly available cohort studies that included a measure of purpose or meaning in life and related constructs (e.g. ikigai) and tracked vital status over time. Based on the previous meta-analysis (Cohen et al., Reference Cohen, Bavishi and Rozanski2016), we expect that higher purpose and meaning in life will be associated with lower risk of mortality. We construe the moderation analyses as exploratory because of contradictory findings reported in the literature (Boyle et al., Reference Boyle, Barnes, Buchman and Bennett2009; Shiba et al., Reference Shiba, Kubzansky, Williams, VanderWeele and Kim2022). Based on previous research on other health outcomes (e.g. dementia; Sutin et al., Reference Sutin, Luchetti, Aschwanden, Stephan, Sesker and Terracciano2023), we expect that the association between purpose and mortality will be attenuated when behavioral and clinical risk factors or depression are included in the model, but that it will remain significant.
Method
The protocol for this study was pre-registered in PROSPERO (#CRD42024588704). Deviations from the preregistration are reported in Supplemental Material. The research questions were developed utilizing the PICOS framework: P (population) = general population; I (intervention) = no intervention, assessment of purpose or related construct; C (comparison) = no control group/comparison; O (outcome) = risk of mortality; and S (study design) = longitudinal observational studies. The meta-analysis included a coordinated analysis of individual-participant data from publicly available datasets combined with results from the published literature.
Coordinated analysis of individual-participant data
Cohorts for the coordinated analysis were identified through the Gateway to Global Aging, ICPSR, and the UK Data Service, as well as through the published literature. Cohorts were included if participants reported on their purpose or meaning in life, the study tracked vital status over time, and the data were publicly available. Eight cohorts were identified for inclusion: the Health and Retirement Study (HRS; https://hrs.isr.umich.edu), the National Health and Aging Trends Study (NHATS; https://www.nhats.org/researcher/nhats), the Panel Study of Income Dynamics (PSID; https://psidonline.isr.umich.edu), the Midlife in the United States Study (MIDUS; https://midus.wisc.edu/), the Wisconsin Longitudinal Study (WLS; https://wls.wisc.edu/), the UK Household Longitudinal Study Understanding Society (US; https://www.understandingsociety.ac.uk/), the Survey of Health, Ageing, and Retirement in Europe (SHARE; https://share-eric.eu/), and the Australian Longitudinal Study of Aging (ALSA; https://sites.flinders.edu.au/alsa/). The first assessment of the purpose-related construct was used in each cohort, and the most current vital status information was used in the analysis (see Table 1 for follow-up length).
Descriptive statistics for the individual-participant samples

Table 1. Long description
The table consists of 9 columns. The first column lists the Variable, followed by columns for eight studies: H R S, N H A T S, P S I D, U S, M I D U S, W L S, S H A R E, and A L S A.
* Age (years): Means range from 45.24 in U S to 79.74 in A L S A.
* Age range: Spans from 15 to 107 across all studies.
* Sex (female): Percentages range from 50.8 percent in A L S A to 58.6 percent in H R S.
* Race (Black): Reported for H R S (17.2 percent), N H A T S (21.1 percent), P S I D (29.1 percent), U S (0.4 percent), and M I D U S (5.1 percent); others are blank.
* Race (Otherwise): Reported for H R S (8.1 percent), N H A T S (8.6 percent), P S I D (7.5 percent), U S (1.9 percent), and M I D U S (4.0 percent).
* Hispanic (yes): Reported for H R S (11.9 percent), N H A T S (5.8 percent), P S I D (4.7 percent), and M I D U S (4.2 percent).
* Education: Mean scores range from 2.92 in S H A R E to 14.03 in P S I D.
* Purpose in life: Mean scores range from 2.47 in U S to 16.51 in M I D U S.
* Mortality (yes): Percentages range from 5.0 percent in P S I D to 86.6 percent in A L S A.
* Time (years): Mean follow-up time ranges from 4.90 in P S I D to 26.53 in W L S.
* Time range: Spans from 1 to 32 years across the studies.
Note: ALSA, Australian Longitudinal Study of Aging; HRS, Health and Retirement Study; MIDUS, Midlife in the United States Study; NHATS, National Health and Aging Trends Study; PSID, Panel Study of Income Dynamics; US, Understanding Society, the UK Household Longitudinal Study; WLS, Wisconsin Longitudinal Study; SHARE, Survey of Health, Ageing, and Retirement in Europe.
See Supplemental Material for details on measures and analysis for each cohort. Each parent study obtained informed consent from participants, and each parent study was approved by the institutional review boards of their respective institutions. Data are available to the public from the websites listed for each parent study. Previous analyses of purpose and mortality have been published for HRS (e.g. Shiba et al., Reference Shiba, Kubzansky, Williams, VanderWeele and Kim2022) and MIDUS (e.g. Hill & Turiano, Reference Hill and Turiano2014). For the present meta-analysis, we re-analyzed the data with the most recent data release from these samples to have the longest follow-up possible. Thus, we include findings from our updated analysis and not these previous publications.
Published literature
The literature search and meta-analytic synthesis followed the MOOSE recommendations for meta-analyses of observational studies (Stroup et al., Reference Stroup, Berlin, Morton, Olkin, Williamson, Rennie and Thacker2000).
Literature search strategy. We searched four electronic databases: MEDLINE/PubMed, Web of Science, PsycINFO, and PsycARTICLES. In addition, medRxiv and PsyArXiv were used to identify preprints of relevant studies. The searches included English publications across all years up to October 2025. The search terms were “purpose in life” OR “meaning in life” OR “life purpose” OR “life meaning” OR “ikigai” OR “usefulness in life” OR “engagement in life” AND “mortality” OR “survival” OR “longevity” OR “death.”
Selection criteria and quality assessment. Studies were included if the following criteria were met: (1) Study design: Longitudinal, observational study. (2) Study population: adults (18+) who reported on their purpose or meaning in life or related construct (e.g. ikigai), consistent with the previous meta-analysis (Cohen et al., Reference Cohen, Bavishi and Rozanski2016). (3) Vital status: vital status must be tracked over time, either through national registries or reported to the study by a knowledgeable informant. (4) Assessment of purpose/meaning: studies that reported how feelings of purpose/meaning were measured, including single items, standard questionnaire measures, and related constructs (e.g. ikigai). Purpose/meaning must be self-reported prior to mortality (i.e. retrospective ratings by informants were excluded). (5) For published studies with public data, if the public data had a longer follow-up than reported in the previous publication, a new analysis of the individual-participant data was included in the meta-analysis rather than the estimates from the previous publication to ensure the longest follow-up.
Two researchers (DZ and EM) screened the title, abstract, and keywords of each article for eligibility. The full text was examined when a study appeared to be eligible for inclusion. The full-text articles were independently assessed for inclusion by both researchers; discrepancies were resolved through discussion with ARS, ML, and AT. Articles had to be published in English; there was no restriction on publication date. The NIH quality assessment tool for observational cohort studies to rank studies by quality (Good, Fair, or Poor).
Statistical approach. Data were combined with random-effects meta-analysis to calculate the pooled effect size for the individual-participant data analysis, the published studies, and then all studies. Hazard ratios (HR) were prioritized. Effects reported as odds ratios and risk ratios in the published studies were considered as HR (sensitivity analysis that excluded those studies indicated that the meta-analytic effect was unchanged). HRs from continuous response scales were standardized; HRs from binary response scales were not. Continuous and binary response scales were analyzed together because the scales were assumed to measure the same underlying normally distributed construct, and meta-regression and a follow-up sub-group analysis directly tested for differences between the types of response scales (see below). Between-study heterogeneity was evaluated with Hedges Q, I 2, and tau2. Model 1 was the association between purpose and mortality, controlling for sociodemographic factors. The same set of covariates (age, sex, race, ethnicity, education) was used in the analysis of individual-participant data (as relevant to each sample); the exact covariates varied for the estimates from the published literature. In the individual-participant data only, a Model 1.1 that excluded deaths within a year of the assessment of purpose was run to help reduce the possibility of reverse causality. Moderation was tested with an interaction between purpose and each sociodemographic factor. In addition to individual-level moderators, meta-regression was used to identify study-level sources of heterogeneity, including content of the scale (purpose versus meaning versus ikigai), length of the scale (1-item versus multi-item scale), location of the sample (United States versus other), mean age of the sample, proportion female, follow-up length, year of publication, and data source (individual-participant data versus published study). We ran another random-effects meta-analysis for Model 2, which was the association controlling for clinical and behavioral covariates and Model 3 (individual-participant data only) that controlled for depression. Individual-participant analyses were conducted in SPSS. STATA was used for the meta-analyses.
Results
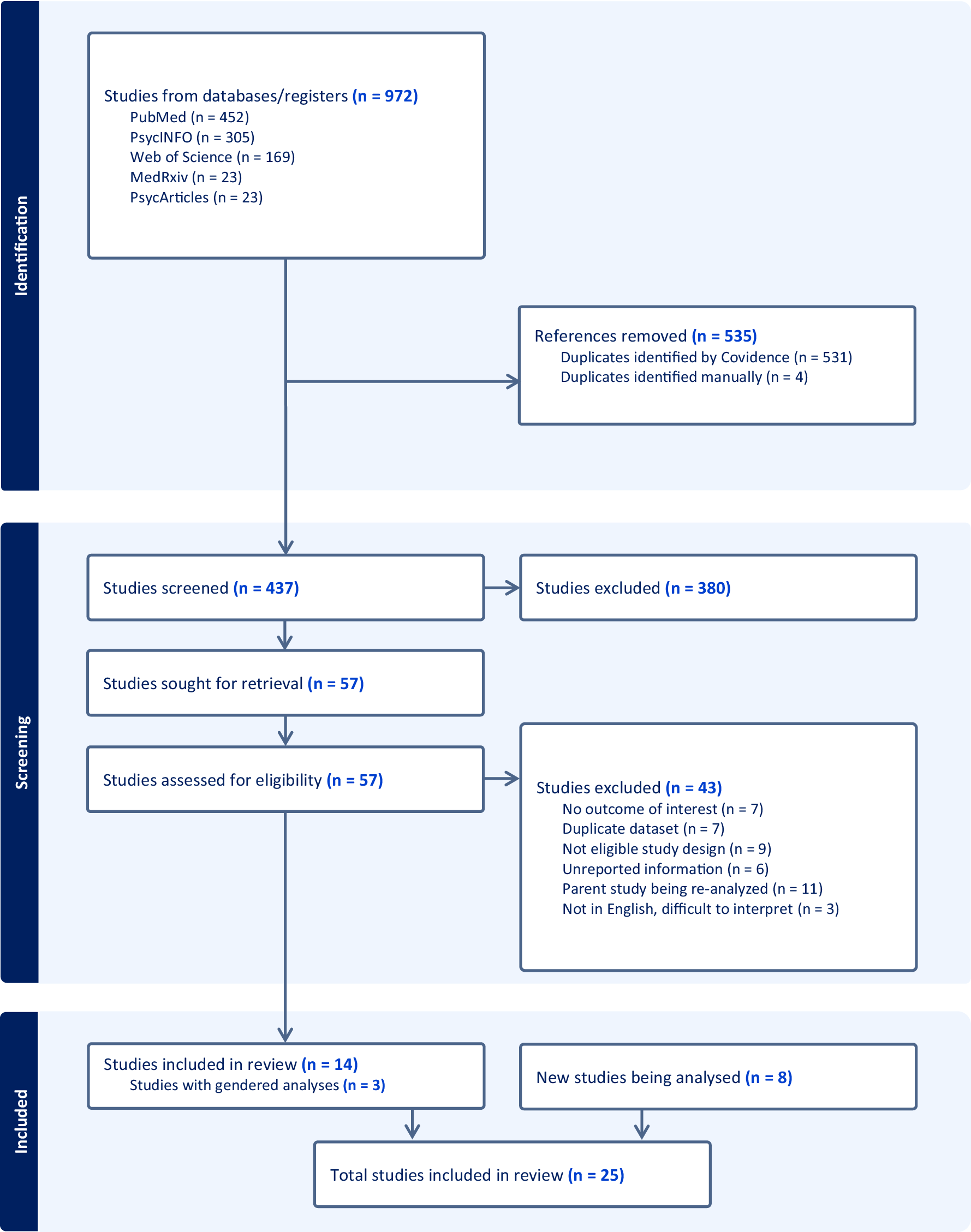
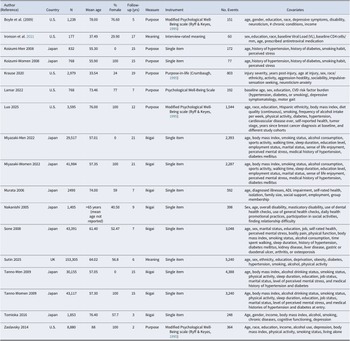
Table 1 reports descriptive statistics for the coordinated analysis of individual-participant data from the public datasets. Figure 1 reports the flowchart of the screening procedures for the published literature. A total of 972 records were identified from the initial literature search. No additional articles were identified through screening the reference list of previous reviews. After title, keyword, and abstract screening, 57 full-text articles were extracted. Of these, 14 articles (17 samples) were eligible for the meta-analysis. Table 2 reports the published articles identified through the literature search that were included in the meta-analysis. Supplementary Table S1 reports the selection and reasons for exclusion. All samples were rated as good quality based on the NIH quality assessment tool (Supplementary Table S2).
PRISMA flowchart of the screening process.

Figure 1. Long description
The flowchart is divided into three vertical phases.
1. Identification Phase.
At the top, a box lists Studies from databases/registers (n = 972), including PubMed (n = 452), Psyc I N F O (n = 305), Web of Science (n = 169), Med R x i v (n = 23), and PsycArticles (n = 23). An arrow points to a lateral box for References removed (n = 535), consisting of Duplicates identified by Covidence (n = 531) and Duplicates identified manually (n = 4).
2. Screening Phase.
The central flow continues to Studies screened (n = 437). An arrow points right to Studies excluded (n = 380). The main path proceeds to Studies sought for retrieval (n = 57), then to Studies assessed for eligibility (n = 57). An arrow points right to a large exclusion box for Studies excluded (n = 43) with reasons: No outcome of interest (n = 7), Duplicate dataset (n = 7), Not eligible study design (n = 9), Unreported information (n = 6), Parent study being re-analyzed (n = 11), and Not in English, difficult to interpret (n = 3).
3. Included Phase.
The flow reaches Studies included in review (n = 14), which includes Studies with gendered analyses (n = 3). A separate box for New studies being analysed (n = 8) joins the final step. Both point to the terminal box: Total studies included in review (n = 25).
Published articles identified through the literature search

Table 2. Long description
The table contains 10 columns: Author (Reference), Country, N (sample size), Mean age, % Female, Follow-up (yrs), Measure, Instrument, No. Events, and Covariates.
Key entries include:
* Boyle et al. (2009), U.S., N=1,238, Mean age 78.00, 76.60% Female, 5-year follow-up, measuring Purpose using a Modified Psychological Well-Being scale.
* Ironson et al. (2021), U.S., N=177, Mean age 37.49, 29.90% Female, 17-year follow-up, measuring Meaning via interview.
* Koizumi-Men and Koizumi-Women (2008), Japan, N=832 and 768 respectively, Mean age ~55, measuring Purpose with a single item.
* Miyazaki-Men and Miyazaki-Women (2022), Japan, N=29,517 and 41,984 respectively, Mean age ~57, measuring Ikigai with a single item.
* Sone (2008), Japan, N=43,391, Mean age 61.40, 52.47% Female, 7-year follow-up, measuring Ikigai.
* Sutin (2025), U.K., N=153,305, Mean age 64.02, 56.8% Female, 6-year follow-up, measuring Meaning.
* Tanno-Men and Tanno-Women (2009), Japan, N=30,155 and 43,117 respectively, Mean age ~57, measuring Ikigai.
* Zaslavsky (2014), U.S., N=8,880, Mean age 88, 100% Female, 2-year follow-up, measuring Purpose.
Covariates across studies typically include age, sex, education, race, body mass index, smoking status, and various health conditions like diabetes or hypertension.
Association between purpose/meaning in life and mortality
A total of 25 samples were included in the meta-analysis: 17 samples from 14 articles identified through the published literature search and eight cohort studies with individual-participant data. There were a total of 488,765 participants and 48,928 deaths over a follow-up of up to 32 years.
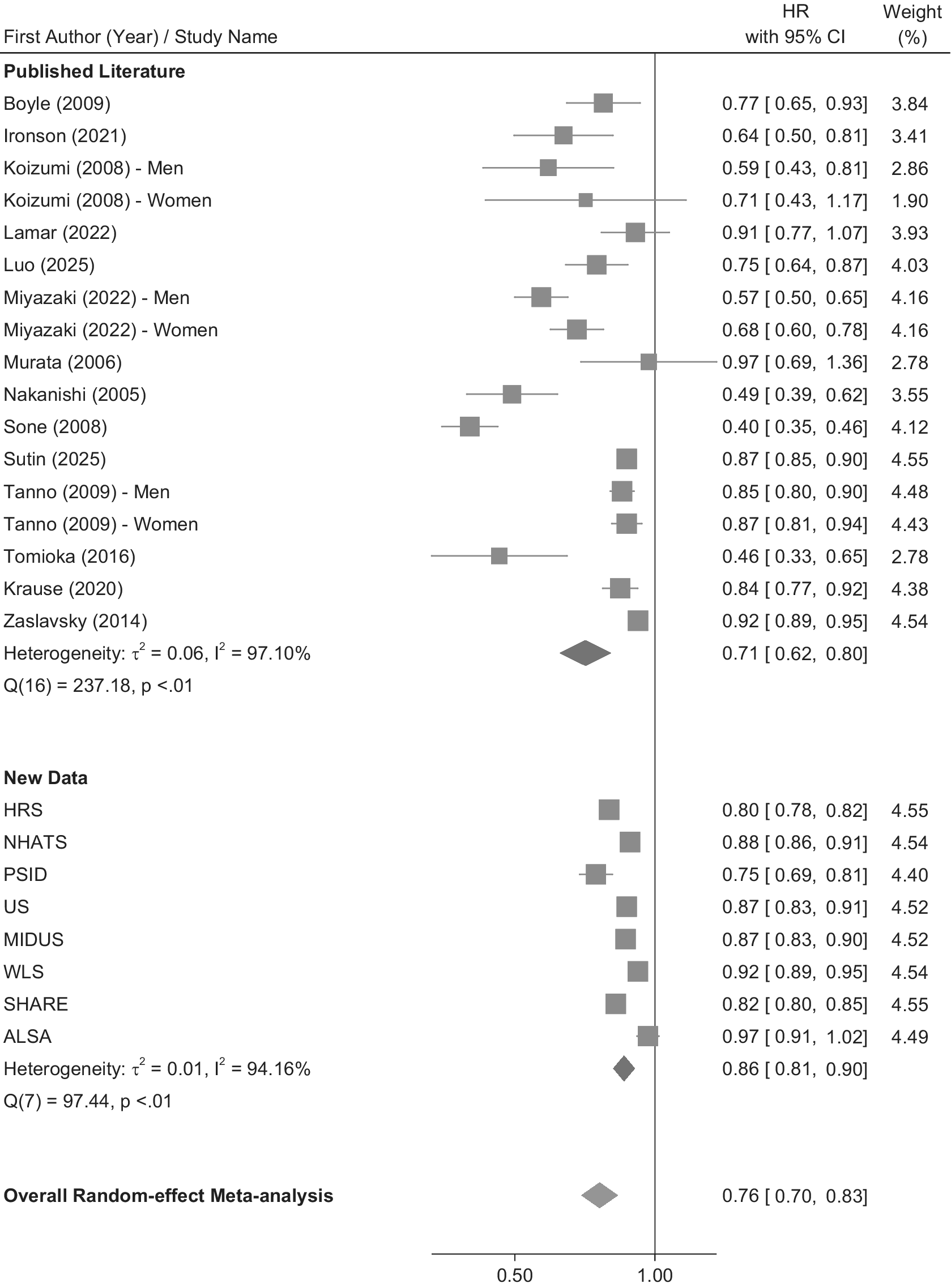
The results of the meta-analysis are in Figure 2 and Supplementary Table S3. As expected, purpose in life was associated with greater longevity: Higher purpose in life was associated with an approximately 30% lower risk of mortality (meta-analytic HR = .76, 95% CI = .70, .83). There was heterogeneity across studies (Q = 334.67, p < .001; I2 = 98.47%; tau2 = .05). The leave-one-out analysis, however, indicated that the meta-analytic effect was not dependent on any single study (Supplementary Table S4). The significant Egger’s test (Egger = −2.19, p = .004) suggested publication bias. Figure 2 and the funnel plot (Supplementary Figure S1) indicated that there was more variability across studies from the published literature (tau2 = .06) than the individual-participant data (tau2 = .01), which were more tightly clustered and symmetrical. The bias-corrected trim and fill estimate was similar to the original estimate (HR = .75, 95% CI = .68, .82). The association remained significant when deaths within 1 year of the purpose assessment were excluded from the analysis (individual-participant data only; Supplementary Table S5).
Forest plot of the association between purpose in life and risk of mortality.

Figure 2. Long description
The forest plot is organized into three vertical sections. The left column lists the First Author Year or Study Name. The center contains a graphical representation with a vertical line at 1.00 representing the null effect. The right column lists the H R with 95 percent C I and the Weight percentage.
Published Literature section includes 17 entries:
- Boyle 2009: 0.77 [0.65, 0.93], 3.84 percent.
- Ironson 2021: 0.64 [0.50, 0.81], 3.41 percent.
- Koizumi 2008 - Men: 0.59 [0.43, 0.81], 2.86 percent.
- Koizumi 2008 - Women: 0.71 [0.43, 1.17], 1.90 percent.
- Lamar 2022: 0.91 [0.77, 1.07], 3.93 percent.
- Luo 2025: 0.75 [0.64, 0.87], 4.03 percent.
- Miyazaki 2022 - Men: 0.57 [0.50, 0.65], 4.16 percent.
- Miyazaki 2022 - Women: 0.68 [0.60, 0.78], 4.16 percent.
- Murata 2006: 0.97 [0.69, 1.36], 2.78 percent.
- Nakanishi 2005: 0.49 [0.39, 0.62], 3.55 percent.
- Sone 2008: 0.40 [0.35, 0.46], 4.12 percent.
- Sutin 2025: 0.87 [0.85, 0.90], 4.55 percent.
- Tanno 2009 - Men: 0.85 [0.80, 0.90], 4.48 percent.
- Tanno 2009 - Women: 0.87 [0.81, 0.94], 4.43 percent.
- Tomioka 2016: 0.46 [0.33, 0.65], 2.78 percent.
- Krause 2020: 0.84 [0.77, 0.92], 4.38 percent.
- Zaslavsky 2014: 0.92 [0.89, 0.95], 4.54 percent.
- Subtotal Heterogeneity: tau-squared = 0.06, I-squared = 97.10 percent. Pooled result: 0.71 [0.62, 0.80].
New Data section includes 8 entries:
- H R S: 0.80 [0.78, 0.82], 4.55 percent.
- N H A T S: 0.88 [0.86, 0.91], 4.54 percent.
- P S I D: 0.75 [0.69, 0.81], 4.40 percent.
- U S: 0.87 [0.83, 0.91], 4.52 percent.
- M I D U S: 0.87 [0.83, 0.90], 4.52 percent.
- W L S: 0.92 [0.89, 0.95], 4.54 percent.
- S H A R E: 0.82 [0.80, 0.85], 4.55 percent.
- A L S A: 0.97 [0.91, 1.02], 4.49 percent.
- Subtotal Heterogeneity: tau-squared = 0.01, I-squared = 94.16 percent. Pooled result: 0.86 [0.81, 0.90].
Overall Random-effect Meta-analysis at the bottom shows a diamond centered at 0.76 [0.70, 0.83].
Moderators of the association between purpose and mortality
Results of the moderation analysis for the sociodemographic factors (age, sex, race, ethnicity, and education) are in Supplementary Table S6. The meta-analysis of interaction terms indicated that the association between purpose in life and mortality was slightly stronger among relatively younger than older participants (HRinteraction = 1.04, 95% CI = 1.01, 1.06, p = .003), among white than black participants (HRnteraction = 1.06, 95% CI = 1.01, 1.11, p = .011), and among relatively more educated than relatively less educated participants (HRinteraction = .98, 95% CI = .96, .99, p = .040) but no difference by sex (HRinteraction = .99, 95% CI = .96, 1.02, p = .707) or ethnicity (HRinteraction = 1.02, 95% CI = .95, 1.10, p = .533). It should be noted that the differences in association were in degree rather than kind, and p-values should be interpreted with caution, given the number of statistical tests. For example, among black participants, purpose in life was associated with lower risk of mortality (HR = .86, 95% CI = .80, .91, p < .001), an association just slightly weaker than for white participants (HR = .83, 95% CI = .78, .88, p < .001). Despite the statistical difference, the protective association was apparent in both populations.
Results of the meta-regressions are in Supplementary Table S7. The largest difference identified with meta-regression was the difference between when the predictor was measured with a binary versus continuous response scale: When the purpose-related construct was measured with a yes versus no binary response, it had a stronger association with mortality risk (HR = 0.62, 95% CI = 0.51, 0.76, k = 8) than when the purpose-related construct was measured with a continuous response scale (HR = 0.85, 95% CI = 0.82, 0.89, k = 17). The association was also stronger from the published literature (HR = 0.71, 95% CI = 0.62, 0.80, k = 17) compared to the individual-participant data (HR = 0.86, 95% CI = 0.81, 0.90, k = 8), when purpose was measured as ikigai (HR = 0.63, 95% CI = 0.51, 0.79, k = 8) compared to purpose (HR = 0.84, 95% CI = 0.79, 0.89, k = 12) or meaning (HR = 0.85, 95% CI = 0.81, 0.88, k = 4), and when the predictor was measured with a single item (HR = 0.69, 95% CI = 0.60, 0.80, k = 14) compared to a multi-item scale (HR = 0.86, 95% CI = 0.82, 0.90, k = 11). These differences, however, were due to the difference between the binary versus continuous response scale (i.e. the binary predictor was in the published literature, measured as ikigai, and a single item). When the binary versus continuous variable was accounted for in the meta-regressions, the other differences were no longer significant (all ps > .05). There was no difference by follow-up time, proportion of deaths, proportion female, sample age, whether the sample was clinical or community, whether the sample was from the United States or elsewhere, or the number of covariates included in the model. Quality assessment was not tested as a moderator because there was no variability in the rating (all were rated “good”). Of note, there was no difference in the association when the construct was measured as meaning compared to purpose.
Purpose and mortality accounting for behavioral and clinical risk factors
All samples included a model that accounted for at least some behavioral and clinical risk factors. The individual-participant samples controlled for physical activity, smoking, hypertension, diabetes, and obesity. The published literature had a model that controlled for a variety of covariates, from few (5; Koizumi, Ito, Kaneko, & Motohashi, Reference Koizumi, Ito, Kaneko and Motohashi2008; Krause, Cao, & DiPiro, Reference Krause, Cao and DiPiro2020) to many (21; Sone et al., Reference Sone, Nakaya, Ohmori, Shimazu, Higashiguchi, Kakizaki and Tsuji2008). The results of this adjusted model for each sample and the meta-analysis are in Supplementary Table S8. The association between purpose and mortality was attenuated by 38% ((HRmodel1 – HRmodel2)/(HRmodel1–1)) × 100) with the inclusion of these covariates (meta-analytic HR = .85, 95% CI = .82, .89), which suggested that these factors may be mechanisms or confounders in the pathway between purpose and greater longevity. The direct association remained significant.
Purpose and mortality accounting for depression
All samples with individual-participant data had a measure of depressive symptoms. Adjusting the model for depression attenuated the association by 62%, but it remained significant (meta-analytic HR = .91, 95% CI = .88, .94; Supplementary Table S9). There is thus a substantial overlap between purpose and depressive symptoms (meta-analytic association = −.32, p < .001; Sutin et al., Reference Sutin, Luchetti, Stephan, Karakose, Mansor and Terracciano2026), but a higher purpose in life continued to be associated with a lower risk of mortality, accounting for depression.
Discussion
The present research provides a 10-year update and extension of the meta-analysis on purpose in life and mortality published in 2016 (Cohen et al., Reference Cohen, Bavishi and Rozanski2016). The number of samples included in the meta-analysis increased from 9 to 25, the total sample size increased from 136,265 to 488,765, and the length of follow-up increased from up to 14 years to up to 32 years. The results of the current analysis support the robustness of the previous meta-analysis: Purpose in life was associated with an approximately 30% lower risk of mortality, an association statistically significant in 21 of the 25 samples (and in the same direction for the samples that were not statistically significant), and stronger when purpose was measured with a binary response scale (60% increased risk) than when measured with a continuous scale (18% increased risk per standard deviation), and stronger in the published literature (41% increased risk) compared to the individual-participant data (16% increased risk).
The previous meta-analysis found that purpose in life was associated with a nearly 50% reduced risk of mortality (Cohen et al., Reference Cohen, Bavishi and Rozanski2016). The slightly lower magnitude in the current meta-analysis likely reflects the greater number of studies with a continuous purpose scale compared to the previous meta-analysis and the inclusion of individual-participant data. Still, this updated meta-analysis supports the conclusion of the previous meta-analysis and strengthens the replicability and robustness of the association between purpose in life and lower risk of mortality. The leave-one-out analysis, for example, indicated that the association was not dependent on a specific study; the association was similar regardless of which study was not included. In addition, well-being tends to have a terminal decline at the end of life (Gerstorf et al., Reference Gerstorf, Ram, Mayraz, Hidajat, Lindenberger, Wagner and Schupp2010). As such, the association may have been driven by processes related to oncoming mortality rather than the protective association of purpose. That is, individuals approaching death may report less purpose, which could drive the association with mortality. The supplemental analysis that excluded participants who died within 1 year of their assessment of purpose, however, found that the association remained significant, excluding participants with impending mortality. Relatedly, meta-regressions found that follow-up time was unrelated to the strength of the association. There was significant heterogeneity that was not fully accounted for by the factors tested with meta-regression. This heterogeneity suggests pooled estimates should be interpreted as an average across highly diverse measures/contrasts rather than a single generalizable effect size. There may be other contextual factors not identified in this study that contribute to the magnitude of the association between purpose and mortality risk.
The present research significantly expands on the previous meta-analysis by addressing moderators, behavioral and clinical risk factors, and the role of depression in the association between purpose and mortality. Previous research that relied on a single sample has found that the association between purpose and mortality is slightly stronger among females than males, with no difference between black and white individuals (Shiba et al., Reference Shiba, Kubzansky, Williams, VanderWeele and Kim2022), and a slightly stronger association among individuals with relatively more than less education (Shiba et al., Reference Shiba, Kubzansky, Williams, VanderWeele and Kim2021). Other research that also used a single sample did not find a difference by sex, race, or education (Boyle et al., Reference Boyle, Barnes, Buchman and Bennett2009). And, indeed, the present research had mixed results for moderation across the individual samples tested. When aggregated in the meta-analysis, there were no differences by sex or ethnicity, but there were slight differences by race and education. These differences should be interpreted with caution, given the modest p-values (p = .011 and p = .040, respectively), the large sample, and the number of statistical tests. An interaction with age indicated that the association was slightly stronger among relatively younger than older participants. The association, however, was still apparent for the relatively older adults. Overall, there was more evidence of similarity than difference across sociodemographic groups, with just slight variations in the strength of the association rather than an absence of an association for specific groups.
The meta-regressions further supported the robustness of the associations. The most notable difference was the larger magnitude when the predictor was measured as a yes/no response compared to a continuous scale. This pattern is consistent with previous research on related constructs (Karakose et al., Reference Karakose, Miller, Luchetti, Stephan, Sutin and Terracciano2025; Luchetti et al., Reference Luchetti, Aschwanden, Sesker, Zhu, O’Súilleabháin, Stephan and Sutin2024) and reflects the difference between a binary yes/no contrast versus the effect of a single unit increment on a continuous scale. Other than this methodological difference, we found limited evidence for the other moderators we tested. The association did not differ, for example, by geographic location, length of follow-up, or type of sample (i.e. clinical versus community). In addition, although there are theoretical differences between purpose in life and meaning in life (Kashdan et al., Reference Kashdan, Goodman, McKnight, Brown and Rum2024), there was no difference in the strength of association between measures of purpose versus meaning on risk of mortality. This similarity suggests that either participants do not make a distinction between purpose and meaning when they report on it, and/or that both aspects of eudaimonic well-being are equally protective against earlier mortality.
There are likely to be multiple pathways between purpose and mortality. The present research addressed behavioral and clinical pathways because models of purpose and health tend to emphasize these pathways for specific health outcomes (Kim et al., Reference Kim, Delaney and Kubansky2019; Sutin et al., Reference Sutin, Luchetti and Terracciano2021) and because purpose is associated with established behavioral and clinical risk factors for mortality. Individuals higher in purpose, for example, are more physically active (Sutin, Stephan, Luchetti, & Terracciano, Reference Sutin, Stephan, Luchetti and Terracciano2023) and less likely to smoke (Weston et al., Reference Weston, Hill and Mroczek2024) or have hypertension, diabetes, or obesity (Hafez et al., Reference Hafez, Heisler, Choi, Ankuda, Winkelman and Kullgren2018; Kim et al., Reference Kim, Delaney and Kubansky2019). The present research found that behavioral and clinical factors accounted for about one-third of the association between purpose and mortality. This reduction suggests that these factors could be mediators, that is, mechanisms in the association between purpose and mortality (e.g. theoretically purpose contributes to healthier behavioral profiles that contribute to lower risk of mortality). Importantly, even if these factors are considered confounders (e.g. healthier individuals have both healthier behavioral profiles and higher purpose in life) rather than mediators, the significant association between purpose and mortality persisted (i.e. even accounting for the shared variance between purpose and healthier behavioral profiles, whether due to a third factor or a mechanistic pathway, purpose in life had an independent association with lower mortality risk).
There are numerous other pathways that may contribute to the association between purpose and mortality. One pathway may be through social processes. Individuals higher in purpose have more social support (Weston, Lewis, & Hill, Reference Weston, Lewis and Hill2021) and experience less loneliness (Sutin et al., Reference Sutin, Luchetti, Aschwanden, Lee, Sesker, Stephan and Terracciano2022). These social processes tend to be beneficial for health and longevity (Freak-Poli et al., Reference Freak-Poli, Ryan, Neumann, Tonkin, Reid, Woods and Owen2021). There could also be more direct biological pathways. Purpose is associated with healthier inflammatory profiles, which have previously been identified as mechanisms in the association between purpose and maintaining episodic memory over time (Sutin et al., Reference Sutin, Stephan, Luchetti and Terracciano2023). Poor inflammatory health is associated with earlier mortality (Li, Liu, & Xie, Reference Li, Liu and Xie2017), and thus may be a pathway from purpose in life to mortality.
The better regulation of stress associated with purpose may also culminate in a lower risk of earlier mortality. Individuals higher in purpose, e.g. tend to report less stress in general (Sutin et al., Reference Sutin, Luchetti, Stephan, Sesker and Terracciano2024), despite not experiencing more or fewer stressors in daily life compared to individuals lower in purpose (Hill et al., Reference Hill, Sin, Turiano, Burrow and Almeida2018). Likewise, individuals higher in purpose tend to have a similar initial response to stressors as individuals lower in purpose, but recover from them faster, as measured in the lab (Fogelman & Canli, Reference Fogelman and Canli2015; Schaefer et al., Reference Schaefer, Morozink Boylan, van Reekum, Lapate, Norris, Ryff and Davidson2013) and in daily life (Hill et al., Reference Hill, Sin, Turiano, Burrow and Almeida2018). Over time, these processes may protect the body from the harmful wear and tear of stress.
There is an association between purpose and depression: Individuals who have more purpose are less likely to experience depression (Boreham & Schutte, Reference Boreham and Schutte2023). Given that elevated depressive symptoms are also a risk factor for mortality (Zhang et al., Reference Zhang, Jackson, Gillespie, Merritt and Yang2023), the association between purpose and mortality may have been due to depression. Depression did account for almost two-thirds of the association between purpose and mortality, which was expected from a process-oriented perspective that views depression as one consequence of low purpose in life (Sutin et al., Reference Sutin, Luchetti, Stephan and Terracciano2026; Wood & Joseph, Reference Wood and Joseph2010). That is, depression may be a mechanism in the association between purpose and mortality risk. It did not, however, completely account for the association.
In addition to longevity, quality of life is an important consideration for older adults (van Leeuwen et al., Reference van Leeuwen, van Loon, van Nes, Bosmans, de Vet, Ket and Ostelo2019). From that perspective, purpose may also promote a better quality of life at the end of the lifespan. It is, for example, associated with the delayed onset of Alzheimer’s disease (Boyle et al., Reference Boyle, Wang, Yu, Barnes, Wilson and Bennett2022) and lower risk of incident disability (Boyle, Buchman, & Bennett, Reference Boyle, Buchman and Bennett2010) and better maintenance of physical function (Kim, Kawachi, Chen, & Kubzansky, Reference Kim, Kawachi, Chen and Kubzansky2017). Thus, in addition to extending lifespan, purpose may also help to compress morbidity to extend health span for as long as possible, contributing to a better quality, as well as quantity, of life.
The present research had several strengths, including the systematic review of the literature and the individual-participant data that included samples new to the literature on purpose and mortality. The larger sample sizes and longer follow-up provided more precise estimates of the overall effect and the opportunity for more robust testing of individual and study-level moderators. There are also limitations to address in future research. First, this research accounted for common behavioral, clinical, and psychological risk factors for earlier mortality, but there are other pathways that likely contribute to the association that were not addressed. Second, the literature search was limited to articles published in English, which may have introduced language/coverage bias, especially for non-English cohorts. Third, the moderation analysis suggested similarity in the association across sociodemographic groups; more diverse samples are needed to fully address generalizability. In particular, the samples in the current research were from high-income countries. Research on purpose and mortality is needed in lower- and middle-income countries to evaluate how widely its protective association generalizes.
Despite these limitations, the present research provides evidence for a robust and replicable association between purpose and mortality: Individuals higher in purpose and purpose-related constructs tend to live longer. Given that purpose in life can be increased through intervention (Manco & Hamby, Reference Manco and Hamby2021), it may be one possible target of intervention to increase the length of life as well as the quality of life.
Supplementary material
The supplementary material for this article can be found at http://doi.org/10.1017/S0033291726104863.
Acknowledgements
We gratefully acknowledge the parent studies whose public data made this work possible: The Health and Retirement Study is sponsored by the National Institute on Aging (NIA-U01AG009740) and conducted by the University of Michigan. The National Health and Aging Trends Study is sponsored by the National Institute on Aging (grant number U01AG032947) through a cooperative agreement with the Johns Hopkins Bloomberg School of Public Health.
Panel Study of Income Dynamics: The collection of data used in this study was partly supported by the National Institutes of Health under grant number R01 HD069609 and R01 AG040213, and the National Science Foundation under award numbers SES 1157698 and 1623684. British Household Panel Study: Understanding Society is an initiative funded by the Economic and Social Research Council and various Government Departments, with scientific leadership by the Institute for Social and Economic Research, University of Essex, and survey delivery by the National Centre for Social Research (NatCen) and Verian (formerly Kantar Public). The research data are distributed by the UK Data Service. The Midlife in the United States (MIDUS) is sponsored by the MacArthur Foundation Research Network on Successful Midlife Development (MIDUS I), the National Institute on Aging (P01-AG020166; MIDUS II), and grants from the General Clinical Research Centers Program (M01-RR023942, M01-RR00865) and the National Center for Advancing Translational Sciences (UL1TR000427). The Wisconsin Longitudinal Study (WLS) has been supported principally by the National Institute on Aging (AG-9775, AG-21079, AG-033285, and AG-041868) since 1991, with support from the Vilas Estate Trust, the National Science Foundation, the Spencer Foundation, and the Graduate School of the University of Wisconsin-Madison. Since 1992, data have been collected by the University of Wisconsin Survey Center. The English Longitudinal Study of Ageing is funded by the National Institute of Aging [grants 2RO1AG7644-01A1 and 2RO1AG017644] and a consortium of UK government departments coordinated by the Office for National Statistics. The content is solely the responsibility of the authors and does not represent the official views of the parent studies or funders. The SHARE data collection has been funded by the European Commission through FP5 (QLK6-CT-2001-00360), FP6 (SHARE-I3: RII-CT-2006-062193, COMPARE: CIT5-CT-2005-028857, SHARELIFE: CIT4-CT-2006-028812), FP7 (SHARE-PREP: GA N°211909, SHARE-LEAP: GA N°227822, SHARE M4: GA N°261982) and Horizon 2020 (SHARE-DEV3: GA N°676536, SERISS: GA N°654221) and by DG Employment, Social Affairs & Inclusion. Additional funding from the German Ministry of Education and Research, the Max Planck Society for the Advancement of Science, the National Institute on Aging (U01_AG09740-13S2, P01_AG005842, P01_AG08291, P30_AG12815, R21_AG025169, Y1-AG-4553-01, IAG_BSR06-11, OGHA_04-064, HHSN271201300071C) and from various national funding sources is gratefully acknowledged (see www.share-project.org). Australian Longitudinal Study of Aging: The first four ALSA waves were funded by the US National Institute on Aging (AG 08523-02). Other funding sources have included the Australian Research Council (DP0879152 and DP130100428).
Funding statement
Research reported in this publication was supported by the National Institute on Aging of the National Institutes of Health under Award Number R01AG074573. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. The funder had no role in study design, analysis, interpretation, preparation of the manuscript for publication, or the decision to publish.
Competing interests
The authors have no conflicts of interest to report.
Ethics standards
IRB approval was not necessary because this research used de-identified data from public datasets and the published literature.




 Open access
Open access