

Key messages
Chapter 3.8 highlights the importance of financing as a tool for preparing for and responding to pandemics. A pandemic can wreak health, societal and economic havoc. Prioritizing common and global public goods for health and specifically for pandemic planning is complex and requires financing mechanisms at the national, regional and supranational levels. Key learning, including from COVID-19, is that:
Pandemic preparedness is subject to inherent market and collective action failures and is often underfunded.
Governments need clear strategies for funding preparedness.
Preparedness depends on strong health system foundations and contingency funding mechanisms that go beyond simply setting funds aside. It is crucial that funds can be mobilized quickly and in a coordinated fashion.
Key steps for planning responses include:
○ assessing existing activities and mapping value for money;
○ agreeing on the need for public financing for population-based functions (i.e. common goods);
○ identifying appropriate types of financing that reflect the complexity of determining resource needs and allow for nuanced cost estimation;
○ developing context-specific financing tools that include flexible funds and address accountability;
○ holding transparent discussions about trade-offs;
○ improving budget transfer mechanisms;
○ integrating domestic finance into multiyear budgets; and
○ managing and strengthening international collaboration.
International guidance and learning from COVID-19 can help inform preparations. Organizations including the World Health Organization (WHO) and the World Bank offer tools to help decision-makers. It is crucial that these are assessed for suitability to context and customized to the national and local setting.
Introduction
COVID-19 highlighted the catastrophic health, social and economic havoc that a pandemic can wreak. The widespread health and socioeconomic impacts of the COVID-19 pandemic devastated lives and livelihoods both directly and indirectly. Its impacts on health were not just the illness and deaths caused by the virus itself, but also its knock-on effects on noncommunicable diseases, mental health and health service delivery. Globally, COVID-19 caused major blows to the progress towards the Sustainable Development Goals (United Nations, n.d.) and disproportionately affected the poor and vulnerable groups in society. In 2020 alone, the global economy contracted by 3.6% (United Nations, 2021) and the pandemic further exaggerated disparities between individuals, groups, regions and countries (Blake & Wadhwa, Reference Blake and Wadhwa2020). Supranational/global plans for pandemic preparedness have proliferated and multilateral support for low- and middle-income countries (LMICs) is available in the form of soft loans (see Chapter 1.4). Yet, nationally, governments devote only a fraction of domestic resources to support national preparedness and capacity development. National pandemic preparedness strategies have often been unclear and have lacked realistic financial mobilization plans, as seen during the COVID-19 pandemic (The Independent Panel for Pandemic Preparedness & Response, 2021).
In terms of national health financing, there are specific aspects of funding pandemic preparedness that set it apart from the support required for personal health services. Supporting prevention and preparedness activities involves specific budgets and considerations of institutional capacity, including measurable costs with their own financing streams, as well as dedicated financing mechanisms (WHO, 2021a). Establishing adequate prevention and preparedness systems is a long-term process that varies country by country.
Critical prevention and preparedness activities go beyond the health sector and have implications for overall government, community and global systems (for a global response that takes into account the reasons for the emergence of new viruses, see the summary of the One Health approach in Box 3.8.1). While health system foundations necessary for pandemic preparedness often sit under the purview of the health sector and ministries of health, preparedness and response-related activities are often financed and implemented by a larger range of agencies and government sectors at national and subnational levels (e.g. national centres for disease control, customs/border control, defence agencies, emergency services and various regulatory agencies) (Global Preparedness Monitoring Board, 2019; World Bank Group, 2019b; WHO, 2021b). Budget transfer mechanisms are often used to move funds that serve the entire population across sectors and levels of government, enabling coordination and efficiency.
Established in response to the H5N1 highly pathogenic avian influenza, the One Health approach explicitly recognizes the influence of the human-animal interface and changing ecosystems on the spread of infectious disease. Various global bodies, including the WHO, the United Nations’s Food and Agriculture Organization, the World Bank and UNICEF, together produced a strategic framework, One Health, that focuses on priority areas for financing and implementation in order to diminish the risk and minimize the impact of epidemics and pandemics caused by emerging infectious diseases, including those of animal origin (i.e. zoonotic diseases) (CDC, 2021). The priority areas comprise of intelligence, surveillance, emergency response systems, strong public and animal health services and effective communication. Implementing One Health explicitly requires multidisciplinary, multinational and multisectoral approaches, which has implications for both governance and financing mechanisms (Food and Agriculture Organization of the United Nations et al., 2008).
Financing mechanisms for pandemic preparedness must be set up in a way that ensures that the necessary systems are already in place to respond when a pandemic (or other crisis) hits. Both nationally and globally, this requires proactive planning and mechanisms that can be quickly and flexibly activated. Due to the inherent uncertainty and fluid dynamics of such events, financing mechanisms that can be deployed rapidly and with strong systems of accountability are critical for an effective and timely response. This goes beyond setting funds aside, and rather comprises contingency funding mechanisms that can be quickly mobilized in ways that coordinate with and build upon other efforts.
This chapter focuses on those financing mechanisms that are distinct from and in addition to the general health system financing that relates to personal health services. These aspects of health financing are covered in other chapters in this volume. However, it is important to note that there are many aspects of personal health services that are critical to pandemic preparedness. In other words, the capacities required for effective pandemic prevention, preparedness and response generally rely on a strong health system foundation (WHO, 2021b).
In this chapter, we first define pandemic preparedness and set out the notions of common goods for health and market failures. We describe the particular challenges of financing pandemic preparedness, including high levels of uncertainty, limited resources and competing priorities, cross-border and cross-sectoral governance arrangements, and issues related to funding common goods for health. We outline how to decide what to finance and how to ensure value for money; we then examine the various financing mechanisms available. Throughout the chapter, we draw upon evidence from country examples to highlight lessons for health policy-makers.
What is pandemic preparedness?
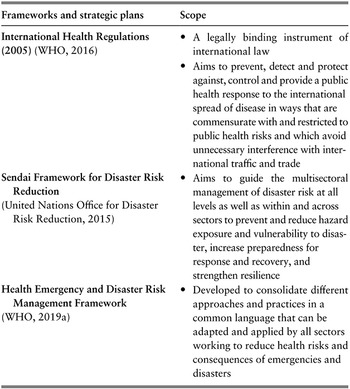
Over the last few decades, there has been growing recognition that the world is unprepared for pandemics (Commission on a Global Health Risk Framework for the Future & National Academy of Medicine, Secretariat, 2016; Soucat, Reference Soucat2019). This was emphatically reinforced by the COVID-19 pandemic. Various national and international bodies have drawn up frameworks and strategic plans to anticipate and reduce the threat of new and existing hazards (Table 3.8.1). These instruments all share the common objective of setting countries, and the world, on a path towards a sustainable future, by introducing measures that minimize vulnerability and strengthen resilience. Generally, the instruments cover a broad remit across all-hazards and all-risks of public health concern as described in the WHO Health Emergency and Disaster Risk Management Framework (e.g. outbreaks of any disease or the occurrence of disasters due to natural hazards or chemical incidents (WHO Regional Office for Europe, n.d. a)). While the financing mechanisms and investment approaches are not necessarily distinct across all these risk domains, our focus is specifically on the financing for pandemic preparedness.

Table 3.8.1 Long description
The table has 10 columns: Name, About or purpose of prize, Prize amount, Stakeholders involved, Eligibility criteria and disease focus, How is prize awarded, Who was awarded, Type of technology, Targeted R and D stage, and I P R implication. It reads as follows. Row 1: XPRIZE Foundation (10 million U S D). About: Milestone inducement prize. Non-profit organisation that designs and hosts public competitions intended to encourage technological development to benefit humanity. Many of the prize competitions are not global health or neglected disease-specific. In 2008, the Foundation has recently partnered with the Bill and Melinda Gates Foundation to develop a prize for a better T B diagnostic tool. Stakeholders involved: Prize partners: B M G F; Qualcomm Foundation, A N A, American, Telemedicine Association, Arthur Clarke Center for Human Imagination, Continua Health Alliance, Health 2.0, H I M S S, I E E E, MemsIndustry Group, Point Clear Solutions, Open Photonics Inc., Quest, Shimmer, U S San Diego Clinical and Translational Research Institute, Wireless Life Sciences Alliance and Xamarin. Eligibility criteria: T B; The winning team was required to develop a tricorder device that: 1. accurately diagnose 13 health conditions; 2. capture five real-time health vital signs; 3. provide a compelling consumer experience. How is prize awarded? Any company can enter a competition-style prize, with awards to first and second place among competing teams from various companies. Who was awarded? Pennsylvania-based team, Final Frontier Medical Devices (first place). Taiwan-based finalist, Dynamical Biomarkers Group (second place). Type of technology: Diagnostics. Targeted R&D stage: Clinical testing and registration. The foundation conducts consumer testing at the Altman Clinical and Translational Research Institute. This testing included the same rigour and protocols as a clinical trial but focused on the objectives of the XPRIZE competition. I P R implications: No information found.
Row 2: E U Vaccine Prize (2 million Euros). About: Inducement prize competition launched in 2012 by the European Commission, with more prizes to be offered via the Horizon 2020 Research Funding programme. The prizes intend to accelerate the development of vaccines and solve common issues of vaccine access. Stakeholders involved: Donors: E U Research Council. Eligibility criteria: Cold chain development for vaccines. Competition criteria, includes alternative ways of formulating, preserving or transporting vaccines. How is prize awarded? Competition cash prize with a jury appraising submissions and deciding on winner. No particular approach was prescribed and competitors were invited to convince the jury that their solution could respond best to the competition criteria, including alternative ways of formulating, preserving or transporting vaccines. Who was awarded? CureVac G m b H (2014). Type of technology: Vaccines. Targeted R&D stage: Discovery, preclinical and clinical stages, and registration. I P R implications: Owner maintains I P R.
For the purposes of this chapter, we follow the Global Preparedness Monitoring Board (2019) (an independent monitoring and advocacy body) in defining preparedness as follows:
the ability (knowledge, capacities and organizational systems) of governments, professional response organizations, communities and individuals to anticipate, detect and respond effectively to, and recover from, the impact of likely, imminent or current health emergencies, hazards, events or conditions. It means putting in place mechanisms that will enable national authorities, multilateral organizations and relief organizations to be aware of risks and deploy staff and resources quickly once a crisis strikes.
The definition thus encompasses both “prevention” and “response” as part of being prepared.
Common goods for health and market failures
The financing rationale for pandemic preparedness presented in this chapter is informed by WHO’s Common Goods for Health agenda.Footnote 1 This defines common goods for health as all population-based functions or interventions that require public financing (supplemented by donor funding in some cases), regardless of whether they are delivered by public or private sector providers, and that fulfil the following conditions:
Common goods for health contribute to human health and sustained economic progress over the long-term.
Provision or preservation of common goods for health are subject to specific market failures, typically because they are either public goods (meaning they are non-rival – so the consumption of the good by an individual does not affect the amount available for others – and non-exclusionary – available for all to use (Samuelson, Reference Samuelson1954)), or they have large social externalities.
Despite their importance and the necessity of public financing to support them, common goods for health suffer from both market and collective action failures, and as a result are often underfunded and underprovided for relative to investments in personal, facility-based services (Gaudin et al., Reference Gaudin2019). For many common goods for health expenditures, which can be either capital or recurrent in nature, it is impossible to charge a price (or a fine) to some or all users or consumers of the function. This can discourage private actors from financing common goods for health for fear that others will “free-ride” on their investments, and it limits optimal production. Pandemic-related activities can be usefully classified as common goods for health (Yazbeck & Soucat, Reference Soucat2019). These activities are notable for their market and collective action failures, which lie at the heart of their underinvestment. This means that the predominant source of funding for pandemic preparedness activities will be through public revenues as described later in this chapter.
In the next section we look at how to decide what preparedness activities to finance at both national and global levels, and how to ensure value for money.
Financing pandemic preparedness: the challenges
Despite the resource gaps in their strategies for pandemic preparedness, many countries have yet to commit to firm plans for financial mobilization. This is partly related to the high levels of uncertainty in this area, the delayed and often difficult-to-measure benefits of preparedness financing and differing attitudes to risk among decision-makers. Governments’ failure to commit is also because pandemic preparedness is only one of many competing priorities for health finances. Global institutions, too, must decide how best to fund crisis preparedness.
Challenge 1: How to decide how much and what to finance?
Deciding what to finance at the country level depends on first assessing the existing pandemic preparedness activities and resources and then identifying the gaps, in the context of total available resources. While the activities for prevention and preparedness are varied and many, guiding questions can be asked of each activity’s cost estimate, such as:
Which threats are being addressed (e.g. pandemic only, or broader emergency and disaster risks)?
What stage of the pandemic do activities correspond to: acute, protracted or no one particular stage?
Do they include animal health along with human health activities?
Do they include health system-related activities that help to improve health even in times of no pandemic?
Are they health-only or do they include non-health-related activities?
At the global level, there have only been a few attempts to understand the resource needs for preparedness. What is clear is that greater investment is needed than has occurred traditionally. Pre-COVID-19, the World Bank estimated that global investments in preparedness need to be approximately US$ 4.5 billion per year (World Bank, 2012). Others estimated even larger sums such as US$ 12.3 billion in one-time capital costs, with US$ 13.8 billion yearly recurrent costs (Peters et al., Reference 569Peters2019). Estimates made after the onset of the COVID-19 pandemic by McKinsey and Co. put the figure at many more billions of dollars – US$ 285 billion to US$ 430 billion over 10 years, with many of the costs being incurred as start-up capital costs in the first few years, and sustained annual costs over the time frame (Craven et al., Reference Craven2020).
Beyond estimating potential costs, there has also been an effort to track external assistance for common goods for health at the global, regional and country levels (Schaeferhoff et al., Reference Schaeferhoff2019). One study estimated that in 2017 there was US$ 0.48 billion allocated to global functions for pandemic preparedness and an additional US$ 1.36 billion for control of cross-border disease global functions (e.g. information exchange, early warning and response systems, risk assessment). Despite these efforts, there is a clear disconnect between the amounts committed as external assistance and the amounts needed (Yamey et al., Reference Yamey2019).
At the country level, the activities to be financed can be established as part of a pandemic risk management plan. When undertaking such plans, it is first useful to undertake a resource mapping exercise to understand where resources are currently being allocated, so that gaps and areas for improvements can be identified. Tools to conduct such mappings include the World Bank’s Health Security Financing Assessment (HSFA) tool and WHO’s REMAP tool (Osornprasop et al., Reference Osornprasop2020; WHO, 2019b). Once resources have been mapped, these can be integrated into planning for current and future preparedness activities, and also costed. WHO developed a National Action Plan for Health Security (NAPHS) framework, which provides a costing tool and has been implemented in several countries. The NAPHS plans conducted to date show high variation in cost distribution and estimates within NAPHS technical areas (World Bank Group, 2019b).
When using these costing tools, policy-makers must make careful consideration of cost drivers and the extent to which they are assessed in these models. For example, in Nigeria, three different pandemic costing tools were comparatively implemented and it was found that while in reality the high cost of developing and maintaining a strategic stockpile of medical countermeasures was a very large cost driver, this was not included as a category in several of the tools. In a similar costing exercise undertaken in Tanzania, animal health activities, such as animal vaccination, were another potentially large cost driver, but did not always feature in costing exercises (Mghamba et al., Reference Mghamba2018). Therefore, in decision-making when planning for pandemic preparedness, it is important to weigh the benefits and constraints of different tools and frameworks and consider how accurately they will estimate resource needs.
Challenge 2: How to ensure value for money?
To understand what constitutes a good investment in pandemic preparedness, it is necessary to look at the value for money of the different potential activities. The cost–benefit outcomes for pandemic preparedness are usually quite favourable due to the large impacts of catastrophic events compared to the costs of prevention, and the related co-benefits of tackling other health issues such as antimicrobial resistance (AMR) (Jonas, Reference Jonas2013). A key challenge, however, is to understand the probability of the catastrophic events occurring and to achieve the right balance of investment for preparedness without drawing resources from other essential activities. The assessment of value for money of activities for all health emergency preparedness also faces challenges such as high levels of uncertainty, uneven impacts and the differing perspectives (including attitude to risk) represented in the health system (Branch-Elliman, Safdar & Nelson, Reference Branch-Elliman, Safdar and Nelson2021).
Moreover, it is not a one-off decision. Policy-makers need to establish and maintain systems for ongoing assessments of the value for money of prevention and preparedness activities in order to continuously inform financing decisions based on the expected costs, the potential impacts from different risks, and overall budget availability. In addition, other elements besides cost may factor into decision-making. For example, the “rule of rescue” principle (when the perceived health needs of an individual or particular group override all other considerations) or wider societal priorities might lead policy-makers to invest in certain areas of preparedness regardless of their cost–effectiveness. The value-for-money considerations will also need to account for financial considerations of affordability and understanding of where costs are incurred. For example, costs for a large vaccine development programme may be incurred at the global level, while the delivery costs for the subsequent vaccinations would be borne by health system budgets at national or subnational level.
Once resource needs are estimated and value for money is assessed, financing mechanisms need to be established to execute preparedness activities. The next sections provide understanding on how to finance the activities needed for pandemic preparedness.
What financing mechanisms are available?
Financing mechanisms for pandemic preparedness sit at the supranational/global, national and subnational levels. While this section focuses primarily on national and subnational mechanisms, it also provides a brief overview of supranational/global mechanisms. First, however, we look at the recommendations for preparedness actions made by a number of high-level global expert review panels,Footnote 2 which helps provide the strategic context for the financing mechanisms we then go on to describe.
High-level recommendations
Despite providing separate analyses and recommendations, there is convergence around several global and domestic financing priorities needed for preparedness – especially in the wake of the COVID-19 pandemic. In its report on Improving Pandemic Preparedness by 2025, the Wellcome Trust (2021) summarizes these as follows.
1. Pooled financing at the global level for global public goods
Funding should be pooled at the global level to finance global public health goods, such as global surveillance of major health threats, grant financing to regional or country-level investments, manufacturing and delivery of countermeasures and R&D (G20 High Level Independent Panel on Financing the Global Commons for Pandemic Preparedness and Response, 2021; The Independent Panel for Pandemic Preparedness & Response, 2021; Pandemic Preparedness Partnership, 2021). Multilateral institutions, governments and nongovernmental organizations should provide contributions to these funds based on their ability to pay, amounting to approximately US$ 10 billion per year (G20 High Level Independent Panel on Financing the Global Commons for Pandemic Preparedness and Response, 2021; The Independent Panel for Pandemic Preparedness & Response, 2021). The governing bodies to allocate and monitor funding from these types of pools could be embedded in pre-existing agencies (e.g. the Investment Board of the World Bank), or set up as a new institution (e.g. an international pandemic financing facility) (G20 High Level Independent Panel on Financing the Global Commons for Pandemic Preparedness and Response, 2021; The Independent Panel for Pandemic Preparedness & Response, 2021).
2. Recommendations for Multilateral Development Banks (MDBs)
MDBs should include pandemic preparedness in their core mandates and add it into their major assessment tools (e.g. International Monetary Fund’s (IMF’s) Article IV) (G20 High Level Independent Panel on Financing the Global Commons for Pandemic Preparedness and Response, 2021; The Independent Panel for Pandemic Preparedness & Response, 2021; Pandemic Preparedness Partnership, 2021; McKee, 2021). Influential governments should raise pressure on these banks to ensure they increase lending for health and require health-related considerations to be incorporated into banks’ and borrowers’ business strategies, risk management frameworks and targets (G20 High Level Independent Panel on Financing the Global Commons for Pandemic Preparedness and Response, 2021; McKee, 2021).
3. Domestic financing and preparedness
Governments should renew their focus on resilient domestic finances for preparedness (G20 High Level Independent Panel on Financing the Global Commons for Pandemic Preparedness and Response, 2021). As part of this, each country should consider the cost implications of a NAPHS, including how it fits with overall health system financing, and ensure that any external financing for these objectives complements the domestic financing agenda (G20 High Level Independent Panel on Financing the Global Commons for Pandemic Preparedness and Response, 2021). Measurable targets and benchmarks for countries’ pandemic preparedness and response capacities are an important element to monitor progress (The Independent Panel for Pandemic Preparedness & Response, 2021). As part of this, WHO should advise on how National Health Accounts systems can be used to define and track expenditure on preparedness activities to help monitor and incentivize investments in preventive services for health security (G20 High Level Independent Panel on Financing the Global Commons for Pandemic Preparedness and Response, 2021; McKee, 2021).
It is the financing mechanisms available at the national level that we turn to first.
National-level mechanisms
As mentioned above, investments in pandemic preparedness activities are made in the context of competing demands for scarce budget resources. Countries face one or both of the following challenges: (i) fiscal, where they do not have enough resources; and (ii) prioritization, where they do not give high priority to investments in prevention and preparedness. The latter may be for several reasons, depending on preferences, incentives, politics or, as is likely, a mix of all of these.
At the national level, strategies to increase the investment base for pandemic preparedness include generating domestic resources from taxes or levies, introducing incentive mechanisms that increase awareness of the risks of infectious disease outbreaks to businesses, leveraging insurance models and pooling donor resources within specific prevention and preparedness and response funds or institutions (International Working Group on Financing Preparedness, 2017).
The precise form of the financing mechanism used not only depends on the level at which the prevention and preparedness activities reside, but also on the nature of what needs to be financed. Financing for pandemic preparedness can generally be differentiated into three types:
1. upfront capital investments for systems and infrastructure;
2. sustained, long-term financing for ongoing operations and recurrent costs; and
3. rapidly scalable surge financing that is, ideally, strategically identified in advance of an emergency, and able to be quickly deployed (Bill & Melinda Gates Foundation, 2021).
Here, we consider the available financing mechanisms in terms of revenue and the role of domestic resources; external assistance and loans; purchasing/payment mechanisms; incentivizing preparedness; and a variety of options for public financial management systems to enable both flexible and accountable financing arrangements.
Revenue and role of domestic resources
Domestic expenditure responsibility is often split between central (national) and state/local (subnational) budgets (International Working Group on Financing Preparedness, 2017). For example, in 2016 approximately 75% of all health security-related funding occurred at the provincial level in Viet Nam (see the Evidence in practice section) (Osornprasop et al., Reference Osornprasop2020). Given the need for a coordinated pandemic preparedness strategy, the dynamic between levels of government requires not only targeted governance platforms, but also financing mechanisms that can incentivize cooperation and joint approaches. For example, conditional transfers can influence and support allocation decisions by only allowing funding to be allocated when certain conditions and standards have been met (Jiménez Fernández de Palencia & Pérez-Foguet, Reference Jiménez Fernández de Palencia and Pérez-Foguet2011; Watabe et al., Reference Watabe2017). This approach is especially useful in devolved settings, where priority-setting and budget allocation decisions are made at subnational levels of government.
These explicit financing incentives also require regulatory, governance-related interventions and systems in place that allow for adaptation in the face of crisis. For example, in the face of COVID-19, the Brazilian intergovernmental transfer system was found to lack adaptability to transfer funds based on epidemiological need rather than on population size, and as a result funding for the pandemic response at the subnational level was insufficient (Fernandes & Pereira, Reference Pereira2020). Argentina, in contrast, successfully leveraged its pre-existing conditional grant system to enable fast and responsive funds to meet the needs created by COVID-19 (Barroy et al., Reference Barroy2020b; Sabignoso, Reference Sabignoso2021).
External assistance and loans
In many LMICs, domestic public resources are complemented by development assistance funding (see Chapter 1.4). This can include linking development assistance for capital or one-time expenses with domestic budget funding for recurrent costs for ongoing operations and human resources (World Bank Group, 2019b). Development assistance can also supplement domestic budget allocations for preparedness with matching grants, or by converting debt to grants upon reaching agreed-upon performance benchmarks through “buy-down” approaches. When executed successfully, this type of complementarity and strategic pooling of resources can contribute to a domestically led and sustained preparedness system. The dominant role of domestic financing for national and subnational level preparedness activities is seen across a range of countries, including Indonesia, Kenya, Lao People’s Democratic Republic, the Philippines, Uganda, Viet Nam, to name a few (Barroy et al., Reference Barroy2020b; Development Initiatives, 2017; Hanvoravongchai et al., Reference Hanvoravongchai2010; Osornprasop et al., Reference Osornprasop2020; Panelo, Reference Panelo and Caballero-Anthony2009).
Global mechanisms that support national-level financing of pandemic preparedness include emergency financial reserves; building contingency capacity for disasters into planning processes; emergency supply prepositioning and training; and forecast-based financing. While external assistance can play a critical supplementary role, it can also have unintended negative consequences. The delay between donor pledges and actual funding received can create inefficiencies in response activities. Such delays have obliged businesses and other stakeholders in recipient countries to use credit to meet their operating expenses. Procurement often requires money in the purchasing body’s bank before placing an order and manufacturing also takes time, which can delay the delivery of often critical goods and services. These delays are compounded by the weak health systems in many countries which are the true binding constraint to effective preparedness capacities (Board on Global Health et al., 2016). As a result, there are important considerations to be considered when utilizing these global funding mechanisms to ensure they achieve their end goals in the most effective and efficient way possible.
Flexible, accountable public financial management systems
Timely, agile and sustainable financing is critical to pandemic preparedness financing. Systems for managing public finances for pandemic preparedness therefore need to be flexible, yet still retain their accountability. Beyond revenue availability, the public financial management systems through which funds are allocated, expended and accounted for are central to meeting these objectives.
Public financial management objective 1: flexibility
Lessons from the Ebola epidemic in west and central Africa in 2014 highlight that flexible (unearmarked), rapidly disbursable funds are critical to meet the ever-changing needs of a public health emergency (World Bank Group, 2019a). The financing-related problems encountered in the epidemic included: delays in disbursement of funds, ineffective use of financing, bureaucratic delays, poor transparency and information sharing, lack of accountability and systems to track funds, low capacity to properly procure and enforce financing management – and all of these issues relate to the mechanics of financing rather than the overall resource envelope (World Bank Group, 2019a).
The need for financing mechanisms that are quick, easy to activate, flexible, and accounted for was seen again in the COVID-19 pandemic (Barroy et al., Reference Barroy2020b). Delayed and ad hoc funding is often at the heart of humanitarian agency concerns about their ability to effectively respond to crises (OECD, 2017). However, as discussed above, projecting how much to budget for preparedness activities in the face of resource constraints can be challenging due to the uncertainty of events (Board on Global Health et al., 2016). Still, the level of agility of fast and flexible spending can be enabled through prenegotiated plans delineating ex post and ex ante financing (Board on Global Health et al., 2016). Some countries may make public financial management adjustments to expand and reprioritize budgetary space to allow funds to flow to preparedness activities (Ndii, Reference Ndii2010).
Additional considerations are particularly necessary in fragile and conflict-affected settings where government capacity for intervention is severely limited. The collective action and consensus building essential for sustainable government action in favour of the commons is a special challenge in countries where societies have been fractured (Adulyanon, Reference Adulyanon2012). At the same time, investing in preparedness activities in these settings has particular urgency, given the potential deficits in the capacity, willingness and ability of the government to ensure provision of these goods. Actions to finance pandemic preparedness in these settings can include: targeted capacity-building efforts; coordination of external agencies’ funding; or, in cases where government structures and processes are too weak, establishment of a substitute or shadow process that can be transitioned to domestic institutions as soon as possible.
In countries where governments have greater capacity to act, programme budgeting offers a way of managing public finances that can allow the flexibility that responding to a pandemic requires. The multisectoral nature of pandemic preparedness means that different parts of the public sector may be responsible for both financing and provision of these activities. From a budgetary perspective, the structure of a country’s budget can place constraints on effectively matching financing with prevention and preparedness objectives (Barroy et al., Reference Barroy2018). For example, rigid line-items can be obstacles to the cross-cutting approaches needed to drive efficiency in organizing, delivering and rapidly deploying prevention and preparedness activities (Sparkes, Kutzin & Earle, Reference Sparkes, Kutzin and Earle2019). Moving away from input-based budgets and towards budgets that are formulated and executed based on programmes can help strengthen the linkages between budget allocations and government priorities, as well as foster the flexibility to quickly adapt budgets in the face of crisis (Barroy et al., Reference Barroy2020a). Australia’s experience of programme budgeting provides an example of how such arrangements can support cross-cutting investments in common goods for health (Australian Government, 2017) (Box 3.8.2).
Dedicated resources from general tax revenues finance Australia’s programme budget for “health regulation, safety and protection”. Its required outcome includes key performance indicators for:
disease surveillance and information systems;
immunizations;
public health security response;
AMR regulations;
stockpiling of medicines.
The table shows these indicators do not sit within any specific departments or health programmes; they are all at the level of the “health portfolio” or sector. Additionally, the budget for these health sector activities is directly linked with other budgetary programmes, including some from outside the health sector. This budgeting approach recognizes the complementarity across sectors that is needed to achieve particular outcomes.
Outcome 5. Regulation, Safety and Protection
Protection of the health and safety of the Australia community and preparedness to respond to national health emergencies and risks, including through immunizations, initiative, and regulation of therapeutic goods, chemicals, gene technology and blood and organ products
Program 5.2: Health Protection and Emergency Response
Program 5.3: Lmmunization
Selected Linked Programs to Outcome 5 outside of Health Sector
- Department of Agriculture and Water Resources
Program 2.1: Biosecurity and export services
- Department of Education and Training
Program 1.2: Child care benefit
- Department of the Environment and Energy
Program 1.6: Management of hazardous wastes, substances and pollutants
- Department of Human Services
Program 1.2: Services to the community
The flexibility that programme budgeting affords was on display in the COVID-19 response, with New Zealand, Mexico and South Africa all adding a COVID-19 budgetary programme to the health budget where they were then able to redirect programme envelopes for the response (Barroy et al., Reference Barroy2020b).
Other countries have worked around budget inflexibility by introducing exceptional spending measures. These measures, often introduced by executive decree, can allow for rapid budget reallocation, activation of contingency funds, emergency spending authorization, simplified approvals and rapid fund disbursement to subnational levels (WHO, 2022). Having systems and plans in place in advance of a pandemic enables a faster response. This may also include the revision of finance laws to ensure that these sorts of flexibilities are baked into legislation for certain crisis circumstances.
Effectively integrating domestic financing for pandemic preparedness into annual and multiyear budgets requires targeted efforts. Funding for cross-cutting activities (such as laboratories, training, surveillance or information systems) requires pooled resources and coordination among the health sector and other relevant sectors (Sparkes, Kutzin & Earle, Reference Sparkes, Kutzin and Earle2019). This coordination can be achieved through a health sector medium-term expenditure framework (van Eden, Gentry & Gupta, Reference van Eden, Gentry, Gupta, Lam, 570Rodlauer and Modernizing2017), public expenditure reviews (World Bank Group, 2017) or other processes that build on evidence-based, high-quality diagnostics of health challenges and policy effectiveness.
These processes provide clear priorities for spending over time, particularly in the face of both fiscal and political constraints, and involve focusing on strengthening national and subnational institutions to deliver cross-cutting activities. New Zealand, for example, has implemented a budgetary framework that enables cross-agency funding as a way to improve collaboration and reduce the transaction costs of working across agencies (The Treasury, 2015). The framework contains three possible funding models to determine both government and financing arrangements associated with delivering activities across agencies that contribute to shared outcomes: cost recovery charges, wherein one agency buys a service from another agency and recovers costs through a service fee; pooled funding, in which a group of agencies combine funds in order to share costs to achieve a common goal; and centrally determined funding, when ministers determine cross-agency collaboration is needed and then identify funding sources.
Public financial management objective 2: accountability
The expenditure flexibility required for pandemic preparedness must be matched with strong accountability mechanisms. Often opaque country financial management systems and outdated information systems make financial accountability difficult and a persistent problem (World Bank Group, 2019a). This dynamic not only lends itself to corruption and lack of transparency but also to inefficiencies and wasteful spending (Khasiani et al., Reference Khasiani2020). Budget accountability mechanisms include ex post and/or risk-based controls, regular updates to public spending systems, developing performance frameworks, using programme envelopes for expenditure tracking and ensuring that finance authorities take a lead role (Barroy et al., Reference Barroy2020a). For example, both France and China have introduced and strengthened tracking procedures that take into account clearly defined policy goals and targets.
Purchasing/payment mechanisms
Pandemic scenarios likely require funding arrangements to pay health workers for working overtime and taking on additional responsibilities, establishing diagnosis and treatment facilities, undertaking vaccine R&D and more. However, there can be financial obstacles that hinder a country’s ability to pay. Countries require systems established in advance of a crisis which allow for budget flexibilities and reallocation to pay front-line health workers under pandemic conditions (Board on Global Health et al., 2016; Mathauer, Dkhimi & Townsend, Reference Mathauer, Dkhimi and Townsend2020). Beyond reallocation mechanisms, these adaptations include lifting budget caps so that providers can actually receive the additional funds needed to respond to the pandemic. Facility accreditation changes (and established plans for flexibilities under crisis conditions) can also enable the emergency activation of certain services and providers. A survey of 31 LMICs during 2020 found that half had made this type of accreditation change in order to expand service provision related to COVID-19, particularly through private sector providers. These adaptations all have implications for information system management and governance mechanisms that similarly can be put in place in advance and facilitate coherence between the public and private sectors.
Incentivizing preparedness
Financing mechanisms for preparedness go beyond funding issues and extend to incentivizing investments into these critical activities. These mechanisms are put forward in recognition of the market and political failures until now associated with prioritizing investments in preparedness activities. These incentive approaches can include offsetting negative externalities from business activities by requiring appropriate investments from the private sector in risk mitigation, prevention and preparedness (International Working Group on Financing Preparedness, 2017). There are also calls to incorporate health security risks into macroeconomic bond ratings and investment criteria (International Working Group on Financing Preparedness, 2017; World Bank Group, 2019b). IMF Article IV consultations, which provide country surveillance to identify economic and financial risks, can also be extended to include infectious disease and health security risks. Similarly, the World Bank’s Country Policy and Institutional Assessment and Systems Country Diagnostics are opportunities to integrate preparedness into economic risk and institutional assessments (Global Preparedness Monitoring Board, 2019).
None of these national-level financing mechanisms can ensure pandemic preparedness in isolation. However, they can be critical enablers when taken in conjunction with one another, along with effective planning, political commitment and dedicated implementation capacities. They can also be complemented/supplemented by global and regional mechanisms, as we describe briefly below.
Global and regional mechanisms
Beyond the national-level mechanisms, global and regional mechanisms for pandemic preparedness financing also play important roles. After all, financing for pandemic preparedness represents a vital investment in global solidarity to avoid or mitigate catastrophic pandemic costs. As noted by the Global Preparedness Monitoring Board 2020 Report, “global preparedness is not simply the sum of national preparedness” (Global Monitoring Preparedness Board, 2020). Mechanisms for pathogen tracking, early alert systems, R&D, regulatory capacity-building and harmonization, allocation of countermeasures, stockpiles and supply chains are all necessary at the global and regional level and require dedicated funding. Regional networks and global coordination of funding and response, as well as sharing general best practices around financing preparedness, are all global prevention and preparedness activities. To establish each of these activities, a range of financing mechanisms to fund them should be considered (Global Monitoring Preparedness Board, 2020). Here, then, we consider the potential of pooled resources.
Pooled resources for pandemic preparedness
COVID-19 exposed clear limitations in pre-existing financing mechanisms that were not at a large enough scale to meet needs, and therefore new mechanisms and donor resources had to be mobilized rapidly for the response (Global Monitoring Preparedness Board, 2020). Pooling is the accumulation and management of prepaid financial resources on behalf of some or all of the population (Mathauer et al., Reference Mathauer, Dkhimi and Townsend2020). Many global mechanisms focus on pooled funding, primarily from HICs, to support the response to pandemics and other emergencies (e.g. COVAX), as well as to incentivize investments in preparedness and prevention at the country level.
At the global level, existing financing mechanisms for pandemic response include the WHO Contingency Fund for Emergencies, which since its inception in 2015 has funded operational and response activities. As the scale of the COVID-19 pandemic and response grew, additional funding mechanisms were created or repurposed, including the development of COVAX (Eccleston-Turner & Upton, Reference Eccleston-Turner and Upton2021), and specific funding windows provided by the Global Fund and the World Bank (Bump, Friberg & Harper, Reference Bump, Friberg and Harper2021). Investments are also being made to build vaccine and other production capacities in LMICs. The pre-COVID-19 pooled global funding mechanisms often targeted specific functions, including vaccine and supply stockpiles, insurance systems, cross-border contagions or global coordination functions, including within WHO.Footnote 3 For example, the World Bank’s Pandemic Emergency Finance Facility is an insurance system established in the wake of the Ebola crisis in 2014 to enable the rapid mobilization and deployment of funds (Box 3.8.3).
Response to the Ebola crisis in 2014 was hampered by the inability to rapidly mobilize and deploy funds. To address this issue, the World Bank established its PEF insurance system which has been in operation since July 2017. It provides coverage for countries already deemed eligible for financial assistance from the International Development Association against the risk of pandemic outbreaks. The coverage consists of a combination of insurance bonds and derivatives and a donor-funded cash window for accessing loans. Importantly, the PEF does not provide funds for preparedness, and rather it is meant just for response needs. The facility has sought to create a market for pandemic risk insurance that draws on funds from the private sector through (catastrophe) bonds and swaps (a temporary agreement between two parties to exchange cash flows or liabilities from other financial instruments, often used to reduce financial risk) in return for highly lucrative interest rates. However, due to the relatively high threshold for countries to be able to access PEF funds, there are concerns about its functionality and utility (Brim & Wenham, Reference Brim and Wenham2019).
In learning from the COVID-19 experience, there was a clear need for more coordinated action to strengthen health system foundations, as well as to rapidly mobilize needed resources for pandemic preparedness at a global level. In light of this, The Pandemic FundFootnote 4 was established in 2022 with the objective to provide additional, long-term financing and technical support to LMICs in the areas of health systems strengthening and pandemic preparedness (The Pandemic Fund, 2024). By the time of the first round of grant allocation, The Fund had already raised US$ 2 billion in seed capital from governments, philanthropies and the private sector (The Pandemic Fund, 2023). The first round of funding awarded 37 country recipients with funds to strengthen disease surveillance and early warning systems, laboratory systems and human resources. Many of these country projects involve efforts that will have wider benefits to neighbouring countries through the One Health approach by building up cross-border and regional collaboration. There is a need to ensure, however, that the implementation arrangements and application of these projects and activities do not create new, parallel efforts or systems and are rather aligned with country systems.
As mentioned, global activities have transnational benefits that may extend regionally or globally. For this reason, both revenue mobilization and pooling mechanisms may also sit at regional levels. One such an initiative is Regional Disease Surveillance Systems Enhancement (REDISSE). Like the PEF, REDISSE was set up in the wake of the 2014 Ebola epidemic and is funded by the World Bank. Both a surveillance and response programme, it takes a regional approach across 11 countries in west Africa to strengthen routine systems to prevent and detect health threats, taking advantage of regional economies of scale (World Bank Group, 2019a).
Before setting out our conclusions, we present a case study of Viet Nam, as an example of a lower middle-income country that undertook a review of its health security financing in the light of recent experience of epidemics and pandemic.
Evidence in practice: financing pandemic preparedness in Viet Nam
Since 2000, Viet Nam has encountered several notable epidemics, such as avian influenza (H5N1) in 2003, influenza H5N6 and the pandemic of H1N1 in 2009. Given the history and the ever present threat of outbreaks and public health emergencies, Viet Nam conducted a HSFA (Osornprasop et al., Reference Osornprasop2020) using a tool developed by the World Bank to better understand the country’s practices around health security financing based on data from the fiscal year 2016.Footnote 5 Health security expenditures and activities were identified using the Joint External Evaluation structure.
From the analysis, the total health security expenditure, which included central and provincial levels, was estimated to be US$ 181.2 million (0.09% of gross domestic product, and 0.29% of the total government expenditure), almost 75% of which was spent at the provincial level.Footnote 6
The government funded the largest share of health security activities in the country (77%), followed by external aid (12%), which was spent primarily at the central level. In order to transfer government funds to the implementing agencies, they used annual budget allocations for recurrent, investment and national target programmes, where recurrent budget allocations accounted for 66% of total health security expenditure. Additionally, their systems allowed for contingency funds and budget, financial and national reserves to be triggered at a time of public health emergency.
Differences in health expenditure at the provincial level were found, where provinces on the country border as well as those provinces that were empowered to mobilize their own revenues, where sufficient, to cover health security spent a higher amount on health security activities. At both the central and provincial level combined, spending on preparedness activities was the highest proportion of expenditure (16%), followed by food safety, zoonotic diseases and workforce development (all between 12% and 15%).
During the 2003–2006 avian influenza outbreak, most domestic funds came from a contingency fund within the recurrent budget allocated to ministries and localities. This was already in place: once the necessary authorities declared an epidemic of public health concern, a contingency fund could be activated for the use of prevention and response activities. The central level fund was allocated to provinces to cover 50% of expenses relating to prevention and response of the epidemic, such as culling of infected poultry, while the remaining 50% was covered by the local level contingency fund. Supplementary budgets were also approved through the Prime Minister, which came from the contingency fund from the central budget, budget surplus revenues and loans from the credit balance.
The analysis identified significant challenges in the planning and financing of epidemic and pandemic preparedness. Viet Nam is working to improve and enforce close cooperation and effective coordination across sectors and levels of government for the accountability and funding of these interdisciplinary activities. However, at the time of the study, there was clear duplication in mandates and mechanisms for information sharing across agencies. Without clear coordination, activities such as disease surveillance lack integration, especially across geographical areas. Additionally, important sectors such as agriculture and tourism were rarely accounted for in planning and coordination activities. These deficiencies highlight the importance of establishing and implementing governance arrangements to enable the coordination and collaboration required across different levels of government and between sectors.
Another challenge lies with the planning efficiency and budgeting processes in the country. Recurrent and nonrecurrent funding for pandemic preparedness is based on the previous year’s amount rather than projected need. Reserve budget is allocated on a per capita basis, and additional amounts are specified by an input-based budget structure, which does not account for the cross-sectoral nature of the activities. Proposed budgets are often higher than the approved funding, which is dependent on the amount of external aid and local budget capacity. This often results in lower funding allocations in poorer areas, thus exacerbating existing inequalities.
The report provided a call to action to improve and efficiently plan and allocate necessary funding for preparedness activities. The actions identified included improved information sharing, shared planning across sectors, integrated disease surveillance, increased understanding of actual workload and a budget for these activities across the central level of government.
Policy relevance and conclusions
Evidence-based principles for establishing pandemic preparedness imply actions that strengthen existing systems, ensure business continuity plans with continuous learning to refine systems and strategies and are supported by adequate and appropriate financing mechanisms. This involves a continuous process of planning, exercising, revising and translating into action national and subnational pandemic preparedness and response plans (WHO Regional Office for Europe, n.d. b).
Establishing pandemic preparedness capacities requires targeted financing mechanisms to ensure funding commitments are translated into activities and interventions. Despite the recognized importance of pandemic preparedness, investments have often been limited or lacking due in part to the uncertain nature of preparedness and risk. As exemplified by the Viet Nam case study, the countries that have taken action to dedicate resources and establish financing mechanisms tend to be those spurred into action by their own particular experience of a health crisis. In the context of COVID-19, however, all countries have now experienced such a crisis. Financing pandemic preparedness must be a core government and global function.
The lessons from countries that have worked both to establish preparedness capacity and to respond to crisis show that effective financing goes beyond resource commitments and considers public financial management mechanisms and incentive structures. These financing mechanisms go beyond health budget allocations and consider transfer mechanisms to ensure coordination across multiple sectors (including the health sector) and multiple levels of government. Good governance and stewardship of preparedness, national and multisectoral coordination, political will and previous experience with pandemics have been found to be predictors of better mobilization and allocation of funds for prevention and preparedness (Hanvoravongchai et al., Reference Hanvoravongchai2010).
Financing mechanisms that support preparedness activities require budgetary space and institutional capacities that include funding for both the capital and recurrent expenditures required. These are measurable, annualized costs that require dedicated financing streams. Financing for activities that support preparedness requires proactive planning, systems and mechanisms that can be quickly and flexibly activated. Due to the inherent uncertainty of these events, the prepositioning of financing mechanisms that can be deployed quickly and with strong accountability systems is critical for an effective and timely response. Prepositioning goes beyond setting funds aside, and rather considers contingency funding mechanisms that can be quickly mobilized.
Importantly, financing pandemic preparedness should not be viewed in isolation, separate from the overall health system or other public financing priorities. For the purposes of this chapter, we have focused on distinct characteristics of pandemic preparedness. However, in practice these financing mechanisms need to be well-coordinated and integrated within overall public investments that promote and protect health and well-being and those that protect against emergencies more broadly. Furthermore, these investments can either leverage existing systems, or can have beneficial spillover effects on non-disease control measures, for example through improved information systems for health care or additional hospital capacity. Therefore, the societal gains from investments and sustainable financing of pandemic preparedness are not limited to the cost savings related to averting or being prepared for a pandemic, but also in relation to strengthening the foundations of the system for other health needs.Footnote 7


 Open access
Open access