

Key messages
Chapter 3.5 reflects on how to use payment mechanisms to support the integration of care. Integrated care is about better management of the care patients receive in different settings (primary, secondary) and from different specialists and teams. It is particularly important for patients with multimorbidity and chronic long-term needs, and as populations age. Key learning includes that:
Health systems’ payment models can play an important role in incentivizing integrated care.
Purchasers are now testing innovative payment models (e.g. pay for coordination (P4C)) which explore how to foster better coordination. These models include:
○ bundling payments to single providers so that the multiple services a patient uses are better linked; and
○ bundling payments for patients being treated by multiple providers, creating joint budget responsibility and a need to work together and avoid duplication.
Policy-makers would do well to focus on careful design of information systems to underpin payment schemes because:
○ information sharing supports clinical effectiveness;
○ quality indicators allow purchasers to tie bonuses or penalties to integration and guard against inappropriate cost-cutting;
○ monitoring activity and health outcomes helps assess value for money;
○ tracking the distributional consequences of incentive schemes is crucial in protecting equity;
○ robust evaluation alongside payment reform allow immediate lessons to be shared and will capture changes over time and across the health care system.
Health systems need to embed financial incentives as part of a broader system approach. Critical elements include:
○ committed leadership;
○ effective communication among providers;
○ structural integration, either through coordinating mechanisms that link provider roles or by the formation of new entities with single management teams.
Introduction
In this introduction, we set out the need for integrated care, and the role that payment models might play in delivering it. Across high-income countries (HICs), the increased burden of chronic disease associated with rising life expectancy has led to a call for health systems to extend their focus beyond the treatment of acute illnesses to the provision of long-term care (LTC) for patients who may require inputs from primary, secondary and social/community care providers (OECD, 2016; WHO, 2015). The growing prevalence of individuals with multiple chronic diseases (multimorbidity) increasingly requires models of care delivery that focus on the multiple care needs of the patient rather than separate treatment of single diseases. Indeed, without action, the increasing burden of multimorbidity poses a fundamental challenge to the sustainability of health systems worldwide (Bloom et al., Reference Bloom2012; European Commission, 2011; Nolte & Pitchforth, Reference Nolte and Pitchforth2014).
There is a broad consensus that this rising need for care inputs from multiple providers and the fundamental concerns for the long-term sustainability of health systems require the provision of care that is better coordinated and less fragmented – commonly referred to as integrated care.
Definition of integrated care
Using Struckmann and colleagues’ (Reference Struckmann2018) definition, integrated care can be understood as:
structured efforts to provide coordinated, proactive, person-centred, multidisciplinary care by two or more communicating and collaborating care providers. Providers may work at the same organization or different organizations, either within the health care sector or across the health care, social care, or community care sectors (including informal care).
This definition encompasses both a system and a patient perspective, where integrated services are those that are experienced by the patient as coordinated (Goodwin, Reference Goodwin2016).
The goal of care integration can be achieved through multiple means – of which payments, the focus of this chapter, are one. According to Poku, Kagan and Yehia (Reference Poku, Kagan and Yehia2019), there is an inverse relationship between care that is truly integrated and the need for care coordination: the more integrated care services are, the less need there is for coordination. The delivery of integrated care may, but need not, involve the formation of new vertically integrated organizations and it is important to note that organizational integration does not automatically solve the need for internal coordination (Williamson, Reference Williamson2002).
The role of payment models
In the same way that health systems may require reform to meet the changing needs of the population, there is a need for new payment methods that better align with current policy goals (Leijten et al., Reference Leijten2018; Struckmann et al., Reference Struckmann2017). This chapter discusses payment models that can support the delivery of integrated care by non-integrated organizations, as well as models intended to incentivize the delivery of integrated care by vertically integrated organizations. The current ways of paying for primary and secondary care (Box 3.5.1) do not fit well with the provision of integrated care. For example, fee-for-service (FFS) and prospective payments based on diagnosis-related groups (DRGs) are based on activity, and primarily incentivize a high throughput of discrete units of care, rather than a long-term, well-coordinated, holistic care effort that ensures quality and cost–effectiveness for the chronically ill and multimorbid across the spectrum of care (Busse & Mays, Reference Busse, Mays, Nolte and McKee2008).
There are three main payment mechanisms for physicians (i.e. general practitioners (GPs), ambulatory specialists):
1. FFS: each individual service (unit of care) provided is reimbursed.
2. Capitation payment: providers receive a fixed amount for providing services to a patient (e.g. per registered patient on a practice list) for a specified period of time, regardless of the volume of services consumed by individual patients.
3. Salary: a payment per time period that depends on the characteristics of the physician, e.g. their years of experience or position in the hierarchy. Salaries are administratively simple but provide limited incentives for productivity (Rechel, Maresso & van Ginneken, Reference Rechel, Maresso and van Ginneken2019).
There are also three main payment mechanisms in hospitals:
1. Global budgets: a type of broad capitation in which a provider, typically a hospital, is paid a fixed amount, based on hospital characteristics or expected activity.
2. DRG case payment systems: hospitals are paid a fixed amount of money per inpatient stay depending on the characteristics of the patient and the treatment provided.
3. Per diem fees: payments per day of an inpatient’s stay (Bell, Charlesworth & Lewis, Reference Bell, Charlesworth and Lewis2021; Rechel, Maresso & van Ginneken, Reference Rechel, Maresso and van Ginneken2019).
The payment mechanisms may be used in combination.
The redesign of payment models to enable more efficient care for patients with one or more chronic diseases requires providers to recognize the interdependency of care delivered across multiple sectors. Although this goal cannot be met by changes to the payment system alone, it is clear that most existing payment models are designed with a single sector in mind, and do not encourage providers to better coordinate their care or consider the implications of care in one sector on the expected cost and benefits of care in other sectors (Mason et al., Reference Mason2015). Although more than 100 integrated care programmes for people with multimorbidity have been implemented in Europe, these challenges are rarely addressed by new innovative payment methods (Struckmann et al., Reference Struckmann2017). However, such methods do exist and are worthy of consideration, as we shall show in what follows.
We begin by outlining a set of criteria by which we can benchmark payment models with respect to their ability to meet the policy goal of greater care integration across sectors; we provide a comparative example to illustrate the need for system change. We then use the criteria to examine traditional provider payment models and their failure to meet the health system challenges of today. Next, we consider the options available for policy-makers looking for new payment models that can encourage integrated care, and the models’ potential to incentivize integrated care, in theory and in practice, including three case studies, from Germany, the Netherlands and the USA, respectively. Finally, we draw policy lessons from the foregoing and highlight where the evidence base still needs further strengthening.
Setting performance objectives for incentives for integrated care
We begin by defining the challenges a payment model needs to address with respect to integration, and the criteria by which its performance should be measured. When providing integrated care, to achieve system-level efficiency from the perspective of a third-party payer, the interconnectivity of care and needs across sectors is a priority. Likewise, the definition of quality has evolved from a narrow focus on clinical processes and outcomes to incorporate patient-reported outcomes and health-related quality of life. At the same time, the increasing prevalence of an ageing and multimorbid patient population means that the care inputs needed from across the system have changed, and therefore the requirements for payment models also need reformulating.
The so-called triple aim of improving patients’ experience of care, improving population health and reducing per capita costs of care (Berwick, Nolan & Whittington, Reference Berwick, Nolan and Whittington2008) is often proposed as the target for efforts to integrate care. The implications from the perspective of payment model design are that provider payment methods should create incentives for health care providers to internalize the impact their care decisions have on (i) patients’ future care needs; and (ii) the expected costs and benefits incurred and delivered by other health care providers. The key requirements for payment mechanisms that are specific to integrated care are therefore:
internalization of the impact of current care on future care needs/costs in the same sector;
internalization of the impact of current care on current and future care needs/costs in other sectors;
delivering care in the most efficient setting and without duplication.
Payment models that meet these requirements will help achieve the stated triple aim of higher levels of patient satisfaction, better population health and lower per capita costs. In what follows, we use these three requirements as a measuring rod for both traditional payment methods and the emerging alternative payment models.
First, though, we underline the need for change with a comparative example. If a patient develops acute appendicitis, the key objectives from a health system perspective are that the patient is treated quickly, cost-effectively and receives good quality care with a minimum of complications and a minimum need for post-treatment care. There is no uncertainty about where the patient is best treated, whether the patient will need care from multiple sectors, or what the impact on future care needs may be. The traditional health system goals of appropriate activity, quality and efficiency are therefore adequate to set requirements for and evaluate the effectiveness of the payment model. Likewise, traditional activity-based payment methods, possibly with an adjustment to incentivize quality in the delivery, are adequate to support these goals.
In comparison, for a patient with one or more chronic diseases, such as diabetes or chronic obstructive pulmonary disease (COPD), the picture is less clear. There is likely expertise available in both primary and secondary care that could treat the patient, and depending on the severity of the condition, there might also be a need for inputs from social care. Considered in isolation, these care needs could potentially be supported by traditional payment methods. However, the chronic nature of the condition means that care for the patient will be needed throughout the patient’s remaining lifetime. Therefore, there is a need to incentivize the performance of each care activity with the impact on future care needs (and costs) in mind.
In addition, it is necessary for each sector to recognize that the care delivered in one sector affects the need for care in others. The typical example is “avoidable” emergency admissions. With the appropriate levels of ambulatory and social care, it is believed that acute emergency admissions can be avoided. Clarity about how emergency hospital visits might be avoided is critical, however, whether clinically unnecessary, clinically divertible or clinically preventable (Parkinson et al., Reference Parkinson2021). Nonetheless, the potential for improvements in primary care quality and scope to reduce emergency hospital visits should not be overestimated (Parkinson et al., Reference Parkinson2020).
Why traditional payment methods fail to support integration
Traditional payment methods such as cost-reimbursement, global budgets, capitation, FFS or activity-based payment based on DRGs do not encourage providers to take care interdependency into account (see Box 3.5.1).
FFS and DRG payments
FFS payments are mostly used in primary or ambulatory care and involve paying for each service unit provided. The fee level usually relates to the type and complexity of the provided service. This generally gives providers the financial incentive to provide as many reimbursable services as possible (Busse & Mays, Reference Busse, Mays, Nolte and McKee2008; Gosden et al., Reference Gosden2000). Therefore, FFS systems may stimulate inappropriate or unnecessary use of services and offer little or no incentive for (macro level) expenditure control (Ellis & Miller, Reference Ellis, Miller and Heggenhougen2008). Particularly for patients living with multiple chronic conditions, this may result in having to make more doctor visits with a greater number of doctors, which could also have repercussions on the quality of the care they receive (Rijken et al., 2017).
DRG-based case payments are frequently used in hospitals. If based on average costs, they provide strong incentives for efficiency (Shleifer, Reference Shleifer1985), but bring the same challenges as FFS payments and equally come with the risk of disregarding patient needs and appropriateness of care (Busse et al., Reference Busse2011).
With regard to care integration, neither FFS nor DRG-based payments offer providers incentives to coordinate care or consider in which setting care will be provided with greater efficiency as this could lower the number of reimbursable services/episodes (Struckmann et al., Reference Struckmann2017).
Global budgets and capitation payments
Global budgets and capitation payments involve paying providers a fixed amount to provide services to patients for a particular time, regardless of the volume of services provided to individual patients. Both payment methods are administratively simple and control macro level expenditure well but they create few financial incentives for providing care proactively and therefore do not incentivize figuring in the expected impact of care on future care needs. Providers may respond by providing as little care as possible to each patient (care-skimping) as the providers bear the financial risk. This in turn may create the potential for undersupply of services, lower quality of service provided, increased referrals and the adverse selection of low-risk patients (Busse & Mays, Reference Busse, Mays, Nolte and McKee2008; Ellis & Miller, Reference Ellis, Miller and Heggenhougen2008; Nolte & Knai, Reference Nolte and Knai2015). The latter particularly threatens access to appropriate care for people with multiple chronic diseases.
Traditional payment models’ inadequacy: summary
In practice, most countries have implemented combinations of these payment methods (blended payments) based on different types of information (about the service, the provider or the patient) in order to mitigate the adverse incentives of the methods individually and create a more balanced set of incentives.
Generally, these payment mechanisms do not sustain a LTC effort, are focused on a single specialty or sector, and do not recognize the interdependency of care delivered across the care spectrum. This particularly affects the appropriateness and quality of care for patients with multiple chronic diseases. In terms of factoring in the impact of care on future needs and therefore costs, only capitation and global budgets give some incentive for reducing future care needs, but only in the same sector and within the current budget period. Providers paid by FFS and DRG could even be seen to benefit financially from maintaining or increasing patients’ future care needs, although altruistic provider motives would be expected to limit the extent of perverse responses to these incentives.
In addition to incentivizing the goals for integrating care, payment models should also support, or at least not work against, other policy goals such as access to care, equality and transparency/accountability, and avoidance of unintended consequences. One of the important benefits of basing payments on provider activity has been that it gives purchasers and regulators access to clear information about activity in the health sectors. If new payment models move away from being activity based, it is important to ensure that information of similar richness and accuracy can still be obtained – a point to bear in mind, when considering new, alternative models.
Paying for integrated care: what are the alternative models?
As the focus on integrated care has increased, a range of new payment methods to support care integration are being considered. Below we present the options available to health systems wishing to deliver better integrated care. These range from simple add-on payments to support coordination and integration for individual providers of primary, secondary or social care that are not organizationally integrated, to models that require financial integration, whether via a new integrated care organization formed vertically or horizontally by care providers, or by individual care providers assuming joint financial responsibility.
Struckmann et al. (Reference Struckmann2017) provided a summary of various options for the adjustment of traditional payment models, illustrating that existing payment mechanisms can be adjusted to promote coordination and ultimately integration of care. That summary formed the starting point for the framework we present in Table 3.5.1 and the alternative payment models we set out below. We look briefly at P4C then in more detail at bundled payment schemes and the different means of financial integration when payments are bundled, in particular the shared-savings model. We also examine how the payment mechanisms can be adjusted to ensure quality of care.

DRG: diagnosis-related group; FFS: fee for service; P4 C: pay for coordination.
Table 3.5.1 Long description
The table has 4 columns: Basis of payment, Provider, Patient or population, and Service. It reads as follows. Traditional payment method: Provider: Global budgets or salary. Patient or population: Capitation. Service: F F S or D R Gs.
Next comes Incentivizing coordination through to incentivizing integration. First, near incentivizing coordination comes P 4 C. Provider: Budgets for multidisciplinary teams (for example, case manager). Patient or population: Higher capitations for providers with multidisciplinary teams. Service: P 4 C activities (for example, case review, documentation, participation in meetings).
Next is Bundled payments to one provider. Patient or population: Bundled payment per patient in target population for multiple providers. Service: Bundled payment for multiple services performed by one provider.
Next is Financial integration. Provider: Pooled budgets or shared savings for (joint budget responsibility between multiple providers). Patient or population: Bundled payment per patient in target population for multiple providers. Service: Bundled payment for multiple services performed by multiple providers. Next, near Incentivizing integration comes Organizational integration (horizontal or vertical mergers) and New organizational forms, for example accountable care organization.
Finally, Supplementary incentives: Providers: Bonus or penalty in relation to meeting structural quality indicators. Patient or population: Bonus or penalty in relation to risk-adjusted mortality, readmissions, complications or patient satisfaction. Service: Bonus or penalty for proportion of patients treated in line with guidelines. Finally, Monitoring structural, process or outcome quality.
P4C
At the most basic level, existing payment methods can be adjusted to promote better coordination of care with a payment type known as P4C (Tsiachristas et al., Reference Tsiachristas2013). The adjustment can be made by: (i) adjusting the care provider’s budget to cover; for example, the cost of employing a case manager tasked with ensuring coordinated care; (ii) increasing capitation payments for each registered patient with a provider that employs case managers or multidisciplinary teams; or (iii) providing additional fees for coordination activities such as case review and participation in meetings. Combinations of the three are also possible.
Bundled payments
Bundled payments is the term used for payments covering more than one episode of care for the same patient. As shown by Stokes and colleagues (Reference Stokes2018), what is included in the care bundle can vary greatly, from payments covering all episodes of care for a given condition from a single provider to payments covering all care for a patient from multiple providers.
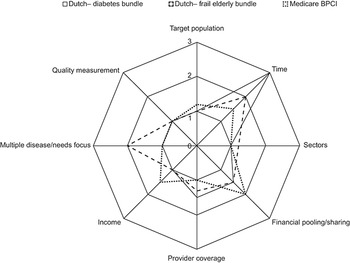
The effect of a bundled payment on care integration depends on the exact scope of the payment in terms of the target population, time perspective, how many sectors are included, how many providers are covered, the number of diseases/activities covered for the population, supporting levers in the form of quality measurement, the proportion of income affected and whether there is additional financial integration or risk sharing in place (Stokes et al., Reference Stokes2018). Fig. 3.5.1 gives an example of how three existing bundled payment systems vary on these dimensions, two from the Netherlands (for diabetes and elderly care, respectively) and one from the USA (Medicare BCPI).
Three bundled payment schemes and how they vary on key dimensions

In general, the broader the scope of the payment, the greater the incentive for integration of care but also the greater the financial risk transferred to the provider (Struckmann et al., Reference Struckmann2017). Therefore, the introduction of a bundled payment model must always consider the existing provision structure and the availability of suitable contractors to accept the financial risks involved with the introduction of bundled payments.
When the payment bundle covers more than one provider, the contractual arrangement required increases in complexity as the mechanism necessitates financial integration between the two or more providers who become jointly responsible for the care of a patient. Such arrangements are much harder to implement than P4C because they require changes that go beyond simply modifying the payment system and imply a transfer of financial risk from the payer(s) to the provider(s). The multiple providers may be from within the same sector (e.g. primary care) or across sectors (e.g. primary and secondary care providers). They may choose to form a new integrated care provision organization, often referred to as an accountable care organization (ACO). But even without forming a new organization, multiple providers can assume joint financial responsibility.
A review by Mason and colleagues (Reference Mason2015) identified eight types of financial integration, including: (i) transfer payments and cross-charging, where one provider either makes contributions to or pays fees to compensate the other entity; (ii) pooled funds, where multiple providers contribute to a common fund that can be spent on shared patients; and (iii) structural integration, where a new entity is formed with a single management team.
The difference to the add-on payment methods previously discussed is that financial integration offers a greater incentive to providers to recognize their joint impact on patient outcomes, by creating a financial interdependency between providers across sectors and assuming a mutual financial risk.
Theoretically, the broadest bundled payment would cover all care provided to all patients living in an area over a defined period of time. However, this type of payment would be usually called a broad capitation payment or a population-based budget. This implies that the question of how to pay providers and how to assure coordination of care is simply transferred from the purchaser to another organization, which then becomes the payer for individual providers (Struckmann et al., Reference Struckmann2017). In this situation, purchasers arguably have less capacity to act as strategic purchasers and influence service provision without supporting collection of information about activity and quality, and care provision under such a payment bundle becomes opaque for the payer and the public.
Shared-savings model
One of the most common models of financial integration designed to promote integrated care is shared-savings. In this model, participating providers agree to cooperate in a network and to collaborate with the aim of achieving joint savings for the care provided to participating patients. If such savings are made, a share is distributed to providers. Of course, the providers, patients and services eligible for participation in the programme have to be explicitly defined before the start of the programme (Hayen et al., Reference Hayen2015). Within the model, each individual provider continues to be paid according to the established payment system, but all costs for patients participating in the integrated care programme are registered and retrospectively compared to previous figures or a benchmark set to ensure that random fluctuations are not rewarded or punished. The payer is thus able to determine if any savings have been made, a share of which can then be shared among the collaborating providers.
Usually, shared-savings models require a new organizational structure to coordinate the roles of the participating providers, (re)distribute savings between them, help with the coordination of care, and facilitate the development of joint clinical pathways or joint electronic medical records. The (re)distribution mechanism is very important as it may well determine the success of the programme and the extent to which all providers gain from the reorganization of care (Struckmann et al., Reference Struckmann2017). Payers will likely want to specify reporting requirements about activity and quality to ensure transparency.
Ensuring quality of care
Finally, payment systems can be adjusted to incorporate incentives for quality. This is often called pay for performance (P4P) or pay for quality (P4Q) and can be based on structures, processes and/or outcomes (Donabedian, Reference Donabedian1988; McManus et al., Reference McManus2021). P4P can be used to achieve agreed quality targets, for which payment to providers (professionals or institutions) is modified upwards or downwards. Within a provider network, target achievements can be recorded electronically and compared among participating providers, for example, with respect to patient experience (Struckmann et al., Reference Struckmann2017).
Measuring and incentivizing quality of care is particularly important when payments allow providers to interpret patients’ care needs broadly, as is the case with shared-savings models, bundled payments and capitation payments made to integrated care structures. This is because broader payments provide larger incentives and room for providers to reduce costs – and, in the absence of adequate mechanisms to monitor and reward quality, providers may attempt to cut costs by reducing the provision of services, disregarding patient needs and providing lower quality care.
Table 3.5.1 also provides examples of these monitoring and rewarding mechanisms. For example, providers could be given penalties or bonuses for having appropriate structures in place for the care of people with chronic diseases (e.g. employing personnel with special training in multimorbidity, case managers) calculated as a percentage of their usual income. Furthermore, bonuses could be given for achieved outcomes of care (e.g. lower than average rates of mortality or hospital admissions, high patient satisfaction). Lastly, providers could receive a bonus if care is delivered in line with recommended treatment pathways and guidelines (e.g. if they perform a biannual polypharmacy review) (Struckmann et al., Reference Struckmann2017).
Designing appropriate P4P programmes is a complicated task because of the many issues surrounding the measurement of quality (e.g. which indicators to use and how), the definition of targets (e.g. absolute targets or relative targets), the level of the payment adjustment (e.g. individuals, groups, institutions), the form of the incentive (bonus or penalty), the use of risk adjustment and so on (Eijkenaar, Reference Eijkenaar2013).
How the new payment models incentivize integrated care: in theory
P4C is the least likely to incentivize providers to figure in the temporal and cross-sectoral consequences of their care, and thus lead to cost-effective care across the pathway. This is because the coordination payment is simply an add-on payment intended to incentivize providers to engage in a coordinating process, but other than signalling the need to coordinate to the provider, it does not give the provider a financial incentive to do so. Moreover, coordination effort is difficult to make contractible because the details of what is needed will vary greatly from patient to patient. It is also difficult to monitor compliance (Kristensen, Bech & Lauridsen, Reference Kristensen, Bech and Lauridsen2016), and there is no incentive for providing cost-effective care across the pathway.
Bundled payments are in principle able to incentivize the figuring in of the impact of current care on future needs in the same sector and the impact of care needs in other sectors, but it is difficult to imagine a cross-sector blended payment without a joint organization or a collaboration between providers from different sectors. To deliver care in the most efficient setting would likely require some form of financial integration.
For example, cross-charging could be used to incentivize the figuring in of care in one sector on care need in other sectors. However, as financial integration moves towards organizational integration, there is a risk of recreating the coordination problems facing payers/purchasers. Joining up entities from across sectors does not guarantee that the coordination problem goes away (Williamson, Reference Williamson2002). In fact, by removing the explicit transaction from the equation, new internal coordination problems may arise (Struckmann et al., Reference Struckmann2017) and benefits from specialization may be lost (Baicker & Chandra, Reference Baicker and Chandra2004, cited in Mason et al., Reference Mason2015) and the payer has effectively transferred the question of how to ensure coordination of care to the providers. In addition, larger budgets across more complex organizations are less transparent and may be more difficult to monitor and control.
Thus, from a theoretical perspective, financial integration without organizational integration (for example, in the form of shared-savings) may be thought to have the greatest likelihood of achieving the goals of integrated care but require careful incentive design which in itself is a complex task.
How the new payment models incentivize integrated care: in practice
Overall, the empirical literature on payments for care integration does not provide very strong evidence that introducing financial incentives alone will incentivize integrated care. On a side note, the same can be said about integrated care interventions in general (Kumpunen et al., Reference Kumpunen2020). This raises a general point about the literature on the effectiveness of payments for care integration – that it is rare to have evidence on interventions that changed the payment system only. Most often, the changes to provider payments are part of a larger system change to stimulate care integration. It can therefore be difficult to separate out the impact of the changes to payment mechanisms from other changes to the organization of care occurring at the same time.
Because the specific payment mechanisms to support integrated care differ widely, the challenge for the literature in terms of condensing the empirical evidence is similar to that facing the literature on P4P (which is another example of an intervention that is not as uniform as the name would suggest). One study that does try to generate generalizable knowledge is Tsiachristas et al. (Reference Tsiachristas2015). The authors used longitudinal variation across 25 countries from 1996 to 2013 to examine the impact of national payment schemes to support integration classified as either P4P, P4C or bundled payments. Nine countries introduced at least one of the three payment schemes to incentivize care integration. The authors examined the impact on total health care expenditure, and outpatient care, hospital care, medication and administration expenses individually. They found that introducing P4C and bundled payments was associated with reductions in outpatient care expenditure, while P4P was associated with reductions in hospital and administration expenditure.
Hayes and colleagues (Reference Hayes, Stokes, Kristensen and Sutton2021) used a similar approach to examine the impact on health and health care utilization, analysing patient-reported data from 20 countries from 2011 to 2015; eight countries introduced payments for integration, with a particular focus on the impact of payment reform on patients with multiple chronic conditions. The health outcomes examined were self-assessed health, limitations to day-to-day living and quality of life. To measure health care utilization, the authors focused on the total number of times respondents had seen or talked to a medical doctor in the past 12 months, the total number of GP contacts (a subset of the previous variable) and the proportion of GP contacts in relation to overall doctor contacts. The authors found that in countries that introduced P4C, multimorbid patients had proportionately more contacts with a GP, suggesting a shift to the primary care level where this payment method was introduced. In countries that introduced bundled payments, there was a relative increase in the number of times multimorbid patients were in contact with a doctor in comparison to patients who were not multimorbid. For both payment schemes, there was no measurable differential impact on health outcomes for multimorbid patients associated with the change. In countries that introduced P4P, multimorbid patients experienced a relative decrease in quality of life and greater limitations to their day-to-day living than other patients, while no measurable changes were detected in their pattern of care seeking.
When interpreting the findings from the studies by Tsiachristas et al. (Reference Tsiachristas2015) and Hayes et al. (Reference Hayes, Stokes, Kristensen and Sutton2020), it should be kept in mind that they both group specific national payment schemes under broader headings, at the cost of reducing potentially important institutional differences across countries. On the other hand, this is a common issue in empirical work and, if nothing else, the results can point interested policy-makers and practitioners in the direction of payment changes that were effective in their respective settings, and dive into detail that might need translation to their own context.
A review of integration of funds for health and social care (Mason et al., Reference Mason2015) looked at 38 examples of financial integration from eight countries. Out of 34 studies that evaluated the impact of financial integration on health care costs and utilization, only three found a reduction in the cost or use of care, while the remaining 31 either found no, mixed or negative results (greater care use or costs after financial integration). Twenty-four studies examined the impact on patients’ health and, here, just five found an improvement, and half of the studies found no effect at all. The authors found that the primary barrier for integration was practical challenges in communicating and exchanging information across sectors. One lesson from this review is therefore that it often takes more than financial integration to integrate care.
Case study 1: Bundled payment scheme for chronic diseases, Netherlands
A pilot of this bundled payment scheme with a focus on diabetes care began in 2007 and the scheme was fully operational from 2010. The scheme is voluntary, and allows health care providers to form care groups consisting of multiple providers that take joint clinical and financial responsibility for the patients covered by the scheme; for example, patients with diabetes, COPD or vascular disease. Participating care groups receive a fixed payment to cover disease-specific care, while other care is still reimbursed separately. The amount is set through negotiation between the payer and the care group. The group participants can then either provide care for patients themselves or subcontract to other providers (Llano, Reference Llano2013). The aim of the scheme is to improve the quality of care, and the contracts specify the care process and outcome quality standards of care that providers must adhere to under the scheme.
An evaluation by the Dutch National Institute for Public Health and the Environment (Struijs et al., Reference Struijs2012) found modest improvements in most process indicators of quality, including foot examinations, kidney function testing and cholesterol testing, while numbers of eye examination declined. Nevertheless, the variation in the quality of care between care groups was considerable. It should be noted, however, that the analysis did not use a control group, and it is therefore possible that the improvements in process quality would have occurred in the absence of the payment change regardless. We have not been able to locate stronger or more recent empirical evidence on the impact of the Dutch bundled payments on the quality of care.
Early empirical evidence suggested that expenditure increased in the short run for patients covered by the scheme (Mohnen, Baan & Struijs, Reference Mohnen, Baan and Struijs2015) and a recent study (Karimi et al., Reference Karimi, Tsiachristas, Looman, Stokes, Galen and Mölken M2021) confirmed that this was also the result in the long run. According to a recent evidence scan (Struijs et al., Reference Struijs2020) the Dutch bundled payment scheme seems to be an outlier in this respect. Summarizing evidence on 11 bundled payment models, the authors found modest savings or modest reductions in spending growth reported in 20 of 32 studies; 18 of the studies reported quality improvements.
Case study 2: Medicare Shared Savings Program, USA
The Medicare Shared Savings Program is a voluntary scheme that enables health care providers (e.g. hospitals and/or primary care physicians (PCPs)) to form ACOs which take population responsibility for the quality, costs and care of their patient population (CMS, 2021). Launched in 2012, the scheme offers participating ACOs a menu of risk-sharing contracts between Medicare and the ACO. ACOs taking on larger financial risk may also receive greater shares of the savings. A one-sided option is the most popular, where only savings – not losses – are shared; this option was taken up by 99% of the participating ACOs in 2015 (McWilliams et al., Reference McWilliams2018). The participating providers are paid by FFS. A prerequisite for accessing the shared savings is that the quality of care meets agreed performance standards. In addition, only savings above a certain level, known as the minimum savings rate, qualify for sharing. As pointed out by Pope and Kautter (Reference Pope and Kautter2012), the minimum savings requirement can be seen as an attempt by Medicare to distinguish random variation in expenditure from expenditure reductions due to the ACO’s “true” cost-control effort.
An evaluation by McWilliams and colleagues (Reference McWilliams2016) after the first year of the programme found that in the 32 participating ACOs spending per beneficiary was about 1% lower for beneficiaries enrolled in an ACO participating in the Medicare Shared Savings Program. ACOs with higher baseline spending generated larger savings, but there was no difference in the savings generated by ACOs whose providers integrated financially, compared with those that did not. In a follow-up study, McWilliams et al. (Reference McWilliams2018) found that shared-savings contracts entered into by groups of PCPs were on average associated with greater savings, and that the savings were higher the longer the groups had been participating in the scheme. The spending reductions generated by physician ACOs in 2015 amounted to US$ 256 million in net savings to Medicare, the payer. Hospital-integrated ACOs, which have weaker incentives to generate savings due to the implications for other revenue streams not covered by the ACO contract, did not on average generate statistically significant spending reductions, and the reductions that were generated were offset by bonus payments. Subsequently, concern about whether savings had been generated by providers selecting patients with lower risk was not supported by empirical evidence (McWilliams et al., Reference McWilliams2020).
Case study 3: Gesundes Kinzigtal, Germany
An example of a European-type ACO is provided by the Gesundes Kinzigtal (“Healthy Kinzigtal”) programme in Germany (Hildebrandt, Schulte & Stunder, Reference Hildebrandt, Schulte and Stunder2012). The programme started in 2005 and targets the entire population of the city of Kinzigtal, regardless of disease or age. The guiding principle of the programme is the triple aim concept – improving patients’ experience of care, improving population health and reducing per capita costs of care – and the main elements of the programme comprise self-management support, prevention, patient-centred care and an electronic networking system (Struckmann, Boerma & van Ginneken, Reference Struckmann, Boerma and van Ginneken2015).
The Gesundes Kinzigtal programme also aims to improve the financial margin for the purchaser, which in the German context are sickness funds, and in this specific case two sickness funds: AOK and LKK. The programme aims to generate savings within the Kinzigtal region as compared to German “standardized” costs, which are average costs across all sickness funds, and a reference period prior to the intervention. These standardized costs are calculated in the German risk adjustment mechanism, which allocates money from a central allocation pool to purchasers. Since 2009, allocations for each individual are based on age, sex and marginal expenditures for one of 80 diseases as coded the previous year (Buchner, Goepffarth & Wasem, Reference Buchner, Goepffarth and Wasem2013). The contracts between Gesundes Kinzigtal GmbH (i.e. the company) and the two sickness funds are based on the virtual budget of each fund’s total allocation from the central allocation pool – the budget is “virtual” because the money is not actually passed through to providers, who continue to receive their reimbursements from the sickness funds as usual. The financial result is measured by the total expenditure for the insured Kinzigtal population both within and outside partner institutions compared to the allocation from the pool. If the sickness fund spends less than it receives, the gain is shared between the fund and Gesundes Kinzigtal (Busse & Stahl, Reference Busse and Stahl2014).
Over the years the programme has managed to achieve savings. By 2010 the per capita expenditures of an LKK policy holder in the Gesundes Kinzigtal programme relative to those in the control group had decreased about 16.9% since 2005 (Hildebrandt, Schulte & Stunder, Reference Hildebrandt, Schulte and Stunder2012). An internal evaluation of the AOK and Gesundes Kinzigtal over the period 2006 to 2013 found that the programme had led to a net annual saving for the sickness funds of close to 3% (after sharing the 6.5% surplus difference with Gesundes Kinzigtal). In 2012, the relative cost reduction that could be allocated to the activities of the programme amounted to around 7.9%.
Policy relevance and conclusions
This chapter has shown why existing arrangements may be seen as failing to deliver appropriate care and has outlined the options for payers wishing to use the payment model to incentivize improvements in care coordination and integration. We then reviewed the available evidence for the effectiveness of these payment methods.
Improving care coordination and integration is, however, a complex task, and payment reform is unlikely to solve all problems of coordination. Rather, changes to the payment system should be seen as one (key) element in supporting the transition to coordinated and integrated services, but as emphasized by the review by Mason and colleagues (Reference Mason2015), leadership and communication across providers remain crucial facilitators for care integration.
Despite the criticisms raised against traditional payment systems such as FFS or payments based on DRGs, one benefit is that they require data to be collected on the activities undertaken by health care providers, making care processes more transparent. If payers change to a system of payment bundles that include multiple services delivered over a longer time period and across settings, it is important to consider how information about providers’ activities will then be collected. Even if new payment systems are supported by the monitoring of health outcomes or other indicators of care quality (which matters), information about providers’ activities remains essential for payers to assess the content of the care bundle that is delivered, and to assess the efficiency of care. Beyond monitoring the impact on health outcomes and activity, it is also crucial for payers to be mindful that payment changes can have distributional consequences and ensure that the equity consequences of reform are either monitored or explicitly addressed by the payment change.
Likewise, payers would do well to consider how to evaluate the impact of payment changes. For example, changes could initially be introduced to just a few providers (ideally randomly chosen), or gradually rolled out (again in a random order) to facilitate a controlled or stepped-wedge design, so allowing a comparison of key outcomes before and after the change, between an intervention and a control group. Moreover, policy-makers should be open to the possibility that some changes will not work out as hoped for, and in that case be prepared to seek explanations for why the change did not generate the desired impact, with the aim of revising the scheme and trying again.
With a key aim for new payment methods being the consideration of the impact of care by one provider on the need for care from another, facilitating the availability and integration of information enables providers to review the changes experienced in care provision. Still, it should be acknowledged that demand for health care is fundamentally uncertain – both for patients and providers. In light of this, new payment methods should not excessively assign risk to providers for outcomes that are beyond their control.
Nevertheless, many new payment methods do include shifting risk from payer to provider. Consequently, payers must redefine their role as one of setting objectives and ensuring that payment systems facilitate the achievement of these objectives. There is also a question of how to deal with changes in patterns of care that ensue from payment reform, which may result in some providers required to undertake fewer activities than previously.
Finally, payers should be mindful that, although demographic changes have created a need to rethink the way care is delivered which may be particularly relevant for patients with one or more chronic conditions, there is still a need for health care providers to respond swiftly to acute illness.
While the combined theoretical and empirical evidence suggests that financial integration such as shared-savings arrangements with careful design of incentives and information collection is a promising policy option for achieving the goals of integrated care, more empirical evidence is required before conclusions can be confidently drawn. Policy-makers are advised to have the need for further research in this area in mind when experimenting with new payment models, and to introduce new policies in a way that allows robust evaluation.Footnote 1


 Open access
Open access