

In the original publication “Guidance for switching from off-label antipsychotics to pimavanserin for Parkinson’s disease psychosis: an expert consensus,” by Black et al. (Reference Black, Nasrallah and Isaacson2018), the authors regret the errors found in Table 1; Boxes 1, 3, and 4; and Figure 1. The correct Table 1, Boxes 1, 3, and 4, and Figure 1 are given below.
Receptor binding affinities for select antipsychotic agents

+ weak binding affinity (100>Ki<1000)
++ moderate binding affinity (10>Ki<100)
+++ strong binding affinity (1>Ki<10)
++++ very strong binding affinity (Ki<1)
Abbreviations: 5-HT = serotonin; α = adrenergic; D = dopamine; H = histamine; M = muscarinic.
Ki (nM) values are derived from functional antagonist R-SATTM assays (ACADIA, San Diego, CA, USA).
“-” denotes no response.
Adapted from Hacksell et. al. Neurochem Res 2014; 39:2008-2017 and from data on file.
Dosing tips for switching to pimavanserin from low-dose (≤ 100 mg) Quetiapine (see Figure 3)
Add full dose (34 mg) pimavanserin to current low dose (up to 100 mg) quetiapine for 4 weeks
Allows pimavanserin to reach steady state and the duration of treatment necessary to reach its delayed onset of therapeutic action
Then reduce quetiapine by 50% weekly until reaching 12.5 mg, then discontinue
If efficacy for PDP diminishes during quetiapine taper, can return to previous dose level and try tapering again in 1 week
Dosing tips for switching to pimavanserin from low-dose (≤ 100 mg) Clozapine (see Figure 5)
Add full dose (34 mg) pimavanserin to continuing clozapine dose for 6 weeks
Then reduce clozapine by 6.25 mg weekly until discontinued and in no event, not less than 4 weeks of tapering
If efficacy for PDP diminishes during clozapine taper, can return to previous dose level and try tapering again in 1 week
Recommend not removing patient from clozapine registry for a few months in case clozapine must be restarted
Dosing tips for switching to pimavanserin from high-dose (> 100 mg) Clozapine (see Figure 6)
Add full dose (34 mg) pimavanserin to continuing clozapine dose for 6 weeks
Then reduce clozapine by 25 mg weekly until discontinued and in no event, not less than 4 weeks of tapering
If efficacy for PDP diminishes during clozapine taper, can return to previous dose level and try tapering again in 1 week
Recommend not removing patient from clozapine registry for a few months in case clozapine must be restarted
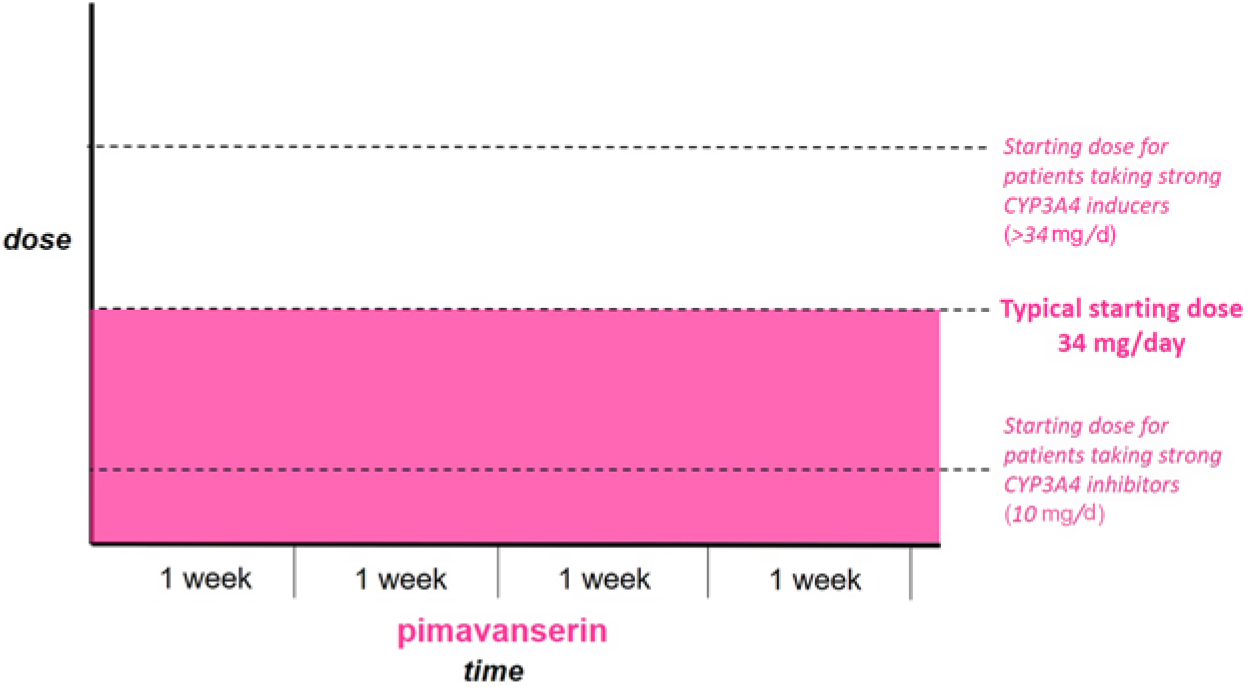
Patients not currently taking antipsychotic medication. Start full dose of Pimavanserin immediately.
In addition, the authors would like to make the following text corrections and clarifications:
Page 405:
The MDS EBM was published in 2011.
Page 406:
The doses in the early phase 2b/3 study were placebo, 8.5, and 34 mg/d.
The P-value for the hallucination and delusions subscales was 0.0012.
Sleep quality, caregiver burden, etc. were exploratory outcomes.
Page 407:
The QT prolongation for pimavanserin is 5-8 msec.
The original publication has been corrected to reflect these changes.



