


Introduction
Hospitals can act as hotspots for the emergence and dissemination of antimicrobial-resistant bacteria. We previously reported that the environments of tertiary care hospitals have a low prevalence of antimicrobial-resistant (AMR) bacteria including carbapenem-resistant Enterobacterales (CRE), AmpC beta-lactamase (AmpC), and extended-spectrum beta-lactamase (ESBL)-producing Enterobacteriaceae. Reference Mathys, Mollenkopf, Van Balen and Wittum1 AMR bacteria present in the environment of hospitals may lead to healthcare-associated infections and pose a risk to patient, visitor, and staff health. Reference Otter, Yezli, Salkeld and French2 We hypothesized that clinically relevant antimicrobial-resistant bacteria are present in publicly accessible areas of hospitals. We aimed to estimate the prevalence of vancomycin-resistant Enterococcus (VRE), methicillin-resistant Staphylococcus spp. (MRS), AmpC-producing, ESBL-producing, and CRE on surfaces in publicly accessible areas of a large tertiary care university hospital.
Methods
This study was performed at the Ohio State University Wexner Medical Center University Hospital (WMCUH) located in Columbus, Ohio, USA, a regional tertiary care facility that maintains approximately 900 beds. We sampled public areas of the WMCUH weekly for twelve weeks using electrostatic cloths (Swiffer, Proctor and Gamble, Cincinnati, OH), with the same 25 sites sampled each week. Sites were chosen to represent areas expected to have high human contact, such as elevator buttons, locations where gut microbiota may be found including bathrooms, and locations where patients with AMR bacterial infections were likely to be present including hospice and gastroenterology waiting areas. These areas of the hospital are expected to be routinely disinfected using disinfectant wipes (Oxivir 1 Wipes, Diversey, Fort Mill, SC).
Each cloth was cultured using selective media intended to facilitate the identification of bacteria expressing the CRE, AmpC, ESBL, VRE, or MRS phenotype following our previously described methods. Reference Mathys, Mollenkopf, Van Balen and Wittum1,Reference Too, Kariuki, Gitao, Bebora, Mollenkopf and Wittum3 Bacterial species were identified using MALDI-TOF and resistance genotypes were confirmed using PCR. The use of selective media allows for the detection of these antimicrobial-resistant bacteria on surfaces even when they are present in low numbers but provides no information about the quantity of these bacteria in the sample.
Results
A total of 299 samples were collected over 12 weeks of hospital sampling between May and July 2024. Of these, 28 (9.4%) samples tested positive for MRS, and all recovered isolates were found to be S. aureus. VRE, which included both E. faecium and E. faecalis, were recovered from 19 (6.4%) samples. Sixteen (5.4%) samples were found positive for ESBL, with 18 total isolates found due to two species of ESBL being recovered from the same sample in two cases. AmpC beta-lactamase producers, which included both bacteria with inducible and plasma mediated AmpC genes due to their clinical relevance, were found in 84 (28.1%) samples.
CRE were recovered from 16 (5.4%) samples, with 18 total CRE isolates recovered. These included Enterobacter hormaechei (n = 11, 61.1%), Leclaria adecarboxylata (n = 4, 22.2%), and one isolate (5.6%) each of Klebsiella pneumoniae, Klebsiella aerogenes, and Pseudomonas putida. Most CRE expressed bla NDM (n = 15, 83.3%) except two of the E. hormaechei and the P. putida which expressed bla KPC. Seven isolates of intrinsically carbapenem-resistant Stenotrophomonas maltophilia were also recovered but were excluded from our results.
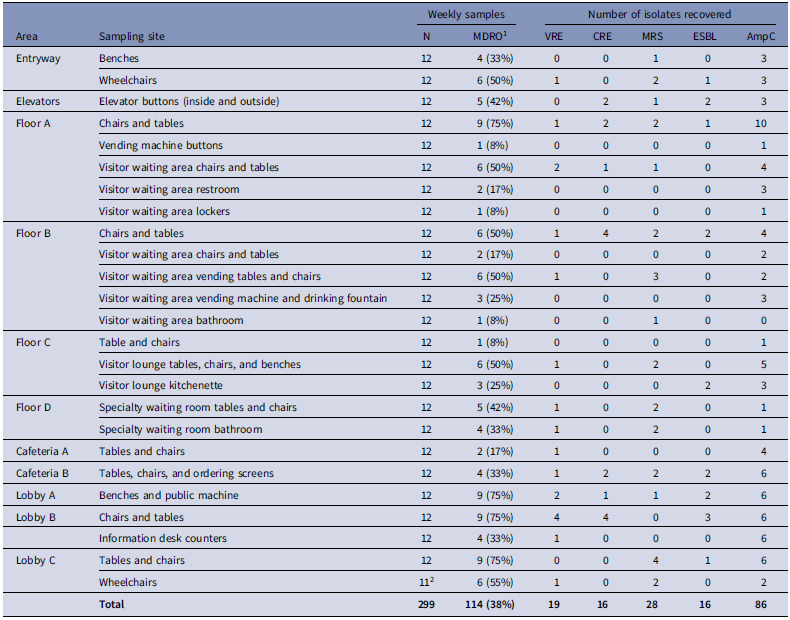
Details of the hospital surfaces from which specific AMR bacteria were recovered are presented in Table 1.
Proportion of samples from which one or more multi-drug resistant organism (MDRO) were recovered and frequency of recovery of antimicrobial resistant bacteria by resistance genotype from various environmental surface sampling sites over 12 weeks in publicly accessible areas of a large metropolitan tertiary care hospital

1 The number and percentage of samples at each site from which one or more MDRO were recovered, including VRE, CRE, MRS, ESBL, and AmpC.
2 The wheelchairs in lobby C were unavailable for sampling during one week of the project.
Discussion
Both the US Centers for Disease Control (CDC) and the World Health Organization (WHO) include CRE, ESBL, VRE, and MRSA in their lists of antimicrobial-resistant bacteria of greatest concern. 4,5 The WHO also lists third-generation cephalosporin-resistant Enterobacterales, including ESBL and AmpC, as a highest priority. 5 Our results indicate that these AMR bacteria can be present in publicly accessible areas of hospitals where visitors, staff, and patients may be exposed. These AMR bacteria may survive on surfaces for months which can result in healthcare-associated infections. Reference Otter, Yezli, Salkeld and French2 In addition, there is potential for further spread outside of the hospital by individuals who may become asymptomatically colonized or infected.
Both CRE and VRE are important causes of healthcare-associated infections resulting in a variety of serious conditions. Reference Abi Frem, Ghanem, Doumat and Kanafani6,Reference Sheu, Chang, Lin, Chen and Hsueh7 These AMR infections have been found to have higher mortality than their susceptible counterparts. Reference Martin, Fahrbach, Zhao and Lodise8,Reference Hemapanpairoa, Changpradub, Thunyaharn and Santimaleeworagun9 The presence of CRE in hospital environments may be of special concern due to their ability to disseminate in patient populations. Reference Cohen, Liu, Cohen and Larson10 Some of the CRE we recovered, including L. adecarboxylata and P. putida are of limited clinical importance. However, they may serve as a reservoir of mobile carbapenemase genes that can disseminate to clinically relevant organisms.
There were multiple instances of sampling sites that were positive with the same organism on consecutive weeks. These may represent failures of cleaning and disinfection or sites that frequently become contaminated.
We observed that chairs and tables in public areas were the most likely sites to be contaminated with AMR bacteria, including CRE expressing bla NDM, suggesting that these surfaces should receive additional cleaning and disinfection. To facilitate this, we shared our results with WMCUH infection control personnel. However, due to the public accessibility and frequent movement of visitors, staff, and patients, it may be challenging to reduce AMR bacterial contamination on hospital surfaces. Increasing the quantity and quality of cleaning in public areas may be one viable strategy to mitigate environmental threats. Routine environmental surveillance in hospitals may also be useful to identify areas where additional cleaning and disinfection should be targeted.
Financial support
The work received no direct financial support.
Competing interests
The authors report no potential conflicts of interest.

 Open access
Open access