Over 1.5 million persons evacuated the US Gulf Coast following Hurricane Katrina, one of the most destructive storms to hit the United States.Reference Groen and Polivka 1 Displacement can be particularly disruptive for children with diabetes. Persons with diabetes need ample supplies of insulin and other medications and must monitor their glucose and respond accordingly if adjustments are required.Reference Cefalu, Smith, Blonde and Fonseca 2 Yet, most families caring for children with diabetes are not prepared for self-management of the disease in the event of a major disaster, and families of lower socioeconomic status are less prepared than are higher-income families.Reference Renukuntla, Hassan, Wheat and Heptulla 3
Subject to federal approval, states can issue Medicaid emergency waivers to provide short-term health insurance coverage to those affected by disasters. Seventeen states issued waivers after Hurricane Katrina to provide coverage for those displaced, and the federal government allocated $2 billion in aid to help assist states defray the costs of the waiver.Reference Zuckerman and Coughlin 4 The waiver issued by Texas, known as TexKat, was the largest waiver and was in effect until June 2006.Reference Quast and Mortensen 5
Relatively little is known regarding how well the Hurricane Katrina Medicaid waivers performed. Furthermore, although it has been shown that local adults experienced a severe disruption in diabetes management,Reference Thethi, Yau and Shi 6 , Reference Fonseca, Smith and Kuhadiya 7 there is a gap in the literature on the effects of Hurricane Katrina on displaced individuals and on children with diabetes.
METHODS
We analyzed individual-level enrollment and claims data for children up to 17 years of age who were enrolled in Louisiana Medicaid from 2004 to 2006. To obtain the most complete picture of health care, we limited our sample to children who were enrolled every month during the 3-year period. We restricted our sample to individuals with an ICD-9 (International Classification of Diseases, Ninth Revision) diagnosis code of 250.xx, 357.2x, 362.0x, or 366.41 prior to September 2005.
We defined our control group as those children who met the above criteria and lived in a county not designated by the Federal Emergency Management Agency after Hurricane Katrina as an individual disaster assistance area. Children in the TexKat group were determined by whether their enrollment data indicated participation in the TexKat waiver program.
The characteristics of the TexKat and control groups are compared in Table 1 . The TexKat group was composed of 43 children, whereas the control group contained 742. Given the low statistical power resulting from the small sample of TexKat children, only descriptive statistics are reported.
Summary Characteristics of the TexKat and Control GroupsFootnote a

a Data are for children enrolled in Louisiana Medicaid from 2004 to 2006. TexKat was the Texas Medicaid Hurricane Katrina emergency waiver.
Generally, the gender and age profiles of the 2 groups were similar. Both groups had slightly more females than males and 11-17-year-olds constituted the largest age group. However, the TexKat group was composed almost entirely of blacks, whereas blacks made up slightly more than half of the control group.
Our analysis consisted of comparisons of the rates of diabetes maintenance tests and diabetes complications. We utilized difference-in-differences estimates, which can be thought of as a combination of pre-post and post-post comparisons. Specifically, we compared changes over time in the test and complication rates across the TexKat and control groups. By doing so, we controlled for differences across groups and over time.
An important condition for difference-in-difference analyses to be valid is the “parallel paths” assumption. This condition implies that, but for the treatment (here, displacement due to Hurricane Katrina), the test and complication rates would be roughly parallel between the 2 groups. Although we did not have sufficient pre-Katrina data to thoroughly test this condition, 2 aspects suggest that this assumption was not violated. First, with the exception of race, the summary statistics shown in Table 1 were quite similar. Furthermore, the pre-Katrina rates shown in Table 2 were also quite similar, which suggests that the use of these 2 groups likely satisfied the parallel paths condition.
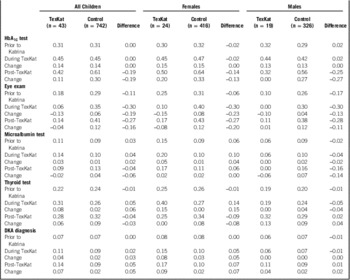
Difference-in-Difference Estimates of the Proportion of Children Receiving Maintenance Tests and Experiencing a Complication

a Data are for children enrolled in Louisiana Medicaid from 2004 to 2006. TexKat was the Texas Medicaid Hurricane Katrina emergency waiver. Abbreviations: HbA1c, glycated hemoglobin; DKA, diabetic ketoacidosis.
We analyzed the frequency of 4 diabetes maintenance tests (glycated hemoglobin [HbA1c], eye exams, microalbumin tests, and thyroid tests) and one diabetes complication (diabetic ketoacidosis, or DKA). (Laboratory test results were not available in our data.) We divided the 2004–2006 time period into 3 sections: the pre-Katrina time period was defined as January 2004 through August 2005, the “during TexKat” period spanned September 2005 to June 2006, and the post-TexKat period was from July 2006 through December 2006.
RESULTS
The annualized proportion of children in the TexKat and control groups who had the specified test or complication for each of the 3 time periods is shown in Table 2. The table is divided into 5 sections: the 4 maintenance tests and the 1 complication (DKA diagnosis). For the during TexKat and post-TexKat periods, the changes in proportions relative to the pre-Katrina period are shown.
The difference-in-difference estimates are reported at the intersections of the change rows and difference columns in the table. For example, for the HbA1c tests for all children, the proportions both prior to Katrina and during TexKat were identical in the TexKat and control groups. Thus, the changes were identical and the difference-in-difference estimate was 0. By contrast, the post-TexKat proportion was 0.42 for the TexKat group and 0.61 for the control group. Thus, the difference-in-difference estimate was −0.19 because the change for the TexKat group was 0.19 less than that for the control group.
Except for eye exams, the pre-Katrina proportions of the tests and complications were remarkably similar across the TexKat and control groups. This characteristic supports the plausibility of the parallel paths condition described above.
Again, with the exception of eye exams, the during TexKat proportions for the maintenance tests were relatively consistent across the 2 groups. The HbA1c proportions were exactly equal, whereas the microalbumin and thyroid proportions were slightly higher for the TexKat group than in the control group. Except for eye exams, the resulting difference-in-difference estimates were quite small and positive in magnitude, ranging from 0 for HbA1c to 0.06 for thyroid.
By contrast, the −0.19 difference-in-difference estimate for eye exams reflects the drop during TexKat period for the TexKat group and the increase in the control group. This relatively large negative estimate suggests that displacement may have caused a fall in the adherence rate for these exams. The proportions by gender indicated that the drop was especially pronounced for females.
The DKA proportions for all children showed a rise during the TexKat period for both groups, with a somewhat larger increase for the TexKat group. The proportions by gender indicated that the increase was largely due to females, with the complication rate nearly doubling for the TexKat group.
The post-TexKat difference-in-difference estimates for all 4 of the diagnostic tests were negative. For 3 of the 4 tests, while the rates increased for the control group, they decreased for the TexKat group. For instance, for microalbumin tests, the proportion for the TexKat group fell from 0.14 to 0.09 while it increased for the control group from 0.10 to 0.13. In the analysis by gender, the drops in the proportions of HbA1c and thyroid tests were driven by males.
The difference-in-difference estimate for DKA diagnosis increased in the post-TexKat period relative to the during TexKat period. While the complication rate stabilized for the control group, it continued to increase for the TexKat group. As was the case for the during TexKat period, the positive difference-in-difference estimate was largely due to females.
DISCUSSION AND CONCLUSIONS
Our results suggest that the TexKat program was largely successful in providing short-term care to children with diabetes who were displaced by Hurricane Katrina. With the exception of eye exams, the proportions of children who received recommended maintenance tests either remained the same or even increased slightly. While the increase in the proportion of children with a diagnosis of DKA during TexKat was slightly greater for the TexKat group than for the control group, the small difference is arguably understandable given the trauma of displacement.
However, those positive findings for the period immediately following Hurricane Katrina were reversed somewhat for the post-TexKat period. Whereas the proportion of children who received recommended tests continued to increase for the control group, the proportions either fell or grew at a much slower rate for the TexKat group. Also, whereas the rate of DKA diagnoses stabilized in the post-TexKat period for the control group, the rate continued to increase for the TexKat group.
Our findings indicate that although the Texas Hurricane Katrina emergency waiver appeared to have functioned well in the period immediately following the hurricane, Medicaid emergency waivers could be improved by ensuring that individuals continue to receive care after the waiver ends. Furthermore, our estimates of the post-waiver effects can be considered as a lower bound, given that our sample was restricted to those who were continuously enrolled in Medicaid. Those who were not enrolled in Medicaid following the waiver likely suffered an even greater disruption in care. Thus, the potential benefits of changes to ensure continuity of care could be greater than our estimates indicate.
Several potential improvements could be implemented to improve continuity of care following emergency waivers. For instance, outreach could be provided to waiver enrollees to assist them in enrolling in traditional Medicaid. For those who transition to traditional Medicaid, information should be targeted to these individuals to ensure that they are aware of their coverage and the availability of care. Furthermore, it has been recommended that for future disaster preparedness, Congress should enact a permanent, emergency Medicaid authority to quickly extend coverage to broad or targeted groups.Reference Lambrew and Shalala 8
Natural disasters like Hurricane Katrina have demonstrated that a key challenge to response and recovery is creating national policies and making national decisions that translate well to local levels.Reference Wizemann and Altefogt 9 Policy makers at the local and state levels should consider partnering with health care providers in pre-disaster planning and organization of resources. The Affordable Care Act’s increased investments in health centers 10 is designed to improve both quality of care and coordination of care, which may prove to be instrumental in helping providers deliver continuous post-disaster care for vulnerable populations.
Limitations
There were several significant limitations to this study. First and foremost, our small TexKat sample prevented us from establishing statistically significant differences across the proportions of the TexKat and control groups. Relatedly, our restriction to children continuously enrolled in Medicaid during the 2004–2006 period, while necessary to observe a complete picture of the health care received by the children, significantly restricted our sample. Also, differences in the racial composition between the TexKat and control groups may have had an effect on the health care received by the 2 groups, and thus our estimates may not purely reflect the effect of displacement.
Funding
Supported by the Eunice Kennedy Shriver National Institute of Child Health & Human Development of the National Institutes of Health under award number R03HD079758. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.