


Introduction
Temporary Childbirth Migration (TCM) is a practice common in much of South Asia, including India, in which a woman returns to her natal (her own parents’) home at some stage during her perinatal period (Diamond-Smith et al., Reference Diamond-Smith, Gopalakrishnan, Patil, Fernald, Menon, Walker and Ayadi2024a; Berkman and Glass, Reference Berkman, Glass, Berkman and Kawachi2000; Bandyopadhyay, Reference Bandyopadhyay2009), whereas her husband and his family continue to stay in their marital home, and this pattern is driven by the underlying common practice of exogamy, where women marry someone often living in another village, district, or state and mostly live with their husband’s parents (her in-laws) (Bhattacharya et al., Reference Bhattacharya, Dwivedy, Nandeshwar, De Costa and Diwan2008). Estimates from previous research conducted by the team indicate that the prevalence of temporary childbirth migration ranges from around 30% to over 80% (Diamond-Smith et al., Reference Diamond-Smith, Gopalakrishnan, Patil, Fernald, Menon, Walker and Ayadi2024a, Reference Diamond-Smith, Patil, Agarwal, Juvekar, Murro and El Ayadi2024b; Berkman, Reference Berkman, Glass, Berkman and Kawachi2000; Bhattacharyya et al., Reference Bhattacharyya, Srivastava and Avan2013).
While a new body of research is describing the patterns of temporary childbirth migration (duration, timing, etc.), little is known about factors driving this practice. Quantitative data from two states of India (Bihar and Madhya Pradesh) found that some women are more likely to return to their natal homes than others; specifically, women are more likely to return for the first birth, and more educated, wealthier women are more likely to return (Bandyopadhyay, Reference Bandyopadhyay2009). The most common reason that women reported returning to their natal home (reported by over 50% of women in both states) was that they would get better care, rest, or comfort at their natal home. A qualitative study in Mumbai also found that women wanted to migrate to receive more care and support and because they expected to work less and have lower health-related costs (Blanchard et al., Reference Blanchard, Bruce, Jayanna, Gurav, Mohan, Avery, Moses, Blanchard and Ramesh2015). Another study in Bangalore found that women highly valued the support of their own mothers during pregnancy, childbirth, and postpartum, and mothers were seen as the most important support source during this time (Bloom et al., Reference Bloom, Wypij and Das Gupta2001). A qualitative study in Tamil Nadu found that returning to the natal family was critical because the woman’s parents were expected to cover childbirth costs in addition to caring for her (Cambridge University Press, 2024). Other studies of traditional pregnancy and childbirth practices mention the return to the natal home as providing mothers with sufficient rest and a break from their routine household chores, important for preventing infection, or influenced by views about ‘ritual pollution’ stemming from menstruation (Edmonds et al., Reference Edmonds, Paul and Sibley2011; Corbett and Callister, Reference Corbett and Callister2012). These suggest that there are various support roles that the natal family can play for women and that impact the decision to migrate.
Thus, while social support has been described as a factor influencing temporary childbirth migration, past research has not disentangled what types of care and support women want and feel that they do not get in the marital home. Understanding more about the types of care, or support, that women expect to get at their natal home and how these play into the migration decision-making process will help us understand drivers of this phenomenon. Higher levels of perceived social support during the antenatal and postpartum periods are associated with better maternal mental health outcomes and a reduced risk of depressive symptoms among new mothers (Stapleton et al., Reference Stapleton, Schetter, Westling, Rini, Glynn, Hobel and Sandman2012); moreover, studies across the United States of America, Japan, Brazil, and India have shown that fewer available supportive persons during pregnancy is a predictive factor for antenatal and postpartum depression (Gawde et al., Reference Gawde, Sivakami and Babu2016), with women who have lower levels of social support having higher odds of developing suicidal ideation (Hodnett et al., Reference Hodnett, Gates, Hofmeyr and Sakala2013). Most research on social support and pregnancy has focused on its effect on mental health, with less research looking more broadly at social support itself, which social support domains women value most, and how the desire for specific domains of social support being provided by specific support persons determines behaviours such as temporary childbirth migration.
Past theory has delineated four common types of social support: instrumental, emotional, informational, and appraisal (Jeyashree et al., Reference Jeyashree, Kathirvel, Trusty and Singh2018). There is some limited past research in South Asia that heightened the importance of the different types of social support that women want during pregnancy and postpartum. In a study in Pakistan, pregnant women most commonly mentioned four types of social support that they highly valued: practical help with routine activities, information/advice, emotional support and assurance, as well as the provision of resources and material goods (Naraindas, Reference Naraindas and Selin2009). However, different people were seen to be best able or positioned to provide certain types of support, with mothers and mothers-in-law equally being mentioned for practice help with routine activities.
The majority of research on support in the perinatal period has focused on women’s support at the time of delivery. A qualitative study in India highlighted the importance to women of having a support person at the time of delivery on their experience of the birth (Pasricha et al., Reference Pasricha, Kochhar, Shah and Bhatia2021). However, quantitative data from India found that 13% of postpartum women reported that they had no one to provide support in labour, and 10% had no one to provide encouragement in labour (another indicator of support). Other indicators of social support were also low (helping them talk to providers, bring them food, etc.) (Raman et al., Reference Raman, Srinivasan, Kurpad, Dwarkanath, Ritchie and Worth2014). Again, different people provided different types of support, with mothers/mothers-in-law providing encouragement (emotional) support and husbands providing instrumental (bringing food/water) support, for example (Diamond-Smith et al., Reference Diamond-Smith, Sudhinaraset, Melo and Murthy2016). A systematic review of interventions (mostly in high-income countries) to increase support for women at delivery (with a birth companion, doula, etc.) found increases in spontaneous vaginal birth, decreased use of anaesthetics, higher APGAR score, and fewer negative feelings about childbirth (Raman et al., Reference Raman, Srinivasan, Kurpad, Dwarkanath, Ritchie and Worth2014). A qualitative study about decision-making around where to deliver (private or public facility) in India found that perceptions about where women could get the most social support were important factors (Rao and Finnoff, Reference Rao and Finnoff2015).
While existing literature shows that supportive social factors during pregnancy, childbirth, and postpartum improve maternal experience and can potentially improve maternal health outcomes, there is little data on the impact of social support on the decision to migrate in the perinatal period. If women are seeking specific forms of support and they perceive that their own mother, compared to their husband or mother-in-law, can provide that better, they may be more likely to choose to migrate during pregnancy, for example. The aim of this paper is to describe perinatal social support needs and preferences and explore how social support considerations influenced temporary childbirth behaviour and how social support norms and structure (health systems access) intersect with the desire for social support. Additionally, this paper considers the differing roles of women, their husbands, and their mothers-in-law in the decision to migrate temporarily or not. Finally, this paper considers the role of cultural factors and community norms surrounding TCM.
Methods
This study was conducted at the Vadu Health and Demographic Surveillance System (HDSS) in Western Maharashtra, India, which longitudinally updates the demographic data and vital events of a population of 180,000 since 2002. Although the overall study is a mixed-methods study, only qualitative findings are reported in this paper. The study was approved by the KEM Hospital Research Centre institutional ethics committee (KEMHRC/RVM/EC-1899 dated 29th September 2022) and the University of California, San Francisco IRB (UCSF IRB no. 22-36484). The study was conducted as per the Indian Council of Medical Research—National ethical guidelines for biomedical and health research involving human participants. The data were collected after administering written informed consent of the participants.
A total of 41 in-depth qualitative interviews were conducted by KT, RP, and SK with triads consisting of the index woman, her husband, and her mother-in-law. Each interview lasted approximately 30–40 minutes. Most interviews were conducted in person at participants’ homes; a few interviews with husbands were conducted at their workplaces in a separate room for convenience, ensuring privacy and safety of the interviewers. Each member of the triad was interviewed separately. All interviews were conducted in the local language, audio-recorded with participants’ consent, and later transcribed and translated for analysis.
All eligible participants (n = 181) were identified from the Vadu HDSS database (January 2022–January 2023). A purposive maximum variation sampling strategy was used to ensure diversity in age (21–38 years); education (no formal education to postgraduate); occupation (working/non-working); type of marriage (arranged/love); migration type and distance; parity; number of live births; and delivery mode (vaginal/caesarean). Women who had delivered within the past two years were included, while pregnant women were excluded to enable reflection on both prepartum and postpartum phases of TCM. Sampling was conducted iteratively. Recruitment decisions were reviewed throughout data collection to ensure coverage across predefined characteristics and to address emerging gaps. Women, husbands, and mothers-in-law were recruited concurrently. Data collection continued until thematic saturation was reached, defined as the point at which no new themes emerged.
Data were collected using the in-depth interview guides, which included sections on perceptions about TCM, timing and duration of TCM, reasons for TCM, decision-making, factors affecting the decision, people involved, factors influencing the TCM, cultural practices or beliefs for TCM, impact on access to health, etc. Support received by the participants, including informational, emotional, esteem, and tangible support that may have influenced TCM and related decision-making, was also discussed.
Two distinct methods of analysis were used. Initially, a rapid analysis method was used to assess and interpret iterative findings and to guide ongoing in-depth interviews (Vindrola- Padros and Johnson, Reference Vindrola-Padros and Johnson2020) with summaries organised in Microsoft Excel. To ensure accurate analysis, the interviews were audio-recorded and later transcribed and translated in Microsoft Word. The translated transcript was imported into Dedoose, a web-based qualitative data analysis software (Socio Cultural Research Consultant, LLC, Los Angeles, CA, United States of America), and systematically coded using a combination of deductive and inductive approaches. Data analysis was undertaken in 2025.
Predefined codes were utilised for consistency, while additional codes identified during the analysis process were also incorporated using an inductive and deductive coding approach (Guest et al., Reference Guest, MacQueen and Namey2012). The analysis was theoretically informed by the four domains of social support (Jeyashree et al., Reference Jeyashree, Kathirvel, Trusty and Singh2018). Each transcript was double-coded by two members of the team to ensure coding reliability and uniformity. Coding was done by a three-person team based in the US, including two individuals of South Asian descent. Further analysis was done by members of the US- and India-based teams, and throughout the process, there was constant communication between teams to ensure that interpretation was informed by the local context. Despite this, the perspective of western-born team members may have influenced some interpretation. All members of the coding and analysis team were also cisgender women, some of whom had gone through childbearing, and thus, the interpretation of data was influenced by the team’s lived experiences.
Result
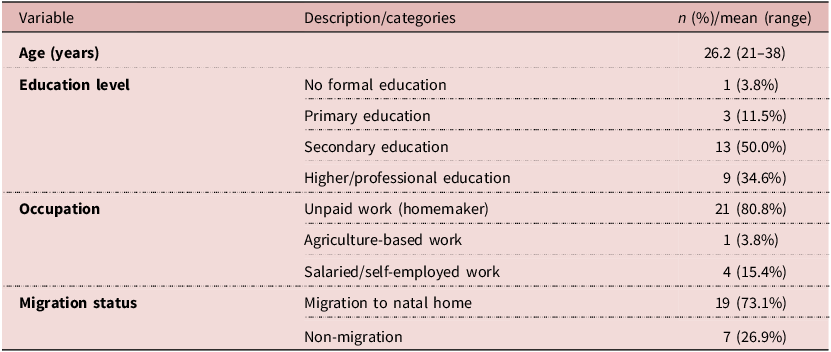
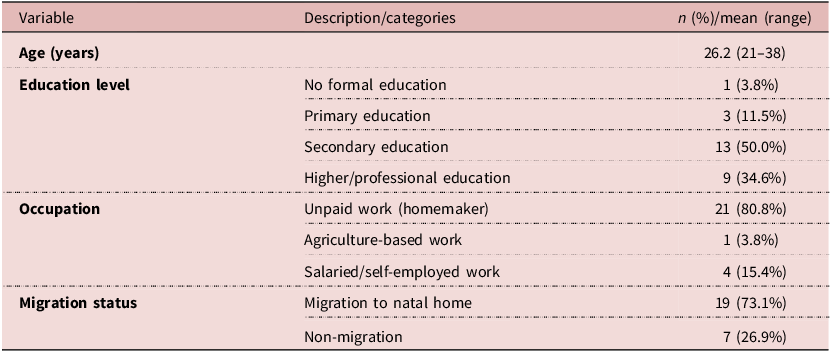
A total of 26 women who had recently delivered were included in the study, the sociodemographic characteristics of which are described in Table 1 below. A further 10 husbands (mean age 31.3 years; range 27–37) and 10 mothers-in-law (mean age 51 years; range 43–59) were interviewed.
Sociodemographic characteristics of delivered women (N = 26)
One focus group discussion (FGD) was also conducted with five women who had delivered within the past two years. Participants described a range of types of social support they desired, the different persons they wanted that support from, and how that impacted their behaviours around migration. They also described how other factors influenced their decision to migrate in pregnancy and intersected with their desire for social support.
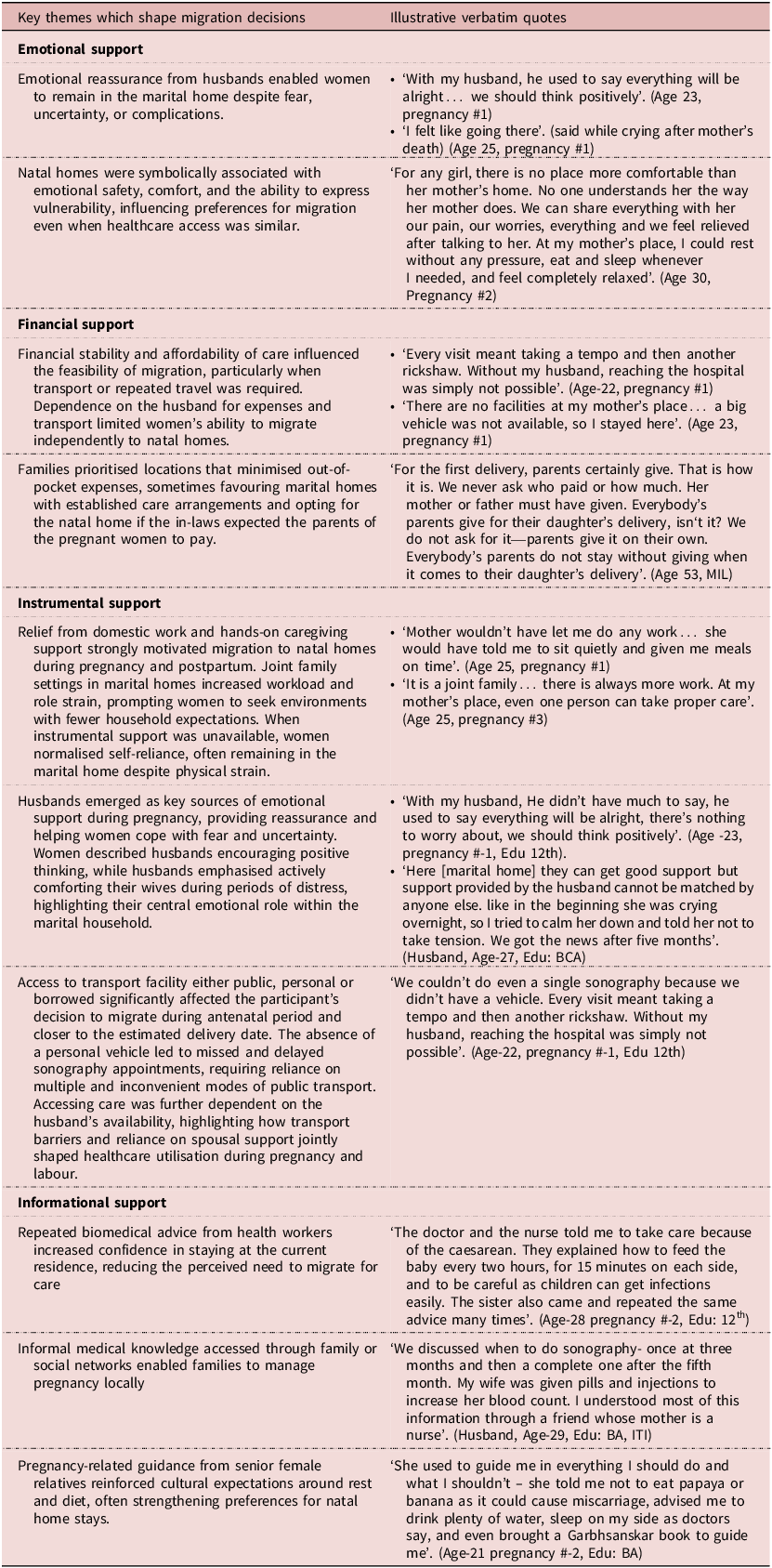
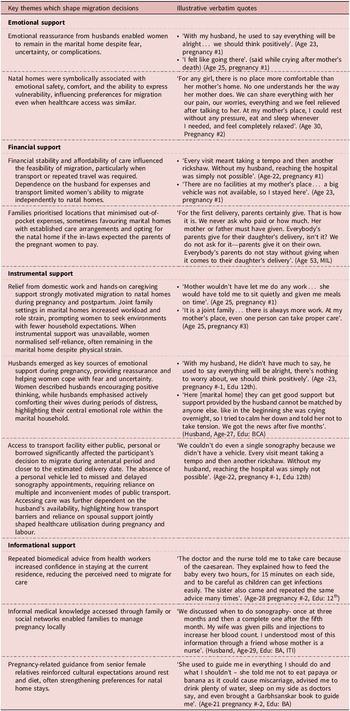
Below we describe main themes, with additional illustrative quotes avaliable in Table 2.
Key themes which shapes migration decisions and illustrative verbatim quotes
Social support
Emotional support
Emotional support during pregnancy and childbirth is an important aspect of overall well-being. Participants emphasised the benefit of emotional backing from family members, particularly their mothers and/or husbands. The study participants highly valued the presence of a supportive environment where they felt understood, cared for, and free from stress and judgement. One participant shared: ‘When I’m at my mother’s place, I feel free. There’s no tension, I can do whatever I want, everything revolves around me’. (Age- 21 pregnancy #-2, Edu: Graduate)
While another participant shared how her mother would provide psychological support and she would not have to worry about people being irritated with her:
‘Yes, psychological support is absolutely required, rest of things are immaterial. No irritation in any case. Mother never gets irritated…You experience everything afresh during your pregnancy and therefore only your mother is required to be nearby for psychological support’. (Age-27, pregnancy #1, Edu: Graduate)
This reflects the nurturing atmosphere that pregnant women or new mothers often seek, where their emotional needs are prioritised. It also highlights the potential fear women have about how they are perceived (being irritating, potentially) in their husband’s home.
Financial support
Participants also highlighted the role of financial assistance from their husbands, in-laws, or parents for expenses related to pregnancy and childbirth. The finances included expenses incurred during pregnancy (including medical check-ups, sonographies, other necessities, and, later, for the delivery itself). The ability to access adequate healthcare, purchase necessary supplies, and cover medical expenses contributes significantly to the overall well-being of expectant mothers. One participant shared the following about her cousin’s experience:
‘At that time, she [her cousin] told me that her in-laws were saying that if you go to your mom’s place, they will take care of the expenses. So, her husband also said that you go there for the delivery, and even she was taking treatment in a private hospital, but they [cousin’s in-laws] insisted she go to the government hospital for treatment, so she told me that she was going to her mother’s place for the delivery. And I was not sure if I would go or not. But afterwards I felt like going to mother’s place so I went’. (Age-24, pregnancy #1, Edu: Graduate)
In contrast, another participant’s husband said he chose to keep his wife at their home due to his belief that he should pay the delivery costs:
‘If she is my wife, then why should I ask her parents for money and medicine? Caesarean costs around 70,000 to 80,000 rupees at least. If it [child] is mine, then it should be my responsibility. Why should I let them [his in-laws] do it? Of course, she can go afterward for a month if she wants to go’. (Husband, Age-37, Edu: primary school education)
Financial support was thus an element of social support that was considered in the temporary childbirth migration decision-making process but could act in both directions.
Instrumental support
Practical assistance with daily chores and caregiving is essential for pregnant women, particularly during the later stages of pregnancy and the postpartum period. As during these stages, women frequently experience reduced mobility due to abdominal enlargement, back pain, pelvic discomfort, fatigue, and medical advice to limit strenuous activity, making it challenging to manage routine household tasks independently. Participants recounted the support received from family members, especially their mothers and mothers-in-law, in managing household chores, cooking, and caring for other family members. If the doctor recommends bed rest and there’s someone available in the marital family to manage household chores, women opt not to travel to avoid discomfort. However, if there’s no assistance available, the family chooses for the woman to relocate to the maternal household, allowing her to rest fully. Intertwined with the desire for help with household tasks was a fear of a negative reaction from mothers-in-law if she was perceived as not working enough or adding work to others (namely, the mother-in-law).
‘I wanted to go to the natal home because you get to rest in the natal home…In the In-law’s home you cannot get it. Mother-in-law will scream if you do not complete it, or she does housework and she gets overburdened with housework. We also feel bad so that’s why going to a natal home is better’. (Age-38, pregnancy #-3, Edu: higher secondary education)
One mother-in-law described how she specifically called her daughter-in-law back to her marital home (away from the natal home) because she needed more help in the house:
R: We hurried [to bring the daughter in law back to marital home] because then I could go to the farm… we thought that if we brought her here, then she would be a company and a person is required to do housework because it is quite troublesome to cook after coming from the farm, isn’t it? (Mother-in-law- Age-59, Edu: illiterate)
Availability of better care and support was one of the most common reasons for migration to a natal home. However, not all women saw there being better instrumental care at their natal homes. Some participants described how the care they received from family members, particularly their mothers-in-law, played a crucial role in ensuring a smooth and comfortable pregnancy experience. For example, a mother-in-law explained how, given her own memories of how hard it was being pregnant as a daughter-in-law herself in her youth, she wanted to try to help her own daughter-in-law.
‘Talking about workload…if my daughter in law is sleeping anytime, I am the one to do all the work…I can understand that she is about complete nine months of her pregnancy and she doesn’t feel like doing (work) now… I look after her just the way I do with my daughter…I do her things. She is daughter in law…previously during our times things used to be like no matter how much mother-in-law asked to bring or do, we were asked to do all the work right up to the time of delivery, but I do not like to do that to her. I do not want her to suffer the way I have suffered… She also has the same feelings as I used to have then I should keep my things in my mind and try to understand her’. (Mother-in-Law, Age-45, Edu: Secondary education)
Thus, there were variations in the level of instrumental support provided at different locations.
Informational support
Access to reliable information and guidance from experienced family members is crucial for pregnant women and new mothers. Participants expressed a preference for seeking advice from older family members, particularly elder women, who have first-hand experience with pregnancy and childbirth. Their wisdom and insights provide reassurance and guidance to expectant mothers during this transformative period. A participating husband emphasised this point, stating, ‘…the actual person who has gone through this procedure, that person can guide you more accurately’. Another participant shared it was her mother who could provide this best to her:
‘Yes, as the due date approaches, there is a fear in the mind about what to do. Now, what will happen? What will happen next? It means, when I get some information from my mom, it is like this or it happens like this, you don’t have to worry about it. That little information shared with my mom gives us some insights, and if it seems appropriate, then we feel like we should go to our mom’s place for a while. We should get information from her about what happens to us, and we should share it with her. That’s why we go there’. (Age-24, pregnancy #-1, Edu: Graduate,)
The availability of elder women who can provide guidance was a primary factor in the decision to migrate during childbirth, and this could act as either a push factor to the natal home or a pull factor to stay at the husband’s home, depending on where there were perceived to be more elder women to provide guidance. For example, a participant’s husband believed his wife should not migrate due to the perceived lack of delivery information at her natal home:
‘Because their side of people had no idea about the delivery, about anything. Her mother does the job and no one is there at home. Room is also smaller… They live there on rent, that’s the situation. And as my sister’s delivery was done by my mother only, she had the information. So that’s why, [my mother] said, let’s do it here only. My mother has all the information, so let’s do it here’ (Husband- Age-29, Edu: Graduate with vocational diploma)
Other factors influencing temporary childbirth migration
Access to health care facilities
Access to adequate healthcare facilities was also cited as an important consideration in determining the most suitable environment to be in during pregnancy, childbirth, and into the postpartum period. A participant explained,
‘Although I wanted to stay with my own family, we decided to stay with my in-laws due to their support and the convenience of being closer to medical facilities’. (Age-38, pregnancy #2, Edu: Higher secondary school)
Women who had higher risk pregnancies were more likely to make decisions based on access to support and medical facilities. As one husband described:
‘The doctor told us that the baby is not growing well from the 6th month of pregnancy due to high blood pressure. Due to this, we took the decision of migrating to maternal home even before dohale jevan [traditional baby shower.]’ (Husband, Age-24, Edu: Graduate)
Household status
Comfort during pregnancy and childbirth is paramount for expectant mothers, as it directly impacts their physical and emotional well-being. Participants described how being able to meet their preferences surrounding eating practices and clothing contributed to their comfort during pregnancy. The ability to choose comfortable attire and adhere to dietary preferences reduced discomfort and enhanced overall satisfaction with the pregnancy and postpartum experience. This choice was often easier to exercise at maternal homes as compared to marital homes, where women have less decision-making power. Relatedly, women’s social standing in the husband’s house, where she generally has low status, contributed to her overall feelings of power and freedom and subsequent comfort and happiness.
‘There were many such restrictions. It felt like being tied up in such bonds…our house doesn’t have the freedom to go out and roam freely like others. We need that freedom, right? To do small things or to organize something special for the children, we eagerly do things or celebrations for small children, right? Our (maternal) house gives a lot of freedom, unlike here. Only the husband supports me, but he is also answerable to his mother, so I feel suppressed because of that’. (Age-29, pregnancy #-1, Edu: B.A,)
Role of husbands
In cases where women decide not to migrate, they seek emotional support with from husbands instead of their mothers-in-law. Nonetheless, husbands may lack the knowledge and experience required to provide effective support during childbirth, and they may express apprehension about potential complications. The husband of a woman who has migrated during childbirth summed up the situation by saying:
‘They share it with the mother (pregnant woman’s mother). The mother has an experience. If she had stayed here, she could share things with me, I could possibly get happiness but there are few conditions in which I have no experience of, so I can’t tell anything. So, the actual person who has gone through this procedure, that person can guide you more accurately. Like, ‘Dear, some distress is normal’. There are types of false labors 10 to 12 days earlier. Such things a mother would know better’. (Husband, Age-27, Edu: BCA)
Discussion
While the tradition of temporarily relocating to one’s natal home during the first childbirth is a prevalent practice, it is important to note that this decision is influenced by various factors. These factors encompass considerations such as the availability and competence of caregivers, access to transportation, and proximity to healthcare facilities in case of emergencies. Financial considerations such as the availability of resources and financial stability influence the choice of where to stay during pregnancy and childbirth. Location choice also hinges on the availability of transportation and proximity to healthcare facilities, particularly in high-risk pregnancies or when the expectant mother faces potential health complications. The decision is further influenced by where the woman believes she will receive better post-delivery care. Aside from these more practical financial, informational, and instrumental forms of support, the desire for emotional support from maternal figures was cited as the most important consideration in determining the most suitable environment for pregnancy and childbirth. This is in line with previous research that highlighted the important role of emotional support from women’s mothers and their broader natal family in the perinatal period and the vital impact that can have on mental health (Gwen and Kruckeman, Reference Stern and Kruckman1983). The findings reinforce the existing conceptualisation of childbirth return as an act of ‘mothering the mother’, providing necessary support during a particularly vulnerable time period (Reji, Reference Reji2012). While prior studies have mentioned other forms of support (aside from social/emotional), including instrumental (for example, a woman’s parents covering childbirth costs) or tangible (postpartum women’s own mothers taking on household chores responsibilities), none of these prior studies looked across the different domains of social support. The findings suggest that there are several different types of support roles that the natal family can uniquely play for women and that impact why women want to return to their parents’ home. While emotional reassurance, financial coverage, respite from domestic labour, and guidance from experienced kin are positively seen, access to healthcare remains a prominent contributor to the decision of migration.
Importantly, these factors can act as both push and pull factors. Where different forms of support are stronger in the natal home, women may prefer going there, but in some cases, women and their families perceive better care and support (of various forms) in the husband’s home. Many women express a preference for returning to their natal home during childbirth because they find reassurance and emotional support from their mothers, with whom they can confide. Newly married women may not have formed a close bond with their mothers-in-law since they are newly married, which adds to their inclination to choose their natal home. In other words, where relationships or resources in the husband’s home were stronger, women might stay, but where bonds and/or access to resources were stronger at the natal home, she might prefer to return. More research on what factors (type of marriage (love/arranged), actual socio-economic status of the respective households, etc.) could help us understand where women are most likely to get the care they need and how to help women meet those goals. Although a prevalent practice in South Asia, the study findings could be contextualised to people of South Asian descent in the global north for childbirth practices.
Of note, for the most part, the decision-making process was described as being inclusive, with women having a voice and often both in-laws, parents, and husbands being involved in the process, which has been found in other studies in urban slum areas of the same state in India (Sudhinaraset et al., Reference Sudhinaraset, Beyeler, Barge and Diamond-Smith2016). Given that this is a more rural area, this was somewhat surprising given the low decision-making power that women often have in the Indian context around other types of household decisions (Taylor et al., Reference Taylor, Nath, Sokolova, Lewis, Howard, Johnson and Sweeney2022). However, prior research has found that women often do have more of a voice in decisions around childbirth than in other aspects of their lives (Webster et al., Reference Webster, Nicholas, Velacott, Cridland and Fawcett2011). Relatedly, a women’s role in her household (her status or empowerment) also played a key role in her desires to migrate or not. Past research has found that women have lower status in their husband’s home compared to their natal home (Wells and Dietsch, Reference Wells and Dietsch2014), and thus, when women have the opportunity to return to their natal home, where they are more able to eat the food they want and express themselves as needed, especially during an emotionally and physically important and potentially challenging time, they may take advantage of that opportunity. Temporary childbirth migration may be a socially sanctioned time for women to return to a safer and more comfortable setting.
While this study has many strengths and adds to the literature by including multiple perspectives (women, husbands, and in-laws) and diving deeply into an understudied topic, it also has limitations. Data was collected from only one district in one state of India, and thus, is not representative or generalisable to other parts of India or other countries. The prevalence of temporary childbirth migration practices differs across India and is particularly high in this region (∼80%); therefore, reasons for migration may differ from those in areas where it is less common. Finally, data was collected in 2023 about women who delivered in the past year, which overlapped with significant COVID-19 waves in India. This may have impacted some women’s experiences of temporary childbirth migration during that time period; however, as no direct questions were asked about the impact of COVID-19, relatively few women mentioned this as something affecting their temporary childbirth migration behaviours.
To conclude, one of the main drivers of temporary childbirth migration is social support, but there are many forms of social support that women desire, and in some cases, these are better met at the natal home, and in other cases, the husband’s, home. A women’s status in her household, and the difference in the status between the two households, underlies and impacts her need for different types of support. By recognising the importance of emotional, financial, informational, and instrumental support, as well as the complex factors influencing decision-making processes, healthcare providers and policymakers can better support expectant mothers and promote positive maternal and child health outcomes. Additionally, prioritising comfort and accessibility of care ensures that expectant mothers receive the support and resources they need to navigate pregnancy and childbirth safely and comfortably.
Author contribution
RP, AMA, SJ, and NDS conceptualised the study and acquired the funding. RP, KT, SK, and DA acquired the data. AN, KT, RM, and SK coded the data; RP, AN, RM, and NDS analysed and interpreted the data. RP, AN, and NDS drafted the manuscript. All authors reviewed and revised the manuscript. All authors have approved the submitted version (and any substantially modified version that involves the author’s contribution to the study). All authors agree both to be personally accountable for their own contributions and to ensure that questions related to the accuracy or integrity of any part of the work, even ones in which the author was not personally involved, are appropriately investigated and resolved and the resolution documented in the literature.
Funding statement
The study was funded by National Institutes of Health grant ID R01HD107197.
Competing interests
The authors have no competing interests as defined by BMC or other interests that might be perceived to influence the results and/or discussion reported in this paper.
Ethical standard
The study was approved by the KEM Hospital Research Centre institutional ethics committee (KEMHRC/RVM/EC-1899 dated 29th September 2022) and the University of California, San Francisco IRB (UCSF IRB no. 22-36484).
Consent process for participants and confidentiality
All participants were informed about the study purpose, procedures, and potential risks and benefits using a participant information sheet. The consent process included verbal explanation by the research team and written or thumb-impression consent from participants. Participation was voluntary, and participants were free to withdraw at any point without consequences. Interviews were conducted only after obtaining written informed consent. All data collected were kept confidential by using coded identifiers instead of names. Audio recordings and transcripts were securely stored, and no personal information was disclosed in any publication or presentation.

 Open access
Open access