


Introduction
In recent years, significant attention has focussed on how we train cardiology fellows within congenital cardiology. Reference McMahon, Tretter and Redington1-4 The quality of training trainees receive is important as it has implications for the care provided to patients with CHD. Although this focus on training is a welcome advance, there has been limited attention drawn to the training provided to their trainers within the wider congenital cardiology community. Reference McMahon, Tretter and Redington1–Reference McMahon, Heying and Budts2 There are several clear guidelines on training in North America, published under the umbrella of the Accreditation Council for Graduate Medical Education 4–Reference Stout, Valente and Bartz9 the standard of training in Medical specialities proposed by the European Union of Medical Specialists (UEMS https://www.uems.eu/about-us/presentation/aims-and-objectives) and publications for general and specialist training from the Association for European Paediatric and Congenital Cardiology working groups. Reference Heying, Albert and Voges10–Reference Reinhardt, Hansmann and O’Sullivan16 However, there are limited data on the current status of training of congenital cardiology trainers, their capacity to train and provide assessment and feedback in this setting applied across different European centres. Recent publications have drawn attention to the fact that trainees often experience stress related to the cognitive overload they encounter in paediatric cardiology fellowship training. Therefore, it is important to have effective trainers to ensure a state of the art training and avoid exacerbating such anxiety. Reference Brown, Binney, Gauthier and Blume17 The importance of how we train trainers in other areas of medicine has received significant focus in recent years, despite its lack of discussion in the congenital cardiology world. Reference Ukachukwu, Petitt and Usman18–Reference Grant23 This is important because the provision of feedback to trainers is fundamental to them improving their methods of teaching, assessment techniques and their own capacity to provide effective feedback to their trainees. Reference McMahon, Tretter and Redington1
We hypothesised that there is marked variation in the training of trainers between different countries. The research questions in this study included (1) what is the current status of trainers among paediatric cardiology training centres across different European countries; (2) what is their knowledge of different instructional techniques; (3) how much support is provided to trainers to teach and train in such centres across Europe; and (4) how could Association for European Paediatric and Congenital Cardiology support the training of trainers.
Definitions
Association for European Paediatric and Congenital Cardiology training centres are registered on the website and are defined as centres capable of providing the core training to enable fellows to reach competency/capability to work as an independent paediatric cardiologist.
Competency-based medical education encapsulates education which focuses on fulfilling critical competencies the trainee must acquire to meet the healthcare needs of their patients (e.g. the Canadian Medical Education Directive for Specialists (CanMEDS) roles of medical expert, communicator, collaborator, leader, health advocate, scholar, and professional). Reference Pritchard, Alavian, Soogoor, Bartels and Hall24
Education relates to gaining theoretical knowledge relevant to a specific field.
Training relates to the action of learning practical skills, acquiring knowledge and experience.
Entrustment assessment combines the evaluation of learners’ knowledge, skills, and behaviours with the evaluation of their readiness to be entrusted to perform critical patient care responsibilities.
Trainer is a paediatric cardiologist with the responsibility of educating and training paediatric cardiology trainees.
Trainee is a postgraduate doctor in training to become a qualified paediatric cardiologist, usually but not always on a defined accredited training scheme.
Workplace-based assessments assess a trainee’s professional skills and attitude and provide evidence of appropriate everyday clinical competences. Reference Martin, Blissett and Johnston25 It has high content validity through assessing actual performance in the workplace. Workplace-based assessments are promoted as an integral part of curriculum design and educational planning, in which teaching, learning, assessment, and feedback are closely integrated. Workplace-based assessments include the following:
Multisource feedback (MSF) is a method of obtaining feedback in a structured form from staff associated with the trainee who have the opportunity to observe their practice. Reference Brinkman, Geraghty and Lanphear26
Summative feedback is provided at the end of the learning process and serves to provide trainees with an overall assessment of their learning, often with an associated grade.
Formative feedback typically contains ungraded or low-stakes opportunities to measure trainee knowledge and skills. Formative feedback is ongoing and helps trainers to focus on trainee learning and trainees to better understand the limits of their own knowledge and how to improve.
Entrustable Professional Activities are key tasks of a speciality or subspeciality, that a trainee can be trusted to perform, once sufficient competence has been demonstrated. Reference Ten Cate, Chen, Hoff, Peters, Bok and van der Schaaf27–Reference Ten Cate and Schumacher29
Methods and materials
In October 2023, an approved and structured questionnaire was designed to ascertain the training of trainers in European training centres. The structured questionnaire was initially designed by one member of Association for European Paediatric and Congenital Cardiology Educational Committee with specific expertise on postgraduate education, based on previously peer-reviewed and published surveys. The survey was approved by the Association for European Paediatric and Congenital Cardiology Educational Committee members. All eight members of the Educational Committee edited and validated the questionnaire. Once approved by the Children’s Health Ireland Educational Committee (CHI/GEN/823), the questionnaire was submitted to the Association for European Paediatric and Congenital Cardiology Council for their validation and approval. Informed consent was obtained from all participants to participate in the study.
The questionnaire, composed of 47 items (Appendix 1), was circulated to all recorded training centres registered with the Association for European Paediatric and Congenital Cardiology (https://www.surveymonkey.com/r/DB7VSZB). We requested that the survey be completed, when possible, by either a training director or one of the cardiologists actively involved in training and/or assessment of paediatric and congenital cardiology trainees/fellows. The questionnaire detailed the number of training programmes, the number of general congenital cardiology fellows (or trainees), teaching design, breakdown in training, assessment techniques, reviews and feedback. Open-ended questions searched for strengths and weaknesses of the programme in addition to challenges faced by trainers. More detailed questions determined which instructional techniques are used and how often they assess trainees. The survey also sought to understand the satisfaction level of the trainers with their performance as a trainer, how they maintain continued competency as a trainer, and how they evaluate their training programme. The last part of the survey addressed what the Association for European Paediatric and Congenital Cardiology could do to support the ongoing activity of the trainers. Consent was obtained from Children’s Health Ireland, Crumlin, Dublin, Ireland to conduct the study. Participants in the survey consented to participate in the study. There were no patients involved in this study.
Questionnaire circulation
The survey was then circulated via email to the head of each training centre or a responsible trainer in all 95 Association for European Paediatric and Congenital Cardiology-affiliated training centres, and failing a response, a repeat email was circulated one month later. After a period of 4 months and multiple efforts to enrol centres, the training centre and trainer were deemed uncontactable.
Results
Complete data was provided by 46 trainers from 46 centres in 20 countries (Figure 1). Thirty-three trainers (72%) were the head of training for their centre and/or head/lead in education in their department, and 14 (30%) described themselves as paediatric cardiologists who provide education at their centre. The median number of trainers in each centre was 6 (range 1–16). The median number of years trainers were in a training role was 20 years (range 2–32 years). The median number of fellows per training centre was 6 (range 1–25).
Location of trainers from paediatric cardiology centres across 20 european countries who participated in the study.

Training received by trainers
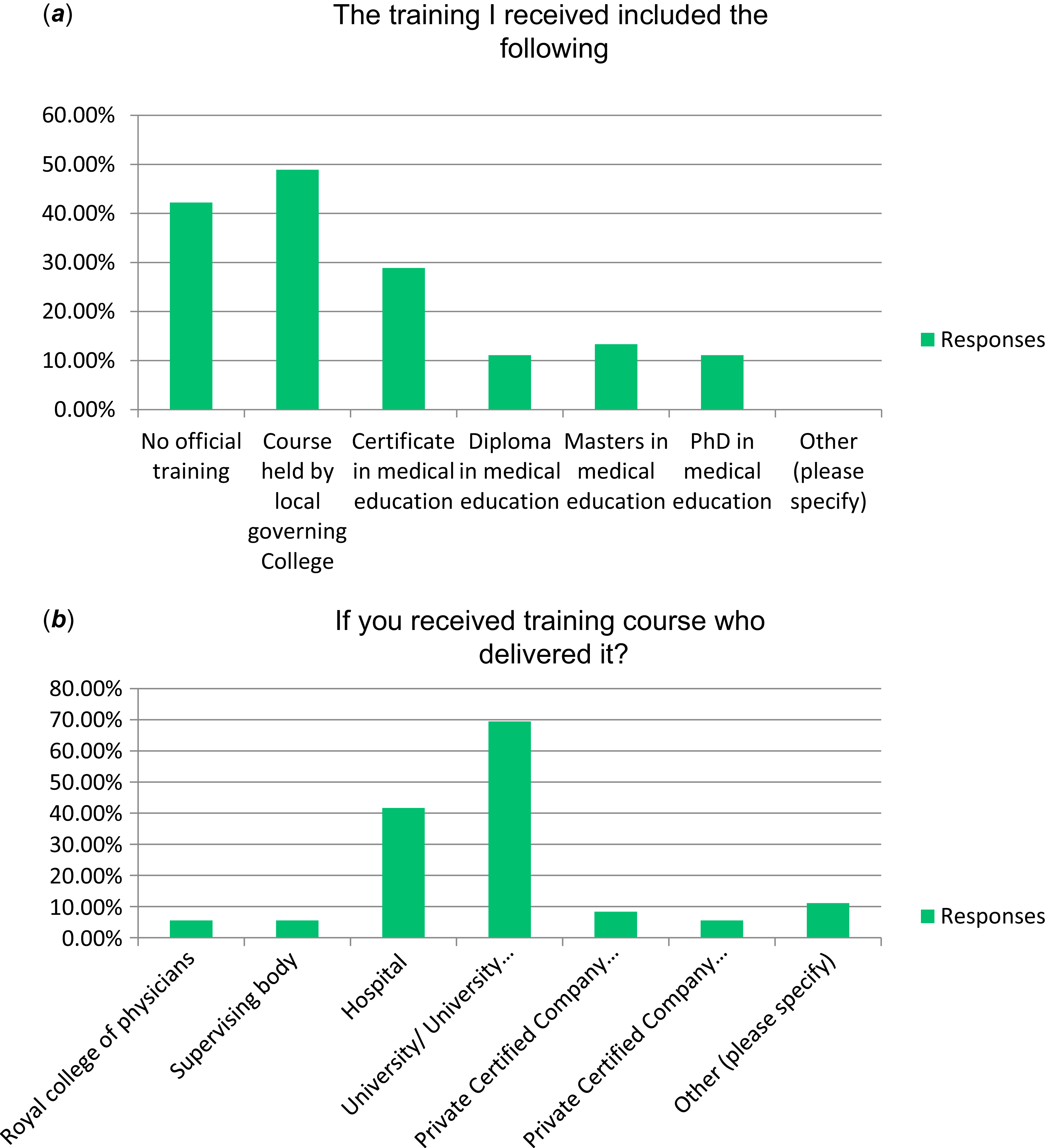
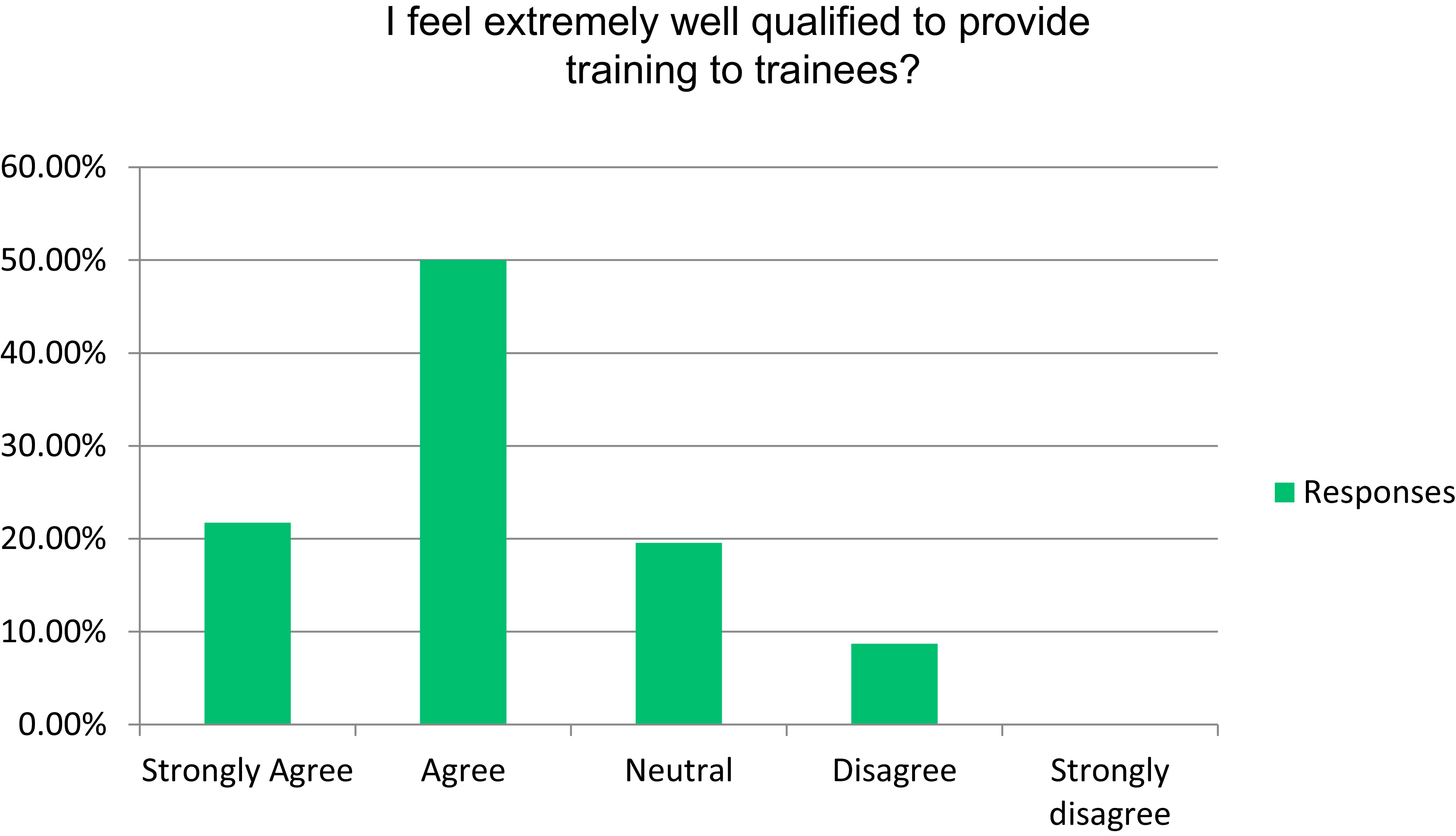
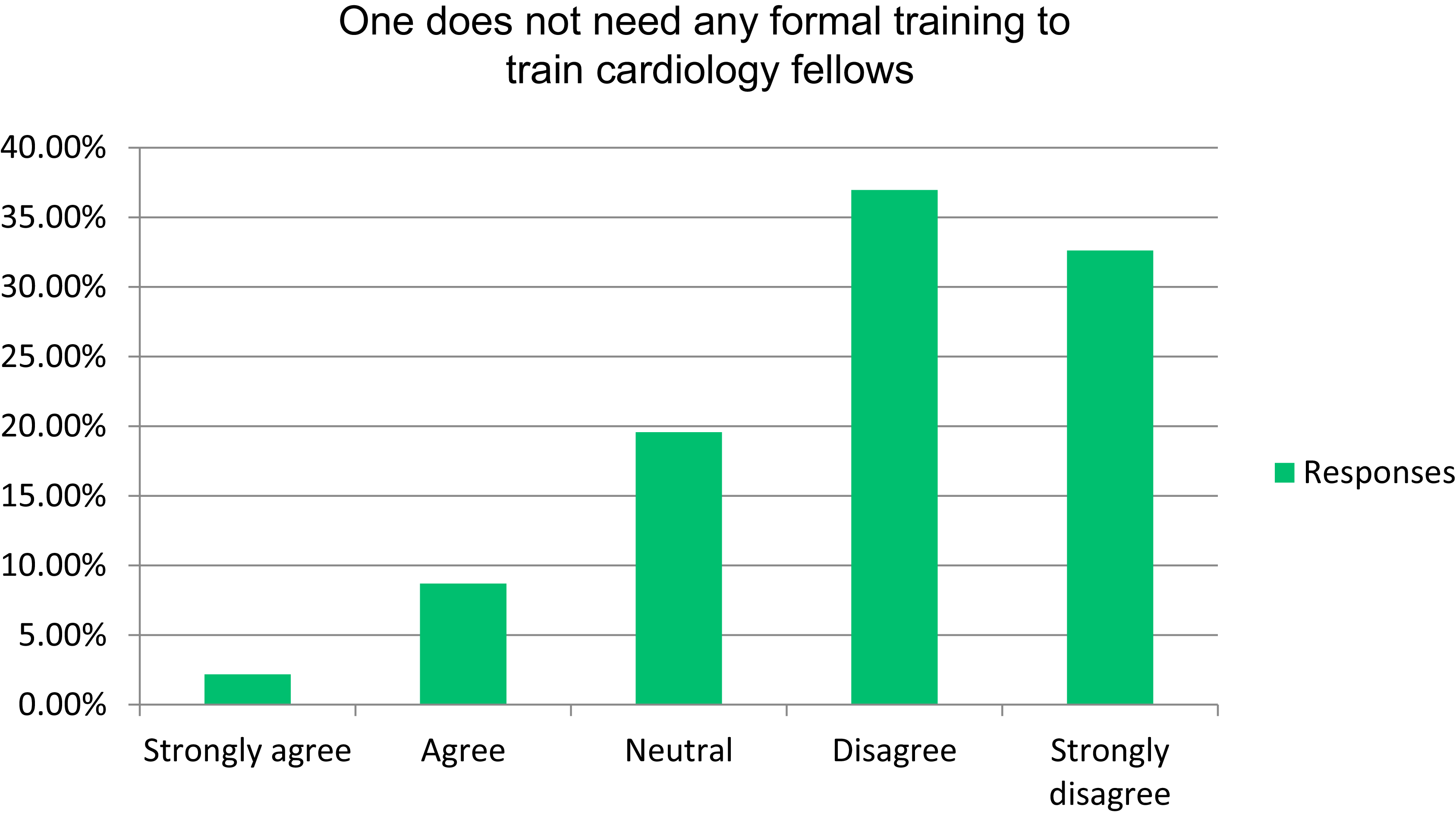
Thirty-one trainers (67%) received some training in being a trainer, and 15 trainers (33%) reported receiving no training. There was a wide range of training received most commonly as a course by a local governing college for 22 trainers (47%), a certificate in medical education for 13 trainers (28%), a Diploma for 5 (11%), Masters in Medical Education for 6 (13%), and PhD in Medical Education for 5 trainers (11%). Training was provided by a university for 25 trainers (54%), a local hospital for 15 trainers (33%), a private certified education company for 3 trainers (7%), and the Royal College of Physicians, supervising body or self-sought private education centre for 2 trainers each (4%) (Figure 2 (a) and (b)). Thirty trainers (65%) believed this training made them better trainers (Figure 3). Thirty-three trainers (72%) believed themselves to be well qualified to train. Furthermore, 33 trainers (72%) disagreed or strongly disagreed with the statement “one does not need any formal training to train cardiology trainees” (Figure 4).
( a ) and ( b ) Type and source of training received by trainers across Europe.

Trainer self-perception of their qualifications to train.

Trainer perception of need for formal training.

Instructional techniques and assessment tools
Taking the patient´s history and clinical investigation are important skills to be covered in the training of fellows. All trainers believe the history and physical examination to be a critical part of investigating the patient: 86% strongly agree, and 14% agree. Forty-five trainers (98%) disagreed (76% strongly disagreed, 22% disagreed) with the statement that “the history and physical examination are made redundant in the presence of imaging technology (echocardiography, MRI or cardiac catheterisation)”.
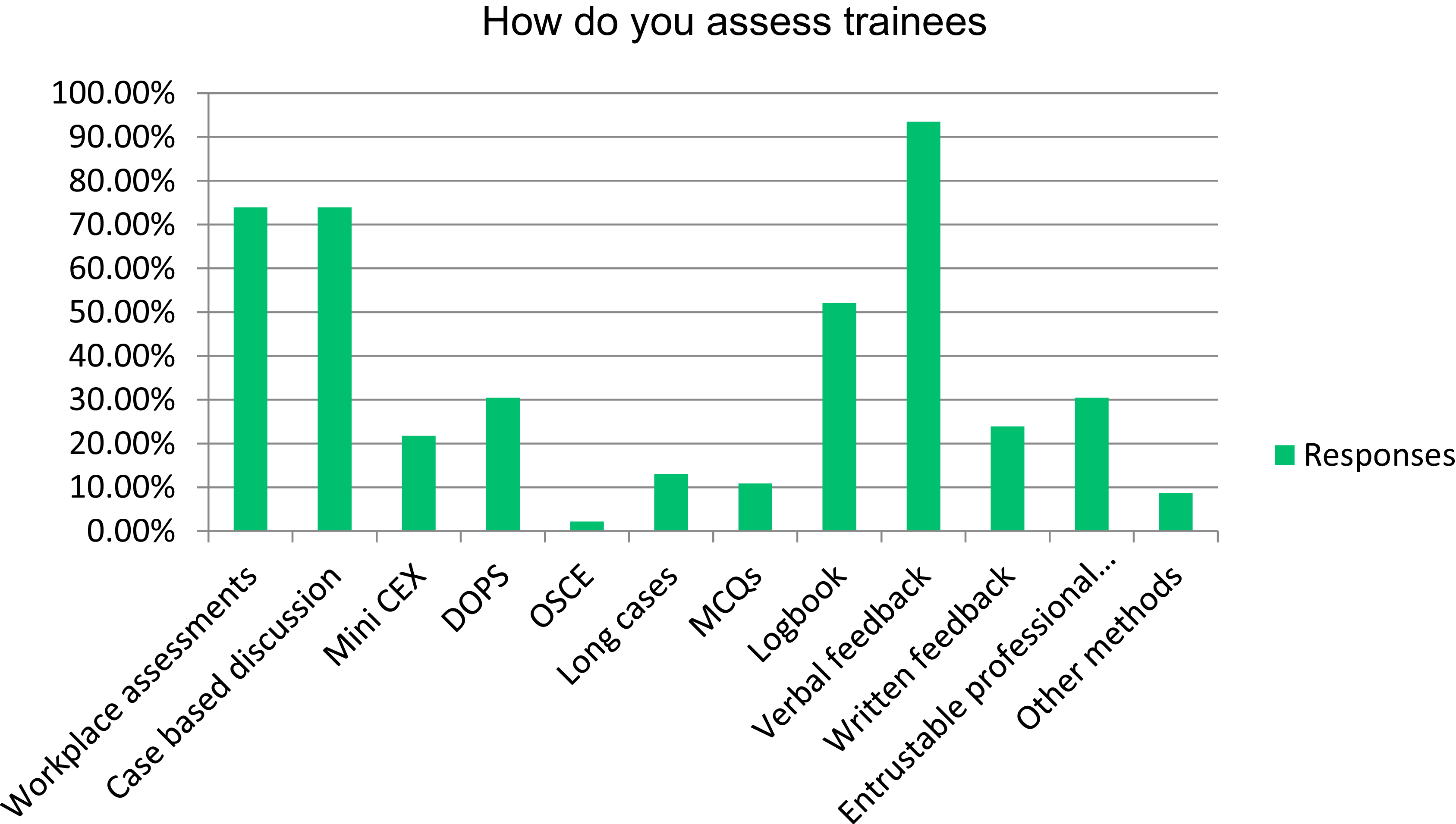
Assessment of trainees varies from daily to monthly between centres: in 17 cases (37%), the assessment was done every 6 or 12 months. Assessment tools used by trainers are shown in Figure 5.
Assessment tools employed by trainers.

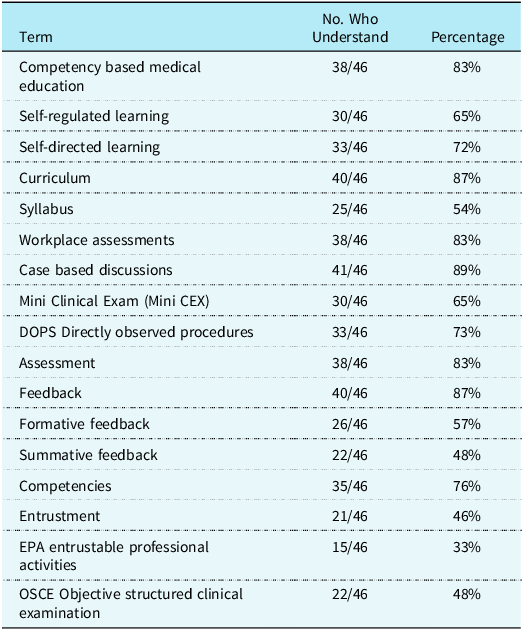
Trainer comprehension of different educational instruments and terms varied significantly and is provided in Table 1. Workplace assessments are used by 42 trainers (91%) as the most common type of assessment. Case-based discussions are used by 42 trainers (91%), mini-clinical evaluation exercise (mini-CEX) by 14 (30%) and directly observed procedures by 42 trainers (91%). Objective structured clinical examinations were used by 13 trainers (28%).
Comprehension of educational terms and instructional techniques among 46 trainers from 20 european countries

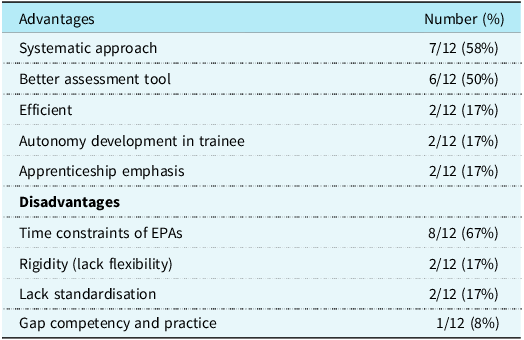
Entrustable professional activities were used in 12 training programmes (26%). Nine of these 12 centres (75%) used entrustable professional activities across all subspeciality areas (clinical examination, imaging, catheterisation, electrophysiology, and intensive care), while they were used in selective subspecialities (imaging or catheterisation) in 3 of 12 centres (25%). Eight of 12 centres (67%) which use entrustable professional activities reported the significant time component spent completing them as a major challenge. The advantages and disadvantages of entrustable professional activities are presented in Table 2. The benefits of entrustable professional activities were clearly outlined by trainers:
“With EPAs it is more clear for a fellow what tasks and activities should be accomplished individually in order to perform certain activities without supervision.”
Furthermore, the clarification on readiness to progress was highlighted in addition to the apprenticeship style of training:
“Much clearer for the assessors and aids assessment of suitability for progression. Emphasises the apprenticeship aspects of training.”
Time constraints on trainers to complete entrustable professional activities was by far the greatest disadvantage:
“Time consuming and administrative additional workload.”
Advantages and disadvantages of entrustable professional activities expressed by 12 trainers currently using EPAs

Data presented as number of trainers (% of total using EPAs).
Our data showed that increasingly trainers are adopting their use, with eleven trainers (31%) in the process of implementing entrustable professional activities into their assessment portfolio.
Trainer feedback to trainees
Feedback was provided by 45 trainers (98%) to their trainees, most commonly formative feedback. Frequency of formalised feedback was monthly in 12 centres (26%), quarterly in 11 centres (24%), every 6 months in 9 centres (20%), and annually in 8 centres (17%). Many centres provide daily in the moment feedback on performance of diagnostic imaging or interventional procedures.
Trainer perceived weaknesses of training programmes
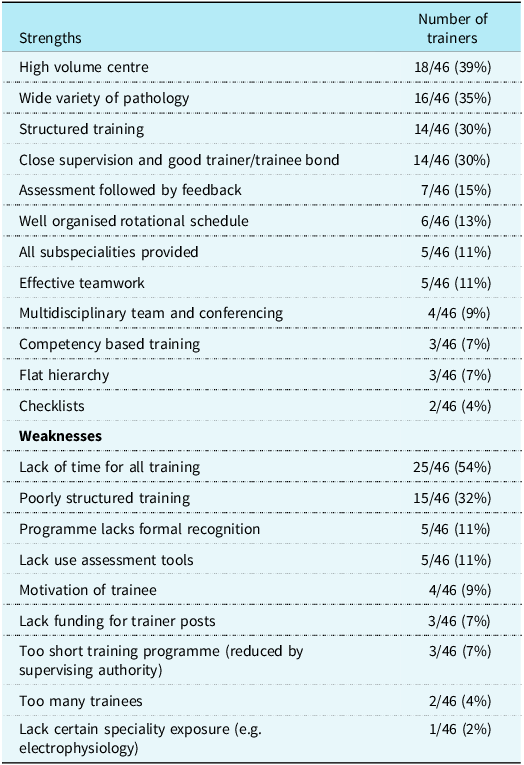
Strengths and weaknesses expressed by trainers are presented in Table 3. Lack of time to provide training was reported as the greatest challenge by 54% of trainers. The majority of trainers expressed a need for formal “training the trainers” courses and development of standards in training. Some of the open-ended responses from trainers included challenges with time constraints
“As a trainer to find the right level and to find time. As head of the department, to encourage all trainers to invest time in teaching”
Motivation was expressed as a challenge in
“getting enough trainees interested in the field of paediatric and congenital cardiology.”
Dealing with the marked variation in trainee aptitude and knowledge:
“to be open for new knowledge and techniques - often presented and picked up by the trainee. You need to be humble supportive when the trainee grows to a level above your own”.
At the other part of the spectrum:
“trainees with slow progress and handling the conflicts is not something that comes easy.”
Furthermore, lack of formal recognition of paediatric and congenital cardiology as a subspeciality was voiced as a problem by several trainers:
“Major challenge to obtain from our regulatory authorities an official recognition of our specialty”.
Trainer perceived strengths and weaknesses of their training programmes

Data presented as number of trainers (%).
Trainer perceived strengths of training programmes
It is important to point out that many centres are excelling in training:
“High volume centres allowing vast clinical experience. There is a lot of multidisciplinary discussion with educational feedback. Regular formal internal training events. Simulation based events. Close follow up of fellows improvements.”
Reciprocity of benefit between trainer and trainee was a well-recognised strength:
“Our strength is our interactions with our fellows and the motto that training is a bidirectional thing where both trainers and trainees benefit.”
Several centres reported a very safe and fostering culture to allow trainees flourish in their training programme:
“Checklist with clear aims of the training program. Secure employment and social security for the trainee. Trainee and trainers (consultants) work close together, low level of hierarchy but with respect for one another’s situation, good environment and resources in providing patient care.”
Time allocation and trainer recognition
Twenty-five trainers (54%) stated they had inadequate time for training trainees (Table 3). Twenty-three trainers (50%) disagreed or were neutral when asked whether they had dedicated time apportioned for training during the week. When asked whether their institution recognised (administratively, dedicated time allocation or financially) their work as a trainer, there was a wide variation in responses with 20 trainers agreeing (43%), 10 neutral (22%), and 16 disagreeing (35%). When asked whether their peers recognised their training efforts, 41 trainers (89%) agreed or were neutral in their response. Thirty-nine trainers (85%) reported their trainees recognised their efforts in training.
Continuous professional development as a trainer
Twenty-seven trainers (59%) attended courses or workshops for education in the preceding 18 months. Twenty-two trainers (48%) attended educational conferences or seminars. Seven (15%) undertook a degree programme in medical education. Twenty-two (48%) participated in individual or collaborative research related to medical education/training. Five (11%) were active in a network specifically for professional development. Eight trainers (17%) visited other training centres. Eleven trainers (24%) received mentoring, peer observation, or coaching training.
Recommendations to improve trainer capacity to train
The following recommendations, in order of frequency, were suggested by trainers:
Structural improvement:
-
• Development of standards of training for trainers, including certification.
-
• Greater formal recognition of training programmes.
-
• Engagement with local or national training authorities/bodies, e.g. SAC in the United Kingdom, to improve trainer education and life-long learning.
Didactic improvement:
-
• Formal in-person training courses for trainers.
-
• Education on training assessment instruments, such as workplace assessments, objective structured clinical examination, and entrustable professional activities.
-
• Webinars and online seminars on training.
Discussion
Trainers have a crucial, albeit underreported, role in educating future paediatric cardiology specialists. This first study of the paediatric and congenital cardiology trainer landscape across European centres affiliated with the Association for European Paediatric and Congenital Cardiology yielded many interesting findings. The wide variation in the number of trainers, disparities in the level of training of trainers, and the variation in support for each trainer were readily evident from the study results. This wide variation in trainer demographics mirrors the wide variation evidenced from recent studies analysing how training is delivered in paediatric and adult CHD across Europe. Reference McMahon, Tretter and Redington1–Reference McMahon, Voges and Jenkins3 These challenges in training are set on a background of rapid developments in medical science, increasing societal expectations and complexity in healthcare environments, including the adoption of artificial intelligence.
The cardiology sections of the European Union of Medical Specialists, the oldest medical organisation in Europe, are tasked with defining European standards of medical education and training. Despite this, there are no reported recommendations on how to train trainers in paediatric cardiology, despite recent extensive efforts to develop a European examination and specialist accreditation in cardiology.
Many other subspecialities have reported their experience with training their trainers. Reference Ukachukwu, Petitt and Usman18–Reference Grant23 In our attempt to sample the current practices in training trainers across Europe, we obtained quite a large participation of current trainers from 20 out of the 28 European countries represented by the Association for European Paediatric and Congenital Cardiology. Therefore, we assume that the collected data presents a faithful representation of the education of the European trainers in paediatric and congenital cardiology. While 68% of the participating trainers supported the need for more structured education to become a trainer, only 66% of the trainers received such training courses. When trainers participated in these educational courses, the majority (78%) found them very helpful. These results show that a structured training programme covering the full curriculum would be highly valued by current trainers. In support of this sentiment, the general vision of the Union of Medical Specialists on training is reported as follows:
“The delivery of high-quality training requires highly skilled trainers with the necessary time to deliver a structured programme covering the cardiology core curriculum and to undertake the assessments required to ensure that trainees have satisfactorily completed their training. Trainers should be experienced cardiologists undertaking clinical practice, they should undergo specific training and continuing professional development in educational supervision and assessment, and their role should be recognized by national training authorities.” (https://www.uems.eu)
Even though this is a very ambitious vision, our data demonstrates several challenges for trainers in achieving such goals. These include time constraints, lack of protected time for teaching, and lack of recognition for their role from both national and local training authorities, as well as local peers and colleagues. The dislocation between the reality on the ground for trainers and the lofty ideals espoused by the aspirations of the Union of Medical Specialists’ vision statement, calls for a more formal recognition of the value of being a trainer. Consequently, we would advocate that being a trainer be recognised as a part of a career path and not as an adjunct duty to the daily clinical routine of a busy clinician. Furthermore, the allocation of protected time to train may prevent the invariable trainer burnout and attrition.
Structured teaching for trainers and specific requirements
Although universities increasingly provide excellent degrees and courses in medical professional education (to certificate, Masters and PhD level), it is uncertain whether this is the best way to train trainers. Perhaps more targeted courses specifically focusing on what skills are required as a trainer are what is required. This was supported by 68% of the European trainers in this study recognising the need to further enrich their skills as a trainer. However, one-third did not recognise the requirement to develop any specific competence on the technical aspect of transferring knowledge, skills, and attitude to trainees. This group, which lacked the perception of the value of training trainers, was from a wide range of trainer experiences and from a wide range of programmes. An intervention for this group, on the value of educating trainers may have significant impact on the quality of their training and hence the quality of care provided by graduates to patients with CHD. Despite these sobering results, the majority of trainers expressed a need for formal “training the trainers” courses and development of standards in training. An interprofessional aspect to train the trainers workshop has been reported as very positive by other authors. Reference Koffel and Reidt30
Didactic content for training the trainers
The topic of training the trainers has been addressed by several recent papers.Reference Mustafa, Omar and Alnair 31 One study evaluated the best strategy to disseminate expertise top/down from a European or North American expert/trainer to an African trainer who then can disseminate the knowledge to other local doctors. This refers to the expertise itself and also to the instructional techniques used in training. Experience gained in the field and using measurable feedback methods has proven that teaching a medical discipline is more than just transferring knowledge and practical skills. The trainer must also be taught in teaching and facilitation techniques. Experience carried out in Sudan confirmed that delivering learning and teaching courses to teaching staff has positive effects on the trainers’ ability to have clear and well-stated learning objectives.Reference Mustafa, Omar and Alnair 31 Trainers improved their presentation skills and their use of different teaching methods, which further highlighted the stated learning outcomes and curricula design. By using a wider range of teaching and assessment methods, the students benefited, and their satisfaction was increased.Reference Olayo, Kirigia and Oliwa 32 – Reference Corbett, Mathenge, Zondervan and Astbury 33
There is an even distribution of trainers who have or have not attended educational courses across all parts of Europe, without any difference between Northern, Central, and Mediterranean countries. This reflects a lack of specific requirements to become an educator in paediatric and congenital cardiology all over Europe. This is highly relevant when one takes into account a survey of German trainees in which the majority of trainees themselves agreed on a promising career perspective, but many complained their training was lacking structure (47%) and lacking transparency (37%). Reference Horst, Michel, Kubicki, Lang, Zschirnt and Moosmann34 Nevertheless, the opinion that training a discipline is different from practising a discipline is not shared by all trainers. Seventy per cent of the responders agreed or strongly agreed with the statement that they feel well qualified to provide training to the trainees.
Critical roles of the trainer
Successful training of trainers and trainees requires a systematic approach, structured curriculum, and protected time. Trainers in paediatric congenital cardiology are often facing multiple tasks beyond training. They serve as a doctor for the sick child, take responsibility as a training director or teacher, undertake research to advance the speciality, and are advocates for the subspeciality. Time constraints in providing training were reported by > 50% of trainers as the greatest challenge in providing training. Given the limited amount of time, the definition of goals for educating the specialist is essential. Therefore, the most important tasks of a good trainer are the implementation of innovations, the assumption of responsibility and the setting of an exemplary attitude. A successful trainer may take the task to transmit a broader vision and goals of the subspeciality rather than assigning the trainees tasks and work.
Trainers should also be aware of themselves as role models for trainees. Jochemsen-van der Leeuw et.al. categorised the roles of medical teachers in patient care qualities, teaching qualities, and personal qualities. Reference Jochemsen-van der Leeuw, Wieringa-de Waard and van Dijk35 Excellent clinicians who were investing in the doctor-patient relationship were identified as positive role models. They inspired and taught trainees while carrying out other tasks, were patient, and had integrity. These identified attributes may help trainers to recognise which aspects of their clinical professional behaviour might be important for trainees in the process of learning professional competencies through observation. Attributes associated with trainers have been summarised for surgical trainers: “character” (approachability, patience, enthusiasm, encouraging/supportiveness), “procedural” (willingness to let trainee operate, balance between supervision and independence), “teamwork and communication” (sets educational aims and objectives, ability to use appropriate feedback, communication skills, and time availability to train) and “clinical” (capable, good relationships with patients, and the health care team). If these key attributes are valuable and have a positive effect on the training of trainees, they would need effective further evaluation before including these topics in teaching courses for trainers.Reference Jochemsen-van der Leeuw, Wieringa-de Waard and van Dijk 35
Assessment of trainees
The prior long-standing teaching method of “See one, do one, teach one” is not adequate anymore from the didactic point of view. The trainer is expected to give teaching, followed by assessment and feedback. An important point raised by the survey is the disparity of the assessment techniques adopted throughout Europe. In all centres, trainees are assessed during their training while the instruments employed vary widely (Figure 5). Workplace assessments have been identified as mostly used (> 90% trainers) with a mix of summative and formative feedback as the most common type of assessment. The timing of the assessment varies from daily to monthly to biannually and annually. Although entrustable professional activities have been proven to be an effective way to evaluate trainees and foster responsibility according to their level of autonomy, knowledge of entrustable professional activities is limited amongst trainers. Furthermore, they are seldom adopted as they are perceived to be time-consuming and not really of value. The Association for European Paediatric and Congenital Cardiology Educational Committee is confident that entrustable professional activities will become a more widely adopted method of evaluation of trainees in the near future. Changing the training paradigm from a time-based to competency-based is an important step forward towards improving the standard of training across European countries.
Feedback to trainees
Feedback is provided by the majority of trainers, most commonly in verbal form. Considering that assessment is a fundamental component of education and an important driver of learning, a formal and possibly written feedback by the mentor evokes an emotional response by the trainee, which goes well beyond the assessment itself, being a powerful contribution to the process of the professional growth of the trainee. On the other hand, assessment and feedback require motivated and skilled assessors and represent a further workload.
Vision on the role of trainers
The relationship of trainers with their trainees is to transmit knowledge and experience while leaving space for innovation. The trainer–trainee relationship should allow trust and respect from both sides. The trainer should be a mentor, not a judge. This core vision of being a trainer is essential to removing obstacles to success. As a mentor, the trainer should allow dedicated time for transmitting professional knowledge, soft skills and supporting the personal development of the trainee. Stimulating career development as well as facilitating the growth of the person are important goals during the training of fellows.
Most importantly, training brings mutual benefits to the trainer and trainee. The trainer also evolves during the trainer process, becoming more self-reflective and more aware of his/her practice. There are two models as a trainer: first as a role model for being a good physician (a caring physician aiming to deliver patient-centred care, a caring colleague and team member, and a good leader) and second as a teacher for clinical discipline-specific skills. The first one is more complex and more difficult to achieve, and is heavily embedded in the culture of the person, institution, and system; the second one requires education and a more structured approach.
To succeed in both approaches requires strongly motivated trainers, given that many of them also have a significant clinical workload. The 3C model is an effective model for trainers to follow. Reference Kehr36 For explicit motives (the head), clearly set goals should be set for trainers, incentives and recognition, and education on the importance of training. For implicit motives (the heart), a positive culture should be adopted in the department/institution, sharing of experiences among trainers, and a way to recognise the effects your training gave. Didactic tools, such as structured training programmes, and teaching to provide feedback are important components of such a model.
It is not only the trainees who ideally should be exposed to different trainers, but also the trainers who should exchange their experiences with each other, to develop in a natural setting, find new motivators and create a culture. It is important to recognise that there is no “gold standard” for a good physician as such. Specific competencies (skills) matter a lot, but typically, there is a balance between different qualities (personal, clinical, etc.). Thus, it is important to be dynamic and self-reflective, always evolving towards becoming a better physician, which also requires different types of interactions, trainer-trainee, trainee-trainer, trainer-trainer, if we look beyond interactions with patients.
Recognising the role of the trainer as one of the essentials for a well-functioning, high-quality healthcare system (i.e. systematic programmes within medical schools to prepare trainers, dedicating protecting time, incentivization, formal and public recognition) is essential to change the paradigm.
Keeping in mind that an important part of the medical profession can be compared with mastering an art, the support of individual talents of trainees and teaching them to master the details of the profession remains extremely important. Despite all structured training and assessment goals, individual human qualities important for interaction with patients and families could be learned from being trained by different individual trainers.
Role of associations and authorities
In the absence of National and European legal requirements to become a trainer in health sciences, the role of Scientific Associations can be very important and should be proactive. The documented interest of Association for European Paediatric and Congenital Cardiology trainers in this topic by replying to the questionnaire reinforces the Association for European Paediatric and Congenital Cardiology Educational Committee and Council’s decision to continue the endeavour of creating a culture of training the trainers at all levels in Europe.
The Association for European Paediatric and Congenital Cardiology could work together with the Union of Medical Specialists and the Council for Specialist European Medical assessment, the oldest and most representative organisations dealing with the standardisation of training in medical specialities, to create guidelines for the education of medical trainers. Minimum requirements to be certified as a competent and updated trainer in Paediatric and Congenital Cardiology could be harmonised at a supra-national level and proposed to the European and National authorities as a standard of education for trainers in medical specialties.
At a basic level, the Association for European Paediatric and Congenital Cardiology is actually creating awareness that training the trainers is an important strategy to deliver a training programme able to prepare excellent specialists who will deliver the best possible care to paediatric and CHD patients. Furthermore, the Association for European Paediatric and Congenital Cardiology can facilitate the education of trainers providing courses, webinars, and in-person meetings. These should focus on theoretical, technical, and practical aspects of the “art” of teaching a medical discipline, stay current on changing requirements and regulations, and allow professional development and networking opportunities.
Conclusion
There is a marked variation in the level of training for trainers from paediatric and congenital cardiology training centres across Europe. They employ a wide mix of assessment tools. Feedback is provided by the majority of trainers, mostly verbal feedback. First, formal recognition of the role as a trainer and, second, supporting a basic training programme for trainers may promote the training skills of such trainers. Greater emphasis on how we educate trainers will hopefully promote a “state of the art” training of our trainees to develop their personal skills (communication, empathy, honesty, integrity), practice the right culture (teamwork, ethics, support) and become excellent adaptive experts (informed by evidence, having the right skills, continuously educating). The Association for European Paediatric and Congenital Cardiology, ESC and EAP could collaborate in such efforts. The tantalising net benefit of these efforts should translate to improved care and better outcomes for our patients with congenital heart disease. Most importantly, greater time provision for training remains a fundamental requirement expressed by several trainers.
Data availability statement
The data underlying this article will be shared on reasonable request to the corresponding author.
Acknowledgements
We thank the Association for European Paediatric and Congenital Cardiology Council for their support in undertaking this project. Ms. Linda Bosschers provided enormous assistance in finalising questionnaires and coordinating the project.
We are grateful to all the trainers and doctors who contributed to this study and especially those, in addition to the authors, for contributing data from their respective centres: Drs. Aphrodite Tzifa, Hakan Wahlander, Birgit Donner, Henrik Brun, Katarina Hanseus, Petru Liuba, Mattias Sigler, Sebastien Hascoet, Jan Sunnegårdh, Jan Janousek, Frances Bu’Lock, María Jesús del Cerro Marin, Nikolaus Haas, Ferran Roses-Noguer, Fernando Rueda Núñez, Marie-Christine Seghaye, Maria Giovanna Russo, Inguana Lubaua, Timur Mese, Nico Blom, Wim Helbing, Anna Kaneva, Chetan Mehta, Marc Gewillig, and Gerald Tulzer.
Financial support
None.
Competing interests
There are none to report.
Ethical standard
Approval of the above study was obtained from the Ethics Department at CHI Children’s Health Ireland, Crumlin, Dublin Ireland (CHI/GEN/823). Survey participants consented to participate in the study.
Consent from patient to publish
Not applicable.


 Open access
Open access