


Introduction
Religion and spirituality are powerful social forces in Africa that inform views of and behaviour towards health, illness, and death (Khorommbi et al., Reference Khorommbi, Masola and Sigida2019; Masola and Sigida, Reference Masola and Sigida2021; Galvin et al., Reference Galvin, Chiwaye and Moolla2023a). Previous studies in Africa have found that health beliefs and help-seeking behaviours are strongly impacted by local religious and cultural formulations (Semenya et al., Reference Semenya, Potgieter and Erasmus2012; Jors et al., Reference Jors, Büssing, Hvidt and Baumann2015; Cooper, Reference Cooper2016). Additionally, medical theories have long contextualised disease within the realms of spiritual and social causation across sub-Saharan Africa (Gyasi et al., Reference Gyasi, Asante, Abass, Yeboah, Adu-Gyamfi and Amoah2016; Opoku et al., Reference Opoku, Manu and Enin Antwi2018).
Research on this subject in sub-Saharan Africa has found that although biomedical explanations for illness and disease have been increasingly accepted over the past centuries, traditional African explanatory models of illness and misfortune remain widespread (Okello and Musisi, Reference Okello and Musisi2015; Falen, Reference Falen2018; van der Zeijst et al., Reference van der Zeijst, Veling, Makhathini, Susser, Burns, Hoek and Susser2021). In particular, bewitchment – imprecations sent by others with the intention to cause harm – is viewed as a common cause of illness as confirmed by many studies in sub-Saharan Africa (Crawford and Lipsedge, Reference Crawford and Lipsedge2004; Edwards, Reference Edwards2011; Sodi et al., Reference Sodi, Mudhovozi, Mashamba, Radzilani-Makatu, Takalani and Mabunda2011; Galvin et al., Reference Galvin, Byansi, Chiwaye, Luvuno and Moolla2023b). In addition to bewitchment, extensive anthropological research in this region of South Africa has also found ritual pollution – when an individual is in a mystically dangerous or marginal state through no fault of his own – to be a particularly significant cause of misfortune when compared with other parts of the country (Hammond-Tooke, Reference Hammond-Tooke1981, Reference Hammond-Tooke1989).
Due to these belief systems surrounding illness and misfortune, many communities in sub-Saharan Africa use traditional healers – or traditional health practitioners (THPs) as they are known in South Africa – instead of, or in addition to, biomedical healthcare services (Sundararajan et al., Reference Sundararajan, Ponticiello, Lee, Strathdee, Muyindike, Nansera and Mwanga-Amumpaire2021). Studies in Limpopo Province, in northern South Africa, have documented how people tend to consult THPs for chronic illnesses (e.g., TB, HIV) or diseases related to ‘social disruption’ (e.g., bewitchment, ritual pollution) (Sodi et al., Reference Sodi, Mudhovozi, Mashamba, Radzilani-Makatu, Takalani and Mabunda2011; Baloyi, Reference Baloyi2014). In particular, this research examines the deep-rooted ideologies with which local populations view the threat of bewitchment and ritual pollution and the ‘spiritual disharmonies’ that they perceive can be resolved by THPs (Nemutandani et al., Reference Nemutandani, Hendricks and Mulaudzi2015). These can also manifest through a variety of ‘traditional illnesses’ that have not been widely studied in the scientific literature (Kriel and Mapogole, Reference Kriel and Mapogole1998; De Villiers and Ledwaba, Reference De Villiers and Ledwaba2003; Galvin et al., Reference Galvin, Coetzee, Leshabana, Masebe, Lebepe, Moolla, Rockers and Evans2025).
Researchers have documented the various types of THPs who operate alongside the biomedical system, including practitioners who work in the African traditional sector, such as diviners (or ‘sangomas’) and herbalists (or ‘inyangas’), and those who practice in the Christian tradition, such as faith healers (or ‘prophets’) (Kahn and Kelly, Reference Kahn and Kelly2001; Peltzer, Reference Peltzer2001; Latif, Reference Latif2010; Khorommbi et al., Reference Khorommbi, Masola and Sigida2019). Yet, these categories can be malleable, as several studies have documented how sangomas almost always use herbs, and inyangas frequently perform divination (prophecy or fortune telling), and therefore both often identify collectively as ‘sangomas’, the term used in this study (Sodi et al., Reference Sodi, Mudhovozi, Mashamba, Radzilani-Makatu, Takalani and Mabunda2011; Galvin et al., Reference Galvin, Chiwaye and Moolla2023c).
Studies in South Africa, including in Limpopo Province, have identified prophets as diagnosing illness by putting a hand on the Bible, praying, and lighting a candle, and treating illness by praying, providing holy water or ash, and laying hands on a patient (Kahn and Kelly, Reference Kahn and Kelly2001; Sorsdahl et al., Reference Sorsdahl, Flisher, Wilson and Stein2010; Sodi et al., Reference Sodi, Mudhovozi, Mashamba, Radzilani-Makatu, Takalani and Mabunda2011). Yet, other studies have found prophets to blend traditional African practices and those of Christianity in their healing rituals, such as by using herbs or animal sacrifice to treat patients (Atindanbila and Thompson, Reference Atindanbila and Thompson2011; Galvin et al., Reference Galvin, Chiwaye and Moolla2023a). More research is, therefore, needed to understand exactly how local populations view this relatively new, and often syncretic, addition to the THP category (Pondani, Reference Pondani2019).
Furthermore, despite their widespread use throughout South Africa, including Limpopo Province, THPs have largely been ignored by policymakers, and additional research is needed to determine exactly how local populations conceptualise distinctions between these two forms of THPs: sangomas and prophets. By better understanding local explanatory models for illness, as well as patient experiences with different THPs, healthcare professionals can create more person-centred approaches to care. Considering the substantial utilisation of THPs alongside the prevalent embrace of Christianity in southern Africa, dimensions of spiritual practice cannot be overlooked in consideration of any aspect of human health.
Methods
Study background, sampling, procedures, and measures were described in previous publications (Galvin et al., Reference Galvin, Coetzee, Leshabana, Masebe, Lebepe, Moolla, Tarullo, Rockers and Evans2024; Galvin et al., Reference Galvin, Coetzee, Leshabana, Masebe, Lebepe, Moolla, Rockers and Evans2025). This was a cross-sectional qualitative study, nested in a larger study called The Developing Belief Network (DBN) Study, which is conducting research across 16 countries and 50 distinct cultural-religious settings (Weisman et al., Reference Weisman, Ghossainy, Williams, Payir, Lesage and Reyes-Jaquez2023). The data collected for this particular study were part of research conducted in Tzaneen, Limpopo Province, South Africa, in 2022. The main goal of the DBN study is to document cultural influence on children’s (a) attainment and construction of religious knowledge or behaviours and (b) conveyance of this religious knowledge and these practices to other individuals. Other questions the DBN study sought to answer include (1) How does the acquisition of religious cognition and behaviour vary within and between populations? and (2) How do processes of social learning support the development of religious cognition and behaviour?
The DBN study employed a snowball sampling strategy in which the Tzaneen-based study team worked with community health workers (CHWs) at six local primary healthcare (PHC) facilities that were participating in the study to identify eligible participants. Tzaneen is a mid-sized town in the hills of the Limpopo province in northern South Africa. Then, the study team asked enrolled participants if they knew of anyone else who would be interested in taking part in the study. If yes, the study team obtained contact details and contacted the potential study participants to assess if they were eligible and willing to participate in the qualitative interviews. Those eligible and willing were invited to participate and attend a scheduled study visit at the study office in Tzaneen.
Participants were included in this study if they were: (1) caregivers of children between 4–10 years of age; (2) 18 years or older; and (3) fluent in Xitsonga and Sepedi. It is important to note that these eligibility criteria were for the larger DBN study, and caregivers were co-enrolled for the main DBN study and this sub-study. The interviews for both were combined, and therefore, participants were interviewed on a single occasion, saving time and resources for participants and the study team. The sample for this analysis was, therefore, a convenience sample of participants enrolled in the main DBN study. As these participants were taken from the larger DBN study and since women are generally the primary caregivers across cultures, all participants were women.
Study visits were conducted at a private study office in Tzaneen, and participants were provided transportation to and from their homes. On the day of their visit, respondents who were invited to participate in the study spoke with a member of the study team who explained the study and obtained written informed consent. Participants were asked to sign a study consent form as well as an audio consent form so that the interview could be recorded and later transcribed and translated. All communication and study documents were conducted in local languages (English, Xitsonga, and Sepedi) by a local study team trained in all study procedures, including participant confidentiality and informed consent.
Interviews took roughly 45 minutes to complete. Participants received a small reimbursement (R150 or roughly $10 USD) to compensate them for their time and any out-of-pocket expenses they may have incurred. They were also provided with refreshments during the visit.
Participants were asked about their age, monthly household income, employment status, education level, ethnic group, religious affiliation, marital status, and number of children. Participants were also asked about their experiences with receiving treatment from THPs, such as sangomas and prophets. Sangomas were referred to as ‘N’aka’ in Sepedi and ‘N’anga’ in Xitsonga. Prophets were referred to as ‘Moporofeta’ in Sepedi and ‘Muporofeta’ in Xitsonga. The questionnaire was originally developed in English, and all translations into Sepedi and Xitsonga were culturally validated by team members prior to incorporation into the questionnaire. Wording was maintained consistently across participants, and assessors asked semi-structured follow-up questions as needed. All interviews were audio recorded and transcribed. Three study enumerators reviewed all transcripts and translated them into English. The analysis utilised a directed content analysis method that combined deductive and inductive aspects of code development (Hsieh and Shannon, Reference Hsieh and Shannon2005). Themes were developed and refined by the three study enumerators and study PI (MG), resulting in a final set of codes. Data were analysed using NVivo software. The survey data were collected and stored in REDCap, an electronic data capture tool hosted by the University of the Witwatersrand, in order to maintain confidentiality.
The study was approved by the Human Ethics Research Committee (Medical) at the University of the Witwatersrand, Johannesburg (Clearance number: M210914). All participants provided written informed consent to participate in the study and for their interview to be audio recorded.
Results
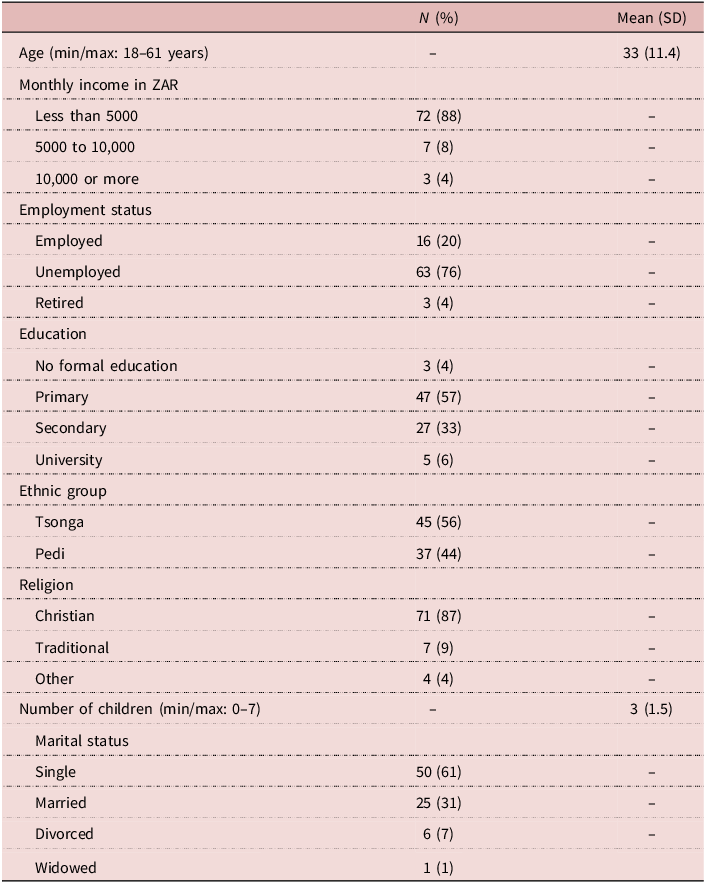
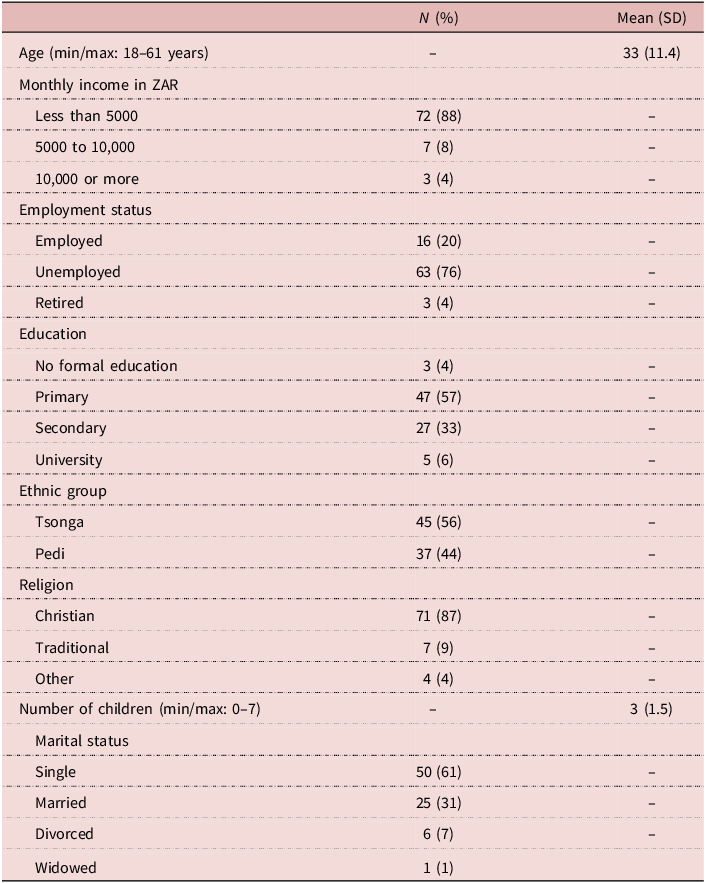
This study examined a population of rural women living near the city of Tzaneen. Eighty-two (n = 82) individuals completed the study interview and were, therefore, included for this analysis. Participants were aged between 18 and 61 years, as seen in Table 1. The population of this study was mostly poor, with 88% making a household income of less than 5000 ZAR (roughly $275) per month, and only 20% were employed – though many participants had husbands who were employed. Over 60% of the sample had only a primary education or less. The sample was relatively evenly split between the Tsonga and Pedi ethnic groups. Eighty-seven percent (87%) identified as Christian, while 9% identified as practicing Traditional African religion, and 4% identified as other. This is similar to the results from the 2016 community survey for Limpopo, which found 74.1% to be Christian and 5.5% identified with Traditional African religion (Stats SA, Reference Stats2016).
Sample characteristics (n = 82)
Belief in bewitchment as a cause of illness
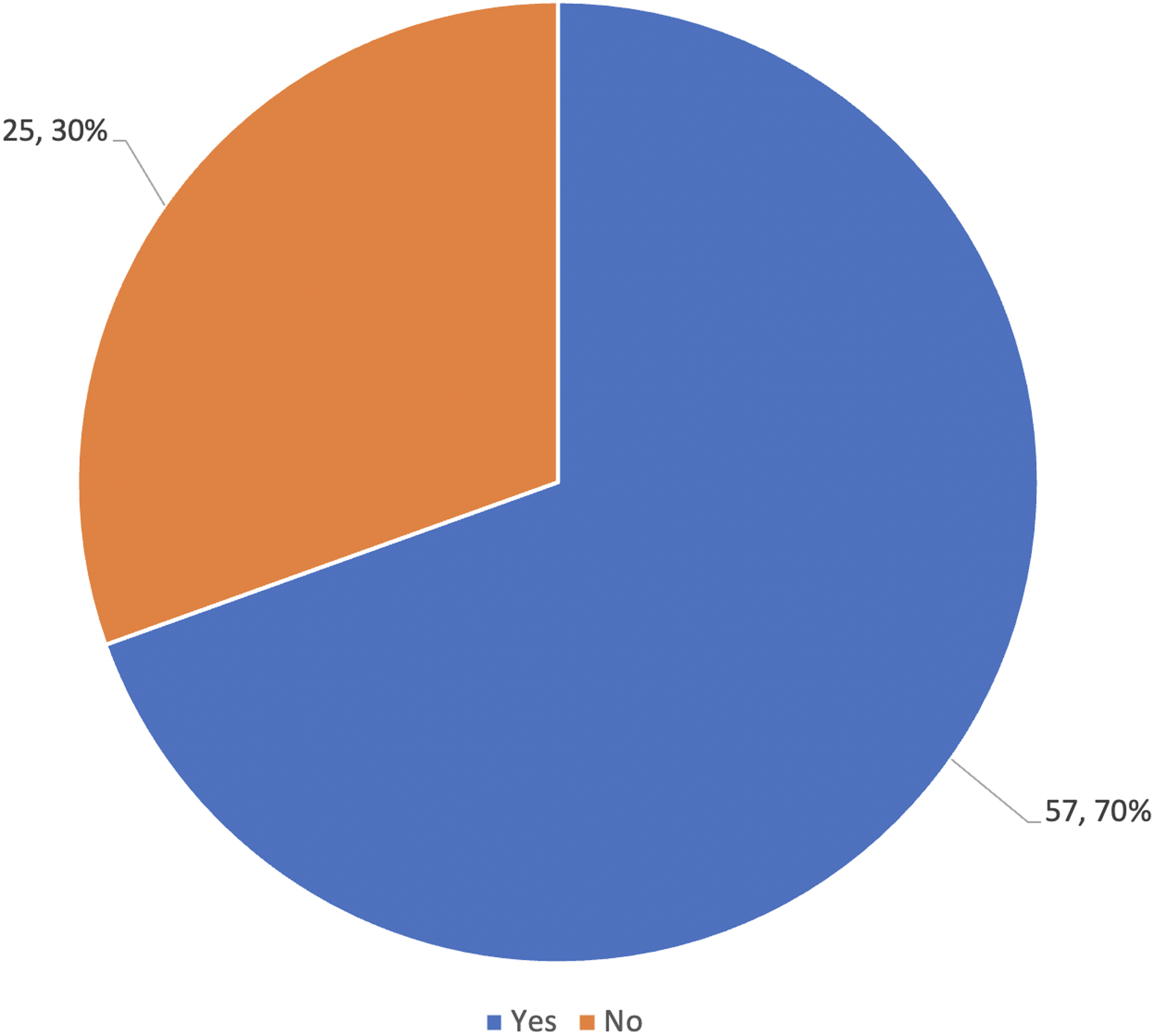
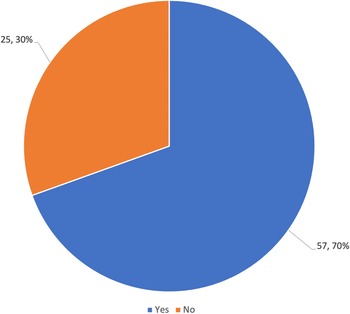
This study examined the perceptions of 82 women regarding beliefs about the spiritual causation of illness and the ability of THPs to cure illness. As seen in Figure 1, 68% (56/82) of respondents believe that bewitchment can be a cause of illness, whereas the remainder (26/82) did not believe bewitchment can be a cause of illness. There were no significant differences between those who believed in bewitchment and those who did not based on demographic characteristics.
Do you believe people can send illness onto others using bewitchment?

As one participant reported, ‘many people are sick because they have been bewitched by other people’ (Participant 38). Illnesses related to bewitchment are often referred to as illnesses that are ‘created by people’ or ‘people’s doings’ (Participant 42). This differentiates them from so-called ‘natural illnesses’, which are not related to witchcraft.
Participants also describe illnesses due to bewitchment as being sent by other people. As one respondent described, ‘they [person doing the bewitching] can send me an illness’ (Participant 67).
Several participants reported loved ones dying due to illnesses caused by bewitchment. As one recounted, ‘my husband was infected by bewitchment and couldn’t get help, then he ended up dying’ (Participant 31).
Pathways to care
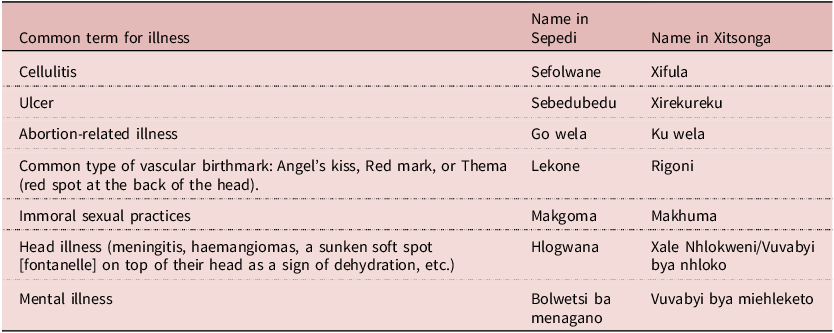
Illnesses that are caused by bewitchment or other spiritual or traditional causes are often surrounded by mystery and considered forbidden to be spoken about; thus, it can be difficult for participants to discuss. ‘Some types of illnesses are too taboo to even talk about’, one respondent reported (Participant 20). Illnesses that were identified as traditional in origin can be viewed in Table 2.
Traditional or spiritual illnesses identified by participants
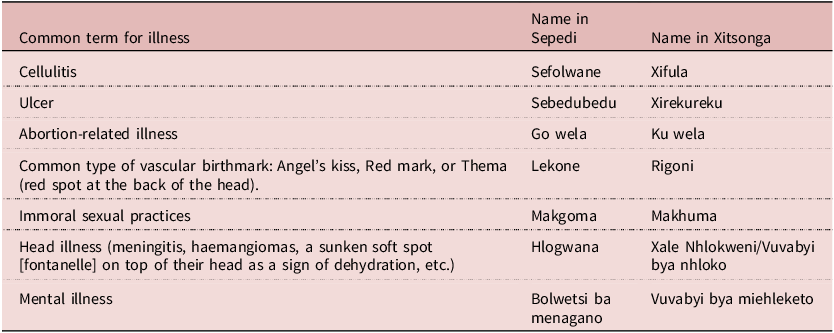
A condition referred to as ‘cellulitis’ – or ‘Xifula’ in Xitsonga and ‘Sefolwane’ in Sepedi languages – was the most commonly cited traditional illness; however, it is important to distinguish this from the common bacterial skin infection easily treated with antibiotics. Cellulitis was identified by 8 participants and described as a condition that could only be fully cured by traditional healers. As one said, ‘I was once bewitched with cellulitis (sefolwane) and I got help at the church [from a prophet]… when I went to the clinic, it didn’t help, but when I went to church and they prayed for me, I became okay’ (Participant 35). As another respondent described, ‘with cellulitis doctors can’t cure it. It requires traditional medicine’ (Participant 81).
Following cellulitis, five participants identified an abortion-related illness commonly referred to as ‘go wela’. One described it as, ‘when they say a man has had sex with a woman who had an abortion’, the man goes on to suffer illness, which manifests in a range of symptoms and can lead to his death (Participant 36). Symptoms were reported to include headaches and pain around the genital region. Traditional illnesses such as these are described as ones that ‘can’t be cured by doctors’ (Participant 24). As another remarked, ‘there are those [illnesses] that can be cured in a Western way, and there are those which can be cured in a traditional way’ (Participant 28).
Several respondents described how even illnesses such as tuberculosis (TB) and HIV can be treated either traditionally or with Western medicine. As one respondent said, ‘you can have TB and HIV and those can be treated traditionally’ (Participant 29). Six participants mentioned that sexually transmitted infections (STIs) can also be cured traditionally.
Patients often start at the clinic when treating an illness. If doctors are unable to treat or cure the ailment, many people will then consult THPs. One respondent said, ‘you start at the clinic… if they fail you consult healers’ (Participant 25). Another concurred, ‘when I see it’s not working here [at the clinic], I take another route’ (Participant 36).
The hospital/clinic is, therefore, often the first step for many, and its failure is seen as a sign of the spiritual origin of the illness. ‘If it [treatment] fails at hospital then they [the community] will say “oh it means she was bewitched”’ (Participant 10). Others found that when they could not receive help from the hospital or clinic, THPs were then able to intervene successfully, thereby cementing their belief in traditional medicine. ‘What makes me believe [in traditional healing] is when doctors are unable to diagnose and so you find that only traditional healers can cure you’ (Participant 18).
Therefore, when illnesses cannot be treated by Western medicine at the clinic or hospital, THPs must be called in to treat. ‘Doctors may not see some things that traditional healers see’, one respondent remarked (Participant 77). Others also claimed that spiritual illnesses caused by bewitchment can be combatted in other ways: ‘Witchcraft can be defeated by prayer’ (Participant 43). Belief is key, however, as faith cannot only fight off illness caused by bewitchment but can also prevent one from being vulnerable to supernatural attacks. As one respondent claims, ‘It [bewitchment] can happen but I do not believe it can affect me; it can occur to people who don’t have faith’ (Participant 6).
Use of different types of healers
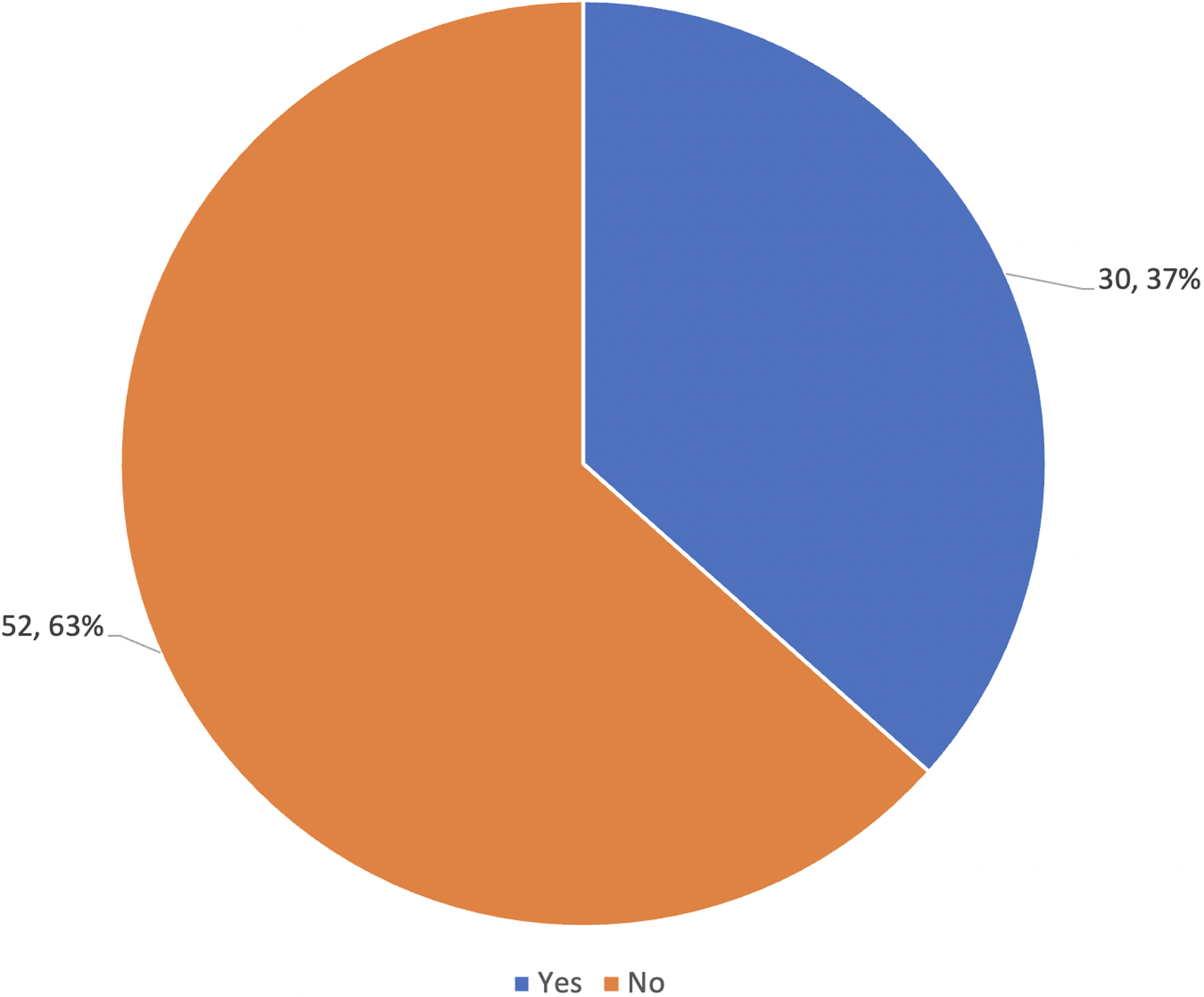
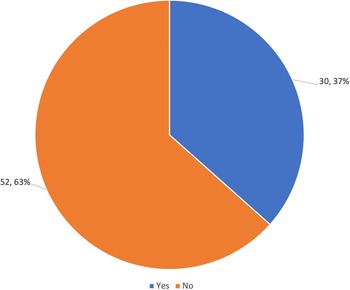
Among the 82 women interviewed, 70% (57/82) reported that sangomas can heal illnesses that doctors cannot, as seen in Figure 2. While a lesser proportion (37%; 30/82) reported that prophets can heal illnesses that doctors cannot, as seen in Figure 3.
Do you believe that sangomas can heal certain illnesses that doctors cannot heal?
Do you believe that Prophets can heal certain illnesses that doctors cannot heal?
Many participants, therefore, believe that sangomas can heal illnesses that are supernatural in origin. While smaller in number, many participants also believe that prophets can heal them using Christian healing. Participants, therefore, go where they believe they can get help. This is often part of a ‘negotiation’ as described by one participant: ‘you can negotiate with the ancestors, but because I’m a Christian, they [ancestors] negotiated the church way [with prophets]’ (Participant 49).
As described previously, some participants seek help through THPs after unsuccessful treatment at the clinic: ‘I was having a problem breathing, only to find out my lungs weren’t the problem. It was ulcer (xirekureku), and I ended up going to an apostolic prophet who helped me and I became alright. The doctor couldn’t cure me though’ (Participant 74).
However, others similarly fail to receive cures with both the clinic and initial visits to THPs and therefore continue seeking help from different sources: ‘I had something in my stomach, and it grew big. The sangoma couldn’t help me so I went to a prophet, who prayed for me… and laid hands on me. The next morning it [the mass in the stomach] had shrank’ (Participant 6). Prophets, therefore, were often reported to serve in the role of prayer warriors who ‘can pray for you and you will be healed’ (Participant 19).
Yet, there was no universal understanding of who exactly could cure which illnesses and how. As one respondent said, ‘illnesses like cellulitis can only be cured by prophets’ (Participant 3). Yet, other participants said prophets only pray for patients and do not cure them (Participant 23). Others added that prophets do not cure, ‘they just predict what will happen to you in the future’ in the form of fortune tellers (Participant 5). This idea was presented by several respondents, who said prophets can only ‘visualize’ the future for patients and do not cure illnesses (Participant 10).
Additionally, as many participants said that neither sangomas nor prophets could heal illnesses, it is important to highlight those who argue that ‘only doctors are capable of healing’ (Participant 15). As another remarked, ‘You can go to a sangoma and they say you have an ancestral calling, but it’s not; you just need medication’ (Participant 80).
Nevertheless, pathways to care for patients are often complex and involve multiple care providers: ‘I think it is better the Western way. I was once helped by the hospital but was sent there by a sangoma. I had TB. When you go to sangomas they are bound to tell you have an “ancestral calling”. My sangoma said, “she might have the ancestral calling but I think you should take this person to the hospital”. Indeed I got help at the hospital’ (Participant 2).
Therefore, belief is of utmost importance when seeking care and even experiencing relief from symptoms. ‘People are healed by what they believe will cure them’, one respondent said (Participant 13). Another added, ‘It all depends on your faith’ (Participant 82).
Discussion
This study explored the way a population of 82 women in rural Limpopo perceive illness and seek care. It found that bewitchment and other traditional forms of illness are common explanatory models and that many believe THPs are able to heal them from these spiritual afflictions. Furthermore, present results – along with the widespread use of THPs by patients in South Africa – highlight the need for implementation of training regarding the integration of traditional and Western healing practices for medical professionals. A lack of such education and training may unintentionally hinder medical treatment or cause harm to patients.
Bewitchment and religious syncretism
Several other studies in Limpopo province have confirmed the findings of this study, arguing that local traditional culture is key to understanding how people conceptualise their experiences and strongly influences how they seek solutions to their ‘predicaments’ (Mashamaite, Reference Mashamaite2015). Similarly, it is essential to understand the ‘supernatural origins’ that many illnesses are perceived to have, often via the explanatory model of bewitchment (Sehoana, Reference Sehoana2015). Another study in this province argued that locals do not often perceive misfortune or illness as caused by viruses or bacteria, for example, but rather due to the ‘valoyi’ (or ‘witches’ in Xitsonga), a subject described in the findings of this study (Baloyi, Reference Baloyi2014). Additionally, extensive anthropological research has been conducted to determine the relationship between bewitchment-based illnesses versus ritual pollution-based illnesses – often referred to as fiša or ‘heat’ – among the local populations of this region (Hammond-Tooke, Reference Hammond-Tooke1981, Reference Hammond-Tooke1989).
It is important to note that membership in a Christian church does not imply a break with traditional African beliefs, as the current context of African Christianity is often an amalgamation of traditional beliefs and Christianity (Peltzer, Reference Peltzer1999). In this sense, many Christians will also visit THPs to seek protection from bewitchment, and many churches in the region have made demon casting and protection from bewitchment the centre of worship services (Baloyi, Reference Baloyi2014). A study from another part of South Africa found that in a sample of urban black South Africans, 90% were members of Christian churches, and 50% said they had performed traditional rituals and would consult THPs for care (Kahn and Kelly, Reference Kahn and Kelly2001). Even Pentecostals – who have a reputation for demonising traditional African beliefs – have been identified to practice prayer and fasting to protect from bewitchment (Baloyi, Reference Baloyi2014).
This syncretism, combining Christianity and traditional African beliefs, highlights a religious system that is united in its questioning of the effectiveness of the biomedical health paradigm (Sodi, Reference Sodi2009). In this sense, while the biomedical paradigm focuses on what caused the disease, traditional African models focus diagnosis and treatment on who caused the disease (Mzimkulu and Simbayi, Reference Mzimkulu and Simbayi2006). Several studies in Limpopo have reiterated this point, arguing that locals use THPs to understand who caused the illness and may be an important factor in why traditional healing remains so prevalent today (Tlou, Reference Tlou2013; Baloyi, Reference Baloyi2014; Masola and Sigida, Reference Masola and Sigida2021). Added to this fact is that THPs are considered knowledgeable figures, live socially near to their clients, and provide a ‘human touch’, either through prayer or laying of hands, providing hope to the patient that the THPs’ touch will protect them from traditional maladies (Baloyi, Reference Baloyi2014; Masola and Sigida, Reference Masola and Sigida2021). However, very few studies currently exist that examine the traditional illnesses identified in this study, and more research is urgently needed on this subject (Kriel and Mapogole, Reference Kriel and Mapogole1998; Rikhotso, Reference Rikhotso2017).
Types of THPs in Limpopo Province
This study further aimed to explore the experiences participants had with different THPs, notably sangomas and prophets. Similar to other studies on this subject in Limpopo, it found that prophets and sangomas largely share a similar theory on health and disease, although prophets primarily divine through the Christian God, whereas sangomas primarily utilise ancestral spirits (Latif, Reference Latif2010). However, this study also argued that both acknowledge illnesses that can be caused by sorcery or bewitchment, even though customs and practices may differ slightly (Latif, Reference Latif2010).
Similar to the findings of this study, another study from Limpopo, which interviewed local populations, found that prophets were not as popular as sangomas, though some said they would go to prophets for advice (Asbahr, Reference Asbahr2023). This reflects the finding in this study’s sample, in which participants said they viewed prophets more as prayer warriors or fortune tellers rather than healers. On the other hand, the above study also found that sangomas were viewed as secondary care services where patients who did not receive relief from the clinic or hospital could then seek assistance from sangomas, as their ailment may be related to ‘ancestral issues’ (Asbahr, Reference Asbahr2023). These results were significant in confirming the findings of this study.
Even though sangomas have served as THPs in this region for millennia, prophets are relatively a new phenomenon, arising with the widespread acceptance of Christianity in recent centuries (Waruta, Reference Waruta2004). Several studies have identified how, in recent decades, there has been a significant increase in the number of prophets in South Africa, as there are now approximately 12,000 different African Independent Churches (AICs) – which generally host prophets – with a total of 30 million members (Kahn and Kelly, Reference Kahn and Kelly2001; Sorsdahl et al., Reference Sorsdahl, Flisher, Wilson and Stein2010; Khorommbi et al., Reference Khorommbi, Masola and Sigida2019; Kroesbergen, Reference Kroesbergen2019; Pondani, Reference Pondani2019; Asbahr, Reference Asbahr2023). Some studies even argue that prophets have begun to replace sangomas as the ‘favored’ THP, as they can coordinate both Christian and African customary convictions (Waruta, Reference Waruta2004; Baloyi, Reference Baloyi2014; Masola and Sigida, Reference Masola and Sigida2021). More research is, therefore, needed on prophets in particular, to understand their role as healers in this quickly shifting religious and cultural landscape.
As the goal of this study is to explore the relationship between local populations in Limpopo and religio-cultural factors that impact health-seeking behaviours, these findings confirm that THPs play a significant role in the management and treatment of illness in the region. Similar to other studies with comparable results, additional research should explore how collaborations can be created between THPs and biomedical services in the area (Masola and Sigida, Reference Masola and Sigida2021).
Lastly, it is important to identify limitations in this study. Firstly, by using snowball sampling to identify participants in only one rural area of Limpopo Province, this study is not meant to be generalisable to a broader population. Secondly, the study data are solely from the female perspective, as males were not included. Additionally, all participants were caregivers of children between 4–10 years old and had some experience with the health system. The perceptions of women who have never engaged with the health system and have only engaged with THPs, therefore, may be different. Thirdly, as medical history was not part of the eligibility criteria or data collected, everything recounted by participants was based on self-report and was not verified against clinical records. Lastly, as this study was qualitative in nature and was conducted with in-depth interviews, there may be some social desirability bias in terms of participant responses regarding local belief systems and utilisation of THPs. However, it is not clear in which direction this may have impacted the data.
Conclusion
This study sought to explore the perceptions of illness and utilisation of THPs among a population of rural women in Limpopo Province, in the north of South Africa. This study found that local religio-cultural constructs play a significant role in the understanding of illness aetiology and health-seeking behaviours among this population. In particular, participants reported seeking care with THPs, which include both sangomas and prophets. As relatively little research currently exists on the role of THPs in this region – and prophets in particular – this study fills a significant gap in the literature.
Data availability statement
The data that support the findings of this study are available from the corresponding author, MG, upon reasonable request.
Acknowledgements
This study was supported in part by personnel, office space, and resources from the South African field site of a large-scale collaborative research effort by the Developing Belief Network (developingbelief.com), a network of researchers affiliated with a variety of institutions, working in diverse field sites around the world.
Funding statement
The Developing Belief Network is funded by Award #JTF61542 from the John Templeton Foundation.
Competing interests
The authors have no conflicts of interest to declare.
Ethical standard
The study was approved by the Human Ethics Research Committee (Medical) at the University of the Witwatersrand, Johannesburg (Clearance number: M210914).


 Open access
Open access