


Introduction
Disasters, including earthquakes, present substantial challenges to health care systems, especially in areas where all hospitals are profoundly affected by these catastrophic events. On February 6, 2023, a pair of devastating earthquakes with magnitudes of Mw 7.7 in Pazarcik and Mw 7.6 in Elbistan struck the Kahramanmaras and Hatay provinces of Turkey at 04:17 and 13:24 local time, respectively. The earthquake caused severe damage to buildings and infrastructure and resulted in the loss of many lives in a total of 11 provinces. After the Kahramanmaras central earthquake that occurred on February 6, 2023, and the next aftershocks, more than 48,000 people lost their lives, and many more needed urgent medical attention. 1 The 2023 Turkey earthquake resulted in a considerable surge of patients seeking medical attention. With local hospitals damaged and unable to supply sufficient care, patient transportation becomes a critical concern. 1 –Reference Görmeli Kurt, Oğuztürk and Akgün 3
The geographical and socioeconomic characteristics of the affected region further complicated the disaster response. The impacted provinces include both densely populated urban centers and rural areas with limited pre-existing health care infrastructure. Many hospitals in the region were either structurally damaged or overwhelmed, necessitating the rapid redistribution of patients to unaffected regions across the country. This context underscores the importance of coordinated medical evacuation strategies and highlights the critical role of interfacility patient transportation in large-scale earthquakes. 1 , Reference Görmeli Kurt, Oğuztürk and Akgün 3
In the aftermath of major earthquakes, it is impractical for public institutions to transfer all patients either by air or land. While the need for air transportation arises for specific patients, others must rely on self-transportation in situations where all hospitals within the earthquake-stricken area have been demolished, as seen in the case of the Turkey Earthquake.
In the aftermath of major earthquakes, hospitals in affected areas often struggle to accommodate the surge in patients. This situation necessitates the transportation of patients to more distant facilities, utilizing both air and land transport. Some patients also seek care in distant health centers independently. A similar scenario occurred during the 1999 Istanbul earthquake, where patients had to be directed to hospitals in surrounding provinces despite the presence of local hospitals. This global issue emphasizes the need for efficient transportation systems to manage the influx of patients in disaster situations. China, India, Japan, Iran, and Turkey have all faced this challenge after large earthquakes in terms of area.Reference Liu, Liu and Zhang 4 Transportation involves the transfer of patients from the disaster site and subsequently from initial treatment facilities to designated hospitals for acute medical management. Patients who were airlifted from the initial treatment facility to Istanbul Dr. Sadi Konuk Training and Research Hospital were included in the study.
The earthquakes centered in Kahramanmaraş on February 6, 2023, highlighted the critical role of air transportation in disaster management, particularly in terms of patient evacuation. Severe damage to road infrastructure and disruptions in ground transportation made the rapid transfer of injured individuals, elderly people, and those requiring urgent medical care extremely difficult. In this context, large-scale air evacuation operations coordinated by the Directorate General of Civil Aviation prioritized patient transport from the very first hours of the disaster. Between February 6 and 28, a total of 3,540 flights evacuated 617,593 earthquake victims, with medical evacuations constituting a significant portion of these operations. The use of air ambulances and specially organized evacuation flights accelerated access to health care services and ensured the safe transfer of critically ill patients to hospitals in other provinces. This case demonstrates that air transportation, beyond its logistical function, serves as a lifesaving mechanism in the aftermath of earthquakes.Reference Ertek 5
Efficient triage and resource allocation are vital during such disaster situations, with a crucial aspect being the identification of patients who require air transfer to specialized facilities for further management.Reference Ono, Ikegami and Shimada 6 , Reference Yi-Szu, Chung-Ping and Tzu-Chieh 7 While air ambulances play a crucial role, they may not be able to accommodate all patients, and ground ambulances alone may not suffice.
Hence, it is imperative to identify patients capable of seeking medical help independently and to prioritize those with critical conditions requiring immediate attention at the disaster site. The lack of substantial research addressing this decision-making process, along with the potential utility of established trauma scoring systems, constitutes one of the primary motivations for our study. The Injury Severity Score (ISS), Trauma and Injury Severity Score (TRISS), and Revised Trauma Score (RTS) are widely recognized tools that quantify trauma severity through anatomical and physiological parameters. ISS provides a numerical assessment of the overall severity of multiple injuries, TRISS combines anatomical and physiological data to predict survival probability, and RTS evaluates trauma severity based on vital signs. These systems have been applied in various trauma contexts to guide clinical decision-making, yet their role in earthquake-related patient transfer decisions remains underexplored. Addressing this gap, our study investigates their applicability in disaster planning strategies, particularly in determining indications for air transfer.Reference Byerly, Benjamin and Biswas 8 –Reference Skaga, Eken and Søvik 12
The aim of this study is to comparatively evaluate the data of patients admitted to our hospital after the 2023 Kahramanmaraş earthquake, either via air ambulance or by self-transport from 1,100 kilometers away, by analyzing trauma scores (ISS, TRISS, and RTS), biochemical markers (such as creatine kinase and potassium), and clinical outcomes (including crush syndrome, fasciotomy, acute kidney failure, and hydration status). The study aims to determine the diagnostic value of air transfer and assess the applicability of these scores and clinical parameters in disaster planning strategies.
Methods
This retrospective study included two groups of patients: the air transfer group and the walk-in group. The air transfer group consisted of patients who were transferred to our facility via air transport, while the walk-in group included patients who arrived at the hospital by other means.
All patient-related information, including demographic characteristics, timing of hospital admission, mode of arrival (air transfer or self-admission), clinical findings, hospital course, and laboratory parameters, was obtained retrospectively from the hospital’s electronic medical records and institutional medical database as routinely collected clinical data (secondary data).
In contrast, trauma severity scores—ISS, RTS, and TRISS—were not routinely available in the medical records and were calculated independently by the authors based on documented clinical, physiological, and anatomical injury data, constituting primary study data.
The diagnostic accuracy of ISS, RTS, and TRISS scores in identifying the need for air transfer was assessed using the right statistical analyses.
Design and Setting
The study was performed using a retrospective design in the Emergency Department of Bakırköy Dr. Sadi Konuk Training and Research Hospital, a high-capacity tertiary referral center located in Istanbul and outside the earthquake-affected region. During the 2023 earthquakes, this hospital functioned as a major referral center for patients transferred from disaster-affected provinces.
Prior to undertaking the study, ethical clearance was obtained from the Ethics Board of Bakirkoy Sadi Konuk Training and Research Hospital (with consent from 20.02.2013 with reference number 2023/04/14 and protocol number 2023-87).
The study sample included 397 patients aged 18 and above, who were admitted to the Emergency Clinic of Bakirkoy Sadi Konuk Training and Research Hospital via air transfer or walk-in between February 6, 2023, and February 22, 2023, and had sustained injuries due to the earthquake.
Inclusion criteria comprised adult patients (≥18 years) who sustained earthquake-related injuries and were admitted to the emergency department between February 6 and February 22, 2023, either via air medical transfer or self-admission.
Exclusion criteria included patients under 18 years of age, individuals without earthquake-related injuries, and patients with incomplete medical records.
The study was planned as a retrospective, cross-sectional, observational study with patients who were admitted to our hospital after the earthquake by air transfer or self-admission.
Study Population
A total of 21515 patients presented to our Emergency Clinic during the study period. Among these patients, 429 were earthquake victims. Of the patients presenting to Bakırköy Dr. Sadi Konuk Training and Research Hospital following the earthquake, 5 were excluded from the study for being under 18 years of age. Additionally, the records of 27 patients were incomplete and therefore excluded. In total, 32 patients did not meet the inclusion criteria and were excluded from the study.
Data Analysis and Programs Used
The statistical analysis was undertaken with IBM SPSS Statistics (SPSS) V.20.0 and MedCalc statistical software V.18.2.1 (MedCalc Software, Ostend, Belgium). The distribution of the groups was figured out by the Shapiro-Wilks and Kolmogorov-Smirnov tests. The continuous variables shown were based on means (±) SD or medians (25% quartile, 75% quartile), as proper. Other variables were shown according to composition ratios (%). This study used the Student’s t-test or Mann-Whitney U test to show comparisons between continuous variables. Similarly, the χReference Yarkaç, Buyurgan and Bozkurt Babuş 2 test or Fisher’s exact test was undertaken to show comparisons between categorical variables. To assess the ability of the scores to predict air transfer, ROC curve analyses were conducted. The prediction performance of these scoring systems to discriminate between outcomes was evaluated by calculating the AUC of the ROC and its 95% CI.
The dependent variable was the mode of air transfer (yes/no).
Multivariate logistic regression was performed to identify independent predictors of air transfer, adjusting for potential confounders such as hospital length of stay, SpO₂ level, pulse rate, presence of major trauma, need for endotracheal intubation, altered mental status, requirement for supplementary oxygen therapy, presence of crush syndrome, acute infectious status, need for fasciotomy, fasciotomy performed during hospitalization, occurrence of amputation, pneumothorax and need for chest tube insertion, cephalic hematoma, subdural hematoma, head injury, cervical injury, thoracic injury, abdominal injury, presence of blunt or penetrating trauma, need for blood transfusion, hospital admission, intensive care unit admission, and admission to specific clinical services (internal medicine, orthopedics).
Laboratory parameters included white blood cell count, neutrophil count, potassium, AST, ALT, calcium, urea, creatinine, sodium, PCO₂, bicarbonate, serum osmolarity, creatine kinase, and the neutrophil-to-lymphocyte ratio.
Results
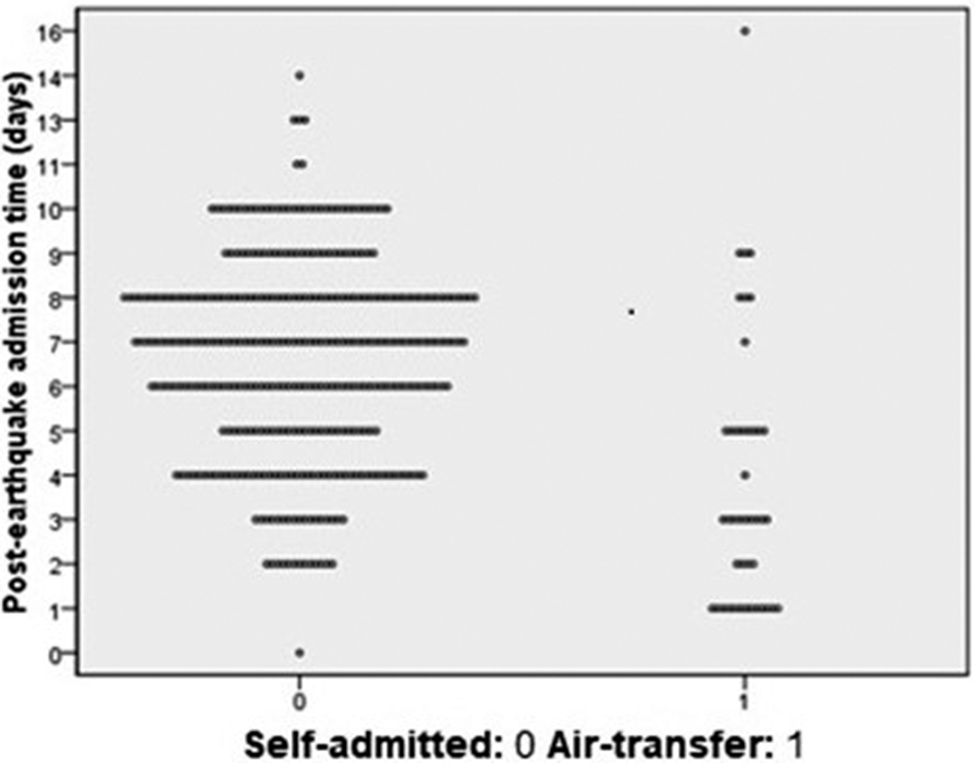
The study enrolled 397 patients, with 43 arriving at our hospital via air transport and 354 self-admitted. Air transport was primarily utilized in the earthquake’s early days. Among air transferred patients, the highest admissions (n = 13, 30.23%) occurred on day 1. For walk-in patients, peak admissions were observed on day 8 (n = 69, 19.49%) (Figure 1).
Distribution of air transfer and walk-in patients according to post-earthquake days of presentation (each point represents 1 patient).

Figure 1. Long description
The horizontal axis has two categories: 0 for self-admitted patients and 1 for air-transfer patients. The vertical axis shows post-earthquake admission time in days, ranging from 0 to 16. For self-admitted patients, dots are densely distributed between days 2 and 10, with a few outliers at days 0, 11, 13, and 14. For air-transfer patients, dots are more sparsely distributed, mostly between days 1 and 7, with a single outlier at day 15. Each dot represents one patient. The distribution for self-admitted patients is broader and more concentrated in the mid-range, while air-transfer patients are clustered in the lower range of admission days.
The study compared the distribution of mean ages of Air transfer group (41.00±17.89 years) and Walk-in group (45.47±18.52 years), revealing no significant difference (P = 0.173, t = 1.370). Gender distribution of Air transfer group had 23 females (53.5%), Walk-in group had 199 females (56.2%), with no significant difference (P = 0.734, Table 1).
Demographic and clinical information about the patients included in the study

Table 1. Long description
The table is organized into three sections. The first section lists continuous variables with columns for demographic and clinical information, air transfer mean plus or minus standard deviation, walk-in mean plus or minus standard deviation, P value, and t value. Variables and values are: Age: air transfer 41.00 plus or minus 17.89, walk-in 45.47 plus or minus 18.52, P 0.173, t 1.370. Systolic blood pressure in millimeters of mercury: air transfer 119.79 plus or minus 9.95, walk-in 123.80 plus or minus 9.70, P 0.031, t 2.180. Diastolic blood pressure: air transfer 68.10 plus or minus 5.67, walk-in 68.86 plus or minus 6.65, P 0.529, t 0.631. Mean blood pressure: air transfer 101.70 plus or minus 15.596, walk-in 54.00 plus or minus 16.84, P 0.157, t negative 1.424. Pulse pressure: air transfer 54.29 plus or minus 19.89, walk-in 60.32 plus or minus 20.97, P 0.252, t 1.154. Duration of entrapment in days: air transfer 13.26 plus or minus 28.31, walk-in 0.70 plus or minus 5.06, P 0.069, t negative 1.932. Length of hospital stay in days: air transfer 20.07 plus or minus 10.61, walk-in 2.91 plus or minus 6.43, P 0.000, t negative 7.977. The second section presents medians with interquartile ranges, with columns for variable, air transfer median I Q R, walk-in median I Q R, P value, and u value. G C S: both groups 15 (15 to 15), P 0.205, u 1166.500. Respiratory rate per minute: both groups 15 (14 to 16), P 0.765, u 1183.000. S P O sub 2 percent: air transfer 95 (91.75 to 98), walk-in 97 (95 to 98), P 0.027, u 830.000. Pulse per minute: air transfer 102 (87 to 120), walk-in 88 (81 to 102), P 0.002, u 738.000. The third section shows categorical data for sex, with columns for variable, air transfer n percent, walk-in n percent, and P value. Male: air transfer 20 (46.5 percent), walk-in 155 (43.8 percent), P 0.734. Abbreviations are listed as G C S for Glasgow coma score, Max for maximum, Min for minimum, S D for standard deviation, and S P O sub 2 for oxygen saturation.
Abbreviations: GCS: Glasgow coma score, Max: Maximum, Min: Minimum, SD: Standard deviation, SpO2: Oxygen saturation.
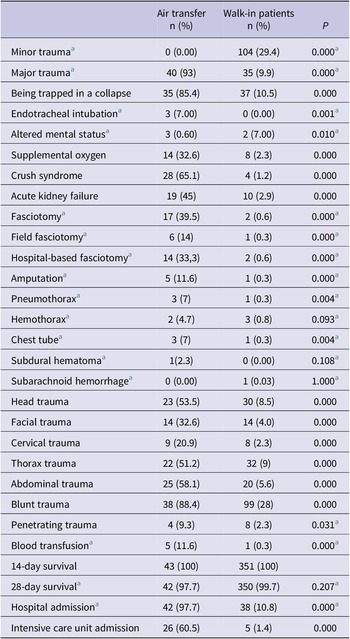
No significant distinctions in comorbidity presence between Air transfer (n = 7, 16.3%) and Walk-in (n = 65, 18.4%, P = 0.738). Similarly, no significant group differences in hypertension, diabetes, malignancy, coronary artery disease, Alzheimer’s disease, chronic kidney failure, cerebrovascular disease, dysrhythmia, or psychiatric illness (P > 0.05, Table 2).
Additional clinical information and comorbidities about the patients included in the study

Table 2. Long description
Beginning at the top row, the leftmost column lists clinical conditions and interventions. The next column presents air transfer patient counts and percentages, followed by walk-in patient counts and percentages, and the rightmost column shows P values. Minor trauma is absent in air transfer patients but present in 29.4 percent of walk-ins, with a P value of 0.000. Major trauma is highly prevalent in air transfer patients at 93 percent versus 9.9 percent in walk-ins, P value 0.000. Being trapped in a collapse affects 85.4 percent of air transfer patients and 10.5 percent of walk-ins, P value 0.000. Endotracheal intubation occurs in 7 percent of air transfer patients and none of walk-ins, P value 0.001. Altered mental status is 0.6 percent in air transfer and 7 percent in walk-ins, P value 0.010. Supplemental oxygen is given to 32.6 percent of air transfer patients and 2.3 percent of walk-ins, P value 0.000. Crush syndrome is seen in 65.1 percent of air transfer patients and 1.2 percent of walk-ins, P value 0.000. Acute kidney failure is 45 percent in air transfer and 2.9 percent in walk-ins, P value 0.000. Fasciotomy is performed in 39.5 percent of air transfer patients and 0.6 percent of walk-ins, P value 0.000. Field fasciotomy is 14 percent in air transfer and 0.3 percent in walk-ins, P value 0.000. Hospital-based fasciotomy is 33.3 percent in air transfer and 0.6 percent in walk-ins, P value 0.000. Amputation is 11.6 percent in air transfer and 0.3 percent in walk-ins, P value 0.000. Pneumothorax is 7 percent in air transfer and 0.3 percent in walk-ins, P value 0.004. Hemothorax is 4.7 percent in air transfer and 0.8 percent in walk-ins, P value 0.093. Chest tube placement is 7 percent in air transfer and 0.3 percent in walk-ins, P value 0.004. Subdural hematoma is 2.3 percent in air transfer and absent in walk-ins, P value 0.108. Subarachnoid hemorrhage is absent in air transfer and 0.03 percent in walk-ins, P value 1.000. Head trauma is 53.5 percent in air transfer and 8.5 percent in walk-ins, P value 0.000. Facial trauma is 32.6 percent in air transfer and 4 percent in walk-ins, P value 0.000. Cervical trauma is 20.9 percent in air transfer and 2.3 percent in walk-ins, P value 0.000. Thorax trauma is 51.2 percent in air transfer and 9 percent in walk-ins, P value 0.000. Abdominal trauma is 58.1 percent in air transfer and 5.6 percent in walk-ins, P value 0.000. Blunt trauma is 88.4 percent in air transfer and 28 percent in walk-ins, P value 0.000. Penetrating trauma is 9.3 percent in air transfer and 2.3 percent in walk-ins, P value 0.031. Blood transfusion is 11.6 percent in air transfer and 0.3 percent in walk-ins, P value 0.000. Fourteen-day survival is 100 percent in both groups. Twenty-eight-day survival is 97.7 percent in air transfer and 99.7 percent in walk-ins, P value 0.207. Hospital admission is 97.7 percent in air transfer and 10.8 percent in walk-ins, P value 0.000. Intensive care unit admission is 60.5 percent in air transfer and 1.4 percent in walk-ins, P value 0.000. Fisher’s exact test is used for statistical comparison.
a Fisher’s exact test.
The crush syndrome rate was markedly higher in the Air transfer group (n = 28, 65.1%) compared to the Walk-in group (n = 4, 1.2%) (P = 0.000). Similarly, fasciotomy rates were elevated in the Air transfer group (n = 17, 39.5%) compared to the Walk-in group (n = 2, 0.6%) (P < 0.001). There was no significant difference in the 28-day survival rate between the Air transfer group (n = 42, 97.7%) and the Walk-in group (n = 350, 99.7%) (P = 0.207). However, the rate of acute kidney failure was significantly higher in the Air transfer group (n = 19, 45.2%) compared to the Walk-in group (n = 10, 2.9%) (P = 0.000, Table 2, Table S-1).
In the Air transfer group, the median pulse was 102 (IQR: 87-120) compared to 88 (IQR: 81-102) in the Walk-in patients’ group, with a significantly higher pulse rate in the Air transfer group (P = 0.002, U = 738.000), suggesting an association between mode of arrival and pulse rate. Mean osmolarity for Air transfer was 274.61±11.12 mOsm/kg, while Walk-in Patients had 285.04±9.53 mOsm/kg, indicating higher osmolarity in Walk-in Patients (P = 0.000, t = 4.154). Sodium levels were 137.75±3.41 mEq/L in Walk-in patients and 134.40±4.50 mEq/L in Air transfer, significantly higher in Walk-in patients (P = 0.000, t = 3.953). Median potassium was 4.60 mEq/L (IQR: 4.20-5.80) in the Air transfer and 4.26 mEq/L (IQR: 4.06-4.51) in the Walk-in group, demonstrating higher levels in the Air transfer group (P = 0.004, U = 579.500; Table 3).
Laboratory test results of the patients included in the study

Table 3. Long description
The first block presents medians and interquartile ranges for air transfer and walk-in patients across hemoglobin, W B C, neutrophil, lymphocyte, potassium, creatinine, lactate, AST, ALT, calcium, INR, and PT. Significant differences are observed in W B C (16.5 all over 8.36, P equals 0.000), neutrophil (12.13 all over 5.81, P equals 0.000), AST (364.70 all over 20.00, P equals 0.000), ALT (135.00 all over 17.50, P equals 0.000), potassium (4.60 all over 4.26, P equals 0.004), calcium (8.34 all over 8.89, P equals 0.013), INR (1.20 all over 1.10, P equals 0.005), and PT (16.20 all over 14.80, P equals 0.010). The second block shows means plus or minus S D and min-max values for hematocrit, platelet count, sodium, urea, glomerular filtration rate, Pa C O sub 2, H C O sub 3, and osmolarity. Significant differences are found in sodium (134.40 all over 137.75, P equals 0.000), Pa C O sub 2 (33.92 all over 42.13, P equals 0.000), H C O sub 3 (21.24 all over 23.60, P equals 0.002), and osmolarity (274.61 all over 285.04, P equals 0.000). All abbreviations are defined in the table foot.
Abbreviations: ALT: Alanine transaminase, AST: Aspartate aminotransferase, INR: International normalized ratio, PaCO2: The partial pressure of carbon dioxide, PaO2: The partial pressure of oxygen, PT: Prothrombin time, SpO2: Oxygen saturation, WBC: White blood cell.
The Neutrophil-to-lymphocyte ratio (NLR) median was 8.37 (IQR: 3.44-12.84) for Air transfer and 3.00 (IQR: 2.11-5.50) for Walk-in, significantly higher in Air transfer (P = 0.000, U = 478.000). Creatine kinase (CK) levels in Air transfer had a median of 6034.50 IU/L (IQR: 1229.75-40753.25), whereas Walk-in had a median of 104.00 IU/L (IQR: 64.75-356.75), showing a significant difference (P = 0.000, U = 175.000). The shock index median was 0.70 (IQR: 0.60-1.00) for Air transfer and 0.70 (IQR: 0.60-0.80) for Walk-in, with no significant difference (P = 0.157, U = 1010.500). RTS median was 8 (IQR: 8-8) for both Air transfer and Walk-in, with no significant difference (P = 0.303, U = 483.000). The median TRISS was 98.87 (IQR: 98.55-99.65) for Air transfer and 9.65 (IQR: 99.52-99.65) for Walk-in, significantly higher in Air transfer (P = 0.006, U = 165.500). Mean ISS was 12.63±10.37 for Air transfer and 0.91±5.20 for Walk-in, significantly higher in Air transfer (P < 0.001, t = −5.152, Table 4, Table S-2).
Clinical scores, ratios, and levels of the patients included in the study

Table 4. Long description
Starting with the first table, columns are: clinical parameter, air transfer median with interquartile range, walk-in median with interquartile range, P value, and Mann-Whitney U test statistic. The rows are: Shock Index (air transfer 0.70, walk-in 0.70, P 0.157, U 1010.500), Revised trauma score (air transfer 8, walk-in 8, P 0.303, U 483.000), TRISS score (air transfer 98.87, walk-in 9.65, P 0.006, U 165.500), Neutrophil-to-lymphocyte ratio (air transfer 8.37, walk-in 3.00, P 0.000, U 478.000), Creatine kinase levels in I U per L (air transfer 6034.50, walk-in 104.00, P 0.000, U 175.000). The second table has columns: ISS, air transfer mean plus or minus S D, walk-in mean plus or minus S D, P value, and student t test statistic. ISS for air transfer is 12.63 plus or minus 10.37, walk-in is 1.91 plus or minus 5.20, P 0.000, t minus 5.152. Abbreviations are listed at the bottom: I S S is Injury Severity Score, T R I S S is Trauma and Injury Severity Score.
Abbreviations: ISS: Injury severity score, TRISS: Trauma and Injury Severity Score.
The ISS score demonstrated strong discrimination (AUC = 0.880) with an optimal criterion (>6), achieving 55.56% sensitivity, 93.75% specificity, and a highly significant association with Air transfer indication (P < 0.0001). In contrast, the TRISS score displayed moderate discrimination (AUC = 0.723) with an optimal criterion (<98.87), yielding 56.52% sensitivity, 84.62% specificity, and a significant association with Air transfer indication (P = 0.0020). Creatine kinase levels also moderately discriminated (AUC = 0.865) with an optimal criterion (>1516), resulting in 69.23% sensitivity, 92.00% specificity, and a highly significant association with Air transfer indication (P < 0.0001) (Figure 2).
The diagnostic accuracy of 3 variables, namely Creatine Kinase level, ISS Score, and TRISS Score, was evaluated using the ROC curve analysis.

Figure 2. Long description
The graph plots sensitivity on the vertical axis from zero to one hundred and one hundred minus specificity on the horizontal axis from zero to one hundred. Three ROC curves are shown: blue circles for Creatine Kinase, brown squares for I S S Score, and green triangles for T R I S S Score. All curves start near the origin and rise toward the upper right, with I S S Score showing the steepest initial increase and highest sensitivity at lower false positive rates. Creatine Kinase and T R I S S Score curves rise more gradually. The legend at the lower right identifies each variable by color and marker shape. The diagonal reference line indicates random performance.
There were no statistically significant differences between the areas under the ROC curves for Creatine Kinase and ISS Score (difference = 0.0435, SE = 0.101, 95% CI: −0.154 to 0.241, z = 0.430, P = 0.6668), between Creatine Kinase and TRISS Score (difference = 0.0955, SE = 0.107, 95% CI: −0.115 to 0.306, z = 0.891, P = 0.3730), and between ISS Score and TRISS Score (difference = 0.0520, SE = 0.0448, 95% CI: −0.0358 to 0.140, z = 1.161, P = 0.2457) (Figure 2).
Discussion
The present study aimed to compare two distinct patient groups following the 2023 Turkey earthquake, namely the Air transfer group and the Walk-in patient group, both of whom were admitted to a hospital situated 1,100 km away from the disaster site. In terms of air transferred patients, the highest number of admissions occurred on the 1st day (n = 13, 30.23%) and initial 5 days. As for walk-in patients, the peak admissions were seen on the 8th day (n = 69, 19.49%) and started in 4th day (Figure 1). According to a study conducted after the 1999 Marmara earthquake in Turkey, most of the patients were hospitalized within the first three days after the earthquake. Additionally, the study by Almeida et al. (2020) in Nepal after the 2015 earthquake showed a first peak of admissions on the fifth day, as our study mentioned. These findings emphasize the importance of early preparedness and developing a work plan to manage patients arriving via air transport and walk-in patients in the immediate aftermath of an earthquake. Even though hospitals are distant from the disaster area, being prepared for patients arriving via air transport from the first day and developing a work plan to manage walk-in earthquake victims, particularly between days 4 and 8, based on the distance, will ease patient management.Reference Almeida, Schlüter and Loenhout 13 , Reference Bulut, Fedakar and Akköse 14
In the comparison between the Walk-in Patients group and the Air transfer group, significant differences were seen in osmolarity and sodium levels. The Walk-in Patients group had a higher mean osmolarity and sodium levels compared to the Air transfer group, showing a potential association with dehydration in the Walk-in patients who did not receive intravenous fluids during transportation. Therefore, it is crucial to supply hydration measures to self-transferred patients both at the scene and during transfer to prevent dehydration. Fluid resuscitation is lifesaving, especially in the first hours after trauma.Reference Bolorunduro, Villegas and Oyetunji 11 Upon arrival at the hospital, prompt administration of intravenous fluids should be started to support these patients after emergency department admission.
Additionally, the white blood cell count (WBC) was significantly higher in the Air transfer group compared to the Walk-in group. Furthermore, the median potassium level was significantly higher in the Air transfer group compared to the Walk-in group. This difference in potassium levels may be attributed to factors such as rhabdomyolysis, commonly associated with multiple traumas in Air transfer patients, showing the importance of considering potassium levels as an indicator of potential muscle injury and the need for proper management in Air transfer patients. Increased serum potassium levels may be related to worse prognosis.Reference Wrzosek, Drygalski and Garlicki 15
In the Air transfer patient group, the rates of crush syndrome were statistically significantly higher (65.1%) compared to the Walk-in patients’ group (1.2%) (P = 0.000). Similarly, the rates of fasciotomy were notably elevated in the Air transfer patient group (39.5%) compared to the Walk-in patients’ group (0.6%) (P < 0.001). The heightened levels of CK and potassium seen in the Air transfer group may have arisen because of these conditions.
In terms of survival outcomes, there was no statistically significant difference in the 28-day survival rate between the Air transfer group (97.7%) and the Walk-in patients’ group (99.7%, P = 0.207). In a similar vein to Guodong Liu et al.’s 2016 study on the Sichuan earthquake, we too did not find a significant difference in mortalities. They attributed this finding to the high-risk patients succumbing in the first hours due to the geographical devastation in the disaster area.Reference Almeida, Schlüter and Loenhout 13 In our study, being situated 1,100 km away from the disaster site, we encountered cases where individuals did not reach our hospital, leading to comparable mortality rates. The substantial geographic distance could have contributed to the observed similarity in mortality.Reference Park, Baek and Lee 16 It can be the result of the distance of the hospital, which is about 1,100 km from the disaster site.
Nonetheless, the incidence of acute kidney failure was markedly higher in the Air transfer patient group (45.2%) when compared to the Walk-in patients’ group (2.9%, P = 0.000). This notable discrepancy could potentially find its explanation in the elevated occurrence of crush syndrome among patients transported via air. Such a circumstance might indeed manifest as a complication of this syndrome, as noted by Kenneth D. Lempert et al. in their 2019 research paper. In their study, Lempert et al. expounded on the association between significant catastrophic events and instances of kidney failure, particularly those linked to crush syndrome. This syndrome engenders systemic manifestations, notably including acute kidney injury, electrolyte imbalances, sepsis, and other systemic effects. These manifestations stem from direct injuries, such as those caused by the collapse of materials and debris, which later induce muscular swelling within the affected regions of the body.Reference Liu, Ou and Qiu 17
These findings highlight the importance of early hydration interventions during disaster response, particularly for independently arriving patients who may experience dehydration. The observed differences in potassium levels and the rates of crush syndrome and fasciotomy further emphasize the significance of proper management strategies for patients undergoing air transfer, with special consideration for potential muscle injuries. Timely interventions and effective coordination between emergency response teams and hospitals are critical in improving patient outcomes and reducing the risk of complications in disaster situations. Future disaster preparedness plans should consider the identified dehydration trends and potential risk factors associated with air transfer patients to enhance patient care during similar events.
The findings of this retrospective study supply valuable insights into the diagnostic accuracy of ISS and TRISS in showing the indication for air transfer in patients admitted after the 2023 Turkey earthquake. The results proved that all these variables showed discriminatory ability in finding the need for air transfer. The elevated levels of CK in the air transfer group compared to the walk-in group suggest a potential association between CK level and the severity of traumatic injuries. Serum creatine kinase (CK) levels, which correlate with the degree of muscle injury, can be used to assess the severity of rhabdomyolysis.Reference Lempert and Kopp 18 In a study analyzing patients with crush syndrome after an earthquake, a significant correlation was found between peak serum CK levels and the number of crushed extremities. CK is a marker of muscle damage, and its elevation may indicate the presence of rhabdomyolysis, which is commonly associated with multiple trauma.Reference Byerly, Benjamin and Biswas 8 , Reference Malinoski, Slater and Mullins 19 This finding supports previous research that has highlighted the role of CK level in assessing the severity of traumatic injuries.Reference Vasquez, DiSanto and Reilly 20
The ISS score, a widely used scoring system that quantifies the overall severity of multiple injuries sustained by a patient, was significantly higher in the air transfer group compared to the walk-in group, as the earlier studies mentioned to.Reference Michaels, Pham and Puckett 21 This shows that patients needing air transfer had more severe injuries, which aligns with the purpose of air transfer to specialized facilities for further management of critically injured patients.Reference Boyd, Corse and Campbell 22 The ISS score has been confirmed as a reliable predictor of mortality and morbidity in trauma patients.Reference Bolorunduro, Villegas and Oyetunji 11 The TRISS score, which combines anatomical and physiological parameters to predict the probability of survival in trauma patients, was also significantly higher in the air transfer group. This suggests that patients needing air transfer had a higher probability of high-degree trauma, emphasizing the need for specialized care in these cases.Reference Rau, Wu and Chuang 23 The ROC curve analysis further supported the diagnostic accuracy of these variables. The AUC values for the ISS score and the TRISS score show their ability to differentiate between the air transfer and walk-in patient groups. In a 2021 study conducted by Yang Pei et al. in China, which aimed to evaluate the accuracy of various injury triage methods including the Simple Triage and Rapid Treatment (START) technique, CareFlight Injury Triage (CareFlight), Rapid Emergency Medicine Score (REMS), Triage Revised Trauma Score (T-RTS), and Triage Early Warning Score (TEWS), in the context of earthquake scenarios, the REMS injury triage method exhibited the most substantial area under the curve (AUC = 0.835) compared to the other four methods.Reference Peng and Hu 24 In our study, we observed that the ISS demonstrated superior performance (AUC = 0.880), while the RTS exhibited limited ability to identify patients accurately.Reference Rau, Wu and Chuang 23
It is important to note that while these variables showed discriminatory ability, they should not be used as standalone indicators for air transfer. Incorporating additional factors or a combination of variables may further enhance the accuracy of identifying the need for air transfer. Future research could explore the integration of other clinical and demographic factors to develop a comprehensive new scoring system that improves the predictive ability of these variables.
In conclusion, the findings of this study support the potential utility of the ISS and TRISS scores in identifying the indication for air transfer in patients admitted after the 2023 Turkey earthquake. These variables can aid health care professionals in making informed decisions on resource allocation and patient management. However, further research is called for to confirm and refine these findings, considering other factors and expanding the scope to different disaster scenarios.
Overall, the study highlights the importance of using air transfer in disaster response, as it offers significant advantages in promptly transporting critically ill or injured patients to appropriate medical facilities. However, it is essential to acknowledge that not all patients can be transferred by air due to logistical constraints. In such cases, the use of scoring systems, such as ISS and TRISS, becomes valuable in finding patients who require air transfer or can be managed as walk-in cases. Moreover, our findings emphasize the critical role of adequate hydration for independently arriving patients, considering the higher rates of dehydration seen in this group. Disaster preparedness planning should take these factors into account to optimize patient care and outcomes during future disaster events.
ISS and TRISS scores can be used in an analogous manner to show the indication for Air transfer, except for RTS and shock index. Our findings show that both the shock index and revised trauma scores were not effective in finding patients suitable for air transfer decisions.
Limitations of Our Study
Due to the retrospective nature of our study, analyses could only be conducted on patients who were able to reach the hospital. The number of cases that deceased during transfer or at the scene cannot be figured out. Additionally, limitations arise from the lack of information on scoring at the time of the incident and the clinical characteristics of the patients. The data collected at the time of admission are subject to constraints as they were obtained during the record-keeping process. Prospective studies with ethical approval that would start once at the time of the earthquake are unfeasible due to the unpredictable nature of earthquake occurrences. Noteworthy strengths of our study include the proximity of the center to the airport, statistical similarity in terms of age, gender, and comorbidity between the walk-in and air transfer populations, as well as the substantial number of patients involved.
Conclusion
In this study, we conducted a retrospective assessment of the diagnostic accuracy of ISS and TRISS in determining the indication for air transfer in patients admitted following the 2023 Turkey earthquake. Our findings revealed that these two variables can be effectively used to identify the need for air transfer, whereas RTS and shock index demonstrated limited utility in this regard. In addition, elevated creatine kinase and potassium levels in air transferred patients highlight the importance of considering biochemical markers as potential supportive indicators of severe trauma and crush syndrome.
To further enhance the accuracy of air transfer decision-making, future research may explore the incorporation of additional clinical and demographic factors or the use of combined variables to develop a more comprehensive scoring system. Moreover, our results emphasize the critical role of hydration strategies for self-admitted patients, given the higher osmolarity and sodium levels observed in this group, which may reflect dehydration during prolonged transport.
From a disaster preparedness perspective, distant hospitals should be ready to accommodate air transferred patients during the first 5 days and should also prepare for self-admitted patients beginning from the fourth day onward. These findings underscore the necessity of coordinated planning between emergency response teams and health care facilities to optimize patient outcomes in large-scale disaster scenarios.
Supplementary material
The supplementary material for this article can be found at http://doi.org/10.1017/dmp.2026.10378.







 Open access
Open access