


Event Description
Event Type: Hurricane and Tropical Storm
Event Date: September 26, 2024
Location: Mitchell and Yancey Counties in Western North Carolina (USA)
Response Type: Community Assessment for Public Health Emergency Management (CASPER)
Introduction
Hurricane Helene made landfall in Florida (USA) on September 26, 2024 and moved inland to severely impact Western North Carolina with catastrophic flooding, landslides, and severe damage to homes, businesses, and transportation and communications infrastructure. A major disaster was declared in 39 of North Carolina’s 100 counties and for the Eastern Band of Cherokee Indians. According to the North Carolina Department of Health and Human Services (DHHS; Raleigh, North Carolina USA), 108 deaths were attributed to the direct impacts of the storm, including eleven in Yancey County and three in Mitchell County, 13% of the total. These two rural counties also experienced two of the top three rainfall amounts measured in North Carolina, with 30.78 inches in Yancey County and 23.31 inches in Mitchell County, while the highest wind gusts (92 miles per hour) were recorded in Yancey County. Reference Hagen, Cangialosi, Chenard, Alaka and Delgado1
The Community Assessment for Public Health Emergency Response (CASPER) has been used to inform and assess post-disaster recovery through the collection of reliable and objective information that can provide data for decision making. Reference Korteweg, van Bokhoven, Yzermans and Grievink2,3 The objectives of this modified CASPER, which was conducted by the University of Delaware (Newark, Delaware USA) and a local community-based organization Sustaining Essential and Rural Community Healthcare (SEARCH; Burnsville, North Carolina USA), were: (1) to assess on-going household impacts and recovery from Hurricane Helene in two rural Western North Carolina counties, and (2) to inform long-term recovery planning conducted by groups such as the Yancey County Long-Term Recovery Group and the Mitchell County Long-Term Resilience Group.
Source
A 29-question survey was adapted from a CASPER that was conducted by the Buncombe County Public Health Department (Asheville, North Carolina USA) in June 2025. The survey included information about each household’s members (eg, age, ownership status, job status, and health insurance coverage); evacuation before, during, or after Hurricane Helene; household repair and recovery status (eg, debris removal, safety, and housing assistance); presence of mold or physical health systems associated with indoor air quality; access to health care; environmental impacts (eg, safety of drinking water, wells, and septic systems); and mental health status (eg, new or worsening symptoms, availability and use of mental health supports, and stressors). The full survey is available as Supplementary Material. This study was determined to be exempt from formal Institutional Review Board (IRB) review by the IRB of the University of Delaware under Study ID 2291737-1.
The CASPER surveys use a two-stage cluster sampling technique modified by Centers for Disease Control and Prevention (CDC; Atlanta, Georgia USA) for use in disaster settings. 3,Reference Malilay, Flanders and Brogan4 The sampling frame for this study included Yancey and Mitchell counties in Western North Carolina, two rural counties directly impacted by Hurricane Helene. Due to the rural nature of these counties and the large number of United States Census blocks with less than 10 households, 20 US Census blocks in each county were selected with probability proportional to population size, with replacement in the first stage of sampling. To reduce the number of very small US Census blocks included, the smallest five blocks were removed. The final sampling frame included 29 selected US Census blocks (14 in Mitchell County [one block selected twice] and 15 in Yancey County); Figure 1. In each selected cluster, seven random addresses were selected, and interview teams of at least two local residents were assigned to each cluster.
Selected US Census Blocks for Community Assessment for Public Health Emergency Response (CASPER) - Hurricane Helene, Mitchell and Yancey Counties, North Carolina (USA).

Data recorded on paper surveys by field teams were entered into Qualtrics (Provo, Utah USA) and downloaded into Microsoft Excel (Redmond, Washington USA) and SAS v9.4 (Cary, North Carolina USA) for analysis. As outlined in the CDC CASPER Toolkit, contact, cooperation, and completion rates were calculated. 3,Reference Malilay, Flanders and Brogan4 Per the Toolkit’s formula, stratified weights were calculated for Mitchell and Yancey counties as the ratio of the total number of households in the county and the product of the number of households interviewed in a given cluster and the total number of clusters selected within the county. 3,Reference Malilay, Flanders and Brogan4 Weighted frequencies, percentages, and 95% confidence intervals (95% CI) were calculated using the SURVEYFREQ procedure. All presented results are weighted. Since prevalence, rather than measures of association, are reported, there were no adjustments for multiple comparisons. Design effects, including stratification by county, were accounted for in the sampling strategy and subsequent weighting of data. Accordingly, 95% CIs should be interpreted as confidence intervals around the weighted prevalence estimates and should not be used in place of hypothesis testing.
Observations
One year after Hurricane Helene, many households in rural Western North Carolina continued to recover. More than one-in-seven still reported they had someone living with them who was displaced by the storm. Nearly one-third of all homes in these two rural counties were moderately or severely damaged by the storm. With a majority of the population covered by Medicare for those over 65 years of age or with certain disabilities (55.5%) or Medicaid for those with low incomes or a disability (26.6%), dealing with the costs of repairs on a fixed or low income could have substantial negative impacts on recovery trajectory. The North Carolina Office of State Budget and Management (OSBM; Raleigh, North Carolina USA) estimated $12.7 billion in direct residential damage of more than 70,000 homes across the region. 5
After the storm, more than 13,000 reports of damage to private roads and bridges were submitted to the State’s Private Roads and Bridges Program, 6 while 1,400 state roads and 818 state-maintained bridges were reportedly damaged and closed. Reference Colburn7 Although many have been repaired, damage to the transportation infrastructure in these mountainous rural counties remains a major challenge to recovery.
While reports of new or exacerbated mental health conditions like anxiety, depression, or posttraumatic stress disorder are relatively common following disasters, identification and referral of individuals to appropriate care remains difficult in this rural setting. Reference North and Pfefferbaum8 Factors that remain common in the study location, like displacement, have been shown to increase the risk for, and symptoms of, mental health sequalae. Reference Schwartz, Liu, Lieberman-Cribbin and Taioli9
This study has several important limitations. Survey data were collected up to 11 months after Hurricane Helene impacted Western North Carolina – there was potential for recall bias. However, Hurricane Helene was a major disaster event in an area not often impacted by hurricanes, making it likely that respondents would accurately remember their experiences. The CASPER surveys were cross-sectional, so the temporal relationship between exposure to Hurricane Helene and outcomes reported by respondents cannot be confirmed. Response bias was also possible if respondents felt that some responses were more socially desirable than others, for example, reporting evacuation. To reduce response bias, surveyors were local residents involved as volunteers with a well-known community-based organization who also experienced the impacts of Hurricane Helene, mitigating potential sources of perceived or realized stigma. Finally, there are limitations inherent in the CASPER method, including the use of US Census data for sampling that may not accurately represent household numbers depending on the time elapsed since the most recent decennial census.
While CASPERs are often conducted rapidly after disasters to prioritize and inform immediate response activities, CASPERs conducted during the recovery period can still provide actionable data and information to public health, public safety, emergency management, and other governmental and community-based organizations involved in community recovery. The results of this CASPER, generalizable to the entire two-county area, can help long-term recovery committees and others prioritize interventions, investments, and activities to address the areas of highest continued need.
Analysis
From June 28 through August 17, 2025, survey teams completed 183 interviews with a completion rate of 87.1%, a cooperation rate of 85.1%, and a contact rate of 55.1% (Table 1).
Community Assessment for Public Health Emergency Response, Hurricane Helene, Mitchell and Yancey Counties, North Carolina (USA): Completion, Contact, and Cooperation Rates, 2011 and 2015

-
1. Completion rate is the number of completed interviews divided by goal number of interviews.
-
2. Contact rate is the number of completed interviews divided by total number of housing units where contact was attempted.
-
3. Cooperation rate is the number of completed interviews divided by total number of housing units where contact was made.
Respondent Demographics
Of the 183 responding households, 90 were in Mitchell County and 93 were in Yancey County, representing 6,411 and 8,188 households, respectively. Most respondents were two-person households (Prevalence: 42.78%; 95% CI, 34.21 – 51.34%), with only 11.86% of households having five or more members (95% CI, 6.83 – 16.89%). Nearly 80% of respondents were single family households (Prevalence 78.92%; 95% CI, 72.73 – 85.11%) and 82.21% owned their home (95% CI, 76.58 – 87.84%).
Housing and Transportation
Fourteen percent of households reported at least one person staying in the home at the time of survey was displaced due to the hurricane (Prevalence: 13.51%; 95% CI, 7.98 – 19.04%). More than 35% of households evacuated because of Hurricane Helene (95% CI, 28.19 – 43.66%). Nearly 18% of all households evacuated after (95% CI, 11.75 – 23.73%), and 8.33% evacuated during the hurricane (95% CI, 4.34 – 12.33%). Barriers to evacuation included but were not limited to concerns about leaving pets and livestock, not being able to buy gas or find safe routes or transport, and prohibitive costs.
Nearly one-quarter of households reported seeing or smelling mold or a musty odor in their home since the hurricane (Prevalence: 22.39%; 95% CI, 15.96 – 28.82%). Barriers to removal or remediation included money or cost, not knowing how, not having access to cleaning supplies or personal protective equipment, being physically unable, or extenuating structural needs. Further, nearly 30% and 16% of households reported environmental hazards such as trees (Prevalence: 29.39%; 95% CI, 22.42 – 36.37%) and household debris (Prevalence: 15.93%; 95% CI, 7.51 – 24.35%), respectively, on their property at the time of survey. Despite all housing and property concerns, nearly 90% of respondents indicated they felt safe living in their home.
Physical and Mental Health Needs
More than 55% of households reported having health insurance through Medicare (Prevalence: 55.51%; 95% CI, 47.25 – 63.77%) and 26.58% reported coverage through Medicaid, medical assistance, or any kind of government assistance plan for those with low incomes or a disability (95% CI, 19.65 – 33.52%); Table 2. Eleven percent of households reported one or more members being uninsured at the time of survey. Fifteen percent of households experienced difficulties in accessing medical care in the aftermath of Hurricane Helene (95% CI, 7.72 – 21.38%). Reported barriers included limited or disrupted transportation and difficulties with insurance coverage.
Community Assessment for Public Health Emergency Response, Hurricane Helene, Mitchell and Yancey Counties, North Carolina (USA): Insurance Coverage

* The 95% CIs around weighted prevalences are not adjusted for multiplicity and should not be used in place of hypothesis testing.
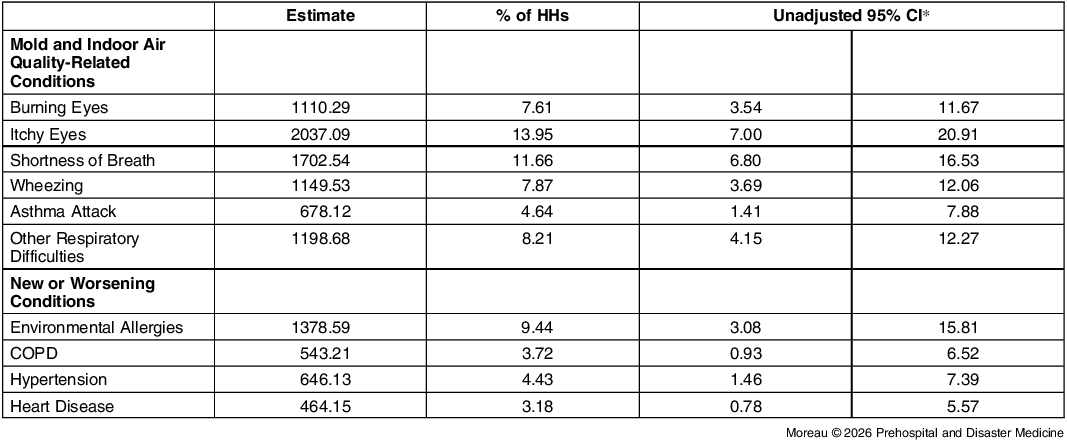
When asked about health outcomes related to mold exposure or indoor air quality, respondents reported a range of respiratory symptoms, including shortness of breath (Prevalence: 11.66%; 95% CI, 6.80 – 16.53%), wheezing (Prevalence: 7.87%; 95% CI, 3.69 – 12.06%), asthma attacks (Prevalence: 4.64%; 95% CI, 1.41 – 7.88%), or other respiratory difficulties (Prevalence: 8.21%; 95% CI, 4.15 – 12.27%). When asked about general health, almost 10% of households reported one or more members experiencing new and worsening environmental allergies, food allergies, asthma, chronic obstructive pulmonary disease, emphysema, hypertension, or heart disease. New or worsening environmental allergies was the most frequently reported condition (Prevalence: 9.44%; 95% CI, 3.08 – 15.81%). One-third (33.72%) of households reported being aware of environmental health hazards – pollutants in the environment that can cause health problems in people – near their residence (95% CI, 24.98 – 42.46%); Table 3.
Community Assessment for Public Health Emergency Response, Hurricane Helene, Mitchell and Yancey Counties, North Carolina (USA): Health Impacts

Abbreviation: COPD, chronic obstructive pulmonary disease.
* The 95% CIs around weighted prevalences are not adjusted for multiplicity and should not be used in place of hypothesis testing.
Following Hurricane Helene, many households reported one or more members having new or worsening mental health symptoms. Over 40% reported anxiety, while roughly 30% reported trouble sleeping and depression. Nearly 60% of households reported being stressed about another disaster affecting their home. New and worsening mental health concerns, as well as sources of stressors, are shown in Table 4. Preferred sources of mental health support were faith-based support (Prevalence: 28.96%; 95% CI, 20.44 – 37.48%), primary care providers (Prevalence: 24.66%; 95% CI, 17.99 – 31.32%), and individualized counseling (Prevalence: 22.94%; 95% CI, 15.23 – 30.66%). Roughly 15% of households reported receiving help from a counselor, pastor/clergy member, therapist, case worker, or social worker to address mental health concerns (95% CI, 9.48 – 20.39%). Transportation, insurance challenges, and difficulty connecting with providers were cited as barriers for accessing care for those who needed but could not obtain care.
Community Assessment for Public Health Emergency Response, Hurricane Helene, Mitchell and Yancey Counties, North Carolina (USA): Mental Health Impacts and Stressors

* The 95% CIs around weighted prevalences are not adjusted for multiplicity and should not be used in place of hypothesis testing
Employment and Economic Impacts
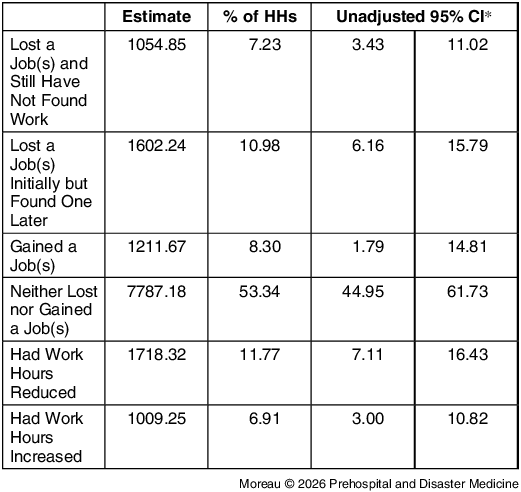
Thirty percent of households reported at least one member having negative changes in their employment (ie, job loss and found work [95% CI, 6.16 – 15.79%], job loss and still unemployed [95% CI, 3.43 – 11.02%], or reduction in work hours [95% CI, 7.11 – 16.43%]). More than one-half reported no change in their employment status (95% CI, 44.95 – 61.73%); Table 5.
Community Assessment for Public Health Emergency Response, Hurricane Helene, Mitchell and Yancey Counties, North Carolina: Changes in Employment

* The 95% CIs around weighted prevalences are not adjusted for multiplicity and should not be used in place of hypothesis testing.
Emergency Response and Recovery Resources
More than 40% of all households received some form of assistance from the Federal Emergency Management Agency ([FEMA; Washington, DC USA] 95% CI, 32.45 – 49.52%). Roughly 30% received assistance from non-profit organizations (95% CI, 22.76 – 38.50%) or church groups (95% CI, 24.18 – 40.22%); Table 6.
Community Assessment for Public Health Emergency Response, Hurricane Helene, Mitchell and Yancey Counties, North Carolina: Sources of Assistance in Hurricane Response and Recovery

Abbreviation: FEMA, Federal Emergency Management Agency.
* The 95% CIs around weighted prevalences are not adjusted for multiplicity and should not be used in place of hypothesis testing.
Author Contributions
MS and JAH planned the research, selected the sample, adapted the survey, and trained data collectors. Data were collected by SEARCH volunteers. Data were entered, cleaned, and analyzed by LM and SES. JAH drafted the manuscript and all authors edited and approved the final submission.
Use of AI Technology
No AI technology was used for constructing this manuscript.
Conflicts of interest
Sustaining Essential and Rural Community Healthcare in Western North Carolina has no financial or non-financial competing interests. Lilly Moreau has no financial or non-financial competing interests. Matt Simon has no financial or non-financial competing interests. Sarah E. Scales has no financial or non-financial competing interests. Jennifer A. Horney has no financial or non-financial competing interests.
Supplementary Materials
To view supplementary material for this article, please visit https://doi.org/10.1017/S1049023X26108863








 Open access
Open access