


1. The challenge of health and social care financial sustainability
How much we can afford to spend on public services, including health and social care, is a hot topic. In the context of fiscal tightening, widening health inequalities and an ageing population, questions inevitably turn to the impacts of demographic change on the fiscal sustainability of public services, in particular health and social care (Charlesworth and Raymond, Reference Charlesworth and Raymond2025; Warner and Zaranko, Reference Warner and Zaranko2025). Recent projections from the Office for Budget Responsibility (OBR) for the United Kingdom as a whole suggest that ’it will be difficult to move to a more sustainable path for public debt‘ (Office for Budget Responsibility, 2024). Based on their latest projections, the Scottish Fiscal Commission recently concluded that Scottish devolved public spending is unsustainable, particularly because of the projected growth of health and social care spending (Scottish Fiscal Commission, 2025). The Commission added the proviso that improvements in population health could ease fiscal pressures, echoing themes developed by Derek Wanless over 20 years ago, that health and spending trajectories are not the inevitable result of an inexorably ageing population (Wanless, Reference Wanless2002, Reference Wanless2004).
How much do we really know about the implications of demographic change for future health and social care costs? Models of future spending often apply current rates of spending by age to forecasts of demographic change and project rapidly rising spending due to an ageing population. Similarly, models of need and demand pressures on spending apply higher disease burdens by age to an ageing population and consequently predict rising demand (Public Health Scotland, 2022). These analyses often rely upon six important assumptions (Table 1).
Six important assumptions often used in considering the future financial sustainability of health and social care

Table 1. Long description
The table consists of two columns and six rows of data.
Row 1. Assumption 1. The population of the United Kingdom and similar countries will continue to age into the future.
Row 2. Assumption 2. Population health and well-being are functions of population age.
Row 3. Assumption 3. Health and social care needs are driven by the health and well-being of the population.
Row 4. Assumption 4. Health and social care spending is driven by age-related population needs for health and social care.
Row 5. Assumption 5. Inequalities are unimportant in estimating future costs.
Row 6. Assumption 6. The increase in the elderly population relative to the size of the working population, known as the dependency ratio, will put pressure on fiscal sustainability.
Assumption 1, which is rarely questioned, is that population ageing will continue. Assumptions 2–5 together imply that health and social care spending is a function of age-driven needs. Assumption 6 concerns the implications of ageing for the proportion of the population that is of working age. Together, these assumptions underpin the concern that population ageing threatens fiscal sustainability.
Some time ago, Charles Normand argued that this concern reflected one of 10 ‘Economic Fallacies’, saying that:
[The assumption that] ‘The ageing of the population will lead to a dramatic increase in health care costs’ [is] Probably wrong. The mistake is to look at costs of care by age, and model how increasing the number of elderly people might increase the total cost. (Normand, Reference Normand1998)
This paper builds on and broadens Normand’s argument, highlighting other factors that may be more important drivers of healthcare spending. In the rest of the paper, we unpack the ‘mistake’ identified by Normand, exploring the validity of, and uncertainties around, the assumptions underpinning these concerns. We then propose three hypotheses as further areas for future research that might help clarify the reality of health and social care financial sustainability.
2. Prelude: on need, supply and demand for (health and social) care
Before discussing the details of the assumptions, it is important to clarify what is meant by need, supply and demand for (health and/or social) care, as this is critical to understanding how demographic and epidemiological trends could and should relate to future spending. Need is often defined as the ‘capacity to benefit’ (Lewis et al., Reference Lewis, Sheringham, Kalim and Crayford2008). This capacity to benefit relates to changes in important outcomes arising from treatment and care (e.g. improvements in health measures, mortality and satisfaction). Crucially, the capacity to benefit depends upon, and varies with, the effectiveness of new and existing technologies, knowledge and provision. In this framing, where there is an absence of a known effective approach to prevention or treatment, a need for treatment does not exist: people do not ‘need’ ineffective care. However, when effective approaches emerge (e.g. with the invention of a new vaccine), the capacity to benefit (i.e. the need) emerges. Designing and implementing policies, services and interventions to address these needs effectively, cost-effectively and equitably is a core task of public health professionals. Needs can be divided into those which are ‘met’ and ‘unmet’, representing whether or not the population has received effective treatment or care.
The supply of care is clearly different from need but is ultimately what determines spending. Supply in this context relates to the services and interventions provided for a population. For governments and the public sector, this is orientated towards meeting as many needs as possible within (budget or other) constraints, whilst minimising supply that does not meet actual needs, for example, due to waste or because treatment is ineffective. This may not always be the case for actors with other motivations. For example, private providers may seek to supply wherever this attracts profits, and this may or may not be aligned with the meeting of needs (e.g. through the provision of ineffective medical ‘supplements’ or treatments).
Demand relates to the request for care from the population. The extent and nature of demand have a relation to health literacy. Better-informed individuals might request or engage in care that evidence shows effectively meets their needs, but may not seek or may choose not to engage with suggested care where it does not. Where demand arises for services and interventions that meet needs, this is often termed ‘expressed needs’. Demand that is somehow artificially created by supply beyond the level that would be demanded by a fully informed consumer is often termed ‘supplier-induced demand’ (Donaldson and Gerard, Reference Donaldson and Gerard2005; Lewis et al., Reference Lewis, Sheringham, Kalim and Crayford2008). The extent of supplier-induced demand will depend on the financial and professional incentives embodied in the way care is financed, organised and regulated.
Differentiating between need, supply and demand is critical for any discussion of the financial sustainability of care. Unlike the market for many economic goods, imperfections in this arena are profound relative to the conditions for markets to operate efficiently (Donaldson and Gerard, Reference Donaldson and Gerard2005). Individuals (and indeed governments) struggle to know what their needs are or identify how best to meet them. In the absence of direct measures of need, in the form of incidence and prevalence data and an understanding of what would most effectively address (or prevent) incident and prevalent disease, we often have to rely on service use data. For the reasons discussed earlier, service use is not the same as need. Analyses can become circular if we infer what we should spend in order to meet needs from what we currently spend based on existing supply. As we discuss further below, we hypothesise that health and social care spending trends are much more about decision-making in relation to supply than about demography- or epidemiology-related changes in need over time.
Assumption 1: The population of the United Kingdom (and similar countries) will continue to age into the future.
The core assumption underpinning much of the concern about the future financial sustainability of health and social care is that the population is ageing, and that future population projections suggest that this trend will continue for many decades to come. The implications of this are twofold. First, with more older people in the population (in absolute and relative terms), there will be greater care needs (see Assumptions 2–4 below), and second, there will be fewer people of working age to pay taxes and work in health and social care, thereby increasing the dependency ratio (see Assumption 6).
Yet, the history of population forecasting is not promising in this regard. Although the population of high-income countries has undoubtedly aged over many decades (Abd-Allah et al., Reference Abd-Allah, Adebayo, Agrawal, Alam, Alicandro, Almasi-Hashiani, Alumran, Alvis-Guzman, Aminorroaya, Androudi, Anjomshoa, Ansari-Moghaddam, Ärnlöv, Bahrami, Bisignano, Briko, Bumgarner, Caetano dos Santos and Callender2020), the accuracy of population projections for the United Kingdom has been poor (Appleby, Reference Appleby2014). For example, the estimated population of the United Kingdom at mid-2022 was 67.6 million. The 1981 population projection for mid-2022 was 59.3 million (8.3 million lower than the actual mid-2022 estimate). In-migration was the biggest source of error, but there were also large overestimates in predicted births that were largely offset by underestimates in projections of mortality (Office for National Statistics, 2025). Each of these errors might affect projections of the dependency ratio (migrants being younger on average).
Recent mortality trends also highlight how challenging (and wrong) projections can be. Mortality trends changed radically to much slower (or non-existent) rates of improvement after 2012 across many high-income countries, including the United Kingdom, because of economic austerity (Walsh and McCartney, Reference Walsh and McCartney2025). This change in average mortality trend obscures important differential impacts. Although almost every age and sex group has seen mortality trends change, the impact has been much worse for populations living in more disadvantaged circumstances, with life expectancy declining rapidly for the 20% of the population living in the most deprived areas of the United Kingdom (de Haro Moro et al., Reference de Haro Moro, Schofield, Munoz-Arroyo, McCartney and Walsh2025). Although more difficult to measure accurately, there is also evidence that morbidity has worsened in the United Kingdom over a similar period. This is true in relation to both Healthy Life Expectancy (HLE, a combination of mortality and self-reported health) (Walsh et al., Reference Walsh, Wyper and McCartney2022) and self-reported mental ill-health (Zhang et al., Reference Zhang, Gagné, Walsh, Ciancio, Proto and McCartney2023). In addition, there are cohort effects, whereby particular generations have better or worse health trends (Hiam and Dorling, Reference Hiam and Dorling2024), along with marked difficulties in estimating and projecting the burden of disease given the reliance on healthcare use data to do so (confusing need, supply and demand).
The implications of this are profound. We know much less than we generally think about future mortality trends, never mind morbidity trends. Mortality inequalities are widening in the United Kingdom, with mortality increasing for our most disadvantaged populations. Future trends are likely to be heavily influenced by economic policy decisions, as well as migration policy (which, in the United Kingdom context, determines how many generally younger and healthier people are allowed into the country). Using Assumption 1 given this context is brave. The implications it has for estimates for future care spending require robust interrogation.
Assumption 2: Population health and well-being are functions of population age.
Building on Assumption 1, that the population will continue to age, Assumption 2 is that population health and well-being are a function of age, implying that an older population will be less healthy. Broadly speaking, Assumption 2 holds, although quantifying the effect this has on need and cost is challenging without recourse to measures of supply or demand (e.g. medical diagnoses and accessed social care) and the confusion they can cause. Notwithstanding these challenges, the prevalence of most medical conditions increases with age (Abd-Allah et al., Reference Abd-Allah, Adebayo, Agrawal, Alam, Alicandro, Almasi-Hashiani, Alumran, Alvis-Guzman, Aminorroaya, Androudi, Anjomshoa, Ansari-Moghaddam, Ärnlöv, Bahrami, Bisignano, Briko, Bumgarner, Caetano dos Santos and Callender2020; Public Health Scotland, 2022), as does health and social care use.
However, a counter-argument has been made that health deterioration (and associated spending) is better understood in terms of time-to-death, rather than with ageing per se (although these are clearly related). The time-to-death thesis is that, on average, people spend X years in ill health before dying, rather than people becoming ill after age Y, such that people who live longer do not necessarily make more use of health and social care across their life course.
More importantly, the relationship between age and health, or time-to-death and health, is not fixed; it is a function of how healthily we age. The mistake often made in forecasts of spend is to assume, as noted earlier, that the relationship between age and health is static and to project costs into the future based on estimates of demographic change and current rates of mortality and morbidity. This is a strong assumption as:
…age-based projections are only valid when it is implicitly assumed that increases in life expectancy [as a proxy for population morbidity] do not change the relationship between age and the onset of health problems (de Meijer et al., Reference de Meijer, Wouterse, Polder and Koopmanschap2013).
In practice, the age:health relationship is subject to change. In the past, this has led some commentators to be quite sanguine about the effects of an ageing population. Normand argued that:
… it is unlikely that ageing per se will have a dramatic effect … [because] the patterns of morbidity are also changing so that the health of a person is likely to be improving at any age … (Normand, Reference Normand1998).
This phenomenon is called the compression of morbidity, the notion that reduced exposure to health risks such as smoking or poverty can reduce the time spent living with ill health.
Whilst it is true that patterns of morbidity are changing, two factors suggest we are not currently in a situation where pressures on the health and care system will fall due to compressed morbidity. First, even if health at any given age was improving, this would not necessarily be sufficient to avoid the pressures arising from an increasingly elderly population, given that the prevalence of morbidity is a function of both age-specific incidences of illness and the number of people in each age category. For example, the REAL Centre project an increase in the number of people living with a major illness by 2040 (an increase of 37%, 80% of which is for those aged 70+ years), even if the incidence of illness by age is more or less stable (Watt et al., Reference Watt, Raymond, Rachet-Jacquet, Head, Kypridemos, Kelly and Charlesworth2023). Second, trends in self-rated health (which are used to estimate HLE) demonstrate marked deterioration since around 2012, indicating that people are living longer in ill health, demonstrating an expansion, rather than compression, of morbidity (Walsh et al., Reference Walsh, Wyper and McCartney2022). Accordingly, the OBR projects a partial expansion of morbidity, assuming half of the life expectancy gains will be spent in good health and half in ill health (Office for Budget Responsibility, 2024).
Nevertheless, Normand is right to highlight that if the population’s health is improving, projections based on the assumption that current age-specific incidences will be the same in the future will overestimate future levels of illness. Although Normand downplayed the importance of the impact of ageing per se on the demand for and cost of health and social care, he acknowledged the importance of healthy ageing:
It is much more probable that the effects of ageing will be … modest …, mainly as a result of some increase in the overall amount of non-life-threatening chronic disease. (Normand, Reference Normand1998)
The OECD also emphasised the importance of morbidity as the population ages, but is less optimistic than Normand was about the effects of current health trends, highlighting:
Upside risks related to extension of the typical pre-death period of ill health as longevity increases, …and increased dependency due to obesity trends or dementia suggest[ing] that the projections provide a lower bound in the absence of more ambitious cost containment policies (de la Maisonneuve and Oliveira Martins, Reference de la Maisonneuve and Oliveira Martins2013).
More generally, as de Meijer et al point out, it is not age per se that is important; it is the illness associated with age, which is likely to change with changes in the health of the population:
the direct effect of ageing … depends strongly on underlying health and disability …age is a predisposing determinant that is not directly responsible for utilisation of health care. Instead, it is the relationship between age and need determinants such as health and disability that explain the age pattern of health expenditures (de Meijer et al., Reference de Meijer, Wouterse, Polder and Koopmanschap2013).
Other international studies argue the same point (Nozaki et al., Reference Nozaki, Kashiwase and Saito2017; Williams et al., Reference Williams, Cylus, Al Tayara, Roubal, Tsilaajav and Barber2022). Ageing increases pressures on the health system due to the higher prevalence of illness and disability in older adults, but those increases can be moderated if the population ages more healthily and HLE increases.
Assumption 3: Health and social care needs are driven by the health and well-being of the (elderly) population.
Clearly, to an extent, the assumption that health and social care needs are driven by the health and well-being of the population is true. However, the challenge for understanding the relationship between the need for (and cost of) health and social care and the underlying health and well-being of the population is that measures of health and well-being don’t tell us what people need nor what they might want from a health and social care perspective.
A health need in the sense of an illness requiring treatment doesn’t necessarily equate to a service need in the sense of there being a treatment option from which a person with the illness has a capacity to benefit, either clinically, or in terms of whether their perception of the likely balance of positive and negative effects mean that they would choose (or demand) the treatment in preference to a more conservative care regime. The ‘Realistic Medicine’ policy approach in Scotland highlights the risk of overtreatment, including where patients receive more intensive medical care than care professionals would choose for themselves or their loved ones. This reflects pressures in the system that encourage people to consume more medical care than they might need or want (Chief Medical Officer, 2016). Through this lens, what might appear to be a met ‘need’ reflected in use of services could actually be overtreatment relative to what would have been requested by a fully informed patient. In this context, a decision not to treat, or a decision to meet need in a less invasive or costly way, would be a good decision rather than an indicator of healthcare failure or unmet clinical need.
In addition, for any given level of health and pattern of illness in the population, the array of treatment and care options that people need in the sense of there being a capacity to benefit, changes (increases) as new technologies are developed. Technology, therefore, can increase costs by creating additional capacities to benefit from care and generating new needs. This is an important way in which technology can drive increased spending, rather than leading to increases in technical efficiency with the potential to reduce costs. It might also pose challenges to allocative efficiency if technological developments are subject to diminishing returns, such that there are generally smaller health gains (and more iatrogenic harms) from newer treatments than in the past (Hensher et al., Reference Hensher, Canny, Zimitat, Campbell and Palmer2020, Reference Hensher, McCartney and Ochodo2024). Even where they are effective in improving life expectancy, the OBR suggest that many medical advancements in the last 30 years have prolonged the average time in which people live with chronic ill health (Office for Budget Responsibility, 2024).
Therefore, the relationship between population health, needs and demands varies over time and reflects policy and (ideally) informed public choices based on the risks and benefits of the care available. It is also shaped by the political and economic interests served by different models of care and the development of new technologies. It is, therefore, overly simplistic in our view to assume that health and social care need is largely or solely a function of the health of the population. We return to this point below.
Assumption 4: Health and social care spending are driven by age-related population needs for health and social care.
The discussion around Assumptions 2 and 3 highlights why the relationship between an ageing population and the need for care is not straightforward. Assumption 4 is that ultimately, needs drive spending. In this section, we question whether this is the case. In suggesting it is not, we also point to alternative drivers of spend that are arguably more powerful than age-driven needs for care.
2.1. Mediators in the age:spending relationship
Earlier, we introduced the suggestion that health care needs and associated spending may be driven by time to death rather than age per se. This argument led Normand to downplay the impact of ageing on health and social care costs:
…the cost of services is related to proximity to death more than age, and it seems to be the case that the cost of terminal illness falls with age (correcting for cause of death). The expensive care is normally the care of the last illness, and we only die once. (Normand, Reference Normand1998)
Zweifel et al. (Reference Zweifel, Felder and Meiers1999) found that health care spending depends on time to death rather than calendar age. They concluded that the positive relationship between age and health care spending may be caused by the fact that in older age groups, many more people are in the last years of their lives and inferred that population ageing might contribute much less to growth in health care spending than is often assumed. Several studies have shown that projections based on the assumption that costs of care are concentrated close to death reduce the projected impact of an ageing population, by as much as 50% in a study by Bjorner and Arnberg (2012) cited by Melberg and Sørensen (Reference Melberg and Sørensen2023), compared to analyses based on the ‘naïve’ assumption that current incidence rates by age (and, therefore, levels of spending by age) continue into the future. Furthermore, several studies indicate that end-of-life costs decrease significantly the older the age at which we die (Brockmann, Reference Brockmann2002; Lubitz and Riley, Reference Lubitz and Riley1993; Polder et al., Reference Polder, Barendregt and van Oers2006), which, in turn, would mean that as the population ages and more people die at an older age, health care costs would fall. For predictions over a longer time horizon, the effect of this could be quite strong, such that if a large share of the population were to move into age categories where the last year of life is significantly less costly, ageing of the population would produce a large cost saving.
However, the implications of the evidence on the impact of time to death on health care spending are uncertain. More recent analyses (Zweifel, Reference Zweifel2022) suggest that the strength of the association between health care spending and time to death depends on the assumptions made, the methods used and the definition of health care expenditure used. Howdon and Rice (Reference Howdon and Rice2018) analysed secondary care expenditures and found support for the hypothesis that time to death rather than age drove expenditures, but that time to death is acting as a proxy for morbidity. Their work underlines the importance of considering morbidity in projections of healthcare expenditure, rather than age per se, and of the potentially severe consequences of an expansion of morbidity with people experiencing more years in ill health.
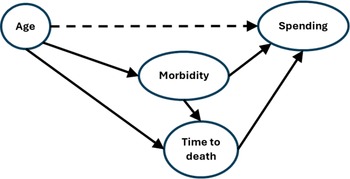
It is also important to be clear that controlling for time to death and/or morbidity and finding that the independent effect of age is diminished should not be taken to imply that an older population will not generate more spending by the health and social care system. Figure 1 depicts a simple directed acyclic graph (DAG) showing the relationships between these variables.
Directed acyclic graph of the relationship between age, spending, morbidity and time to death.

The dashed arrow highlights the commonly observed association between age and health care spending. The pathways through morbidity and time to death show how the above analyses ‘explain away’ the age-spending relationship by adjusting for time to death and morbidity. If we are interested in the effect of age on spending, adjusting for morbidity or time to death over-adjusts the total effect by blocking those pathways, assuming age is a determinant of both morbidity and time to death, both of which are safe assumptions to make. The correct interpretation is not that age doesn’t matter in terms of its impact on spending; it is that age exerts an effect on spending through time to death and morbidity.
Both these pathways point to areas where policy and practice have scope to intervene to change the ultimate effect of age on spending. These relationships between age, time to death and cost of care are not fixed. First, to the extent that better prevention can help the population age more healthily, then the age–morbidity relationship can be weakened. Second, the age:‘time to death’:expenditure pathway reflects choices between models of care at different stages of the life course, whose costs and appropriateness vary:
Another reason for high end of life costs is the (ultimately unsuccessful, and often inappropriate) hospital treatment of the primary cause(s) of death (Normand et al., Reference Normand, May and Cylus2021).
This points to the need to consider how the needs of older populations are met and the impact this has on the costs of an ageing population (Chief Medical Officer, 2016). Third, both pathways are influenced by political choices about the level of funding in the system. This comes back to some of the challenges mentioned in the prelude about inferring need and demand from patterns of service use in a supply-constrained health and social care system.
2.2. Alternative drivers of health and care spending
There is a strong case that trends in health and social care spending should be determined by trends in population need, reflecting both trends in health and illness in the population and technological developments which generate new ‘capacities to benefit’. As our knowledge of how to improve health increases, it might be expected that spending will generally increase, subject to the possibility that technological development may be subject to diminishing returns (Hensher et al., Reference Hensher, Canny, Zimitat, Campbell and Palmer2020, Reference Hensher, McCartney and Ochodo2024).
Yet it is not at all clear that spending is determined by need. Here, we highlight two other important drivers of spend. First, the risks of a ‘medical-industrial complex’, whereby governments become trapped in high levels of spending through the power of a medical industry sector, are well recognised (Grouse, Reference Grouse2014; Relman, Reference Relman1980). Within the NHS there are institutional safeguards in place which are designed to prevent spending on ineffective or cost-ineffective healthcare, such as the cost-effectiveness threshold used by the National Institute of Health and Care Excellence, or NICE, although recent proposals to give Ministers more powers to set the threshold ‘to take into account a broader range of factors, such as industrial policy objectives, economic growth and investment’ are likely to raise the threshold and weaken this mechanism (Department of Health and Social Care, 2025). Insurance-based healthcare systems have similar protections. Yet, perverse incentives remain for health and social care industries to create treatments that are costly yet ineffective; research ameliorative treatments that will generate ongoing revenue streams rather than curative or preventative treatments (e.g. daily medication); and/or misuse or fund fraudulent research (Angell, Reference Angell2005; Goldacre, Reference Goldacre2012).
Second, levels of spending are largely a political decision, driven in part by a view on the level of need, but mainly by arguments relating to (1). the impacts on wider economic and social objectives of the ways of generating the money required to fund spending on health and social care, that is, taxes and borrowing; and (2). the relative value and importance of health and social care compared to other uses of public money. The outcome of these decisions historically has been that aggregate demand for health and social care outstrips supply, and this requires that service provision is limited by policy and institutions in different ways. These include toleration of unmet need, risks and lower service quality; the use of waiting lists or other rationing tools; restrictions on the range of interventions available to health and social care providers; and creation of cultures or social contracts whereby demand for services from the public is limited. These ‘strategies’ affect the perceptions of the gap between demand and supply and can generate pressures to spend more on health and social care as people demand additional spending through the democratic mechanisms available to them. For example, the large increase in health and social care spending in the period 1997–2010 by the United Kingdom ‘New Labour’ government was clearly a political decision to meet what was perceived to have been a large amount of unmet need, exemplified by hospital waits (Crisp, Reference Crisp2023). However, views legitimately differ on whether we should spend more on health and social care, either by raising more money through taxation and/or borrowing, or by allocating more of the available public money to health and social care. We would suggest that the level of spending reflects the outcome of these debates rather than changes in need.
In summary, Assumptions 2–4 oversimplify and mis-specify the main drivers of healthcare spending. Although trends in age-related population needs are clearly relevant, they are not the only nor the most powerful drivers of spending trends. Jayawardana et al. (Reference Jayawardana, Cylus and Mossialos2019) assessed the impact of an ageing population and concluded that although the elderly, on average, are heavier per person users of care, the proportion of the population at the oldest and most costly age groups increases very slowly over time, even if it is assumed that the health of the elderly will generally be worse in the future under an expansion of morbidity scenario. The result of their modelling is that the changing needs arising from the changing age structure of the population will only lead to slow growth in total healthcare spending over time. They also argued that decisions around the adoption of new technologies have been and will continue to be one of the main drivers of growth in health care expenditure, along with prices paid for healthcare. Both, they suggest, are amenable to policy intervention, and both are consistent with our emphasis on the supply-side drivers of healthcare expenditure.
Assumption 5: Inequalities are unimportant in estimating future costs.
Projections of need, demand and spend across populations as part of Assumptions 1–4 often focus on population averages and fail to take into account health inequalities, even where their potential importance is acknowledged (Office for Budget Responsibility, 2024; Public Health Scotland, 2022; Scottish Fiscal Commission, 2025). There are exceptions, and the conclusions drawn by those who do not assume inequalities are unimportant are instructive. For example, the Christie Commission, which examined the financial sustainability of public services in Scotland in 2011, concerned itself particularly with ‘failure demand’ (Christie, Reference Christie2011):
the consequences of disadvantage impose significant financial burdens on public services and society in general… High levels of public resources are devoted annually to alleviating social problems and tackling ‘failure demand’ – demand which could have been avoided by earlier preventative measures.
This foregrounds that health and care needs, and therefore potentially costs, are observed unequally across social groups, and that these needs are caused in large part by the societal context in which populations live (McCartney et al., Reference McCartney, Collins and Mackenzie2013). At the current time, it is difficult to argue that inequalities don’t affect the sustainability of health (and wider public) spending, given that mortality trends are diverging across social groups in countries like the United Kingdom, and mortality and morbidity rates are increasing in more disadvantaged areas of the United Kingdom in an unprecedented change in long-term trends (de Haro Moro et al., Reference de Haro Moro, Schofield, Munoz-Arroyo, McCartney and Walsh2025; Walsh et al., Reference Walsh, Wyper and McCartney2022).
Assumption 6: The increase in the elderly population relative to the size of the working population (the dependency ratio) will put pressure on fiscal sustainability.
Assumptions 1–5 relate to factors driving need and demand for health and care services.
Assumption 6 relates to the ‘supply-side’, specifically the concern that demographic change will increase the proportion of the elderly in the population and reduce the population of working age, thereby shifting the balance between those making heavier use of services funded by tax revenue and those generating tax revenue on which the supply of services depends. This increases the ‘dependency ratio’ (the ratio of the size of the population not in the labour force to the population within it). It is closely linked to Assumption 1, that populations will age into the future.
Although there is a clear logic to this assumption, its implications have been questioned. First, changes in productivity with technological development (in particular with the development of computing, the internet and Artificial Intelligence (AI)) might mean that each worker can produce more in the future. For some writers, this holds the prospect of a post-work society (Hester and Stronge, Reference Hester and Stronge2025) or ‘luxury communism’ in the future if such technologies can be owned and used for the public good (Bastani, Reference Bastani2019).
Second, notwithstanding the assumptions above, population ageing holds the prospect of increasing both the number of people in need of care and the number of ‘… more informal carers who are fit and able to help’ (Normand, Reference Normand1998). Furthermore, there may also be positive impacts on the formal economy through, for example, the positive impacts on productivity as a result of working-age people being enabled to enter the labour market by (healthy) older people providing help to parents or others with caring duties, and potentially more older people remaining in work for longer, especially if morbidity is compressed and people remain healthier for longer.
3. From assumptions to hypotheses: towards a research agenda
Given the centrality of the six assumptions (or their counterparts) listed above for understanding the future fiscal sustainability of providing health and social care, there is clearly a need to increase our collective understanding of whether these assumptions hold, in what circumstances, and what the evidence for each of them suggests can be done to manage the system sustainably in the future. It is our view that future research in this area could usefully be focused on testing each of these assumptions to better understand for whom they hold, and in what contexts. We also wish to propose three hypotheses, linked to the assumptions above, for which we believe a case can be made, but which remain far from ‘proven’.
Hypothesis 1: Health and social care spend is primarily a function of political decisions on supply, not demand or need.
Building on our assessment of Assumptions 2–4 in particular, we hypothesise that health and social care spending trends are not primarily driven by population ageing nor the health of the population. Instead, we contend that spending is primarily a function of political decisions. In some ways, this is a tautological argument—that is, government spending on health and social care is determined by how much the government spends on it! But the simplicity of this argument is, in our view, too often overlooked in considerations of future spending. In short, governments spend what they want to spend or what they feel they can spend on these areas. The question instead might be better put: why do governments spend what they do on health and social care? Is it to address changing population needs, including any changes in need related to ageing, evolving health trends or technological advances? Or is it instead a political decision based on the demands of voters, lobby groups and other powerful actors? If so, to what degree do these demands relate to changing needs? What role do industry and researchers play in determining spending by creating technologies which (to varying degrees, and with varying qualities of evidence) create new needs? How do the decision-making processes vary across different models of health and social care provision, including differences in funding (out-of-pocket, insurance, tax-funded) and delivery (private, commissioned, publicly owned)? How far does the level of funding reflect wider policy debates about the impacts on the wider economy of public spending and the ways in which it is funded?
We argue that politicians have substantial agency here. In tax-funded systems, they make decisions on spending. In other systems, they set the rules and regulations by which markets operate. Moreover, they can implement different models of care which have different spending implications. Political decisions are in turn influenced by changes in population need, public demands and pressures to spend arising from the medical-industrial complex, but politicians retain substantial agency. For us, this is an important area for future research, as testing the degree to which this hypothesis holds is integral to understanding future spending trajectories.
Hypothesis 2: Policy action to reduce health and social care need through ‘prevention’ is important in improving population health outcomes, but is unlikely to reduce spending without other action.
One of the most commonly proposed ‘solutions’ to the projected increases in health and social care spending is to implement ‘preventative’ policies to improve the health of the population. This is perhaps best exemplified by the idea of ‘compressed morbidity’ described in the Wanless reports (Wanless, Reference Wanless2002, Reference Wanless2004), which describe a prevention-based, ‘fully-engaged’ scenario whereby the time spent in ill health decreases and the rate of growth in health spending is reduced even where lifespans are increasing. This is clearly reliant on the assumptions above that health and social care spending is largely a function of the health of the population. We agree that prevention is important. Primary prevention is particularly so because it holds great potential to improve health and reduce health inequalities in a highly cost-effective way (Owen and Fischer, Reference Owen and Fischer2019; Vos et al., Reference Vos, Carter, Barendregt, Mihalopoulos, Veerman, Magnus, Cobiac, Bertram and Wallace2010), especially when policies are introduced to reduce income, wealth and power inequalities in society and where tax and regulatory policies are used to reduce exposure to harms (Beeston et al., Reference Beeston, McCartney, Ford, Wimbush, Beck, MacDonald and Fraser2013; McCartney et al., Reference McCartney, Collins and Mackenzie2013). Many forms of secondary and tertiary prevention are also likely to contribute to improved population health, but care must be taken not to assume this is the case. For example, the current enthusiasm for cardiovascular risk screening in primary care in the United Kingdom by Chief Medical Officers (Whitty et al., Reference Whitty, Smith, McBride, Atherton, Powis and Stokes-Lampard2023) is not supported by the highest quality evidence (Dyakova et al., Reference Dyakova, Shantikumar, Colquitt, Drew, Sime, MacIver, Wright, Clarke, Rees and Rees2016), and interventions that require individual agency or navigating service pathways are at high risk of exacerbating health inequalities.
However, we hypothesise that such preventative actions, even where they are effective and cost-effective, are unlikely to substantially reduce pressures on health and social care spending (Craig and Robinson, Reference Craig and Robinson2019). This is based on our questioning of the assumptions detailed above, in particular Assumption 4, which suggests that spending tracks population health needs. Furthermore, even with population health improvements, we contend that substantial impacts on spending growth are unlikely because: care systems have a large number of fixed costs (e.g. clinics, care facilities, the training completed by staff in particular specialisms, technology and equipment maintenance); there are substantial unmet needs in the population that will be revealed and met if other aspects of health improve; and there are numerous vested interests in the ‘medical-industrial complex’ to maintain spending in particular areas or on particular forms of technology. In addition, the effects on healthcare spending of increases in life expectancy that might arise from prevention are mediated by changes in the care costs in the later years of life as age-at-death increases and by our health during the years of additional life expectancy. For the reasons discussed above, the balance of these factors remains uncertain.
Hypothesis 3: The best approach to achieving fiscally sustainable health and social care spending combines ‘prevention’ policies with decommodification and ‘realistic medicine’.
As noted above, preventative policies are important and necessary for improving health and reducing health inequalities. However, we hypothesise that achieving fiscal sustainability requires additional measures, aligning with the observation of the OECD, which has highlighted fiscal risks ‘in the absence of more ambitious cost containment policies’ (de la Maisonneuve and Oliveira Martins, Reference de la Maisonneuve and Oliveira Martins2013). The two key aspects of change that we hypothesise are necessary to contain health and social care spending are: decommodification of provisioning and ‘realistic medicine’.
The argument for decommodification has several aspects. As noted earlier, health and social care is a clear example of economic activity which breaches core assumptions for market provision of a service or commodity (Donaldson and Gerard, Reference Donaldson and Gerard2005). ‘Consumers’ (aka the public) are at an information disadvantage in any health and social care ‘transaction’ as they cannot be expected to know what evidence suggests are the most beneficial treatments, interventions and services. Even where insurance companies or other intermediaries are put in place to navigate information asymmetry, as in the US healthcare system, the results are often disappointing and expensive (Gunja et al., Reference Gunja, Gumas and Williams2023; Relman, Reference Relman2012). Within the United Kingdom system, with largely taxpayer-funded provisioning, the introduction of markets and quasi-markets has been demonstrated to increase costs, create inequalities in who receives services and generate inefficiencies (Pollock and Leys, Reference Pollock and Leys2004; Tudor Hart, Reference Tudor Hart2010). Health and social care systems which have large commercial interests tend towards higher spending because of the power these interests exert over decision-makers at all levels. We hypothesise that breaking this ‘medical-industrial complex’ requires decommodification, public ownership, tight regulation and effective systems for robustly evaluating the utility of technologies and services, both current and new, to ensure cost-effectiveness.
‘Realistic medicine’ is a phrase popularised by the Scottish Government which refers to an approach to health and social care provision which is more relational than transactional, and encourages fuller consideration of the balance between risks and benefits of treatments and interventions. For example, it encourages healthcare professionals to consider whether embarking on treatment courses for patients close to the end of life, or for whom the benefits are likely to be marginal, is what they would wish for themselves or their families. It also encourages deeper conversations with patients about what they want and what matters most to them from courses of treatment, and about the risks of overtreatment and iatrogenic harm. Conceptualising health and social care delivery through this lens has the potential to reduce the desire for ever more marginal gains from intervention and treatment, and to cast a more critical eye on the unintended consequences and costs of such approaches. This has the potential both to improve the experience of care and to reduce costs.
Testing the hypothesis that prevention policies, decommodification, ‘realistic medicine’ and effective systems for evaluating current and new technologies and services can contain health and social care costs is, in our view, an important and testable proposition.
4. Implications and conclusion
So how much do we really know about the implications of demographic change on future health and social care costs? The debate is polarised. Some fear that higher costs of health and social care, combined with an ageing population, threaten fiscal sustainability. Others argue that these concerns are overblown because the elderly account for a relatively small and slowly changing proportion of total health care costs and because population health improvements will increase life expectancy and compress morbidity. This has the potential to limit health and social care demand to the latter stages of life and reduce end-of-life costs if, as some have argued, these costs decrease if we die at increasingly older ages.
The truth probably lies somewhere in between, but finding where the balance lies is challenging for several reasons, some of which have been alluded to already. First, although many analyses extrapolate from current associations between demography, health and cost, current costs of responding to particular health or care needs are not necessarily a good guide to the actual costs required to meet those needs adequately and appropriately. Current costs will reflect many factors other than need that have driven historical resource allocations, such as politics and the efficiency with which resources have been used to date. As Normand put it in relation to the observation that end-of-life care is lower the older we die:
There should, however, be some concerns. It may be that the observed lower costs of terminal illness reflect undertreatment (in the sense of failure to provide cost-effective services) in older people. (Normand, Reference Normand1998)
Second, current costs are amenable to change through the choices made regarding the way services are delivered, the types of services provided (including the balance between prevention, primary care and secondary care, their cost-effectiveness and unintended harms), and the priority we attach to different uses of public resources.
Third, Greer et al. fear that framing the current debate in terms of fiscal unsustainability driven by an ageing population risks turning the debate into an argument about inequity between generations rather than inequalities within generations, with the potential to undermine political support for increasing investment in public services:
… talk of an ageing crisis is frequently just another version of longstanding arguments against public social investment from the cradle to the grave. (Greer et al., Reference Greer, Lynch, Reeves, Raj, Gingrich, Falkenbach, Cylus and Bambra2022, p. 10).
The opposite is the intention here. The aim is to acknowledge and highlight the consequences of current epidemiological and demographic trends, including the current inequalities in health, so that they can be better managed and mitigated through ‘public social investment’ that improves health trajectories throughout the life course and across the socio-economic spectrum. The extent of current pressures is such that we need to give greater priority, not primarily to policies targeted at older people, but to policies throughout the life course that enable the population to age more healthily and equitably and in a more economically sustainable way. This points to the need for more effective primary and secondary prevention, delivered in ways that reduce health inequalities, and to the provision of more appropriate end-of-life care.
More broadly, whilst it is important to consider demography and epidemiology in discussions about the sustainability of funding to meet the rising costs of health care, they are not as important in driving spending as the potential to meet a wider range of needs for more people due to technological change, the response of the political system in terms of how much money it decides to allocate to the health system, and the political structures that determine whether and how these technological possibilities are taken up. Exploiting the potential of new technologies is a good thing, and something that an increasingly wealthy country might reasonably aspire to, if the new technologies and/or increased capacity meet needs in an appropriate way. However, it increases fiscal challenges if the institutional structures within health and social care lead to supplier-induced demand for ineffective care, cost-ineffective care or care in excess of what would be chosen by a fully informed service user. We have argued that this points to the need for conceptual clarity in the debate around fiscal sustainability: cost, need, demand and supply are all related, but they are not the same and the relationships between them are not fixed. We, therefore, need to be careful in our language and assumptions when we try to work out how (fiscally and in terms of the balance between prevention, treatment and care) we should respond to demographic, epidemiological and wider economic and political pressures on the public’s health and the health system. The ageing of the population is an important factor to consider in debates about the sustainability of health and other public services, but it is not a demographic time bomb waiting to explode.


 Open access
Open access