


Introduction
Infants and children with congenital heart disease (CHD) are at a high risk of arterial ischaemic stroke secondary to anatomical, physiological, and management factors. Reference Mandalenakis, Rosengren and Lappas1,Reference Dowling, Hynan and Lo2 Neonates and infants with cyanotic heart disease requiring palliative surgery are at an especially high risk of arterial ischaemic stroke, presumably related to cerebral thromboembolic and/or hypoperfusion events. Reference Chen, Zimmerman and Jarvik3,Reference Asakai, Cardamone and Hutchinson4 Moreover, their labile clinical state and limited neurological examination secondary to sedatives and neuromuscular blockade may lead to late recognition of major neurological events. Rapid identification of arterial ischaemic stroke is essential to provide appropriate management of resulting electrographic or electroclinical seizures that are a source of morbidity and mortality and inform decisions regarding initiation or cessation of anticoagulation. Reference Mayne, Mailo and Pabst5
The gold standard for diagnosing stroke is MRI. However, use of this modality is not feasible in many critically ill patients. To overcome this significant limitation, real-time and easily-deployable monitoring modalities are necessary. Reference Chen, Zimmerman and Jarvik3,Reference Mahle, Tavani and Zimmerman6–Reference Kosiorek, Donofrio and Zurakowski11 These include amplitude-integrated electroencephalography (EEG), continuous electroencephalography, head ultrasound, and mobile head computed tomography (CT) American Clinical Neurophysiology Society guidelines recommend continuous electroencephalography (cEEG) monitoring following congenital heart surgery in young infants, and multiple studies have reported an incidence of post-operative seizures ranging from 3.8 to 18%. Reference Shellhaas, Chang and Tsuchida12–Reference Levy, Mayne and Sandoval Karamian18 The use of continuos electroencephalography remains especially important given that clinical seizures are often missed, and the majority of seizures in critically ill infants are subclinical. Reference Naim, Gaynor and Chen16,Reference Naim, Gaynor and Chen16, Reference Massey, Weinerman and Naim19, Reference Claessens, Noorlag and Weeke20 Head ultrasound is portable and can be performed at the bedside in the the Cardiac Intensive Care Unit (ICU); however, it has significant limitations in identifying neurologic injury compared to brain MRI. Reference Massey, Weinerman and Naim19,Reference Rios, Welty and Gunn21–Reference Rollins, Yoder and Moore26 A combination of multiple monitoring and imaging techniques increases the injury detection rate. Reference Massey, Weinerman and Naim19,Reference Austin, Edmonds and Auden27–Reference Gannon, Kornhauser and Gross29
Our comprehensive neuromonitoring strategy, including head ultrasound and continuous electroencephalography in the perioperative period (described further in methods) in critically ill infants with CHD was designed to overcome the limitations of physical examination and recognise neurologic cause for acute changes in vital signs. Our primary goal was to assess the arterial ischaemic stroke detection rate of our neuromonitoring strategy in critically ill CHD patients 0–6 months of age.
Methods
We conducted a retrospective cohort study of all consecutive patients 0–6 months of age who were admitted to the Pediatric Cardiac ICU at UPMC Children’s Hospital of Pittsburgh (CHP) and underwent an index cardiac operation or catheterisation from January 1st, 2016, to December 31st, 2022. Patients were identified by querying the PC4 registry and local cardiac critical care database. All patients with the diagnosis of “arterial ischaemic stroke” were our case group, while the controls were all patients without stroke. Exclusion criteria were medical cardiac ICU admission, patent ductus arteriosus ligation as the only intervention, and age >6 months during the time of index operation/procedure. Two strokes diagnosed as part of a research study with preoperative brain MRI were excluded from the analysis. There were 3 patients that neurologists determined no evidence of signs and symptoms of arterial ischaemic stroke with false positive brain image studies. We also excluded 8 patients who did not have any cardiac interventions in the 72 hours prior to the documented episodes of arterial ischaemic stroke (Supplemental Figure 1).
Cardiac ICU neuromonitoring strategy
-
1. Neonates (0–28 days): All newborns with critical CHD admitted to our cardiac ICU from the delivery room underwent screening head ultrasound to rule out midline defects or acute changes. Head ultrasound was performed in the immediate postoperative and post-cardiac catheteriaation phase. cEEG monitoring was initiated following all neonatal operations.
-
2. In 28 days–6-month-old infants, continuos electroencephalography monitoring was performed if the patients were on neuromuscular blocking agents or based on clinician preference. In the acute post-operative/procedure phase, abnormal head ultrasound or continuos electroencephalography findings or clinician concerns prompted bedside head CT. Brain Magnetic Resonance Imaging (MRI) was performed based on Neurology recommendations when clinical stability was achieved.
-
3. All patients receiving Extracorporeal membrane oxygenation (ECMO), regardless of age, receive daily head ultrasound and underwent continuos electroencephalography monitoring while on neuromuscular blockade and unstable.
Clinical data and laboratory values
Patient data were collected from the electronic health records, Pediatric Cardiac Critical Care Consortium (PC4) registry, and the local cardiac critical care database. Data collected included demographic and surgical factors, imaging results, and postoperative outcomes. Strokes within 72 hours of a procedure were assigned to the periprocedural group. Arterial ischaemic strokes were confirmed by the presence of decreased signal attenuation on head CT or cytotoxic oedema on brain MRI diffusion-weighted imaging and apparent diffusion coefficient sequences. We defined a large ischaemic stroke by involvement of the Circle of Willis including anterior, middle, and posterior cerebral arteries and branches. A small ischaemic stroke was defined as a point lesion on imaging, and multiple strokes were defined as more than one large and/or small lesion. To evaluate long-term neurologic outcomes, we conducted a chart review of the most recent cardiology and/or neurology clinic visit. If physical therapy or occupational therapy was documented, patients were assigned to the residual deficit group.
Statistical analysis
R software, Version 4.4.2 (R Foundation for Statistical Computing, Vienna, Austria) was used to perform all statistical analyses. Mann–Whitney U test was used to calculate two-sided P-values between neonatal and control variables for numerical variables. Shapiro–Wilk tests were run to assess the normality of the distribution of numerical variables. All Shapiro–Wilk tests were significant, and the sample sizes were not sufficient to use the central limit due to the extreme skew of the distributions, so non-parametric tests were used. We also created side-by-side boxplots for each numerical variable to visualise the distributions and visually verify our results. Chi-square tests were used to perform hypothesis tests between neonatal and control variables for categorical variables. A Yates’ continuity correction was applied to any test where the assumptions of a chi-squared test were violated. We also created stacked bar charts and contingency tables to visualise the distributions of each categorical variable and visually verify our results. A P value < 0.05 was considered a significant difference between the two groups. We used a lower P value to avoid the multiple comparisons fallacy.
Ethics
The Institutional Review Board of UPMC Children’s Hospital of Pittsburgh approved this study. It waived the need for written informed consent from the patients’ families, as this study involved only the retrospective analysis of clinically acquired data (IRB# STUDY19090052). This study was reviewed and approved by the UPMC Quality Review Council.
Results
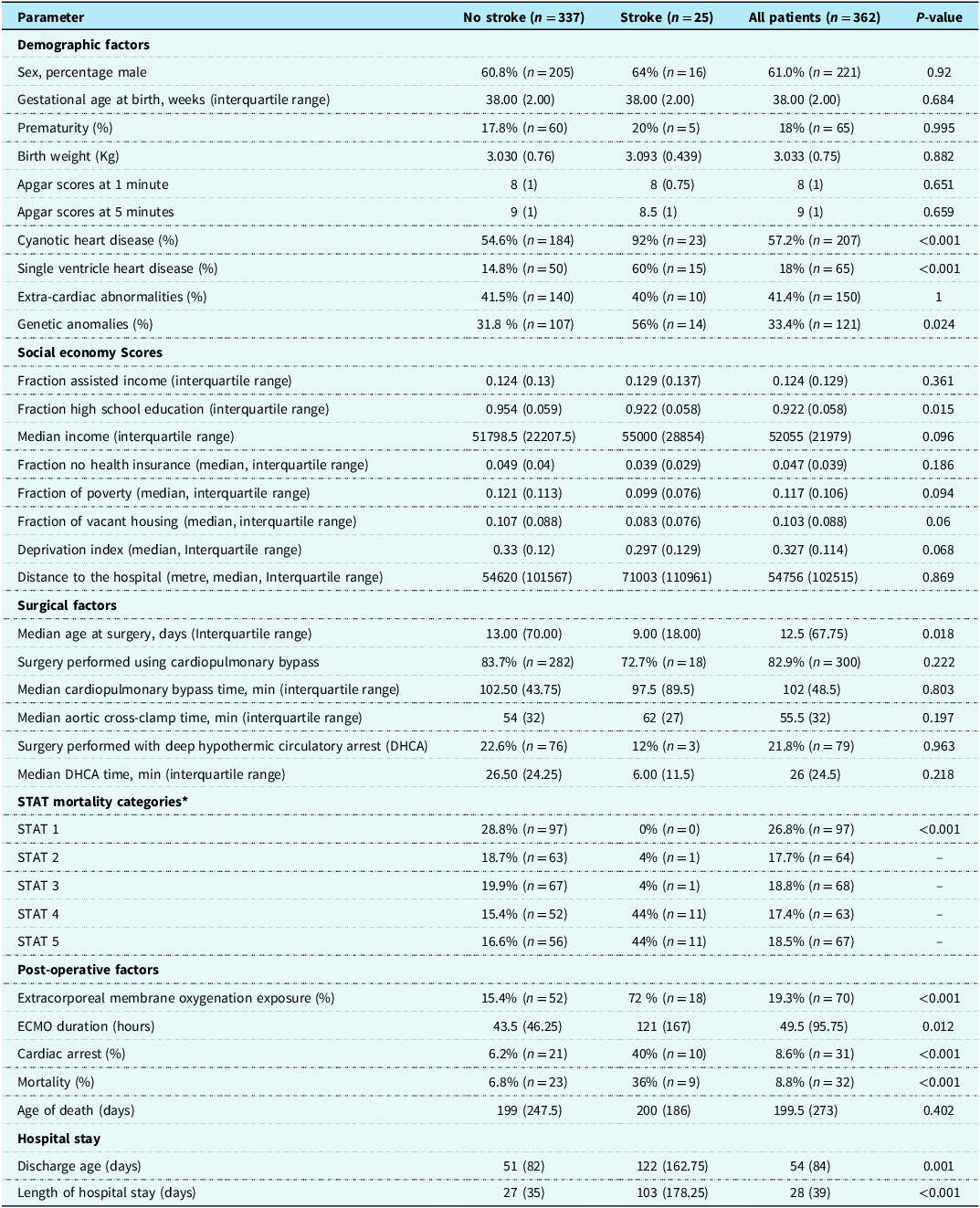
Initial review identified 403 infants. Following exclusions, 362 infants were analysed. We identified 25 patients (6.9%) with arterial ischaemic strokes within 72 hours of procedures. Four patients had 2 strokes. The control and stroke patients did not differ significantly in sex or median gestational age at birth. The stroke group patients had a trend of younger at the time of surgery, median age 9 (5, 22) days versus 12.5 (7, 77) days in the control group (P = 0.018). Patients with strokes had a higher incidence of genetic abnormalities including abnormal karyotype, microarray results or pathological variants, 56% (n = 14) versus 31.8% (n = 107) (P = 0.024) (Table 1).
Summary of demographic, surgical factors, and postoperative factors for patients included in this study

STAT Category = Society of Thoracic Surgeons – European Association for Cardio-Thoracic Surgery Congenital Heart Surgery Mortality Category.
*3 Patients have no STAT value.
Stroke patients had a higher incidence of cyanotic CHD 92% (n = 23) versus 54.6% (n = 184) (P < 0.001), single ventricle 60% (n = 15) versus 14.8% (N = 50) (P < 0.001), and a higher incidence of hypoplastic left heart syndrome 44% (n = 11) versus 8.6% (n = 29) (P < 0.001) (Table S1). 88% (n = 22) of stroke patients underwent STAT 4 or 5 operations versus 32% (n = 108) of control patients (P < 0.001). There was no statistically significant difference in median CPB time (P = 0.803) and median aortic cross-clamp time (P = 0.197). There was no difference on the use of deep hypothermic circulatory arrest: 12% (n = 3) in stroke group versus 22.6% in controls (n = 76) (P = 0.963), nor deep hypothermic circulatory arrest time: 6 minutes (5.5, 13) in stroke group and 26.5 mins (9, 33.25) in controls (P = 0.218) (Table 1).
More stroke patients suffered cardiac arrest [40% (n = 10) versus 6.2% (n = 21) (P < 0.001)] and underwent ECMO support [72% (n = 18) versus 15.4% (n = 52) (P < 0.001)] and longer ECMO duration 121 hours versus 43.5 hours (P = 0.012). Mortality was higher in the stroke group, 36% (n = 9) versus 6.8% (n = 23) (P < 0.001). Three patients withdrew support due to embolic strokes while on ECMO support, among them, one patient had haemorrhagic conversion.
There was no statistical significance in the social–economic index between control and stroke groups except the stroke group had less parents finishing high school education (P = 0.015) (Table 1).
Clinical signs
Thirteen episodes of embolic strokes were identified as a part of routine post-procedure or ECMO monitoring with head ultrasound(n = 5) and continuos electroencephalography (n = 8). Clinical signs prompted imaging that identified a stroke in less than half of the episodes (11 of 25) and clinical signs concerning for a focal neurologic process or clinical seizure occurred in less than one-third (5 of 25) of our patients (1 with clinical seizures and 4 with a focal neurologic deficit). Six patients presented with non-specific clinical signs that prompted imaging. In one case, a new stroke was identified on serial monitoring due to a known previous neurologic insult (Figure 1). Brain MRI identified bilateral thalamic infarct in a patient with unexplained agitation.
Summary of clinical signs or management decisions leading to imaging that identified a stroke.

Performance of imaging modalities
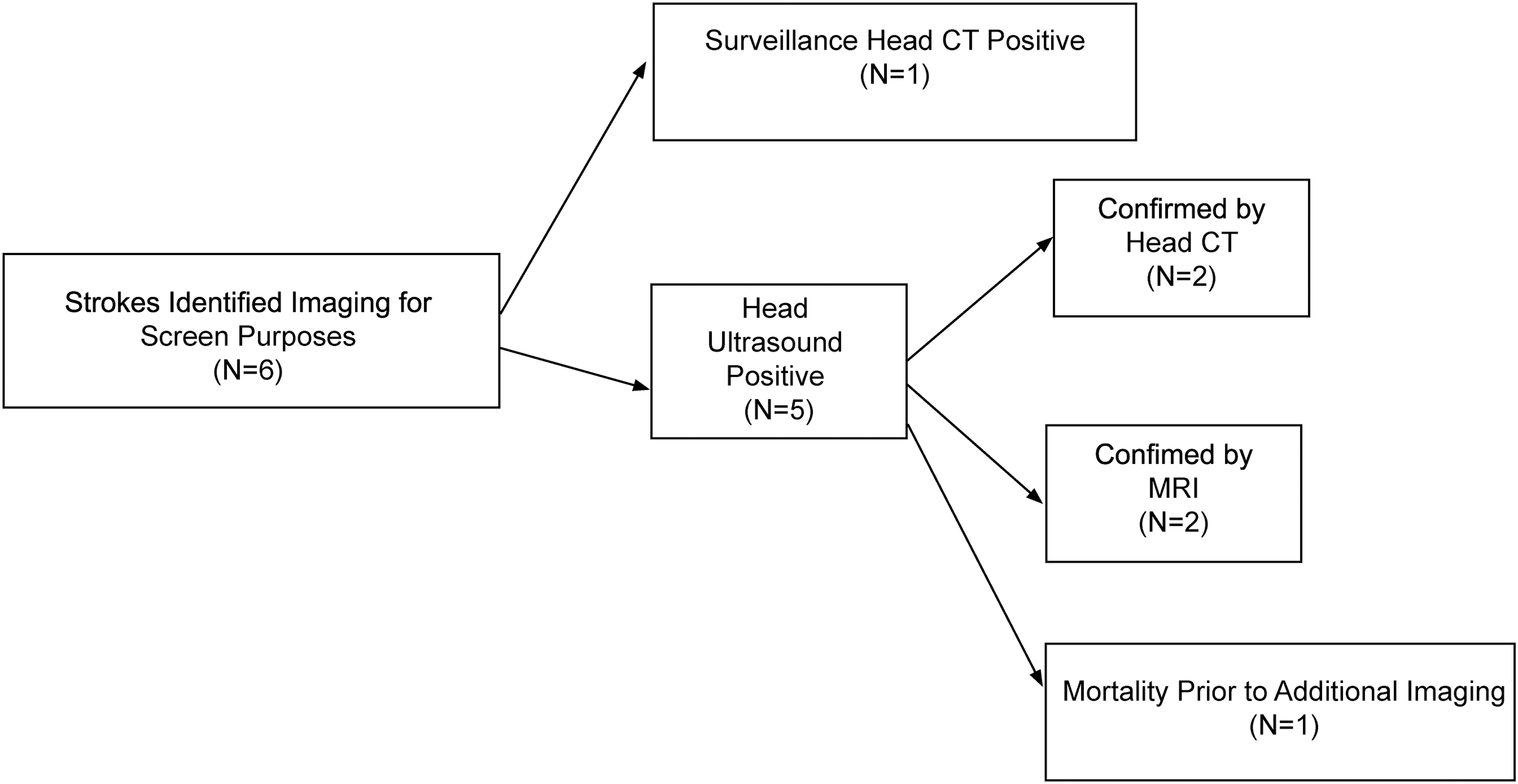
Imaging prompted by clinical symptoms or subclinical seizure on continuos electroencephalography identified 19 episodes of stroke. Of those 19 episodes, 1 had a positive MRI, 8 had a positive head CT, and 13 underwent head ultrasound: 10 were positive and 3 were negative with positive follow-up head CT (Figure 2). In one episode, embolic stroke was identified as part of serial head CT monitoring (Figure 3). Taken together, a head ultrasound first diagnosed 60% of strokes (15/25); 36% (9/25) were diagnosed by head CT, the remaining 4% (1/25) were diagnosed by MRI. Head ultrasound predominantly identified strokes in midline structures.
Performance of various imaging modalities when there was a clinical concern for a cerebrovascular insult, including focal neurologic findings, positive cEEG, non-specific symptoms. cEEG, continuos electroencephalography.

Performance of imaging modalities utilised to screen for stroke.

Events prior to stroke
Of the total, 25 episodes of stroke were associated with a procedure in the preceding 72 hours. Twenty-three (92%) episodes of embolic stroke were associated with cardiac procedures (18 cardiac operations, 14 cardiac catheterizations, 14 episodes of strokes were identified while patients were on the ECMO support (some patients were exposed to multiple interventions) and 16 of the stroke patients had an additional unplanned procedure beyond the initial intervention (Table S2).
Neurologic outcomes
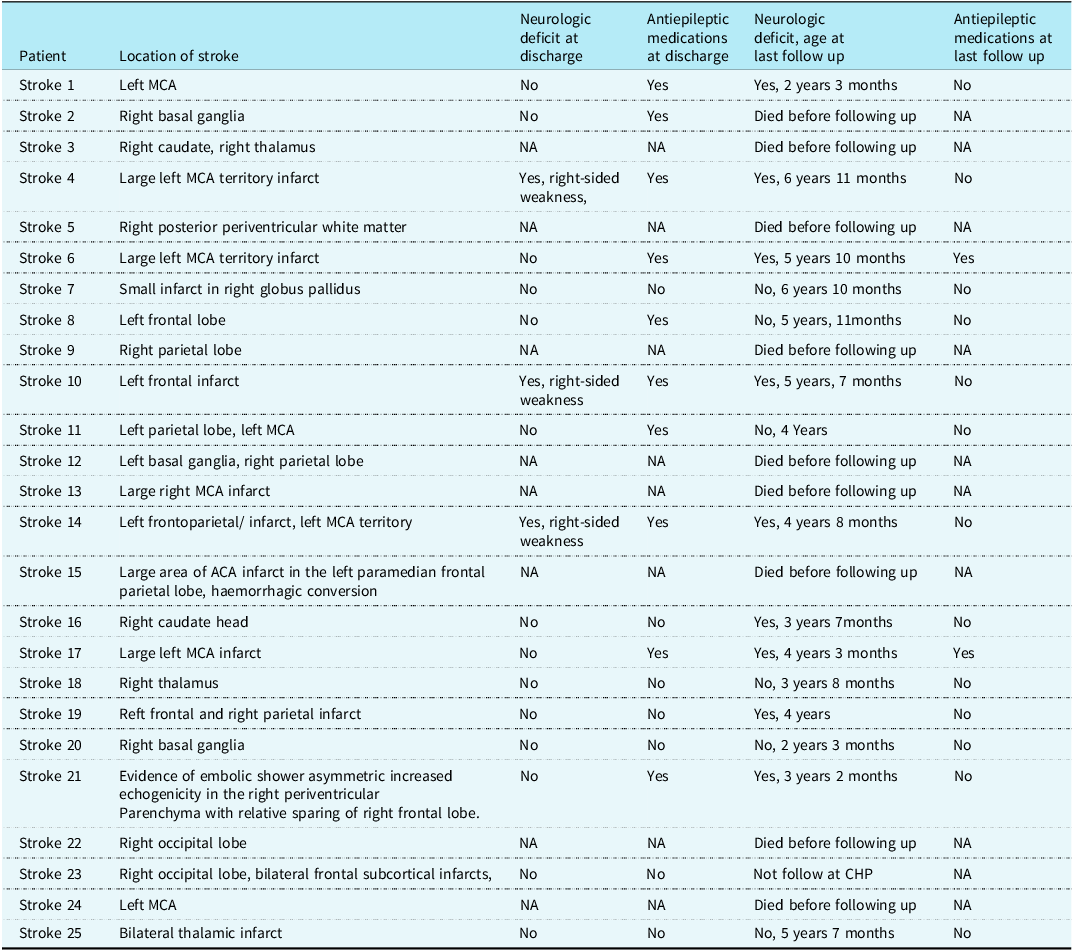
The average discharge age of 16 stroke survivors was 123 days old. The stroke group had a longer hospital stay (103 days versus 27 days) (P < 0.001). At discharge, 18% of patients (n = 3) were noted to have a neurologic deficit, and 59% (n = 10) were discharged on anti-epileptic medications. Follow-up data were available for 15 patients at an average age of 54 months (range 15 months–83 months). One patient died prior to the scheduled neurology follow-up, and one patient does not follow at CHP. At the time of the last follow-up, 60% (n = 9) of patients had motor deficits. Four patients with motor weakness had a large territory stroke, and 1 had a small lesion, 3 had multiple lesions, and 1 had two separate stroke episodes. For patients without any motor deficit, none had an isolated large stroke, 4 had a small lesion, and 1 had multiple lesions. A full description of the type of delays and associated lesion(s) is given in Table 2. At the time of last follow-up, only 2 patients (13%) remained on anti-epileptic medications
Description of neurologic outcomes for stroke group

ACA = anterior cerebral artery; MCA = middle cerebral artery; PICA = posterior inferior cerebellar artery.
Discussion
Our data demonstrate the benefit of comprehensive monitoring in identifying arterial ischaemic strokes in infants undergoing operations or cardiac catheterisation procedures during their cardiac ICU stay. Thirteen of 25 stroke episodes were identified as part of our standard monitoring practice, and less than half (11/25) of the stroke episodes were identified with clinical symptoms, with 20% (5/25) of the stroke episodes associated with focal neurologic signs or clinical seizures. Six of 25 were associated with non-specific symptoms. The remaining episode was identified by serial imaging. Patients with stroke tended to have more complex cardiac lesions, more high-risk operations, and more need for ECMO support.
The use of comprehensive monitoring and imaging for stroke detection, as demonstrated in this cohort, aligns with prior studies indicating that clinical signs alone are insufficient for timely diagnosis of stroke in critically ill infants. In our cohort, 4% of stroke patients presented with clinical seizures, 16% (4/25) with focal deficits, and 64% (14/25) were clinically asymptomatic. Our use of continuos electroencephalography, head ultrasound, and head CT in the acute post-procedure phase led to the identification of ∼60% (15/25) episodes of stroke. Our findings add to the existing literature on electroencephalography in the postoperative period with multiple studies previously demonstrating the utility of electroencephalography and continuos electroencephalography to detect seizures and predict neurologic injury. Reference Claessens, Noorlag and Weeke20,Reference Lin, Du and Feng30,Reference Algra, Schouten and Jansen31 Although combined head ultrasound and EEG have been demonstrated to identify intracranial injury in the neonatal ECMO population, our study is unique in examining a real-world clinical practice of comprehensive bedside monitoring with continuos electroencephalography, serial head ultrasound, and head CT in the cardiac ICU. Reference Gannon, Kornhauser and Gross29
The stroke rate in our study cohort (6.9%) is comparable to prior works (4–19%). Reference Chen, Zimmerman and Jarvik3,Reference Mahle, Tavani and Zimmerman6,Reference Beca, Gunn and Coleman8,Reference McQuillen, Barkovich and Hamrick9 Our study is unique in detailing the performance of a comprehensive monitoring practice to identify arterial ischaemic strokes. Timely detection of stroke is critical for anticoagulation and ECMO management. Similar to previous studies, more than half of the strokes (60%, 15/25) in our patient population were diagnosed with head ultrasound. Reference Rollins, Yoder and Moore26,Reference Said, Guilliams and Bembea32,Reference Lazar, Abramson, Weinstein and Stolar33 This finding highlights the value of head ultrasound in in the cardiac ICU, particularly as a trigger for advanced imaging. We do not have data on the rate of false positives head ultrasounds in our patient group or percentage of patients who underwent screening head imaging that was negative. Therefore, statistical analysis, with determination of sensitivity and specificity, was not possible.
Long-term follow-up revealed persistent motor deficits in 60% of stroke survivors. Our finding of increased identification of deficits at long-term follow up is consistent with other works that have shown most infants with stroke do not demonstrate symptoms until later. Reference Armstrong-Wells and Ferriero34 Multiple studies examining electroencephalography have demonstrated that abnormal activity in the post-operative period has associations with worse neurodevelopmental outcomes. Reference Hanalioglu, Temkit and Hildebrandt28,Reference Latal, Wohlrab and Brotschi35–Reference Vaughan, Hammoud and Pande40 Seizures on continuos electroencephalography in the preoperative period have also been shown to be associated with worse developmental outcomes. Reference Pittet, Marini and Ly41
Limitations
The main limitations of our study are inherent to its retrospective single centre design and expected variation in peri-procedure neuroimaging related to clinical judgement. We chose to focus on arterial ischaemic stroke as it has been demonstrated that seizures and neurologic outcomes are more often associated with arterial ischaemic stroke versus intracranial haemorrhage. This focus, however, does limit the conclusions that can be made for monitoring to identify all potentially clinically relevant pathologies. Finally, retrospective chart review limited our ability to obtain complete neurodevelopmental data.
Conclusion
In conclusion, our study provides further evidence that infants with critical CHD are at a high risk for ischaemic stroke. Comprehensive peri-operative neuromonitoring can identify strokes in this vulnerable population. Despite guideline recommendations, a recent survey of European cardiac surgery centres demonstrated that only 12% of centres routinely use continuos electroencephalography following surgery for children <28 days of age and a review of the Pediatric Health Information System Database demonstrated that only 62% of children receiving ECMO underwent an electroencephalography. Reference Feldmann, Hagmann and de Vries42,Reference Kohne, MacLaren and Shellhaas43 By utilising new tools including a stroke risk score Reference Yelton, Flores and Sun44 or NeuroSPARK score to predict injury on ECMO, Reference Shah, Mathur and Shanmugham45 it should be possible to improve selection of high-risk patients for comprehensive neuromonitoring. There is increasing evidence for clinically relevant serum biomarkers of neurologic injury, and addition of these markers to a monitoring protocol may increase its utility. Reference Algra, Schouten and Jansen31,Reference Van Loo, Cools, Dereymaeker and Jansen37 It might also be possible to tailor the chosen set of neuromonitoring modalities for monitoring and timing for such monitoring to each patient’s clinical condition. Monitoring protocols could also include management algorithms that may ultimately improve outcomes when strokes are identified. Reference Yelton, Flores and Sun44,Reference Phelps, Silos and De La Torre46,Reference Chung and Pabst47 As targeted comprehensive neuromonitoring expands, hopefully more can be done to address the sequela of strokes and improve long-term clinical and neurodevelopmental outcomes
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S1047951126113043.
Author contribution
-
• Conception and design: TSK, JHL
-
• Administrative support: TSK, TB, AG, JHL
-
• Provision of study materials or patients: TSK, TB, JHL
-
• Collection and assembly of data: TSK, AF, JM, BC, TB, JHL
-
• Dataanalysis and interpretation: TSK, DC, JHL
-
• Statistics: AT
-
• Manuscript preparation: TSK, JM, AT, DC, AG, JHL
Competing interests
All authors declare no competing interests.





 Open access
Open access