


Introduction
According to 2016 Irish census data, approximately 360,000 non-Irish residents spoke a language other than English at home in Ireland and only 44% of non-Irish people spoke English very well in their first year in Ireland (CSO 2017). Compared to the general population, there is a higher prevalence of post-traumatic stress disorder, depression, anxiety, and psychosis among refugees and asylum seekers (Blackmore et al. Reference Blackmore, Boyle, Fazel, Ranasinha, Gray, Fitzgerald and Gibson-Helm2020). Effective communication is vital in mental service provision, especially in inpatient settings. The Mental Health Commission of Ireland Judgement Support Framework (MHC 2020) mandates addressing communicating barriers in inpatient care by requiring interpreter and translation services to be available, and patients to be supported, irrespective of their primary language.
Mental health care relies primarily on verbal communication as the basis for diagnosis. In this context, language discordance can affect the accuracy of assessment, the working relationship between patient and clinician, the management of stigma and patient centred care (Lewis-Fernández & Kirmayer Reference Lewis-Fernández and Kirmayer2019). The ‘black box’ approach to interpreter use involves removing the interpreter from the therapeutic process through verbatim translation (Searight & Searight Reference Searight and Searight2009). This model, although necessary at times (e.g. for diagnostic purposes), has been criticised for losing valuable clinical data in translation (Miller et al. Reference Miller, Martell, Pazdirek L.Caruth and Lopez2005). Another role for the interpreter is that of the ‘bicultural worker’: an approach that views the interpreter as an integral part of a triadic therapeutic alliance. This may involve the interpreter explaining sociocultural aspects of the patient’s life to the clinician (Searight & Searight Reference Searight and Searight2009). A recent commentary argued for the interpreter’s role in clarifying information, being cultural brokers, and acting as advocates and mediators for patients (Chang et al. Chang et al. Reference Chang, Hsieh, Somerville, Dimond, Thomas, Nicasio and Lewis-Fernández2021).
Previous qualitative studies have identified several barriers to working, using this partnership approach with interpreters, in mental health. Leanza and colleagues (2015) found that clinicians can fear losing authority and be anxious about the loosening of clinical boundaries. They also identified how different working approaches and styles of communication can lead to mutual mistrust between the clinician and the interpreter. Research exploring the interpreters’ perspectives on their experience in mental health settings has uncovered challenges with understanding psychiatric terminology, the impact of vicarious trauma, and emotional toll of interpreting (Villalobos et al. Reference Villalobos, Orengo-Aguayo, Castellanos, Pastrana and Stewart2020). Available data indicate that interpreters can contribute both positively and negatively to the therapeutic alliance (Gartley & Due Reference Gartley and Due2017). However, previous studies all have limited transferability. They focus on interpreter use in counselling (Paone & Malott Reference Paone and Malott2008), trauma specific services (Villalobos et al. Reference Villalobos, Orengo-Aguayo, Castellanos, Pastrana and Stewart2021), the refugee context (Gartley & Due Reference Gartley and Due2017), cross-language mental health treatment (Becher & Wieling Reference Becher and Wieling2015), or in ‘mental health encounters’ in services more generally (Zimányi Reference Zimányi2013). We were unable to identify any previous research that investigated the clinician perspective on the use of interpreters in mental health assessment.
This study aims to address this gap in the literature by exploring how clinicians, from several different disciplines in mental health, in both community and inpatient settings, experience the use of interpreters in mental health assessment.
Methods
Participants and recruitment
Two sites were identified for the purposes of participant recruitment: one, an inpatient mental health unit and the other, a community mental health service, both based in Dublin, Ireland. A clinical gatekeeper (administrator working in the same community mental health service, based in Dublin) was responsible for participant identification, making first contact, and recruitment. We declare no biases in our choice of clinical gatekeeper and efforts were made to ensure that participants were approached guided by the methodology of purposive sampling.
Forty-five clinicians working in either or both the inpatient mental health unit and/or community mental health service were contacted by email by the clinical gatekeeper and invited to participate in the study. Twenty-seven clinicians who had experience of using interpreters in mental health assessment (60% of those contacted) responded to our email invitation indicating their willingness to participate. To select study participants, we used a purposeful sampling matrix to pursue maximum variation across the variables: sex (male or female), clinical role, years of clinical experience, and number of occasions using an interpreter in patient assessment.
In line with the guidance offered by Braun & Clarke (Reference Braun and Clarke2022), we conducted an appraisal of ‘information power’ to determine when we stopped sampling participants. Information power is a concept that is based on the understanding that the more relevant information a sample holds the less participants are required. Our assessment considered the study characteristics impacting dataset quality that were necessary to achieve our objectives. Our study aims were narrow, our sample was specific, the interview dialogue was mostly strong, our analysis was cross-case, and data interpretation was informed by a limited theoretical background. As per Malterud et al. (Reference Malterud, Siersma and Guassora2016) strong dialogue between researcher and participants requires fewer participants to offer sufficient information power than a study with unfocused dialogues and is dependent on features such as the rapport between the interviewer and participant, the competence of the interviewer, and the articulateness of the participant. We concluded interviewing, after 15 interviews, when information power was deemed sufficient. 15 participants represent 33.3% of the total number of potential participants (N = 45) invited to take part.
All 15 participants had a prior professional relationship with at least one of the study authors. Prior to the commencement of recruitment, all participants had spoken with at least one of the authors regarding clinical matters.
Data collection
Semi-structured interviews, lasting 20–55 minutes, were conducted with 15 clinicians. All interviews were informed by an interview guide (see Table 1) and focused on eliciting the participant experience of using interpreters in mental health assessment as well as perceived benefits and difficulties associated with interpreter use. EG, who had moderate experience of qualitative interviewing previously, conducted the 15 interviews. Participants were assigned pseudonyms. Interview data were recorded using an audio recorder, transcribed verbatim into Microsoft Word files, and any information that could be used to identify participants redacted.
Semi-structured interview guide

Data analysis
Data were analysed by hand using Reflexive Thematic Analysis (Braun & Clarke Reference Braun and Clarke2022). Analysis was exploratory, inductive and essentialist; underpinned by relativism; and data were analysed at a semantic level. Using Reflexive Thematic Analysis enabled us to systematically identify, interpret, and describe, in rich detail, key elements of participants’ accounts across our dataset and to organise them into meaningful themes. This process involved: (1) becoming acquainted with the data; (2) developing initial codes; (3) seeking, revising, defining, and naming themes; and (4) generating a report.
Actions taken to address issues of study rigour and reflexivity, followed principles set out by O’Keeffe et al. (Reference O’Keeffe, Sheridan, Kelly, Doyle, Madigan, Lawlor and Clarke2022). Participants were selected based on their ability to provide data to enable achievement of the study’s aims. Two research team members (EG and MC) analysed data independently and compared and agreed codes and themes to ensure rigour in data analysis. So that our thematic interpretation could be deemed a reasonable representation of participant narratives, we sought to strike a balance between presenting extracts to illustrate themes and our analysis.
Results
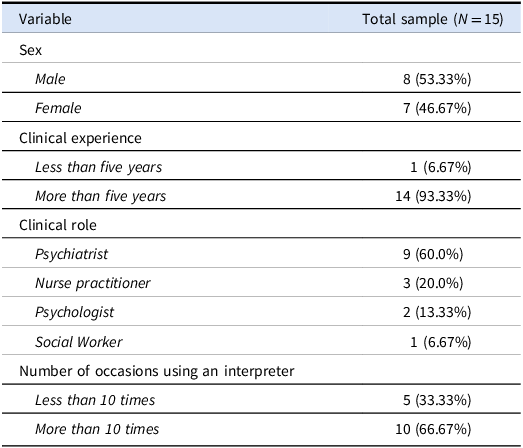
Participant characteristics are presented in Table 2.
Demographic and clinical characteristics of study sample

Overview of the findings
The overarching thematic structure of the six themes develop, that reflects the experiences of clinicians who have used interpreters in mental health assessment, is presented in Fig. 1.
Overarching thematic structure of themes generated.

These are ‘Interpreters providing depth and adding cultural meaning to assessment’, ‘The absence of control over interpreter performance and selection’, ‘Interpreters being a reassuring presence for patients’, ‘Interpreters undermining patient freedom to express their thoughts and feelings in confidence’, ‘Further training, guidance, and regulation are needed’, and ‘The practical barriers to interpreter use’. We will now describe each in detail and provide a small number of extracts from our dataset in support of each theme. Additional interview quotes supporting themes developed are displayed in Supplement 1.
Interpreters providing depth and adding cultural meaning to assessment
Clinicians experienced interpreters as serving to make patients feel understood and giving patients a greater capacity for linguistic expression. Some described the value of the interpreter as providing linguistic nuance and assisting in deciphering of meaning in patient responses to questions. This was particularly important in the acquiring of diagnostic clarity. As Sam explained:
‘With an interpreter [present in assessment], I’m definitely aware of a much richer assessment… Often [assessments] for people who lack insight into what’s happening to them necessitate a really high degree of linguistic mastery and… there’s ample opportunity to miss crucial information, even when somebody thinks that what they’re conveying to you is accurate to what they’re feeling’.
The absence of control over interpreter performance and selection
Clinicians’ indicated concern that they cannot independently corroborate verbal exchanges between interpreters and patients during the clinical interview. They reported that they had no means to ensure that the clinical questions posed during interview are accurately translated by an interpreter or that patient responses to questions are accurately interpreted for the clinician. As Eugenie described:
‘It is awkward [using an interpreter in assessment] because it changes the dynamic and then like obviously there’s the element of them [the interpreter and patient] going off and having their own separate conversation’.
Clinicians also described lacking agency and autonomy in the selection of an interpreter for an assessment. Some felt this choice could facilitate an improved therapeutic relationship between clinician and patient and ensure that the interpreters selected have adequate experience. In his interview, Derek commented:
‘Wouldn’t it be great if there was a translator service that you know had a special interest or a special remit to operate within the HSE [Irish public health service] or within health services’.
Interpreters being a reassuring presence for patients
Clinicians felt the presence of an interpreter can engender in patients a sense of comfort, borne from the presence of someone in the assessment who can freely understand them. Many clinicians felt that this allowed patients to express themselves and articulate their needs more openly. Harold observed:
‘When there’s an interpreter there, they [the person being assessed] can relax a bit more “I can say stuff” and then the doctor or the nurse or whoever is going to understand what they’ve said. So it could be relieving for them ‘cause yeah it [the assessment] makes sense’.
Sam noted:
‘[Interpreters] can be, you know, good at reassuring patients that they can trust the process… being accompanied by somebody who is more similar to the patient in terms of their linguistic background can be really helpful’.
Interpreters undermining patient freedom to express their thoughts and feelings in confidence
Clinicians were concerned about the possibility that an interpreter and a patient might directly or indirectly known each other if they were both members of an ethnic community with a relatively small presence in Ireland. If they did, the patient might not feel comfortable disclosing personal information about themselves due to psychiatric stigma. Clinicians felt that this inhibition could undermine the assessment process. In her interview, Leila recounted an experience that impacted an assessment:
‘I forget the ethnic group of this service user, but the interpreter was of the same ethnic group, and I know the service user was afraid to disclose personal information because of living in Ireland in a small ethnic community and she didn’t want things to get out about her, because maybe the interpreter might have known people that she knew and things like that’.
Further training, guidance, and regulation are needed
Clinicians felt they would benefit from training and guidance in the use of interpreters in the assessment process. Many clinicians believed that interpreters are not used often enough in assessment to give them adequate experience to feel confident and comfortable with their use. As Lily remarked:
‘I wouldn’t say I do it [use interpreters in mental health assessment] often enough; I would love some training on it’.
Clinicians reported concerns that interpreters working in Ireland are not subject to regulatory oversight, are not trained in upholding the right of patient confidentiality, and are not provided with even rudimentary training in mental health assessment. Lia reported:
‘They [interpreters] should probably be trained in patient confidentiality and all that stuff, like you’d worry maybe in that sense that they [interpreters] might not like hold it [protecting patient confidentiality] to that kind of same respect as we [clinicians] would’.
The practical barriers to interpreter use
The theme describes the real-world challenges encountered by clinicians when using interpreters. For example, arranging room bookings. These factors can negatively impact time and clinical availability for other patients. In his interview, Bruce remarked:
‘I guess it can be difficult to get interpreters on a practical level. Sometimes asking the team secretary to try and arrange it can be awkward… and to find a time and obviously it takes a little bit more time to do the interview to go through all the introductions’.
Clinical time can unduly be taken up by arranging for an interpreter to be present at clinical assessments and this has been put forward as potentially leading to clinicians being swayed from providing patients with interpreters in assessment. Dorothy observed:
‘Where was my responsibility to book them [an interpreter]… which, could be a bit obstructive as well, so it might make you less likely to book one’.
The cost associated with interpreter use was another practical barrier reported by participants. Some argued that the clinicians may be dissuaded from utilising an interpreter when considering the cost to their employer of acquiring one. As Anabel explained in her interview:
‘I’ve certainly had it brought to my attention [by HSE management] that it [interpreter use in assessment] is very expensive. I guess that probably goes to the fact then that maybe I wouldn’t push for an interpreter [in mental health assessments]’.
Discussion
Main findings
The study offers a novel conceptualisation of the clinician experience of using interpreters in mental health assessments. Overall, interpreters were perceived as valuable: assisting in clarifying information; helping patients communicate their needs; understanding what thoughts, feelings, and behaviours mean in a cultural context; and dispelling fears to make patients feel comfortable. However, participants expressed concerns about interpreter use in clinical assessment. A particular emphasis was placed on the need for training and guidance for both interpreters and clinicians. The juxtaposition of the benefits and pitfalls of using interpreters in mental health assessments reflects the real-world realities of navigating this complex, challenging process on the ground in services.
Our findings contribute to the debate on whether interpreters should only focus on verbatim translation or simultaneously translate, be a cultural broker, and an advocate (Chang et al. Reference Chang, Hsieh, Somerville, Dimond, Thomas, Nicasio and Lewis-Fernández2021). While participants had to sacrifice some control in the assessment process by using interpreters, the provision of culturally appropriate, contextualised understandings of patients’ core concerns was considered invaluable. For many participants, the benefits of interpreters not solely focusing on verbatim translation broadly outweighed the risks (e.g. the interpreter and patient forming an alliance and discussing the assessment subsequently). These concerns correspond with previous studies that found clinicians fear interpreter involvement leads to a loss of control, therapeutic power, bias from interpreter opinions, and the patient and interpreter having conversations without translating them for the clinician (Becher & Wieling Reference Becher and Wieling2015; Hadziabdic et al. Reference Hadziabdic, Albin, Heikkilä and Hjelm2010; Leanza et al. Reference Leanza, Boivin, Moro, Rousseau, Brisset, Rosenberg and Hassan2015). In previous research, the interpreter-patient relationship has been described as a pathway to ‘open doors’ in the assessment process (Leanza et al. Reference Leanza, Boivin, Moro, Rousseau, Brisset, Rosenberg and Hassan2015) and patients have perceived interpreters conveying warmth and respect in culturally appropriate ways, during assessments, even if the clinician did not (Chang et al. Reference Chang, Hsieh, Somerville, Dimond, Thomas, Nicasio and Lewis-Fernández2021).
Implications for policy and practice
Our data can inform the development of service models for patients that do not speak the language of the clinician assessing them. Participants felt that further clinician and interpreter training and experience is needed to ensure effective clinical assessment can be utilised to facilitate optimal clinical care. Clinicians should be trained to assess patients’ cultural backgrounds to enhance interpreters’ efforts at communicating culturally relevant meaning and context in the assessment process. This could help elicit symptoms and assist in coproducing and explaining treatment plans to patients.
For interpreters, it is important that they are educated in the importance of maintaining patient confidentiality, psychiatric terminology, and in the subtleties of advocacy. Interpreters need to balance delivering an accurate translation of the words spoken by both parties against communicating cultural meanings and context. Our findings suggest that clinicians’ experience in using interpreters in clinical assessment has been that interpreter’s competence and attitude towards patients may impact the quality of clinical assessments. This highlights the need for regulation and training to ensure interpreters in mental health assessments can demonstrate adequate language skills but also respect for patients, professional competencies, and appropriate boundaries.
Our findings highlight the practical barriers providers and patients face in working with interpreters. Participants identified that working with an interpreter in an assessment requires more time. Given that assessment with an interpreter requires a significantly longer interaction between clinician, patient, and interpreter, time should be protected when managing clinical caseloads to allow for this. Core tenets of the Recovery Approach are prioritising access, engagement, and relationship building over time (O’Keeffe et al. Reference O’Keeffe, Sheridan, Kelly, Doyle, Madiga, Lawlor and Clarke2018). Our data suggest that until all non-English speaking patients are afforded access to adequately resourced, appropriately defined interpreter services to support a comprehensive, humanised, and culturally appropriate mental health assessment, a recovery-oriented mental health system will remain an unfulfilled promise in Ireland.
Strengths and limitations
The study had a number of strengths. Before this study, the interviewing author (EG) had moderate qualitative interviewing experience (enabling us to collect rich in-depth data). We included and community mental health settings (increasing transferability across different clinical contexts). Finally, findings have clear policy and practice implications offering actionable insights to improve interpreter regulation, training, and guidance (enhancing the likelihood of impact on service provision).
However, findings should be viewed in light of a number of limitations. We did not consider race or ethnicity when sampling. Most participants were psychiatrists and worked in both community and inpatient mental health setting, rather than exclusively in one setting. Therefore, the experiences analysed may reflect the sample rather than being transferable to clinicians working in other clinical settings. Although we engaged a purposeful sampling to obtain maximum variation across variables, we were unable to achieve balance for the dichotomous variable ‘Clinical experience’. Only one participant out of the 15 (7%) had less than five years clinical experience. Or for the variable ‘Clinical role’. Nine of 15 participants were psychiatrists (60%). These factors impact the transferability of findings beyond our sample.
Potential bias may exist due to a prior professional relationship between the interviewer and the 15 participants in the discussion of clinical matters. This may have caused participants to give socially desirable responses or to answer questions in a way that they perceived as
‘socially acceptable’. We did not conduct member checking with participants with the themes that were developed in this study. Doing so may have increased the accuracy, transferability, validity and credibility of findings.
Finally, we did not examine patient or interpreter perspectives. Triangulating theses three viewpoints may bring added insight and would enable an analysis of areas of shared and contrasting concern.
Conclusion
Findings emphasise the importance of interpreters in providing culturally relevant and meaningful information in clinical assessment, while also providing a reassuring presence for patients. However, our data also highlight the challenges reported with using interpreters in clinical assessment. For example, clinicians described concerns that interpreters may undermine their ability to control the clinical interview and affect patient confidence that they can communicate confidentially, and without prejudice. Deficits exist in interpreter and clinician training, guidance, and regulation that warrant urgent action to ensure that language does not prevent adequate, appropriate, and timely recovery-oriented assessment in mental health services.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/ipm.2025.17.
Acknowledgements
The authors would like to acknowledge the clinicians Saint John of God Community Services, who participated in this study and the Saint John of God Community Services Clg who supported deliver of this study.
Author contribution
EG wrote the first draft of this manuscript. All authors critically edited and revised the work and agree to be accountable for all aspects of the study. All authors conceived of and designed the study; collected, analysed, and interpreted the data; and contributed to data analysis. MC and DOK provided academic supervision for research activity planning and execution.
Financial support
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Competing interests
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Ethical standard
Ethical approval for the study was obtained from the Saint John of God Hospitaller Ministries Research Ethics Committee. The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committee on human experimentation with the Helsinki Declaration of 1975, as revised in 2008.





 Open access
Open access