


Introduction
The UK NICE guideline (National Institute for Health and Care Excellence, 2014) recommends CBT for everyone with a diagnosis of schizophrenia, yet many people do not access therapy or other recommended treatments promptly (cf. Birchwood et al., Reference Birchwood, Connor, Lester, Patterson, Freemantle, Marshall and Singh2013), and duration of untreated psychosis (DUP) predicts poorer clinical and social outcomes (Marshall et al., Reference Marshall, Lewis, Lockwood, Drake, Jones and Croudace2005; Perkins et al., Reference Perkins, Gu, Boteva and Lieberman2005; Sullivan et al., Reference Sullivan, Carroll, Peters, Amos, Jones, Marshall and Tilling2019). Treatment delays are typically 1–2 years and incur considerable personal and healthcare costs (Boonstra et al., Reference Boonstra, Klaassen, Sytema, Marshall, De Haan, Wunderink and Wiersma2012; Penttilä et al., Reference Penttilä, Jääskeläinen, Hirvonen, Isohanni and Miettunen2014; Salazar de Pablo et al., Reference Salazar de Pablo, Aymerich, Guinart, Catalan, Alameda, Trotta and Correll2024), leading the World Health Organisation (2001) to identify reduction in DUP as an international priority for over a quarter of a century.
In the UK, delays within secondary mental health services make the largest contribution to DUP, followed by delays in help-seeking (Birchwood et al., Reference Birchwood, Connor, Lester, Patterson, Freemantle, Marshall and Singh2013). To expedite access to specialist Early Intervention Services, Access and Waiting Time Standards were introduced in 2016 to reduce delays from initial referral to start of treatment for people with first episode psychosis. While there is some evidence that within service waiting times have improved (Adamson et al., Reference Adamson, Barrass, McConville, Irikok, Taylor, Pitt and Price2018), there is as yet no clear evidence of reduction in overall DUP. Additionally, we need to understand and address barriers to help-seeking.
Once in contact with services, around a third of people with psychosis disengage prior to receiving ‘full dose’ interventions (Doyle et al., Reference Doyle, Turner, Fanning, Brennan, Renwick, Lawlor and Clarke2014; Kreyenbuhl et al., Reference Kreyenbuhl, Nossel and Dixon2009). The evidence for CBT for psychosis delivered in routine clinical settings also indicates high drop-out rates (e.g. Fanning et al., Reference Fanning, Foley, Lawlor, McWilliams, Jackson, Renwick and O’Callaghan2012; Richardson et al., Reference Richardson, Dasyam, Courtney, White, Tedbury, Butt and Newman-Taylor2019), though this is likely to be better in research trials (e.g. Jolley et al., Reference Jolley, Garety, Peters, Fornells-Ambrojo, Onwumere, Harris and Johns2015). In summary, many people with psychosis delay making contact with services, and are then vulnerable to disengaging when they have done so.
It is tempting to assume that paranoia, a characteristic symptom of psychosis and experienced by up to 90% of those with a diagnosis of schizophrenia (Moutoussis et al., Reference Moutoussis, Williams, Dayan and Bentall2007, after Tarrier et al., Reference Tarrier, Lewis, Haddock, Bentall, Drake and Dunn2004), accounts for initial and ongoing hesitancy to access services. Certainly, interpersonal mistrust and beliefs that others intend harm are likely to affect willingness to seek help. However, the wide variation in help-seeking in people with psychosis (Birchwood et al., Reference Birchwood, Connor, Lester, Patterson, Freemantle, Marshall and Singh2013), the majority of whom experience paranoia in the form of persecutory delusions (Moutoussis et al., Reference Moutoussis, Williams, Dayan and Bentall2007), suggests that other factors may be more predictive of help-seeking and service engagement than paranoia per se.
Insecure attachment is common in people with psychosis (Berry et al., Reference Berry, Barrowclough and Wearden2007; Gumley et al., Reference Gumley, Taylor, Schwannauer and MacBeth2014), clinical levels of paranoia (Lavin et al., Reference Lavin, Bucci, Varese and Berry2020; Murphy et al., Reference Murphy, Goodall and Woodrow2020), and analogue groups with high levels of non-clinical paranoia (Murphy et al., Reference Murphy, Goodall and Woodrow2020), and may account for some of the variation in help-seeking in psychosis (Gumley et al., Reference Gumley, Taylor, Schwannauer and MacBeth2014). There is also evidence that insecure attachment is associated with paranoia specifically (and not hallucinations), in both clinical and non-clinical groups (Pickering et al., Reference Pickering, Simpson and Bentall2008; Wickham et al., Reference Wickham, Sitko and Bentall2015). Attachment theory assumes that our early caregiving relationships shape enduring internal working models (cognitive representations of self, others and relationships) which influence affect regulation and interpersonal behaviours (particularly help-seeking) at times of distress (Bowlby, 1969/Reference Bowlby1982). The overlap with cognitive behavioural theory and implications for practice will be clear to CBT clinicians and researchers.
Broadly consistent and responsive caregiving in infancy is associated with a secure attachment style in adulthood, characterised by expectations that we can manage difficult situations and emotions, that others are safe and helpful, and that we can seek help when needed (Mikulincer and Shaver, Reference Mikulincer and Shaver2007). Infants who experience absent or rejecting early care are likely to develop an insecure avoidant style, characterised by negative beliefs about others as rejecting and unhelpful, deactivating emotion regulation strategies (e.g. suppression), and a failure to seek help when needed (Mikulincer and Shaver, Reference Mikulincer and Shaver2007). Inconsistent and unpredictable early care is associated with an insecure anxious style, characterised by negative self-beliefs, expectations that others are unreliable, hyperactivating emotion regulation strategies (e.g. rumination and catastrophisation) and repetitive, often ineffective help-seeking (Mikulincer and Shaver, Reference Mikulincer and Shaver2007). Those without a discernible pattern of attachment behaviours are categorised as disorganised (Main and Soloman, Reference Main, Solomon, Brazelton and Yogman1986; Main and Soloman, Reference Main and Solomon1990), which may follow early experiences with a caregiver who was both frightened and frightening, possibly due to unresolved traumas of their own (Main and Hesse, Reference Main, Hesse, Greenberg, Cicchetti and Cummings1990).
Dozier (Reference Dozier1990) showed that attachment style was associated with help-seeking in a heterogenous sample with severe mental health conditions; avoidant attachment was associated with reduced help-seeking, reduced self-disclosure, and increased likelihood of rejecting help offered, whereas anxious attachment was associated with increased help-seeking and self-disclosure. Initial systematic reviews showed that insecure attachment is over-represented in people with psychosis, and associated with poorer service engagement (Berry et al., Reference Berry, Barrowclough and Wearden2007; Gumley et al., Reference Gumley, Taylor, Schwannauer and MacBeth2014). Similarly, a more recent review found that people with psychosis who are anxiously or avoidantly attached are less likely to seek help than those who are securely attached, and that this pattern is strongest for avoidant attachment, and broadly consistent across correlational, experimental and longitudinal designs, and for analogue, early psychosis and established psychosis samples (Sood et al., Reference Sood, Carnelley and Newman-Taylor2022b). This consistency of findings indicates that problems with help-seeking exist across the psychosis continuum, are apparent early in the illness trajectory, and can usefully be explored in analogue as well as clinical groups to inform practice (cf. van Os et al., Reference van Os, Hanssen, Bijl and Ravelli2000).
Threat activates the attachment system (Bowlby, 1969/Reference Bowlby1982). We would expect, therefore, that moments or extended periods of heightened paranoia would activate an individual’s dominant attachment style. This means that paranoid fears, in both clinical and non-clinical groups, are likely to be compounded by unhelpful affective and interpersonal regulation responses if insecurely attached. These in turn are likely to influence help-seeking. Within a CBT framework, if we can clarify the beliefs and behaviours associated with a hesitancy to seek help, we will be in a stronger position to anticipate and respond to threats to initial and ongoing engagement with CBT and other recommended treatments.
We used a cross-sectional design to examine theoretically predicted relationships between attachment style and (1) beliefs about self and others, (2) underlying assumptions, and (3) help-seeking intentions, across the psychosis continuum – in an analogue sample with high levels of paranoia, and a clinical sample with psychosis. We selected the non-clinical group as a limited proxy for psychosis vulnerability (Johns and van Os, Reference Johns and van Os2001; van Os et al., Reference van Os, Linscott, Myin-Germeys, Delespaul and Krabbendam2009) and given the link between attachment insecurity and paranoia specifically, across the psychosis continuum (Pickering et al., Reference Pickering, Simpson and Bentall2008; Wickham et al., Reference Wickham, Sitko and Bentall2015). We hypothesised that:
-
(1) insecure anxious attachment will be associated with negative beliefs about self (controlling for the effect of avoidant attachment);
-
(2) insecure avoidant attachment will be associated with negative beliefs about others (controlling for the effect of anxious attachment);
-
(3) insecure anxious attachment will be associated with problematic underlying assumptions (controlling for the effect of avoidant attachment), and vice versa;
-
(4) insecure avoidant attachment will be associated with reduced help-seeking intentions (controlling for the effect of anxious attachment).
Given the lack of evidence for associations between disorganised attachment and CBT relevant variables to date, we did not make specific predictions for this attachment style but sought to explore whether:
-
(5) insecure disorganised attachment is associated with beliefs about self and others, underlying assumptions and help-seeking intentions.
Method
Ethical considerations
This study received ethical approval from the University of Southampton, UK (ID: 61766) and was pre-registered on the Open Science Framework (https://osf.io/uafbn/overview?view_only=74a6f7586dc64a84a2cec73059c2c4bd).Footnote 1
Design
We used a cross-sectional observational design to examine predicted relationships between attachment style and beliefs about self and others, underlying assumptions, and help-seeking intentions, across the psychosis continuum – in a general population analogue group with elevated paranoia, and in a clinical group with self-reported psychosis. A G*Power analysis for multiple regression indicated that, to obtain .95 power and detect a medium effect size of .15, at the .05 alpha error probability, we needed 119 participants for each sample.
Participants
We recruited participants from open research, university research, and social media websites. Participants in the analogue group were screened using the Paranoia Scale (Fenigstein and Vanable, Reference Fenigstein and Vanable1992) and selected for the study if they scored at or above 53 (one SD above the standardisation sample mean), following Bullock et al. (Reference Bullock, Newman-Taylor and Stopa2016) (cf. Combs and Penn, Reference Combs and Penn2004).
In the analogue sample, a total of 172 participants, aged 18–56 years (M=21.30, SD=6.16), completed the study. The majority were female (n=136, 79.1%) and the remaining participants were male. Most reported their ethnicity as White (n=126; 73.3%) and others as Black/Black British (6.4%), Asian/Asian British (10.5%), mixed (5.8%) and other (4.1%).
In the clinical sample, a total of 130 participants with self-reported psychosis, aged 20–66 years (M=32,87, SD=9.84), completed the study. Most were male (n=64; 49.2%), followed by female (n=51; 39.2%) and non-binary (n=13; 10.0%), and two preferred not to say (1.5%). Most reported their ethnicity as White (n=95; 73.1%) and others as Hispanic (10.0%), Black/African/Caribbean (6.9%), mixed (6.2%) and other/prefer not to report (3.8%).
Procedure
We recruited two samples: (1) an analogue sample with elevated paranoia from the general population, and (2) a clinical sample with self-reported psychosis. To recruit the non-clinical sample, we advertised on relevant websites available to the general public (e.g. The Paranoia Network) and students (e.g. SMARTEN – a student mental health research network), as well as university social media platforms. Non-clinical participants were offered the opportunity to be entered into a draw for one of four £50 vouchers or given research credit (university participants). We recruited the clinical sample via the online research platform Prolific and advertised the study to people who had been previously screened for psychosis and expressed an interest in research participation. Prolific is an online research site used to recruit participants in exchange for a small financial incentive. The site has been shown to yield high quality data as participants are more diverse (and likely to be representative of the general population) and honest than on other platforms (Peer et al., Reference Peer, Brandimarte, Samat and Acquisti2017, Reference Peer, Rothschild, Gordon, Evernden and Damer2022).
The study was conducted online. Participants were required to be 18 years or over and fluent in English (as all measures were provided in English). All gave informed written consent. We used the Paranoia Scale (Fenigstein and Vanable, Reference Fenigstein and Vanable1992) to determine eligibility for non-clinical participants. All completed measures of attachment, beliefs about self and others, underlying assumptions, and help-seeking intentions. Clinical participants also completed a brief measure of hallucinations to describe the sample. Finally, participants were debriefed and thanked. The entire study took approximately 20 minutes.
Measures
Paranoia
The Paranoia Scale (PS; Fenigstein and Vanable, Reference Fenigstein and Vanable1992) is a 20-item measure of trait paranoia. Participants rate items on a 4-point scale (from ‘not at all applicable to me’ to ‘extremely applicable to me’). The PS has acceptable internal reliability (α=.72), which was acceptable to excellent in the current samples (non-clinical α=.72; clinical α=.93).
Attachment
The Experiences in Close Relationships-Short (ECR-12; Lafontaine et al., Reference Lafontaine, Brassard, Lussier, Valois, Shaver and Johnson2016) is a 12-item measure of attachment style. Items for anxious and avoidant subscales are rated on a 7-point scale (from ‘disagree strongly’ to ‘agree strongly’). The measure has adequate to good internal consistency (anxiety α=.81; avoidance α=.79), which was good to excellent in the current non-clinical (anxiety α=.81; avoidance α=.84) and clinical (anxiety α=.91; avoidance α=.90) samples.
The Psychosis Attachment Measure-Revised (PAM-R; Pollard et al., Reference Pollard, Bucci, MacBeth and Berry2020) is a 26-item self-report measure of attachment anxiety, avoidance and disorganisation. Items are rated on a 4-point Likert scale (from ‘not at all’ to ‘very much’). Internal consistency is good for anxiety (α=.82), and acceptable for avoidance (α=.76) and disorganisation (α=.76). Internal consistency for the current non-clinical sample was questionable for anxiety (α=.62), poor for avoidance (α=.14), and good for disorganisation (α=.83). In the clinical sample, internal consistency was good for anxiety (α=.89), acceptable for avoidance (α=.79), and excellent for disorganisation (α=.92).
Beliefs about self and others, and underlying assumptions
The Brief Core Schema Scales (BCSS; Fowler et al., Reference Fowler, Freeman, Smith, Kuipers, Bebbington, Bashforth and Garety2006) consist of 24 items measuring four subscales of core beliefs: negative-self (6 items), positive-self (6 items), negative-others (6 items), and positive-others (6 items). We used adapted anchors for clarity (following Sood et al., Reference Sood, Carnelley and Newman-Taylor2021); participants rate items on a 5-point scale (from ‘no – I do not hold this belief’ to ‘yes – I believe this totally’). Internal consistency is acceptable to good for all subscales (α>.78), and these were all good to excellent in the current non-clinical and clinical samples (α>.89).
The Dysfunctional Working Models Scale (adapted) (DWM-S(A); following Perris et al., Reference Perris, Fowler, Skagerlind, Olsson and Thorsson1998) is a 35-item measure of conditional interpersonal beliefs (underlying assumptions). Participants rate items on a 7-point scale (from ‘I totally agree’ to ‘I totally disagree’). The authors of the scale identified three factors (32 items loaded), and labelled these fear of rejection (17 items), negative self-evaluation (10 items) and perfectionist attitude (5 items). We adapted the original measure to include only the 32 items which loaded in the factor analysis, plus three items designed to represent secure, anxious and avoidant interpersonal beliefs, respectively. Internal consistency for the original scale is excellent (α=.97) and was also excellent in the current samples for both 32-item (non-clinical α=.92; clinical α=.94) and 35-item versions (non-clinical α=.91; clinical α=.94).
Help-seeking
The Help-Seeking Measure (trait version) (HSM-T; following Sood et al., Reference Sood, Carnelley and Newman-Taylor2021) is a 3-item questionnaire of help-seeking intentions. Participants rate the likelihood of seeking help when feeling upset on a 5-point scale (from ‘not at all’ to ‘extremely’). Internal consistency is good to excellent (α=0.89–0.93), and this was also good to excellent in the current samples (non-clinical α=.87; clinical α=.92).
The General Help Seeking Questionnaire (GHSQ; Deane et al., Reference Deane, Skogstad and Williams1999) is a 10-item measure of help-seeking for specific concerns. We used the scale for ‘personal or emotional problems’ in line with the original instructions. Participants rate the likelihood of seeking help from a series of eight people (e.g. intimate partner, friend, health professional) on a 7-point scale (from ‘extremely unlikely’ to ‘extremely likely’). Participants also report if they are unlikely to seek help from anyone or would seek help from someone not listed. The measure has acceptable internal consistency (α=.70) (Wilson et al., Reference Wilson, Deane, Ciarrochi and Rickwood2005), which was also acceptable in the current non-clinical sample (α=.71), although poor in the clinical sample (α=.42).
Hallucinations
A brief, 4-item measure of trait auditory and visual hallucinations (Sood et al., Reference Sood, Carnelley and Newman-Taylor2024) was administered to participants in the clinical group to describe the sample. Participants rate frequency of hallucinatory experiences (e.g. voices, seeing things others cannot see) on a 7-point scale (from ‘never’ to ‘almost always’). Internal consistency was excellent in the current sample (α=.92).
Data analysis
We analysed the data using SPSS 29 for Windows. We excluded participants with more than 5% missing data and replaced all other missing data (<5%) with the participant mean (n=16), following Tabachnik and Fidell (Reference Tabachnick and Fidell2013). We provide descriptive statistics and intercorrelations of all variables to describe the data and show multi-collinearity (Tables 1 and 2). We tested hypotheses and ran exploratory analyses using simple/multiple linear regression analyses, having calculated a sample size that would allow for up to two covariates in the case of collinearity. Given poor internal consistencies of the PAM-R anxiety and avoidance subscales in the non-clinical sample, we used the ECR-12 subscales for analyses examining anxious and avoidant attachment, and the PAM-R for disorganised attachment in both samples.
Descriptive statistics and intercorrelations in the non-clinical sample

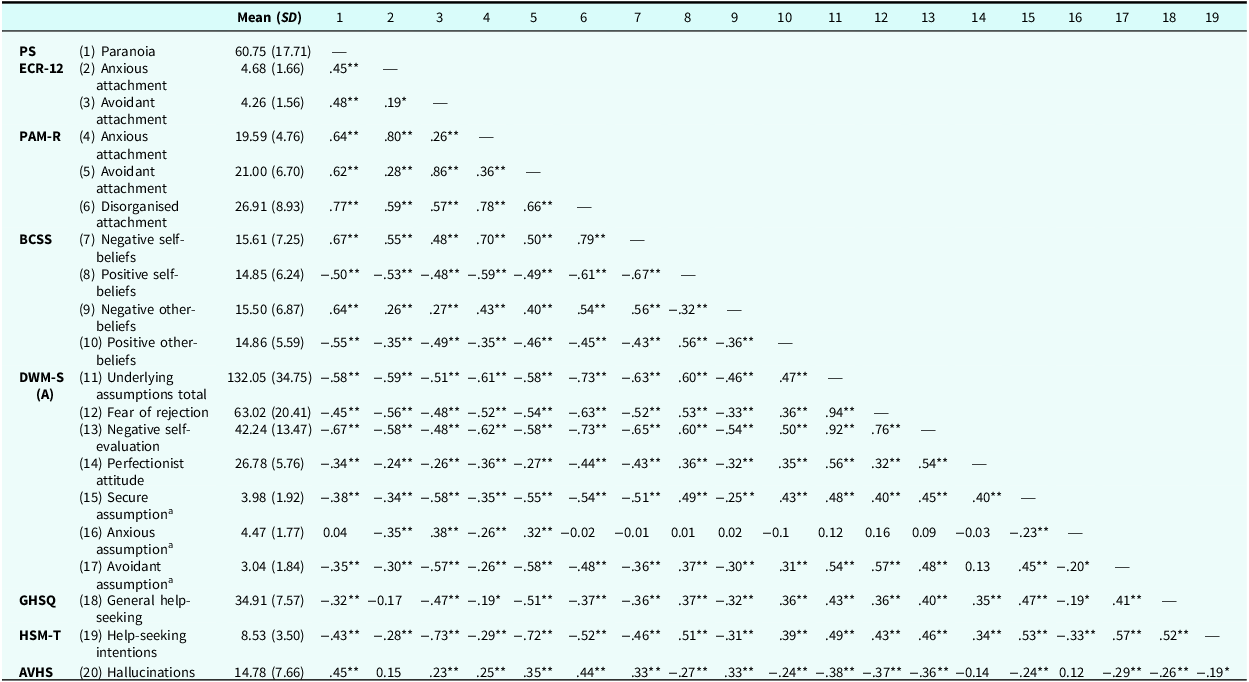
PS, Paranoia Scale; ECR-12, Experiences in Close Relationships (12-item); PAM-R, Psychosis Attachment Measure-Revised; BCSS, Brief Core Schema Scales; DWM-S(A), Dysfunctional Working Models Scale (adapted); GHSQ, General Help Seeking Questionnaire; HSM-T, Help-Seeking Measure (trait version); AVHS, Auditory and Visual Hallucinations Scale. aSecure, anxious, and avoidant assumptions refer to additional, single items. *p<.05, **p<.01.
Descriptive statistics and intercorrelations in the clinical sample

PS, Paranoia Scale; ECR-12, Experiences in Close Relationships (12-item); PAM-R, Psychosis Attachment Measure-Revised; BCSS, Brief Core Schema Scales; DWM-S(A), Dysfunctional Working Models Scale (adapted); GHSQ, General Help Seeking Questionnaire; HSM-T, Help-Seeking Measure (trait version); AVHS, Auditory and Visual Hallucinations Scale. aSecure, anxious, and avoidant assumptions refer to additional single items. *p<.05, **p<.01.
Results
Descriptive statistics and intercorrelations
Tables 1 and 2 show descriptive statistics and intercorrelations for all measures for the non-clinical and clinical samples. Both groups reported high levels of paranoia, and the clinical group reported frequent hallucinatory experience.
Inspection of histograms indicated that most variables were at least approximately normal; in the non-clinical sample, paranoia was positively skewed (and negative beliefs about self/others were slightly positively skewed). In the clinical sample, attachment anxiety and avoidance and positive beliefs about self/others were negatively skewed. We completed planned analyses as these are robust to minor departures from normality (Field, Reference Field2024).
Regression analyses
Is insecure attachment associated with negative beliefs about self and others?
Attachment anxiety and avoidance (measured with the ECR-12) were positively correlated with negative self-beliefs in both non-clinical and clinical groups (Tables 1 and 2). Regression analyses showed that increased attachment anxiety predicted increased negative self-beliefs while controlling for the effect of attachment avoidance, and vice versa, in both non-clinical and clinical samples (Tables 3 and 4).
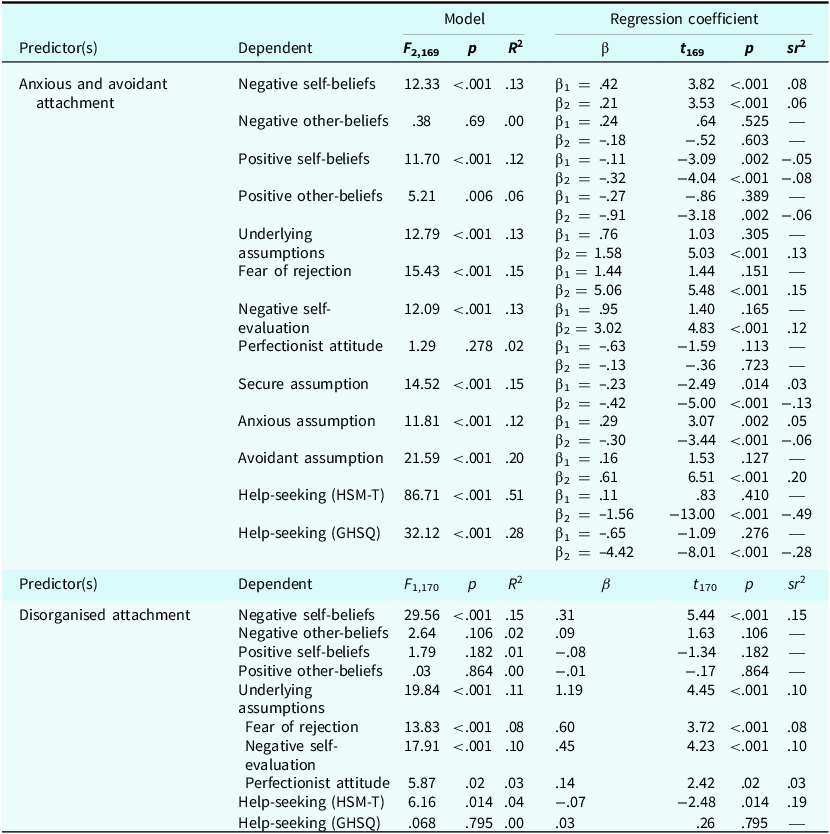
Regression analyses in the non-clinical sample

HSM-T, Help-Seeking Measure Trait; GHSQ, General Help-Seeking Questionnaire. β, unstandardized regression coefficient. β1, the effect of anxious attachment while controlling for the effect of avoidant attachment. β2, the effect of avoidant attachment while controlling for the effect of anxious attachment. sr2, squared semi-partial regression coefficient.
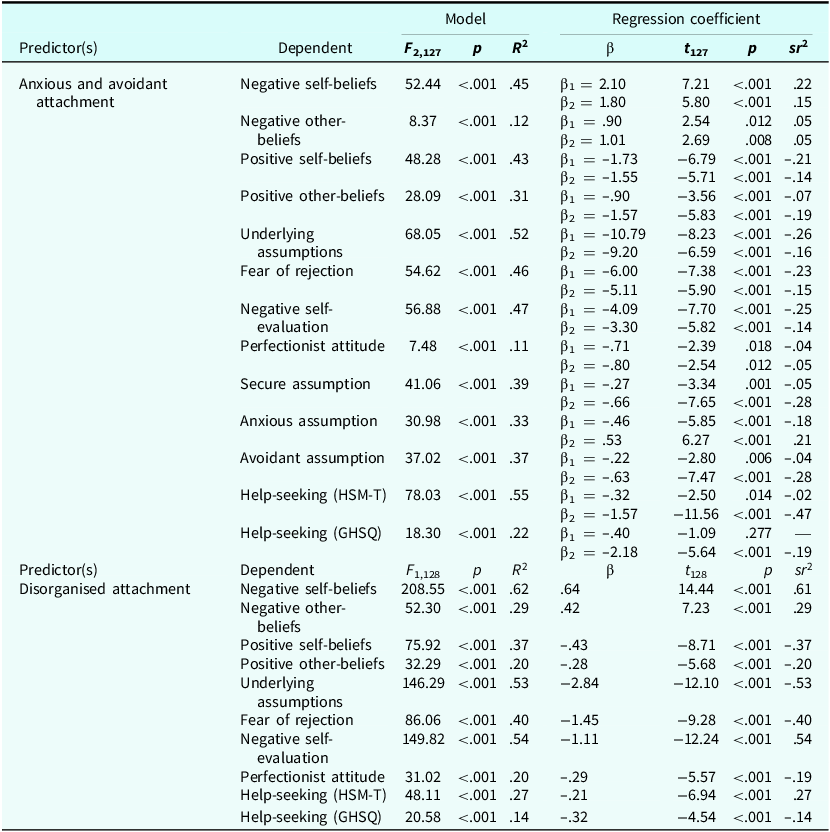
Regression analyses in the clinical sample

HSM-T, Help-Seeking Measure Trait; GHSQ, General Help-Seeking Questionnaire. β, unstandardized regression coefficient. β1, the effect of anxious attachment while controlling for the effect of avoidant attachment. β2, the effect of avoidant attachment while controlling for the effect of anxious attachment. sr2, squared semi-partial regression coefficient.
Attachment anxiety and avoidance (ECR-12) were not associated with negative beliefs about others in the non-clinical group, but were associated in the clinical group (Tables 1 and 2). In the non-clinical group, attachment anxiety did not predict negative other-beliefs while controlling for attachment avoidance, or vice versa (Table 3). However, in the clinical group, increased attachment anxiety predicted increased negative other-beliefs while controlling for attachment avoidance, and vice versa (Table 4).
Is insecure attachment associated with problematic underlying assumptions?
In the non-clinical group, attachment avoidance was positively associated with problematic underlying assumptions (total score, 32 items), but attachment anxiety was not; in this group, increased attachment avoidance predicted increased problematic underlying assumptions while controlling for attachment anxiety, although attachment anxiety did not predict problematic underlying assumptions while controlling for attachment avoidance (Table 3). In the clinical group, attachment anxiety and avoidance were negatively correlated with underlying assumptions (total score, 32 items); in this group, increased attachment anxiety predicted decreased problematic underlying assumptions while controlling attachment avoidance, and vice versa (Table 4).
Is insecure avoidant attachment associated with help-seeking?
In the non-clinical group, help-seeking (on both HSM-T and GHSQ) was negatively correlated with attachment avoidance but not associated with attachment anxiety; in this group (on both measures), increased attachment avoidance predicted decreased help-seeking while controlling for attachment anxiety, and attachment anxiety did not predict help-seeking while controlling for attachment avoidance. In the clinical group, help-seeking (on both measures) was negatively correlated with attachment anxiety and avoidance; in this group, increased attachment avoidance predicted decreased help-seeking (both measures) while controlling anxious attachment (and vice versa for HSM-T but not GHSQ).Footnote 2
Is disorganised attachment associated with beliefs about self and others, underlying assumptions and help-seeking intentions?
In the non-clinical group, disorganised attachment was positively associated with negative self-beliefs and problematic underlying assumptions (all three factors), and negatively associated with help-seeking on the HSM-T, though not associated with negative other-beliefs, positive self-/other-beliefs, or help-seeking on the GHSQ (Table 1). In the non-clinical group, increased disorganised attachment predicted increased negative self-beliefs, more problematic underlying assumptions (all three factors), and decreased help-seeking (on the HSM-T), but did not predict negative other-beliefs, positive self-/other-beliefs, or help-seeking (on the GHSQ).
In the clinical group, disorganised attachment was positively correlated with negative self- and other-beliefs and negatively correlated with positive self and other beliefs. Disorganised attachment was negatively correlated with problematic underlying assumptions (all three factors), and help-seeking (on both HSM-T and GHSQ) (Table 2). In this group, increased disorganised attachment predicted increased negative self- and other-beliefs and decreased positive self- and other-beliefs, decreased underlying assumptions (all three factors), and decreased help-seeking (on both HSM-T and GHSQ).
Exploratory regression analyses
Is insecure attachment (anxious/avoidant) associated with positive beliefs about self/others?
In both non-clinical and clinical groups, attachment anxiety and avoidance (using the ECR-12) were negatively associated with positive self-beliefs; in both groups, increased attachment anxiety predicted decreased positive self-beliefs while controlling for the effect of attachment avoidance, and vice versa.
In the non-clinical group, attachment avoidance (but not anxiety) was negatively correlated with positive other-beliefs; in this group, increased attachment avoidance predicted decreased positive other-beliefs while controlling for the effect of attachment anxiety (although not vice versa). In the clinical group, both attachment anxiety and avoidance were negatively associated with positive other-beliefs; in this group, increased attachment anxiety predicted decreased positive other-beliefs while controlling for the effect of attachment avoidance, and vice versa.
Discussion
In this study, we aimed to determine whether attachment style is associated with key therapeutic targets (or potential treatment targets) in CBT for psychosis: (1) beliefs about self and others, (2) underlying assumptions, and (3) help-seeking intentions. While CBT first targets automatic thought level appraisals and behaviours linked to psychosis experience, therapy often extends to addressing beliefs about self and others, and underlying assumptions, particularly when initial interventions have not effected sufficient change in line with personal goals (e.g. Garety et al., Reference Garety, Kuipers, Fowler, Freeman and Bebbington2001; Morrison, Reference Morrison2001). Additionally, we suggest that a focus on help-seeking as a particular category of behaviour is likely to benefit those who are also insecurely attached.
We ran the study with both an analogue sample with elevated paranoia, and a clinical sample with self-reported psychosis to assess these associations across the psychosis continuum. Both groups reported high levels of paranoia, and the clinical group also reported frequent hallucinatory experience, supporting generalisability of findings.
In both groups, attachment anxiety and avoidance were associated with negative self-beliefs. Attachment anxiety and avoidance were also associated with negative other-beliefs in clinical but not analogue participants. Attachment avoidance was associated with lower help-seeking intentions in both groups, and attachment anxiety was associated with lower help-seeking intentions in clinical participants.
Disorganised attachment was associated with more negative self-beliefs and lower help-seeking intentions in both groups, and more negative other-beliefs in clinical participants. The exploratory analyses showed that both attachment anxiety and avoidance were associated with less positive self- and other-beliefs in the clinical group, and that attachment avoidance was also associated with lower positive self- and other-beliefs in the analogue group.
These results largely align with our hypotheses regarding self- and other-beliefs, and help-seeking intentions. Interestingly, predictions regarding underlying assumptions were broadly as expected for the analogue sample, but contrary to hypotheses for the clinical group. These results show that attachment style was associated with key treatment targets in CBT for psychosis (beliefs about self and others, underlying assumptions, and help-seeking intentions), as described below.
For people with elevated paranoia in the general population, those with attachment anxiety are likely to have more negative self-beliefs and lower positive self-beliefs. This, together with the fact that attachment anxiety was not associated with other-beliefs (positive or negative), raises the interesting question of whether targeting self-beliefs may be more effective than targeting other-beliefs in groups vulnerable to psychosis, and whether this in turn leads to reduced paranoia. People with elevated levels of non-clinical paranoia and attachment avoidance are also likely to have more negative self-beliefs, lower positive self-beliefs, lower positive other-beliefs, more problematic underlying assumptions, and lower help-seeking intentions. With the increasing emphasis on community, preventative and early interventions (Darzi, Reference Darzi2024), these results have implications for emerging UK services designed for people at elevated risk of psychosis (cf. Salazar de Pablo et al., Reference Salazar de Pablo, Davies, de Diego, Solmi, Shin, Carvalho and Fusar-Poli2021).
For people with psychosis, we found clear and consistent evidence that those who are also insecurely attached (anxious, avoidant or disorganised) are likely to report more negative self- and other-beliefs, lower positive self- and other-beliefs, and lower help-seeking intentions. This is likely to account for hesitancy in seeking, accepting and remaining engaged in recommended interventions such as CBT, and indicates potential flexibility in treatment targets at the point of initial contact. This group is likely to be particularly vulnerable to longer DUP and early disengagement from CBT and other therapies, if we do not take account of these cognitive and behavioural barriers to help-seeking.
The unexpected results regarding underlying assumptions require replication before drawing any firm conclusions. The measure used may not have been appropriate, particularly for the clinical group. Importantly, the number of questionnaire items endorsed does not necessarily equate to severity of impact – in clinical practice we know that a single problematic assumption held with a high level of conviction can have a considerable effect on an individual’s distress, interpretation of events, and functioning. Clinically viable measures of the impact of underlying assumptions would be extremely valuable for future studies.
Disorganised attachment is characterised by high levels of anxious and avoidant attachment behaviours without a discernible pattern (Main and Hesse, Reference Main, Hesse, Greenberg, Cicchetti and Cummings1990; Main and Soloman, Reference Main, Solomon, Brazelton and Yogman1986; Main and Soloman, Reference Main and Solomon1990; Mikulincer and Shaver, Reference Mikulincer and Shaver2007). We found that disorganised attachment was associated with negative self-beliefs, problematic underlying assumptions and lower help-seeking intentions in the analogue group, and negative and positive self- and other-beliefs, and lower help-seeking intentions in the clinical group. Exploration of associations between disorganised attachment and therapeutic targets in CBT, namely beliefs, assumptions and behaviours, is both novel and potentially significant (if replicated) given the prevalence of disorganised attachment in non-clinical and clinical populations with paranoia.
Limitations
This study is limited by a cross-sectional design and reliance on self-reported psychosis in the clinical sample, and an analogue sample with high levels of paranoia as a proxy for psychosis vulnerability. Experimental and longitudinal studies with participants whose presentations have been verified are now needed to examine causal (potentially mediating) links between attachment style, beliefs, assumptions and behaviours in psychosis and vulnerability to psychosis. Furthermore, while the two groups are on the psychosis continuum, they do not represent the full range or severity of psychosis experience. Additionally, the internal consistency of the PAM-R (analogue sample) and GHSQ (clinical sample) were unsatisfactory. This may be because the PAM-R was designed for clinical groups, and the GHSQ has not been validated with a clinical psychosis sample to our knowledge. We therefore relied on alternative measures (ECR-12 and HSM-T) for our analyses and interpretation.
Research implications
Based on the current results, we recommend future research:
-
(1) Examine causal links between attachment and CBT relevant variables, and whether interpersonal beliefs and assumptions mediate the relationship between insecure attachment and help-seeking in people vulnerable to or with established psychosis.
-
(2) Determine whether attachment style predicts engagement and/or drop-out in CBT and other recommended treatments for psychosis.
-
(3) Investigate whether CBT targeting attachment congruent factors (beliefs and help-seeking) improves retention and outcomes for people with psychosis who are also insecurely attached.
-
(4) Investigate whether it is more effective to target positive or negative self- or other-beliefs with people with elevated paranoia who are insecurely attached, and whether this reduces paranoia.
Public health, service level, and clinical implications
Our findings indicate that attachment style affects cognitive and behavioural factors contributing to the maintenance of distressing psychosis, including poor help-seeking. In line with previous findings (Dozier et al., Reference Dozier1990; Sood et al., Reference Sood, Carnelley and Newman-Taylor2022a), our results suggest that people with psychosis or high levels of non-clinical paranoia who are also insecurely attached are likely not to seek help when needed. Public health campaigns should target adolescents and their families via schools and colleges to improve mental health literacy and healthcare pathways, specifically regarding: the nature of psychosis (alongside other severe mental health conditions), treatment options, how and where to seek help, likely obstacles (including understandable ambivalence about help-seeking for those who are also insecurely attached), and optimism regarding likely outcomes (cf. Skrobinska et al., Reference Skrobinska, Newman‐Taylor and Carnelley2024; Tiller et al., Reference Tiller, Maguire and Newman-Taylor2023).
Our results also suggest that young people with psychosis who are insecurely attached are at risk of dropping out of treatments prematurely following initial contact with services. This group are likely to benefit from an early and explicit focus on engagement to encourage people to stay in therapy and access ‘full dose’ CBT and other recommended treatments. As service leads and clinicians, we can:
-
(1) Routinely measure both attachment (e.g. ECR-12 and PAM-R) and help-seeking intentions (e.g. HSM-T), considering the psychometric limitations of these tools alongside practical benefits such as self-report format and length.
-
(2) Prioritise engagement for people scoring highly on insecure attachment – pay particular attention to the therapeutic relationship and consider interventions that foster felt security and effective help-seeking (cf. Liu et al., Reference Liu, Carnelley and Newman-Taylor2025; Pitfield et al., Reference Pitfield, Maguire and Newman-Taylor2020).
-
(3) Name beliefs about self and others, and help-seeking (or self-reliance) behaviours when formulating, and target these in therapy, knowing they will be activated at times of perceived threat.
-
(4) In acute, forensic and other in-patient or residential settings – consider attachment informed approaches to case conceptualisation (e.g. Berry et al., Reference Berry, Haddock, Kellett, Roberts, Drake and Barrowclough2016; Bucci et al., Reference Bucci, Roberts, Danquah and Berry2014; Newman-Taylor et al., Reference Newman-Taylor, Harper, Maguire, Sivyer, Sapachlari and Carnelley2022; Newman-Taylor and Sambrook, Reference Newman-Taylor and Sambrook2012) to facilitate effective interactions, reduce restrictive practice (cf. Salzmann-Erikson and Yifter, Reference Salzmann-Erikson and Yifter2020) and improve recovery outcomes.
In terms of service level implications, assertive outreach approaches aim to engage people with psychosis for whom traditional services are often ineffective, although most of the dedicated teams set up in the 1990s have now been disbanded and the function passed to already over-stretched community mental health teams. A gently persistent approach that gives the person with psychosis an opportunity to learn that they can trust and rely on others is likely to be essential for people who are insecurely (particularly avoidantly) attached in community and acute care settings.
Conclusion
Insecure attachment is associated with problematic beliefs and reduced help-seeking in analogue and clinical psychosis groups. Duration of untreated psychosis remains an international priority (World Health Organisation, 2001), and a third of people with psychosis drop out early from recommended interventions (Doyle et al., Reference Doyle, Turner, Fanning, Brennan, Renwick, Lawlor and Clarke2014; Kreyenbuhl et al., Reference Kreyenbuhl, Nossel and Dixon2009). Insecure attachment is likely to constitute an important barrier to seeking, accepting and continuing to accept help, including CBT for psychosis.
This is the first study to map out the beliefs, assumptions and behaviours associated with anxious, avoidant and disorganised attachment in analogue and clinical psychosis samples with elevated paranoia. By articulating attachment patterns in terms of self- and other-beliefs, underlying assumptions, and help-seeking intentions, we can anticipate likely barriers to initial and ongoing engagement, and target these in public health campaigns and early in therapy to improve initial access to recommended treatments, ongoing engagement, and recovery outcomes.
Key practice points
-
(1) An individual’s attachment style is associated with specific cognitive and behavioural factors contributing to the maintenance of distressing psychosis.
-
(2) People with psychosis who are also insecurely attached are at risk of delaying contact with services, and then dropping out of recommended treatments early.
-
(3) As CBT clinicians, we can assess attachment to inform formulation and treatment planning.
-
(4) People with an insecure attachment style are likely to benefit from a clear focus on the therapeutic relationship and interventions that foster felt security very early in therapy.
-
(5) Beliefs about self and others, linked assumptions, and help-seeking (or self-reliance) behaviours can be named in the formulation and targeted in therapy, and this may improve engagement and outcomes in CBT for psychosis.
Supplementary material
To view supplementary material for this article, please visit https://doi.org/10.1017/S1754470X26100543
Data availability statement
The data that support the findings of this study are available from the corresponding author, upon reasonable request.
Acknowledgements
The authors would like to thank Kylise Palmer, Muskan Samani and Amelia Lawrence, who helped with data management. Thanks also go to our students – Rebekah Carrington, Sophia De Araujo, Molly Jordan, Sylvia Maneiro, Jessica O’Callaghan and Jack Ockwell – who drew on this data for their projects and raised thoughtful questions in supervision.
Author contributions
Katherine Newman-Taylor: Conceptualization (lead), Investigation (equal), Writing - original draft (lead), Writing - review & editing (equal); Monica Sood: Data curation (lead), Formal analysis (lead), Investigation (equal), Writing - original draft (supporting), Writing - review & editing (equal); Alison Bennetts: Conceptualization (supporting), Investigation (equal), Writing - review & editing (equal); Katherine Carnelley: Investigation (equal), Writing - review & editing (equal); Tess Maguire: Conceptualization (supporting), Investigation (equal), Writing - review & editing (equal).
Financial support
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Competing interests
Katherine Newman-Taylor is an Associate Editor for the journal. She was not involved in the review or editorial process for this paper. The other authors have no declarations.
Ethical standards
The authors have abided by the Ethical Principles of Psychologists and Code of Conduct as set out by the BABCP and BPS. We obtained informed consent from participants to take part and for results to be published.




 Open access
Open access
Comments
No Comments have been published for this article.