

Introduction
In 2021, the National Institute of Minority Health and Health Disparities (NIMHD) funded a portfolio of research centers to accelerate the prevention, treatment, and management of multiple chronic diseases that disproportionately affect populations facing health disparities. The portfolio includes 11 regional research centers and a coordinating center. This consortium, the Health Excellence Action Network (HEAN), is charged with conducting interventions to advance health in multiple chronic disease outcomes by addressing the social determinants of health at two or more levels of influence [Reference Pardo, Joseph and Rojo1,2]. This communication describes the development and implementation of one of the 11 research centers, namely, the Forge AHEAD (Achieving Health Excellence Across the Deep South) Center.
Alabama (AL), Mississippi (MS), and Louisiana (LA) represent the heart of the Deep South region of the United States, which has the highest cardiovascular disease (CVD) rates in the nation [3]. These high CVD rates can be attributed, in part, to the high prevalence of cardiometabolic risk factors, including obesity, diabetes, and hypertension across the region [Reference Yasmin, Moeed and Ur Rahman4,Reference Uddin, Zhu and Malla5]. There are significant disparities in the burden of these chronic conditions, with higher prevalences and shortened life expectancy among Black adults and those with low income [6–Reference Benson9]. Among the 50 states plus the District of Columbia, AL, MS, and LA have the 45th, 49th, and 51st highest rates of poverty in the country [Reference Benson9]. Moreover, disparities in cardiometabolic outcomes by education level and other measures of economic stability such as food insecurity and housing instability are well documented [Reference Jia, Carnethon, Wong, Lewis, Schreiner and Kandula10–Reference Amireh and Makaryus15]. Rurality is another important contributor to cardiometabolic health disparities in the Deep South given the high proportion of rural-dwelling residents (AL, 45%; MS, 51%; LA, 31%) and the higher rates of cardiometabolic disease among rural compared to urban residents in the U.S. [Reference Pierce, Ng, Stouffer, Williamson and Stouffer16].
Reducing health disparities in the Deep South requires comprehensive approaches targeting multiple cardiometabolic risk factors from individual to societal levels. Obesity, diabetes, and hypertension frequently co-occur, with lifestyle modification serving as the cornerstone of initial treatment [17–Reference Krist and Davidson19]. A precision public health approach, described below, emphasizes contextual factors, including multi-level social and structural determinants of health. Sustainability of these approaches requires partnerships with the communities and organizations where evidence-based interventions are translated and implemented. The name Forge AHEAD reflects the Center’s collaborative foundation – it was developed through close input from academic and community partners to represent their shared vision of progress and partnership across the Deep South.
Center overview
Mission and Aims
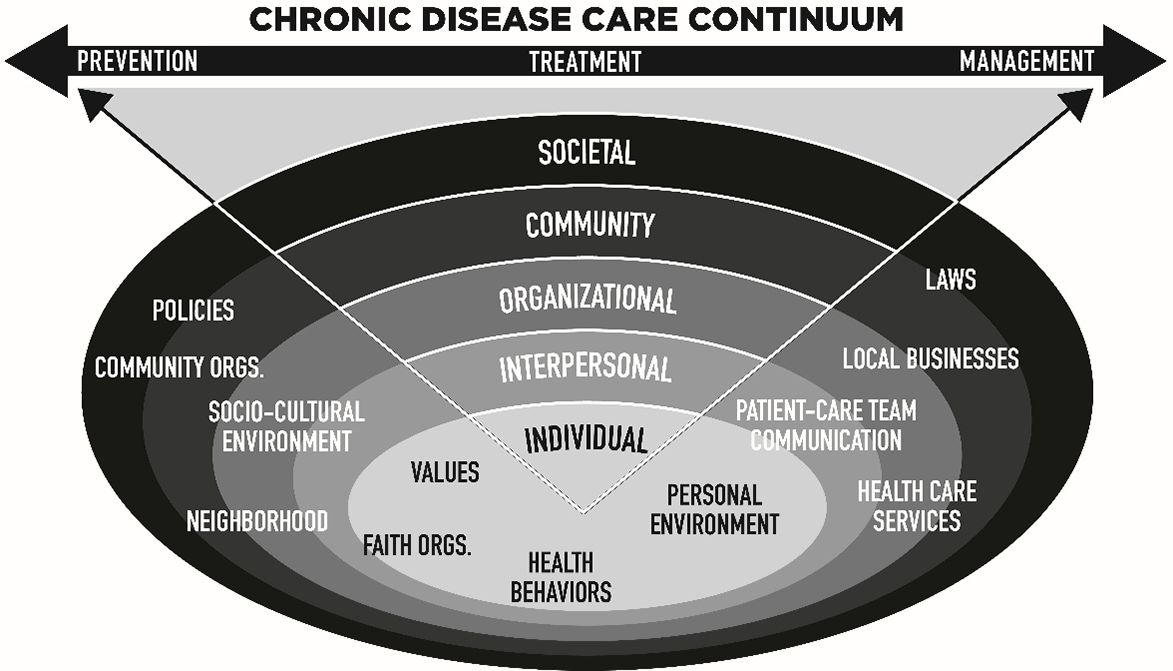
The mission of the Forge AHEAD Center is to improve health outcomes and reduce the burden of cardiometabolic diseases across the Deep South, with a particular focus on obesity, diabetes, hypertension, and related risk factors and complications from these chronic diseases. The Center focuses on disparities among populations who suffer disproportionately from these conditions across AL, MS, and LA (i.e., primarily Black and low-income adults). The Center is thematically focused on the application of a precision public health approach across the care continuum to reduce the burden of cardiometabolic disease. Precision public health is best viewed as “providing the right intervention to the right population at the right time” and recognizes that, to have an impact on population health, initiatives must acknowledge the importance of individual beliefs, preferences, culture, context, and policy, among other factors [Reference Khoury, Iademarco and Riley20,Reference Olawsky, Keohane and Roberts21]. This means intervening at multiple levels of influence (from the individual to the societal level), and across multiple domains of influence, including biologic and behavioral domains, the sociocultural and built environments, and healthcare systems, as is described in the NIMHD research framework [22]. To maximize impact, this also requires addressing the full continuum of care, including prevention (addressing risk factors and early stages of a condition, e.g., prediabetes), treatment (increasing access to or quality of healthcare), and management (self-management for chronic diseases and co-existing complications; Figure 1).
Conceptual framework for the application of the precision public health approach at multiple levels of the socio-ecologic framework and across the care continuum.

Figure 1. Long description
The diagram illustrates the chronic disease care continuum, which spans prevention, treatment, and management. It features concentric layers representing different levels of influence: societal, community, organizational, interpersonal, and individual. Each layer includes specific factors such as laws, local businesses, policies, community organizations, socio-cultural environment, neighborhood, faith organizations, patient-care team communication, health care services, values, personal environment, and health behaviors. Arrows indicate the flow from prevention to management, emphasizing the interconnectedness of these factors in addressing chronic diseases.
The Center consists of 4 primary institutions from 3 contiguous states in the heart of the Deep South (the University of Alabama at Birmingham [UAB], Tuskegee University, Pennington Biomedical Research Center [PBRC], and the University of Mississippi Medical Center) (Figure 2). The Center leverages an existing foundation of internally and externally supported infrastructure, including Nutrition Obesity Research Centers (UAB and PBRC); the Diabetes Research Center (UAB); Institutional Development Award Networks for Clinical and Translational Research (LA Clinical and Translational Science Center and MS Center for Clinical and Translational Research); and the Center for Clinical and Translational Science (CCTS; the Clinical and Translational Science Awards hub at UAB), which consists of an 11-member Partner Network that provides an existing platform for dissemination of investigator development opportunities. Forge AHEAD has launched a collective effort to reduce the persistent burden of cardiometabolic diseases and promote translational research by increasing crosstalk between these institutions as well as within each institution, creating an additive effect possible only through collaboration. As such, the Center’s short-term goal is to extend cardiometabolic research into real-world community and clinical settings in the Deep South to achieve the long-term goal of improving health outcomes in the region. The specific aims of the Center include:
Administrative structure of the Forge AHEAD Center.

Figure 2. Long description
The diagram illustrates the administrative structure of the Forge AHEAD Center, which is divided into several key components. At the top, it features the Pennington Biomedical Research Center, Tuskegee University, University of Alabama at Birmingham, and University of Mississippi Medical Center. Below these institutions, the structure is divided into three main boards: the Scientific Advisory Board, the Executive Committee, and the Community Advisory Board. These boards oversee three core areas: the Investigator Development Core, the Administrative Core, and the Community Engagement Core. The diagram further breaks down into Primary Research Projects, Supplemental Research Projects, and Pilot Projects, each with specific initiatives and funding details. The relationships and flow between these components are clearly depicted to show the center’s comprehensive approach to reducing disparities in chronic diseases.
-
1. Create intellectual synergy by linking investigators across the region and coordinating with existing Centers to identify areas of research collaboration and innovation through regular scientific seminars, annual regional meetings, and bi-annual scientific advisory board meetings.
-
2. Expand the region’s workforce of investigators focused on translational research in chronic disease through enrichment activities and a pilot and feasibility grant program.
-
3. Promote bidirectional collaborations between researchers and non-academic partners in all phases of research and beyond.
-
4. Advance empirical knowledge through rigorous and innovative research projects that will evaluate multi-level and multi-domain interventions, informed by academic and community partners in the region, to improve cardiometabolic health outcomes.
-
5. Promote sustainable impact through widespread dissemination of Center-generated scientific discovery to academic, clinical, community, public health, and policy stakeholders across the region.
Center design, governance, and structure
The Forge AHEAD Center brings together an interdisciplinary group of scientists with complementary skills and expertise relevant to cardiometabolic disease and health outcomes research. Center activities are administratively managed by an Executive Committee. The Center, which was funded in September 2021, comprises an Administrative Core responsible for the overall Center operations, an Investigator Development Core (IDC) responsible for funding pilot proposals and Scholar professional development, a Community Engagement Core (CEC) responsible for facilitating community engagement in all phases of the translational research process, and three R01-level research projects (Figure 2). Additional funding was awarded in September 2022 and October 2023 to expand one of the primary research projects to include individuals living with HIV, and to fund additional awards in the pilot and feasibility grant program. The Center is supported by a Scientific Advisory Board of leaders from regional institutions and affiliated organizations who provide scientific and administrative guidance for the Center, as well as a 12-person Community Advisory Board (CAB) focused on advising Center leaders and pilot project investigators and engaging in long-term strategic planning.
Center projects
The project selection process was guided by several overarching principles and goals, including identification of research projects that collectively: (1) address multiple cardiometabolic conditions; (2) span different levels of the cardiometabolic disease care continuum (prevention, treatment, and management); (3) focus on populations with high burden of cardiometabolic disease disparities; (4) address multiple levels of influence on health outcomes; (5) include meaningful involvement of at least one nonacademic clinical and/or community partner; (6) represent the geographic heterogeneity of the region; and (7) involve investigators across multiple institutions in the region. Three primary projects, Projects 1 through 3, were selected, developed, and submitted in the initial grant application, whereas Projects 4 through 7 were selected and submitted in a competitive revision in July 2023.
Project 1: Stepping into Lifestyle Changes (SILC). The SILC study is a hybrid type 3 implementation trial [Reference Curran, Bauer, Mittman, Pyne and Stetler23] of a multi-level lifestyle modification intervention combining lay health educators and home gardens on weight management, diabetes prevention, and hypertension control. The study includes Black women with overweight or obesity plus prediabetes or hypertension from 12 rural counties in AL and MS.
Project 2: Promoting Successful Weight Loss in Louisiana Using Information Technology (PROPEL-IT). PROPEL-IT is a hybrid type 1 implementation trial [Reference Curran, Bauer, Mittman, Pyne and Stetler23] of a remotely delivered weight loss program using patient portals through electronic medical records and augmented with health coaches embedded in the digital medicine program of a large healthcare organization. The study includes Black adults with obesity plus prediabetes or diabetes in a large health system in LA.
Project 3: Food Delivery, Remote Monitoring, and Coaching-Enhanced Education for Optimized Diabetes Management (FREEDOM). The FREEDOM study is a type 1 hybrid optimization-implementation trial [Reference Curran, Bauer, Mittman, Pyne and Stetler23] using a randomized factorial design-based multiphase optimization strategy (MOST). Based on three intervention components, including: (1) digital health coaching, (2) remote patient monitoring, and (3) stable-shelf food boxes, this study evaluates which combinations of intervention components are optimal for improving glycemic control among medically complex Black adults with uncontrolled diabetes and cardiorenal disease in two university health systems and one safety-net health system in MS and AL.
Project 4: Teen Mom Study. This is a hybrid cluster randomized trial designed to evaluate the effects of a multi-level, multicomponent digital health intervention versus usual care on moderate-to-vigorous physical activity and blood pressure at 26 and 36 weeks’ gestation. The study includes pregnant Black adolescents participating in the Women, Infants, and Children (WIC) federally funded nutrition program in MS.
Project 5: Remotely Delivered Resistance Training for Cardiometabolic Health among Black Women: A Pilot Trial. The objective of this pilot trial is to examine the feasibility, acceptability, and preliminary efficacy of a remotely delivered resistance training intervention among Black women in Birmingham, AL.
Project 6: Remotely Delivered Mindfulness-Based Diabetes Education for Rural Adults with Uncontrolled Diabetes and Elevated Distress. This is a pilot trial to test the effect of Mindfulness-Based Diabetes Education, which integrates Mindfulness-Based Stress Reduction and Diabetes Self-Management Education, on glycemic control in an urban safety-net healthcare system in rural AL.
Project 7: Weight Inclusive Adaptive Strategies to Enhance Cardiometabolic Health in Black Adults Health Study. The primary aim of this study is to determine the feasibility and preliminary effectiveness of a Sequential Multiple Assignment Randomized Trial (SMART) to compare weight-focused or weight-neutral biobehavioral interventions for improving cardiometabolic health among Black adults in Birmingham, AL.
Monitoring center progress
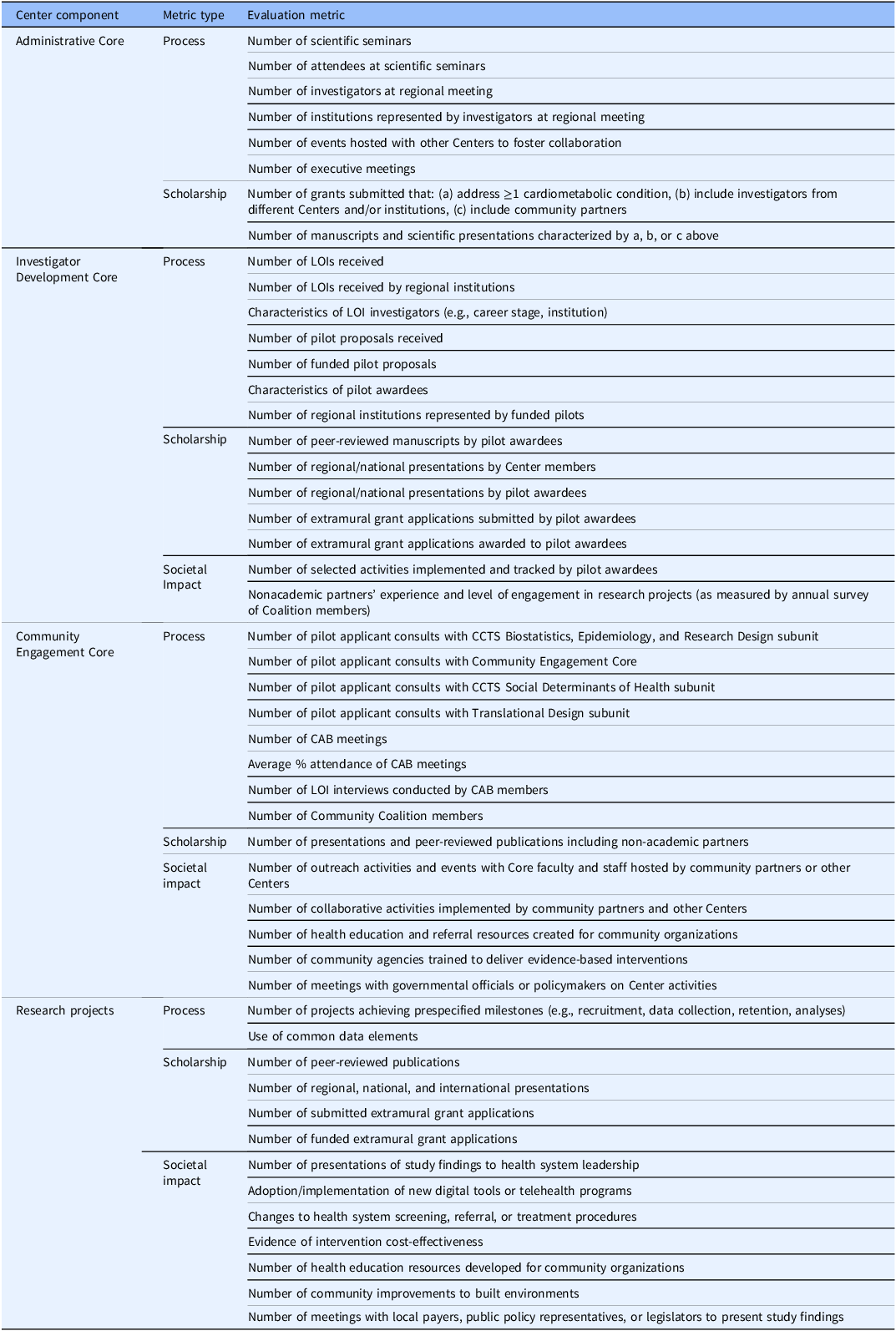
Annual evaluations of the Center overall and its specific components (i.e., Cores and Projects) are based on a combination of metrics including: (1) process measures, (2) measures of scholarly output, and (3) indicators of societal impact (Table 1). For tracking potential societal impact, evaluation metrics are guided by the Translational Science Benefits Model (TSBM), a novel framework for evaluating clinical and community health impacts beyond the more typical biblio-metric measures [Reference Luke, Sarli and Suiter24]. This model includes 30 measurable indicators that reflect possible downstream health and societal benefits (e.g., translation of scientific discoveries into new clinical procedures, products, or techniques; adoption of new healthcare guidelines; policy changes; increased healthcare access; delivery of community-based health services; improvements in life expectancy). While it remains challenging to measure and demonstrate the direct influence of research on some of these downstream effects, the Administrative Core has identified short-term indicators of societal benefit (e.g., reduced financial costs for care; meetings with health system administrators or policymakers to review Center research findings). Longer term indicators of societal benefit are expected to emerge as projects are completed and through continued input from community partners.
Center evaluation metrics

Table 1. Long description
The table presents evaluation metrics for a center and its components, including the Administrative Core, Investigator Development Core, Community Engagement Core, and Research Projects. It is structured with three main columns: Center Component, Metric Type, and Evaluation Metric. The table has multiple rows detailing specific metrics under each core. The Administrative Core tracks process measures such as the number of scientific seminars, attendees, and executive meetings, as well as scholarship metrics like grants submitted and manuscripts published. The Investigator Development Core focuses on the number of Letters of Intent (LOIs) received, funded pilot proposals, and scholarly output. The Community Engagement Core measures process through consults and meetings, scholarship through presentations and publications, and societal impact through outreach activities and policy meetings. Research Projects are evaluated based on milestones, publications, grant applications, and societal impact indicators. The table aims to capture the center’s overall performance and societal impact using a combination of process, scholarly, and impact metrics.
LOI = Letter(s) of Intent; CCTS = Center for Clinical and Translational Science; CAB = Community Advisory Board.
Note: Metrics are collected quarterly and evaluated at the end of each grant year (June 30). Overall evaluation will occur upon grant completion on June 30, 2026.
Early-stage investigator pilot program
The IDC directs a competitive pilot program to enable early-stage investigators to accelerate innovative ideas while attaining research development training in the conduct of research related to dissemination and implementation, comparative effectiveness, and translation of evidence-based interventions for real-world settings (i.e., T3–T4 research). Toward this goal, the IDC funds one-year $50,000 pilot grants on a competitive basis and fosters the career development of investigators through training programs that complement the execution of pilot research.
Early-stage or new investigators are eligible to submit a Letter of Intent (LOI) for pilot funding. The Scientific Review Committee (SRC), with representation from the CAB, reviews LOIs for scientific merit using NIH scoring criteria, after which meritorious applicants are invited to submit full (four-page) research proposals expanding upon project aims, significance, innovation, and approach. Proposals are reviewed by two Core faculty and two CAB members, selected based on expertise. Then the SRC evaluates applications using prespecified criteria assessing scientific and community engagement factors and assigns a priority score using the NIH scale (1–9) to guide funding decisions. The Center funds 6–10 projects annually. To strengthen the pilot and feasibility program and set it apart as a unique professional development opportunity designed to train pilot awardees (“Scholars”) in true interdisciplinary team science, the IDC offers an enrichment series of monthly seminars, workshops, and regional symposia on translational methods to advance ongoing cardiometabolic research. Each Scholar is supported by a Project Management Team for ongoing engagement and oversight. Together these components support research project management, skills and professional development, and peer mentoring.
To date, the Center has awarded 34 pilot awards to 32 investigators across 5 institutions. Forge AHEAD scholars have produced over 200 peer-reviewed publications and nearly 100 scientific presentations during their affiliation with the Center. As of February 2026, 11 publications are directly attributable to their Center-funded projects. In addition to tracking scholarship products and extramural grant support, the IDC tracks short-term metrics of potential health and societal benefits. Finally, the IDC conducts follow-up surveys of pilot awardees to assess career advancement, engagement in teams, and project impact including bibliometric analysis and other innovative methods. Feedback from funded Scholars is reviewed by the IDC co-directors to identify opportunities to strengthen program effectiveness.
CEC evaluation
The role of the CEC is guided by the Community-Based Participatory Research philosophical framework [Reference Duke and Aldenderfer25] and Havelock’s Research Development Dissemination Utilization theoretical framework [Reference Havelock26], and consistent with the TSBM used in the overall evaluation of the Center. The CEC focuses on activities that maximize bidirectional communication between researchers and community stakeholders, co-learning, and broad dissemination of research findings. The CEC accomplishes this by directing the CAB, Community Coalition, and Community Microgrant programs.
CAB. An important component of the CEC, the CAB is comprised of four members from each state, representing a variety of sectors including healthcare, civic, and faith-based organizations. Members were recruited through partner institution community contacts and existing partnerships. The CAB receives training on the research process, benefits of partnering in research, and how to evaluate opportunities for community participation in research and ensures that Center research is both informed by and actively involves the communities the Center serves. CAB members also advocated for a more active role in research activities, leading to expanded involvement in the pilot awardee selection process, including CAB review of the applicant LOIs, and requiring pilot award applicants to undergo a community engagement consult with CAB members and CEC leadership prior to funding decisions. Additionally, funded Scholars present annually to the CAB for feedback and guidance. The Center also hosts an annual Community Research Showcase to share research findings with the community. CAB members receive activity-based compensation as follows: $25 per grant review, $75 per hour for consultations, and $150 per CAB meeting, with reimbursement for out-of-pocket expenses such as travel to in-person meetings. Since the Center’s inception, the CAB has met on a monthly basis, reviewed 49 letters of intent, conducted 46 project consultations, reviewed 38 pilot grant applications, and developed innovative partnerships with 61 community-based organizations.
Community coalition. The Forge AHEAD Center has created a Community Coalition that includes representatives from multiple sectors including, but not limited to, community-based and faith-based organizations, public health agencies, and local and state government across AL, MS, and LA. The CEC has assembled a curated list of community organizations that currently function as an informal coalition as we develop the infrastructure for formalized collaborations. Collectively, this group provides local insight, strengthens the Center’s connections across the Southeast, and establishes a foundation upon which a more structured coalition will be developed.
Community Microgrant Program. The CEC implemented a Community Microgrant Program to support locally driven health promotion activities. The program provides seed funding to community-based organizations to carry out projects that address chronic disease disparities in their communities. The Microgrant Program enhances community capacity while strengthening CEC engagement with various partners and promoting sustained collaborations to reduce cardiometabolic disease burden.
Sustaining academic–community partnerships and successful interventions in the prevention, treatment, and management of cardiometabolic diseases in populations living in the Deep South is of paramount importance to the Center. The CEC views sustainability as an active process involving relationships, practices, and actions toward a common goal. The Core has personnel embedded at each partner site to collaborate with other Center leaders and community stakeholders, employing best practices from the Community Tool Box (https://ctb.ku.edu/en) and other sources to identify goals, steps to achieve them, past successes and failures, current and future barriers to success, resources needed, and metrics based on findings from the research projects.
Discussion
The Forge AHEAD Center has several notable points of innovation and impact. First, the application of a precision public health approach to address disparities in cardiometabolic diseases is novel and provides an overarching thematic framework for the entire Center. Published in 2016, the approach is gaining traction in public health circles but is not yet widely applied [Reference Khoury, Iademarco and Riley20]. Second, the Center houses expertise in methodologies relevant to translational research, including MOST, hybrid trial designs, health economics, multi-level measurement of social and structural determinants of health, and leveraging health system data. Finally, by actively engaging four academic institutions in three contiguous states, the Center increases synergy between disease-focused centers and across multiple institutions, allowing investigators to apply lessons learned on prevention, treatment, and management of obesity, diabetes, and hypertension more broadly throughout the region.
Collectively, the partner institutions have several NIH-funded Centers and cohorts that provide a foundation for the Forge AHEAD Center, including existing centers focused on cardiometabolic disease, funded cohorts and networks, and disease-agnostic centers that focus on methods and training. Our intersectional Center leverages and expands institutional resources in several ways. First, the Center engages content and methodologic experts from across the Centers and institutions to serve as mentors for early-stage investigators. Second, enrichment activities and pilot award infrastructure are leveraged to expand those proposed by the Center. The CCTS’s Partner Network provides existing infrastructure to the Center’s regional collaborations, significantly expanding the pool of potential early-stage investigator pilot award applicants and increasing opportunities to enhance the workforce, with an emphasis on investigators from groups under-represented in science. Finally, the Center has garnered $365,000 in institutional support to augment IDC activities, including pilot awards.
Implementing a multi-institutional collaborative research center revealed several foundational lessons critical for long-term success. First, early challenges such as staff turnover, transitions in key leadership roles, and the need to build rapport across various institutions highlighted the importance of deliberate structures for relationship development. Initiating kick-off meetings, collaboratively defining the Center’s Mission, Vision, and Values (Figure 3) with the CAB, and adopting transparent processes for personnel replacement proved essential for maintaining continuity and shared purpose. Second, creating and promoting synergy across the Center, including the identification and implementation of common data elements and harmonized measures across its various projects has been complex, but critical for maximizing scientific rigor, research translation, and Center contributions to reducing the burden of cardiometabolic disease across the Deep South. Third, evolving national funding priorities have underscored the necessity of flexible strategies for scaling pilot studies and the value of strong institutional champions. Sustaining wide participation has required intentional infrastructure, particularly opportunities for both structured in-person and virtual engagement supported by committed site leadership. Finally, community engagement poses additional complexities. Quarterly meetings were insufficient for maintaining meaningful involvement, prompting a shift to monthly meetings and inclusion of community representatives in more of the Center’s decision-making bodies. Maintaining engagement across geographically dispersed CAB members demands multimodal communication and investment in travel to cultivate in-person relationships. Bridging academic and community perspectives further requires bidirectional training to ensure accessible research processes and shared ownership. Collectively, these experiences emphasize adaptable planning, transparent communication, relationship building, and mutually beneficial community partnership practices, which have become hallmarks of the Center.
Forge AHEAD Center mission, vision, and values.

Figure 3. Long description
The image features the Forge AHEAD Center logo at the top, followed by three sections detailing the center’s mission, vision, and values. The mission section emphasizes improving health outcomes and reducing the burden of cardiometabolic diseases in the Deep South, focusing on obesity, diabetes, hypertension, and related risk factors. The vision section highlights achieving health equity by eliminating disparities and improving outcomes in diabetes, obesity, and hypertension through partnerships with academic, non-academic, and community organizations. The values section lists teamwork, fairness and inclusion, excellence in research, trustworthiness, transparency, and innovation as key principles to promote the center’s mission and vision.
In summary, Forge AHEAD Center’s work spans the care continuum, applying a precision public health approach to the prevention, treatment, and management of cardiometabolic diseases. The Center fosters the development and growth of the research workforce by supporting and guiding the research efforts of early-stage investigators and other trainees focused on real-world strategies to improve cardiometabolic health in the Deep South. Our partnering institutions provide access to a professionally, demographically, and geographically expansive cohort of investigators who are integrally involved in the Center’s training and research activities. Finally, the Center facilitates ongoing and meaningful collaborations between researchers and nonacademic partners (e.g., community-based organizations, health systems, and policymakers) in the region. Such collaborative efforts strengthen the impact and sustainability of research conducted in the Center because of the capacity to disseminate, translate, and integrate effective strategies into existing communities, clinical and public health organizations, and health policies in the region. Only a coordinated effort such as this has the potential to meaningfully intervene upon the significant challenge of cardiometabolic diseases and their multi-level determinants and interventions.
Acknowledgments
This publication was supported by the National Institute on Minority Health and Health Disparities (NIMHD) of the National Institutes of Health under award number P50MD017338. This research was also partially supported by the following award numbers: U54MD007585 from the NIMHD; U54GM115428 and U54GM104940 from the National Institute of General Medical Sciences; P30DK072476, P30DK056336, and U54DK137307 from the National Institute of Diabetes and Digestive and Kidney Diseases; UM1TR004771 from the National Center for Advancing Translational Sciences; T32HD071866 from the National Center for Medical Rehabilitation Research; and U54CA118623 from the National Cancer Institute. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. The authors would also like to thank the members of the Forge AHEAD Center Community Advisory Board: D’Andra Bradford Odom, Jill Buckley, George Dixon, Cheryl Ferguson, Brooke Floyd, Bernice Frazier, KiTani Lemieux, Cassandra Mobley, Evon Roquemore, Chris Williams, and Cynthia B. Wilson.
Author contributions
Gareth R. Dutton: Conceptualization, Funding acquisition, Methodology, Project administration, Resources, Supervision, Writing – review & editing: Monica L. Baskin: Conceptualization, Funding acquisition, Methodology, Project administration, Writing – review & editing: Orlando M. Gutierrez: Conceptualization, Funding acquisition, Methodology, Project administration, Resources, Supervision, Writing – review & editing: Caroline E. Compretta: Conceptualization, Funding acquisition, Methodology, Project administration, Resources, Writing – review & editing: Michael J. Mugavero: Conceptualization, Funding acquisition, Methodology, Project administration, Resources, Writing – review & editing: April A. Agne: Project administration, Validation, Writing – review & editing: Lauren Hebert-Henderson: Resources, Writing – review & editing: Trudi V. Horton: Project administration, Validation, Writing – review & editing: Rikki M. Tanner: Writing – original draft: April P. Carson: Methodology, Project administration, Resources, Writing – review & editing: Peter T. Katzmarzyk: Conceptualization, Methodology, Project administration, Resources, Writing – review & editing: Timothy Turner: Conceptualization, Investigation, Methodology, Project administration, Writing – review & editing: Tapan S. Mehta: Conceptualization, Funding acquisition, Methodology, Project administration, Resources, Writing – review & editing: Kara D. Denstel: Project administration, Writing – review & editing: Aseel El Zein: Project administration, Writing – review & editing: Michael E. Hall: Methodology, Project administration, Writing – review & editing: Sharonda Hardy: Project administration, Writing – review & editing: Eboni Price-Haywood: Methodology, Project administration, Writing – review & editing: Andrea L. Cherrington: Conceptualization, Funding acquisition, Methodology, Project administration, Resources, Supervision, Writing – review & editing.
Competing interests
The authors declare none.


 Open access
Open access