


Attention-deficit hyperactivity disorder (ADHD) is a neurodevelopmental condition defined by a persistent pattern of inattention and/or hyperactivity/impulsivity which affects functioning or development. 1 In the UK, clinical demand for ADHD assessments has greatly increased, with individuals waiting years for a diagnostic assessment in the National Health Service. Reference Smith, Mukherjee, Müller-Sedgwick, Hank, Carpenter and Adamou2 There was an increase in ADHD symptoms in children and adolescents during the COVID-19 pandemic according to a meta-analysis which included participants from 10 countries (n = 6491). Reference Rogers and MacLean3 Further, there was a global increase in ADHD medication use during the pandemic (after an initial decrease in 2020). Reference Gimbach, Vogel, Fried, Faraone, Banaschewski and Buitelaar4
There is substantial public interest in the diagnostic label, with ADHD being the seventh most common health-related hashtag on TikTok. Reference Zenone, Ow and Barbic5 Misinformation about ADHD is rife, particularly on social media. Reference Verma and Sinha6 Terminology about ADHD is also evolving, with some English-speaking community members using identity-first terminology (‘ADHDer’), rather than person-first terminology (‘person with ADHD’), as in the autistic community. Reference Kenny, Hattersley, Molins, Buckley, Povey and Pellicano7 Members of the English-speaking autistic community have argued that identity-first terminology is less stigmatising because it situates autism as an inherent part of the self, rather than an identity to be distanced from. Reference Kenny, Hattersley, Molins, Buckley, Povey and Pellicano7 However, preferences for person-first versus identity-first terminology vary by diagnostic group, with person-first language still most common in reference to those with intellectual disability. Reference Friend8 Preferences will also vary depending on language and cultural context. Research is lacking into terminology preferences in the ADHD community, including in the UK.
Public perceptions of ADHD are changing, with much greater public awareness of the condition and more focus on strengths associated with ADHD. Such changes may encourage individuals who do meet the criteria for ADHD to pursue assessment, and for those who are diagnosed, to integrate this as a positive part of their identity. ADHD is indeed seen by some individuals as reflecting an identity as well as a medical diagnosis Reference Hansson Halleröd, Anckarsäter, Råstam and Hansson Scherman9–Reference Redshaw and McCormack11 with an increasing focus on the strengths that come with ADHD, Reference Schippers, Horstman, Velde, Pereira, Zinkstok and Mostert12,Reference Sedgwick, Merwood and Asherson13 which could afford benefits to some individuals.
There are also multiple reasons why correctly taking on an ADHD identity could be harmful to well-being. First, ADHD is a stigmatised condition. Systematic reviews of qualitative studies in both adults Reference Rosenthal, Mitchell, Weisner, Silverstein, Yi and Arnold14 and children Reference Ringer15 have reported far more extensively on themes linked to negative experiences, such as self-stigma and a lack of belonging, as compared with positive experiences, such as perceived strengths including adventurousness. A systematic review that included ten studies indicated that negative attitudes towards people with ADHD are widespread in the broader community. Reference Bisset, Winter, Middeldorp, Coghill, Zendarski and Bellgrove16 Further, unlike most neurodevelopmental conditions, including autism, the features of ADHD can be mitigated through use of medication, which is highly effective. Reference Cortese, Adamo, Del Giovane, Mohr-Jensen, Hayes and Carucci17 Therefore, the identity management strategy of distancing oneself from the group ‘people with ADHD’ could be a highly effective strategy for those who respond well to medication and therefore do not always experience difficulties associated with ADHD. Indeed, qualitative studies have indicated challenges associated with ADHD, including that ADHD medication can contribute to a tension between self-acceptance and integrating ADHD into one’s sense of self. Some adults with ADHD wondered whether taking medication represented a disloyalty to one’s authentic self, while also viewing medication as a positive force in managing challenges associated with ADHD. Reference Redshaw and McCormack11
The increase in public awareness of ADHD could also lead individuals who do not meet ADHD diagnostic criteria to identify as having ADHD, when their experiences are best explained by another label, or represent an overmedicalisation of typical behaviour. Incorrectly identifying as having ADHD could lead to risky self-medication behaviour. This has implications for healthcare professionals working with individuals who self-identify as having ADHD.
Social identity theory posits that humans have a drive to belong to groups and to define ourselves and others through this group membership. Reference Tajfel, Turner, Austin and Worchel18 Social identification with particular groups has been proposed as a social cure. Reference Jetten, Haslam and Alexander19 This is because there is evidence that the number of social identities and strength of identification with social groups is associated with improved mental and physical health, including in autistic individuals. Reference Davies, Cooper, Killick, Sam, Healy and Thompson20 The self-esteem hypothesis suggests that social identification boosts self-esteem, thereby improving well-being and mental health. Reference Rubin and Hewstone21 Social identity theory therefore provides a theoretical framework that could explain how people with ADHD manage their identity, providing hypothesised pathways from ADHD social identification to well-being and better mental health, via self-esteem.
In this study, we aimed to measure ADHD social identification and preferred terminology in a sample of adults with ADHD in the UK and to understand whether ADHD social identification is related to improved self-esteem, well-being and mental health.
We hypothesised that higher scores on the ADHD social identification measure would be associated with higher self-esteem scores, which in turn would be related to higher well-being, and lower anxiety and depression scores.
We reported the sample’s ADHD terminology preferences (identity-first versus person-first), medication use and sources of learning about ADHD (i.e. professionals, influencers and community members). We investigated whether ADHD terminology preferences are associated with ADHD social identification, medication use and sources of learning about ADHD, to ultimately inform how health professionals and researchers should engage with the language and identity needs when providing medical care to people with ADHD.
Method
Participants
Three-hundred and twenty participants participated in the study. Inclusion criteria were:
-
(a) 18 years or older (with no upper age limit)
-
(b) based in the UK
-
(c) self-identify as having ADHD, or have a diagnosis of ADHD.
We chose to include both self-identified and diagnosed participants because of long adult ADHD diagnostic assessment waiting lists in the UK, since there is a substantial population of individuals who would meet the criteria, but who remain undiagnosed. This also provided the opportunity to test if psychological correlates of ADHD social identification were consistent across those with and without formal diagnosis, providing a check on the robustness and generalisability of our findings, and in line with the increasing recognition for self-identification within the neurodiversity movement. Reference Pellicano and den Houting22
A power calculation indicated that 310 participants is appropriate to achieve a power of 0.81 in the serial mediation model. Participants were recruited via the recruitment platform, Prolific, and were paid via the platform for their time.
Procedure
Participants were already members of the Prolific platform. Participants who met our eligibility criteria on Prolific were invited to participate. Potential participants were directed to an online survey platform where they could read the information sheet, and provide fully-informed consent via an online form. If participants consented to participate, they were directed to the questionnaires, which included the measures below, as well as two attention check questions. Upon completion of all measures, participants were paid £3.75, equating to approximately £10/h.
Measures
Demographic information was collected via a survey which included: age, sex, gender, educational attainment, employment, relationship status, age of ADHD diagnosis, who gave diagnosis, medication use (current frequency/past use, frequency, impact and side-effects), preferred ADHD terminology in English (person-first e.g. ‘person with ADHD’ or identity-first, e.g. ‘ADHDer’) and other psychiatric diagnoses including neurodevelopmental and mental health conditions.
ADHD social identification was measured using the Leach et al social identification scale, Reference Leach, van Zomeren, Zebel, Vliek, Pennekamp and Doosje23 adapted for ADHD. This scale measures the extent to which an individual identifies with other people with ADHD. It has two components, each containing subscales; self-investment (solidarity, satisfaction, centrality) and self-definition (individual self-stereotyping, in-group homogeneity). An example item from the satisfaction subscale is ‘I am glad to be a person with ADHD’, with responses on a seven-point Likert scale from ‘strongly disagree’ to ‘strongly agree’. This widely used scale has good psychometric properties, but is, to our knowledge, its first use in adults with ADHD. Cronbach’s α for the total score and subscale scores in this sample were good (total 0.90, solidarity 0.90, satisfaction 0.89, centrality 0.82, self-stereotyping 0.88, homogeneity 0.83).
Self-esteem was measured using a 10-item scale (Rosenberg; Cronbach’s α = 0.92 in our sample). Reference Rosenberg24 An example item is: ‘On the whole, I am satisfied with myself’, rated on a four-point Likert scale from ‘strongly agree’ to ‘strongly disagree’. This questionnaire has excellent psychometric properties, but has not been validated in adults with ADHD.
Mental health was measured via two brief questionnaires of anxiety and depression: Generalised Anxiety Disorder-7 (GAD-7) and the Patient Health Questionnaire-9 (PHQ-9). Anxiety was measured using the widely used and thoroughly validated seven-item GAD-7 questionnaire (Cronbach’s α = 0.88 in our sample) which measures anxiety symptoms over the past two weeks. Reference Spitzer, Kroenke, Williams and Löwe25 An example item is ‘Feeling nervous, anxious or on edge’. Depression was measured using the PHQ (PHQ-9; Cronbach’s α = 0.85 in our sample) which has nine-items and measures depression symptoms over the past two weeks. Reference Kroenke, Spitzer and Williams26 An example item is ‘Little interest or pleasure in doing things’. Both questionnaires are answered on a four-point Likert scale from ‘not at all’ to ‘nearly every day’.
Well-being was measured using the Warwick-Edinburgh Mental Well-being Scale (WEMWBS; Cronbach’s α = 0.92 in our sample). Reference Tennant, Hiller, Fishwick, Platt, Joseph and Weich27 This well-validated questionnaire has been used in the past with adults with ADHD. It has 14 items which are rated on a 5-point Likert scale from ‘none of the time’ to ‘all of the time’, and an example item is ‘I’ve been feeling optimistic about the future’.
Finally, we also measured the sources of participants’ learning about ADHD. This was adapted from a questionnaire previously used with autistic people. Reference Bury, Haschek, Wenzel, Spoor and Hedley28 It lists sources of learning about ADHD (e.g. professionals, influencers) and asks participants to rate how much each source has influenced their understanding of ADHD on a five-point Likert scale from ‘very much’ to ‘not at all’. Ten sources of learning were provided in the questionnaire. We recoded the ten variables so that higher scores indicated greater influence on ADHD knowledge. The ten variables were condensed down into five variables for analysis. Conceptually similar sources were grouped together (e.g. ‘online blogs’ and ‘online research’ became ‘online resources’) and scores given for each individual source were averaged across the combined variables to create a composite score. There were further questions about social media use and length of time spent on social media for each social media platform endorsed.
Data analysis
We preregistered our analysis plan (https://osf.io/2jenr/). To test H1, we conducted a serial mediation analysis using PROCESS v4.2 macro in SPSS (model 6) (version 27.0 for Windows; IBM, Armonk, New York, USA; https://www.ibm.com/support/pages/downloading-ibm-spss-statistics-27), testing the model that higher ADHD social identification scores will be associated with higher self-esteem scores, which in turn will be related to higher well-being, and lower anxiety and depression scores.
To conduct the planned exploratory analyses, we calculated descriptive statistics (e.g. describing the proportion of participants who select person-first versus ADHD-first terminology, medication use and sources of learning about ADHD). We also conducted correlations between all key study variables to investigate the associations between ADHD social identification, ADHD terminology preferences (0 = person first, 1 = ADHD first), current ADHD medication use (0 = no, 1 = yes) and lifetime medication use (0 = no, 1 = yes). A linear regression model was used to examine the association between ADHD social identification and different sources of learning about ADHD. Data across all measures, apart from the social identification total score and well-being score, violated the assumption of normality. Therefore, Spearman’s rho correlations were used unless indicated otherwise.
After receiving the data and finding a high number of participants who self-identified as having ADHD in the absence of a formal diagnosis, we decided to re-conduct the analyses with and without those who self-identified as having ADHD. This analysis was not pre-planned or preregistered, and was to assess whether there were differences between those diagnosed with ADHD compared with those who self-identified. We also decided to re-run the mediation analyses with the satisfaction subscale as the predictor variable, given our unexpected pattern of findings, which was not preregistered.
Results
A total of 320 participants took part, and one participant was excluded based on survey completion time, which was more than 1 s.d faster than the mean. This resulted in a final sample of 319 participants with a mean age of 34.96 (s.d. = 10.89, range 18–73 years).
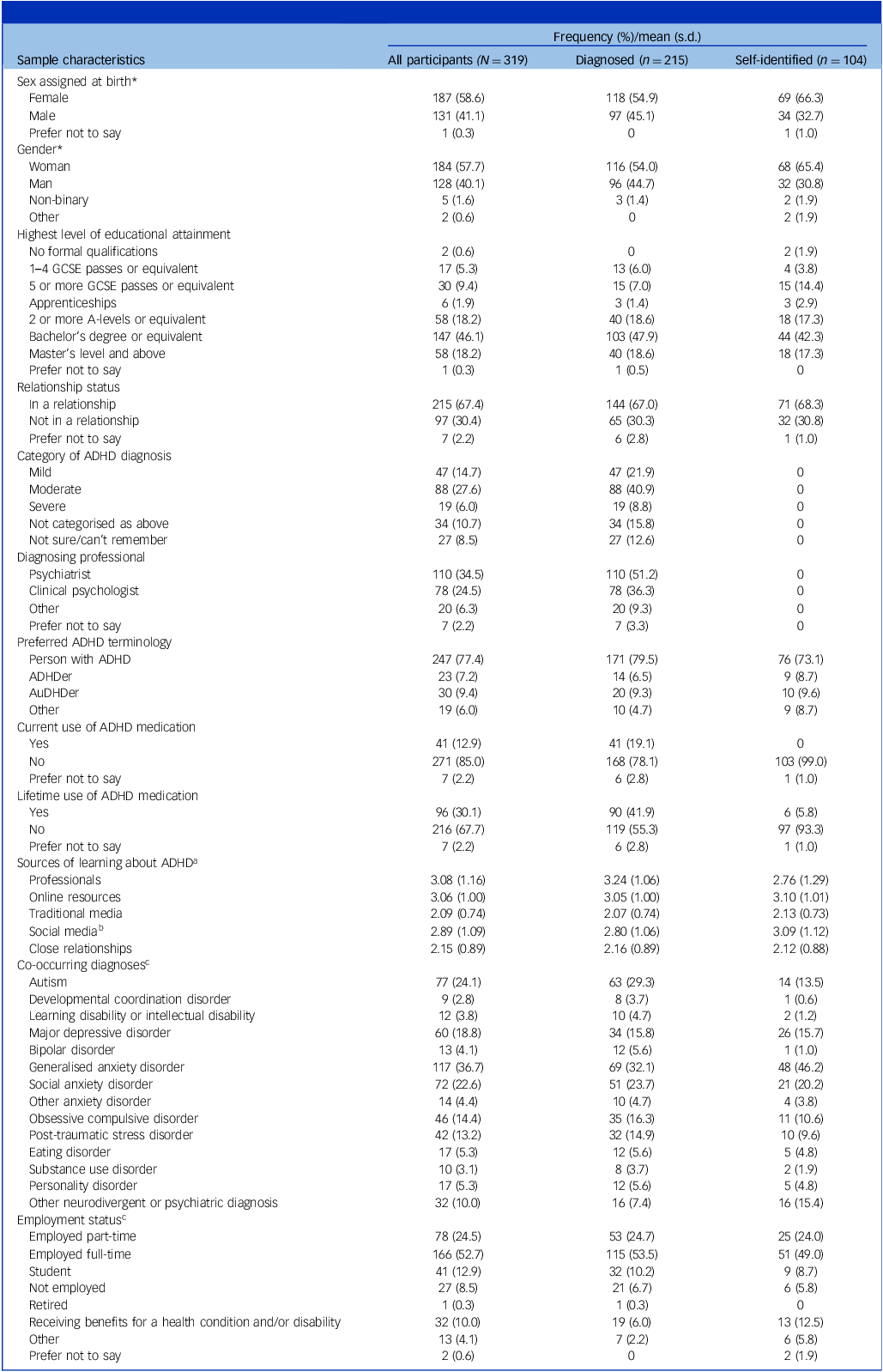
In the final sample, 215 participants had received an ADHD diagnosis and 104 participants self-identified as having ADHD. Participants who had an ADHD diagnosis received their diagnosis between the ages of 4 and 66 years (mean = 26.22, s.d. = 11.21) and were younger when they first identified as having ADHD (mean = 22.92, s.d. = 11.25, range 2–64 years) compared with those who self-identified as having ADHD (mean = 30.78, s.d. = 12.01, range 4–58 years). Further demographic information for the whole sample is presented in Table 1.
Sample characteristics for all participants and split by ADHD diagnosis status

GCSE, General Certificate of Secondary Education; ADHD, Attention-deficit hyperactivity disorder. AuDHDer is a community term describing individuals with ADHD and autism.
a. Ten sources were condensed down to five for analysis. The final categories and original sources were: professionals, online resources (online blogs and online research), traditional media (TV and movies, traditional media and books), social media (social media and influencers) and close relationships (parents and friends). Higher scores indicate greater influence of source on ADHD knowledge.
b. T-tests were performed to analyse differences between the diagnosed and self-identified groups on sources of learning about ADHD. Significant differences were found for the social media source of learning only.
c. Participants were able to select multiple response options so percentages may exceed 100%.
* χ2 tests revealed significant associations with ADHD diagnostic status. ‘Category of ADHD diagnosis’, ‘Diagnosing professional’, and ‘Current/Lifetime use of ADHD medication’ were not analysed due to small numbers of self-identified individuals who endorsed these variables. ‘Co-occurring diagnoses’ and ‘Employment status’ were not analysed as participants were able to select multiple responses.
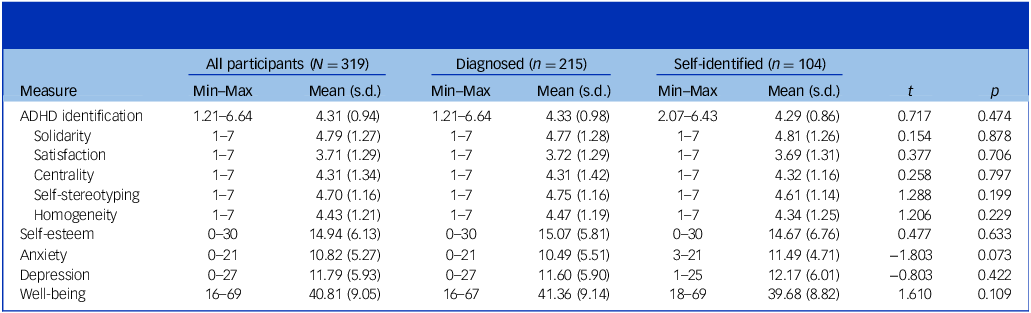
A t-test compared questionnaire scores between participants who reported a formal ADHD diagnosis (n = 215) and those who self-identified with ADHD (n = 104). This revealed no significant differences between the groups across all questionnaire measures (Table 2). χ2 tests investigated whether any demographic factors were associated with ADHD diagnostic status: sex and gender were the only factors with significant associations, with female sex and gender associated with higher rates of self-identification of ADHD.
Descriptive statistics for the questionnaires (N = 319), and by group (diagnosed ADHD versus self-identified ADHD), with t-tests for group differences on validated questionnaires

ADHD, attention-deficit hyperactivity disorder; Min, minimum; Max, maximum.
Split by diagnostic status: diagnosed: mean = 34.00, s.d. = 10.85, range = 18–73; self-identified: mean = 36.92, s.d. = 10.76, range = 18–68.
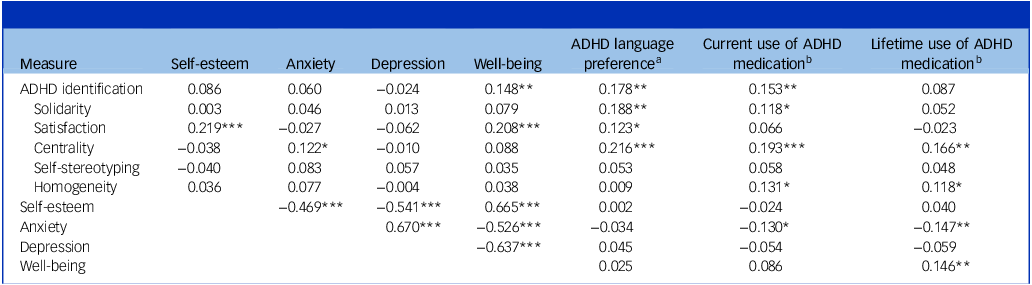
To test our hypothesis that higher ADHD social identification scores would be associated with higher self-esteem scores, which in turn would be related to higher well-being, and lower anxiety and depressive scores, we first conducted correlational analyses (Table 3).
Spearman’s rho correlations between questionnaire measures (N = 319)

ADHD, attention-deficit hyperactivity disorder.
a. 0 = person first, 1 = ADHD first.
b. 0 = no, 1 = yes. Pearson correlations are reported for correlations between ADHD identification (total score and subscales) and ADHD language preference and use of medication.
*p < 0.05, **p < 0.01, ***p < 0.001.
ADHD social identification total score was not significantly correlated with self-esteem, anxiety or depression. However, participants with higher ADHD social identification had significantly higher well-being scores, preference for ADHD-first language and current use of ADHD medication. Higher self-esteem was significantly correlated with higher well-being scores, and lower anxiety and depression scores.
When we examined individual subscales of the ADHD social identification measure, we found higher levels of ADHD satisfaction were significantly correlated with better self-esteem, well-being and preference for ADHD-first language. Additionally, participants who reported ADHD as being a more central identity had higher levels of anxiety, and a preference for ADHD-first language, as well as both current and lifetime use of ADHD medication. We found no meaningful differences when we excluded participants who self-identified as having ADHD, as well as when we excluded those who reported a co-occurring autism diagnosis (see Tables A and B in Supplementary Materials available at https://doi.org/10.1192/bjp.2026.10652).
Serial mediation models examined whether self-esteem and well-being mediate the paths between ADHD social identification and depression/anxiety (Fig. 1). Two separate serial mediation models had the dependent variables depression and anxiety, respectively. In both models, we found ADHD social identification did not have a significant association with self-esteem or well-being. However, higher levels of self-esteem were significantly associated with higher levels of well-being. Higher levels of depression and anxiety were significantly associated with lower self-esteem and well-being.
Serial mediation model displaying the associations between attention-deficit hyperactivity disorder (ADHD) social identification, self-esteem, well-being, depression and anxiety (N = 319). Hypothesised pathways are indicated by the solid line arrows. Dashed line arrows indicate non-hypothesised pathways, while dotted line arrows represent direct pathways.

When depression was the dependent variable, the direct association between ADHD social identification and depression was non-significant. The total effect (b = 0.03, t = 0.08, p = 0.93) and all indirect associations were not significant. For anxiety, the direct association between ADHD social identification and anxiety was significant, with higher identification linked with more anxiety when accounting for self-esteem and well-being. However, the total effect (b = 0.35, t = 1.12, p = 0.26) and all indirect associations were not significant. We found no meaningful differences when both serial mediation models were re-conducted excluding participants who self-identified as having ADHD (see Fig. A in Supplementary Materials).
The satisfaction subscale of the ADHD social identification measure was positively correlated with self-esteem and well-being, while none of the other identification subscales were. We therefore followed up the previous serial mediation models with an exploratory analysis focused on this variable, which was not preregistered. We replaced the ADHD social identification measure with the ADHD social identification satisfaction subscale, but all other variables remained the same (Fig. 2).
Exploratory serial mediation model displaying the associations between attention-deficit hyperactivity disorder (ADHD) social identification satisfaction, self-esteem, well-being, depression and anxiety (N = 319). Hypothesised pathways are indicated by the solid line arrows. Dashed line arrows indicate non-hypothesised pathways, while dotted line arrows represent direct pathways.

In both models, higher ADHD social identification satisfaction was significantly associated with higher self-esteem, but not well-being. However, higher self-esteem was significantly associated with higher well-being. Higher depression and anxiety were significantly associated with lower self-esteem and well-being.
When depression was the dependent variable, higher ADHD social identification satisfaction was associated with higher depression when accounting for self-esteem and well-being. The total effect (b = −0.32, t = −1.23, p = 0.22) was not significant; however, the indirect association from ADHD satisfaction to depression through self-esteem was significant (b = −0.25, 95% CI (−0.46, −0.08)), with higher ADHD satisfaction associated with lower depression. As was the indirect association from ADHD satisfaction to depression through self-esteem then well-being (b = −0.39, 95% CI (−0.62, −0.19)). For anxiety, the direct association between ADHD social identification satisfaction and anxiety was not significant. As we found with depression, the total effect (b = −0.18, t = −0.77, p = 0.44) was not significant. However, the indirect associations from ADHD satisfaction to anxiety through self-esteem (b = −0.22, 95% CI (−0.43, −0.06)) and from ADHD social identification satisfaction to anxiety through self-esteem then well-being (b = −0.27, 95% CI (−0.43, −0.12)) were significant, with higher ADHD satisfaction associated with lower anxiety. Overall, no meaningful differences were observed when we re-conducted the analyses excluding participants who self-identified as having ADHD. However, the direct association between ADHD social identification satisfaction and depression was no longer significant once these participants had been excluded (see Fig. B in Supplementary Materials).
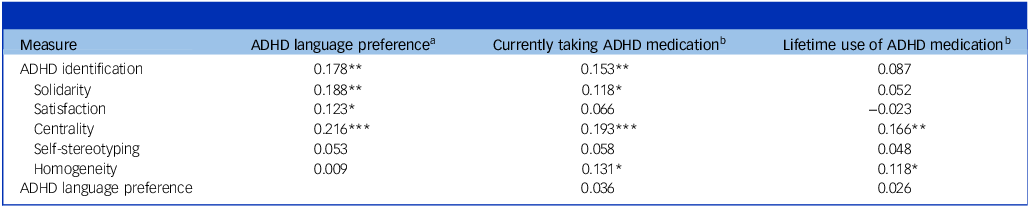
Exploratory analyses explored associations between ADHD social identification and ADHD language preference, ADHD medication and sources of learning about ADHD. As shown in Table 4, the majority of participants reported a preference for person-first language (i.e. ‘person with ADHD’) rather than ADHD-first language (i.e. ‘ADHDer’). This preference was seen in both those with an ADHD diagnosis and those who self-identified with ADHD. Most participants were not currently taking ADHD medication; and only participants with an ADHD diagnosis (and no self-identified participants) reported currently taking ADHD medication. We found nearly half of participants with an ADHD diagnosis had taken ADHD medication at some point in their lives, while a small number of participants who self-identified with ADHD reported lifetime use of ADHD medication.
Pearson’s correlations between ADHD social identification, language preferences and ADHD medication use (N = 319)

ADHD, attention-deficit hyperactivity disorder.
a. 0 = person first, 1 = ADHD first.
b. 0 = no, 1 = yes.
*p < 0.05, **p < 0.01, ***p < 0.001.
Exploratory correlational analyses revealed significant associations between higher levels of ADHD social identification and a preference for ADHD-first language (Table 4). This association with language preference was found for most of the ADHD social identification subscales apart from self-stereotyping and homogeneity. When exploring current and lifetime use of ADHD medication, we found higher levels of ADHD social identification for those currently taking ADHD medication. This association was particularly evident for the ADHD social identification centrality subscale. A weaker positive association was found between ADHD social identification and lifetime use of ADHD medication. Only ADHD social identification centrality and homogeneity subscales were significantly associated with taking ADHD medication during the lifetime.
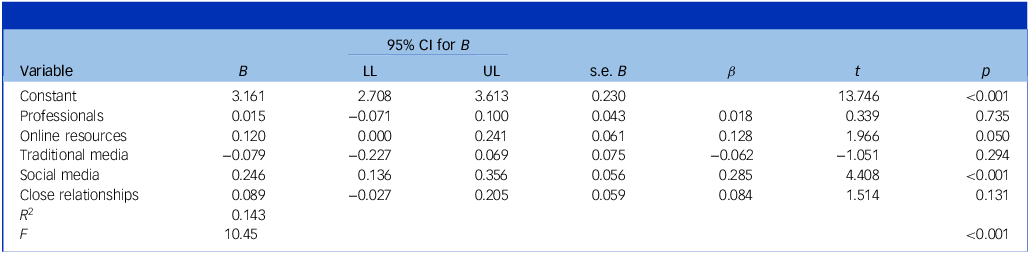
To explore associations between ADHD social identification and sources of learning about ADHD, we conducted a multiple linear regression (Table 5). When all five sources of learning were entered into the model as independent variables, we found the model to be significant (F (5, 312) = 10.45, p < 0.001, R 2 = 0.143). However, only greater use of social media was significantly associated with higher ADHD identification.
Multiple linear regression of sources of learning about ADHD a on ADHD social identification (N = 319)

ADHD, attention-deficit hyperactivity disorder; B, unstandardised regression coefficient; LL, lower limit; UL, upper limit; β, standardised coefficient; R 2, coefficient of determination.
a. Ten sources were condensed down to five for analysis. The final categories and original sources were: professionals, online resources (online blogs and online research), traditional media (television and movies, traditional media and books), social media (social media and influencers) and close relationships (parents and friends). Higher scores indicate greater influence of source on ADHD knowledge.
Discussion
In our cross-sectional UK sample of adults with ADHD, we did not find support for the hypothesis that ADHD social identification would be associated with lower anxiety and depression via self-esteem and well-being. Instead, ADHD identification and its satisfaction subscale were both associated with higher depression and anxiety when accounting for self-esteem and well-being, although their correlations with these mental health variables were non-significant. In exploratory analyses, we found that a subcomponent of ADHD social identification – satisfaction – was indirectly related to better mental health via self-esteem and well-being. Most participants preferred to be described as a ‘person with ADHD’, indicating that ADHD was not prioritised as a central identity in our sample. Those taking ADHD medication were more likely to have higher ADHD identification and prefer identity-first terminology (e.g. ‘ADHDer’). To examine whether there were differences between participants who were diagnosed with ADHD compared with those who self-identified as having ADHD, we conducted our analyses with and without those participants who self-identified as having ADHD. Overall, we found no meaningful differences.
In this study, ADHD identification correlated with higher well-being but not with anxiety, depression or self-esteem, while ADHD satisfaction (the affective subcomponent of social identification) correlated with higher well-being and self-esteem but not directly with anxiety or depression. While ADHD identification did not show the hypothesised associations with depression or anxiety, ADHD satisfaction was indirectly beneficial through self-esteem and well-being. For all models there was evidence of suppression effects: with direct paths to anxiety and depression either significant or approaching significance, indicating a negative impact of ADHD satisfaction on mental health. In contrast, indirect paths suggested a protective role, with higher identification linked to fewer mental health problems, a pattern significant only for ADHD satisfaction.
These findings suggest that interventions should focus on strengthening self-esteem and well-being, with ADHD satisfaction as a factor which could support better mental health via improved self-esteem and well-being. This further indicates that ADHD satisfaction may be a more promising intervention target than the broader construct of social identification, as feeling good about oneself likely relates to feeling good about belonging the group ‘people with ADHD’. In practice, this means that psychosocial interventions for adults should take a strengths-based approach and support self-acceptance in the face of ADHD-related challenges. A strengths-based approach further allows practitioners to harness the individual’s abilities to promote positive feelings and meaningful experiences, thereby supporting improved well-being. The findings align with meta-analytic evidence that identification with active or less stigmatised groups is more strongly related to lower depression and anxiety. Reference Tennant, Hiller, Fishwick, Platt, Joseph and Weich27,Reference Bury, Haschek, Wenzel, Spoor and Hedley28 Because ADHD is a stigmatised identity, Reference Bisset, Winter, Middeldorp, Coghill, Zendarski and Bellgrove16 opportunities for group identification may be limited. Where identification enhances self-esteem and well-being, however, it may still provide mental health benefits, helping explain the complex relationship between ADHD identification, satisfaction and depression or anxiety. Should ADHD stigma reduce in future, a replication of this study may produce a different pattern of findings.
These findings could indicate that ADHD identification does not confer the same benefits reported in autism Reference Davies, Cooper, Killick, Sam, Healy and Thompson20 or other social identities. Reference Jetten, Haslam and Alexander19 In one sample of autistic adults, autism identification correlated with lower depression and higher well-being but not anxiety, Reference Maitland, Rhodes, O’Hare and Stewart29 while in another sample of autistic 15–22-year-olds, autism satisfaction was associated with better well-being but not social anxiety. Reference Cooper, Russell, Lei and Smith30 However, caution is needed in making direct comparisons, as no autism studies to our knowledge have tested similar models including both self-esteem and well-being. It might also be that autism social identity is more established than ADHD social identity, leading to different impacts on well-being and mental health, but further research is needed before any comparisons can be made.
Participants with higher ADHD identification were more likely to be currently taking ADHD medication. Medication may increase the salience of ADHD, promoting identification. Significant associations between medication use and solidarity, centrality and in-group homogeneity support this. However, the small proportion of participants taking medication (n = 41 current; n = 96 lifetime) means these analyses may be underpowered. Qualitative findings suggest medication may also reduce an individual’s sense of expressing their ‘true’ self. Reference Redshaw and McCormack11 Our findings suggest ADHD identification may be reinforced by medication but since this is not linked to better mental health, distancing from ADHD identity (which could include a choice to not use medication) may be a helpful strategy some adopt.
Consistent with the limited benefits of ADHD social identification, most participants (77%) in the English-speaking, UK-based sample, preferred person-first terminology, suggesting ADHD is not viewed as integral to the self and that individuals prefer to foreground their personhood. This may represent an adaptive identity management strategy when ADHD identification does not reliably enhance self-esteem or protect against mental health problems. Participants with higher ADHD identification were more likely to prefer identity-first terminology, particularly on the solidarity, satisfaction and centrality subscales, which reflect self-investment. Reference Leach, van Zomeren, Zebel, Vliek, Pennekamp and Doosje23 For those invested in their ADHD identity and community, identity-first terminology may affirm ADHD as central to self. The only source of ADHD information that was significantly associated with ADHD identification satisfaction was social media and influencers; this could mean that ADHD satisfaction was linked to investment in being part of an online community.
Clinically, health professionals should note that most UK ADHD community members prefer person-first terminology, but individual preferences should always be honoured. ADHD identification did not appear to provide unilateral mental health benefits, and there is heterogeneity in how individuals interpret their ADHD identity. Some may benefit more from investing in other social identities linked to higher self-esteem, though ADHD identification satisfaction may provide benefits when it improves self-esteem. In post-diagnostic therapeutic work, exploring how an individual interprets their ADHD identity, and how it relates to self-esteem, well-being and mental health, may be critical, especially in group interventions where identification may not be uniformly beneficial. Attention should therefore be paid to ADHD strengths and how these relate more broadly to one’s self-esteem and well-being. Clinicians should also attend to how medication use interacts with identification: if it strengthens ADHD identity without improving self-esteem, this may not support mental health.
A strength and limitation of this study is the inclusion of both diagnosed and self-identified participants, producing a heterogeneous sample. While some may not meet diagnostic criteria, diagnostic practices vary widely and in this study, questionnaire scores were similar across groups, suggesting ADHD identification operates similarly irrespective of formal diagnosis. However, this methodological choice means the sample may include false positives and greater heterogeneity with respect to features of ADHD. Recruitment of participants via ADHD/neurodiversity-specific platforms may well yield different results, because participants would self-select based on their interest in ADHD, whereas on the online platform we found participants who earn money by taking part in a range of studies. Further, the use of online platforms comes with the risk of fraudulent responses, which could jeopardise data integrity and therefore the validity of the findings. To mitigate these risks, we conducted checks on the data including an attention check. Another strength was linking terminology preferences to ADHD identification, an issue discussed in autism but rarely studied in ADHD. However, our sample size limited power for these analyses, and larger international studies are needed. Indeed, findings are likely to vary depending on the language spoken and cultural context. The findings are based on a UK sample and cross-sectional data, and are therefore tentative, with much more research required to understand identity processes and terminology preferences. Reference French, Dekkers, Barclay, Black, Bölte and Daley31
In sum, our findings did not support the hypothesised relationship between overall ADHD social identification, self-esteem, well-being and mental health outcomes. However, a subcomponent of identification (satisfaction), was positively associated with mental health. Further, participants preferred terminology that de-emphasised ADHD identity (‘person with ADHD’). Given our cross-sectional design, future longitudinal research should clarify the role of ADHD identification (and satisfaction) in self-esteem, well-being and mental health, and examine identity processes among individuals with multiple neurodivergent diagnoses. Longitudinal studies should further investigate whether these processes impact on well-being and then protect against mental health difficulties developing later. Reference Keyes, Dhingra and Simoes32 Further, it remains to be tested whether ADHD identification predicts medication use, or medication use increases identification. Further qualitative and survey research is needed to test whether these findings generalise beyond the UK and to unpack underlying mechanisms contributing to self-esteem and well-being in this population.
Supplementary material
The supplementary material is available online at https://doi.org/10.1192/bjp.2026.10652
Data availability
The data and materials that support the findings of this study are available from the corresponding author (K.C.) upon reasonable request. Data analytic code is not available.
Acknowledgement
Thank you to the adults with ADHD who contributed to this research.
Author contributions
K.C. acquired funding. K.C., K.T., A.B. and L.G.E.S. conceptualised the study and reviewed and edited the draft of the manuscript. K.C. and K.T. collected the data. K.T. conducted the quantitative analysis and prepared all tables and figures.
Funding
This study was funded by Avon and Wiltshire Mental Health Partnership National Health Service Trust Research Capability Funding. K.T. is funded by a Health and Care Research Wales Advanced Fellowship award (2024–2027).
Declaration of interest
None.
Ethical standards
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2013. All procedures involving human participants were approved by Life and Medical Sciences REC, ID 0116 (redacted).





 Open access
Open access
eLetters
No eLetters have been published for this article.