

Imagine being a nurse who needs to speak to the relative of a patient. The relative has just arrived at the unit and seeks information about a family member who is currently in the operating theatre. The hospital staff could communicate with the patient without any problems, but the relative does not speak the local language and is finding it difficult to understand the nurse. Failing to understand when the patient can receive visitors could cause anxiety and unnecessary concern but would be unlikely to have significant health consequences for the relative, much less for the patient. Perhaps the relative in that case would need to wait to speak to the patient directly. The wait might be unpleasant for the relative, and the inability to help is likely to be frustrating for the nurse, so the nurse decides to use Google Translate to explain the visiting times on the ward.
A nurse in this scenario could in principle try to get help from a human interpreter. But since the individual who needs assistance is not a patient, budget holders at the hospital would probably see the use of an interpreter as a waste of resources. The nurse could also have pointed at a timetable of visiting times or handed out a pre-translated leaflet. Pre-translated materials may be unavailable, however, and in any case just pointing at written information is probably not as personal as the type of assistance that the nurse would provide to other next of kin who speak the local language. Given the non-clinical nature of the interaction, the nurse may see no reason why machine translation should not be used.
This chapter is about contexts of this nature where the risks of using machine translation are ostensibly low. The data that underpins the chapter was collected in a 2024 survey of 2,520 UK professionals. The survey included a nurse who described a scenario like the one above. This same survey provides the data for Chapter 4 and Chapter 5. Only those who worked in healthcare, social assistance, emergency services, legal services and the police were eligible to take the survey. Approximately eighty per cent of the sample worked in either healthcare or social assistance. Although response rates for each sector were not controlled to match national statistics, the NHS is the UK’s biggest employer,1 so the prominence of healthcare workers in the sample is likely to reflect national workforce distributions.
Of the 2,520 professionals who submitted a valid response, 828 had used machine translation at work. In this chapter – and in Chapter 4 – I focus on these professionals’ descriptions of how machine translation had been used. On occasion I draw on other aspects of their submissions, such as responses to a question that asked what advice they would give to colleagues who were considering using a machine translation tool.
I analysed the data inductively. My goal was to examine uses of machine translation that are qualitatively relevant for how this technology is socially conceptualised. The sections below present insights that emerged from this analysis. Where responses were particularly rare or particularly frequent, I indicate this in the text. I do not, however, seek to quantify any patterns. Similarly, my intention is not to provide a breakdown of popular machine translation tools. Details of this nature are inevitably time-constrained, which also applies to the number of machine translation users reported above, a figure that is likely to grow considerably in coming years. My objective is instead to examine the social, communicative and professional factors that characterise uses of machine translation in the service contexts selected for analysis. Full notes on the data collection methodology are available in Notes on Methodology together with a summary description of the survey sample. A quantitative snapshot of the data is available in a report published by the Chartered Institute of Linguists in 2024.2 In what follows, when reproducing any accounts verbatim, I provide participants’ responses between quotation marks together with their self-described professional role. I quote the professional’s broader industry sector where a professional role is unavailable or where the one provided is unspecific. I adopt this same data reporting format in Chapter 4 and Chapter 5.
* * *
In February 2023, a London girl died after sipping a hot chocolate which her mother had bought for her at a café. The girl had a dairy allergy. When placing the order, the mother mentioned her daughter’s allergy and asked for the hot chocolate to be made with soy milk. Tragically, this crucial piece of information was missed in the ordering process.3 When the girl’s death was investigated at an inquest, the barista who served the girl’s mother gave evidence through an interpreter. The barista was a speaker of Bengali, and the girl’s mother had placed the order in English. Following the inquest, it was concluded that miscommunication was one of the factors that had led to the girl’s death.
The barista had not used machine translation when the order was placed, but it later transpired that baristas at the same café chain had a habit of using Google Translate to complete online allergy training modules. When asked if the use of machine translation was a cause for concern, a regional manager in charge of operations at the chain replied: ‘To my understanding, Google Translate is used as a dictionary as well. It’s not concerning for me … To my understanding, it’s not that they don’t know English – it’s that they don’t understand a certain word.’4
If Google Translate allowed the baristas to understand words from the training that they would otherwise have been unable to understand, it could be argued that brief uses of machine translation of this nature can provide access to critical information. The assumption that brief or occasional uses of machine translation carry less risk was also reported by participants of my survey. Plausible though it is, this assumption is not straightforward. Besides the possibility that even brief uses of this technology can be consequential, just the fact that the technology is in use is a sign that the user is experiencing some type of language or communication need that may merit attention. Ad hoc machine assistance can be helpful, but it can also conceal the nature of language barriers experienced at an organisation. In the case involving this coffee chain, Google Translate allowed the baristas to pass allergy training modules while the real extent of communication difficulties experienced by staff went unnoticed until a tragedy happened.
Uses of machine translation that may be perceived as low risk should therefore be approached with caution. My intention in this chapter is not to declare any uses of machine translation as reliably safe, not least because, as previously discussed, human-mediated communication cannot be declared entirely safe either. Rather, many of the machine translation use purposes reported by the project participants occupied a middle ground where the immediate risks were ostensibly low, but where systemic root causes for the use of the technology may raise alarm bells. Some of these use purposes were only indirectly related to the core service being provided. Others were closer to the core service itself. These purposes tended to involve synchronous, bidirectional communication that took place in a shared physical space. I examine three such use purposes in the sections below.
Between Ancillary Communication and Core Care
I call ‘ancillary communication’ those communicative tasks that either complement or surround a service without forming part of the core service itself. In healthcare settings, these will be exchanges that do not directly concern someone’s health. The scenario reported at the beginning of this chapter where a nurse had to answer a family member’s query about the unit’s visiting times would be an example of this type of interaction. Giving directions so that someone can find their way around a hospital would be another, as would booking appointments or responding to patient complaints that are unrelated to a health issue.
A lot of what I call ancillary communication concerns aspects of customer service. Customer service was indeed the phrase used by some project participants when describing why they had used machine translation: ‘To assist with customer service enquiries’ (Admin, Medical/Healthcare). But customer service can cover a wide range of activities, including aspects of the service that arguably cannot be considered ancillary or peripheral – for example, how attentive doctors are or how promptly patients are seen. Ancillary communication can also easily turn into a core service, as I will discuss later, but it will often concern exchanges that would not usually be expected to pose significant risks.
The low-risk nature of these exchanges was sometimes emphasised by the professionals in their explanations of when and why they had used machine translation tools. For example, a ward sister (a nurse who oversees a ward in a hospital) explains that machine translation is only used for simple questions and that professional language services are used for more complex communication: ‘Occasionally we have patients that don’t speak English and use [their] phone to ask questions to us, simple questions usually like what time is lunch etc. We have Language Line [a provider of professional language services] for more complex conversations.’
Another example, also mentioned by a nurse, involved a patient who wanted to leave the premises: ‘The patient was asking to go to the shop and buy some food.’
In these two examples, the communication was initiated by the service users. But often the professionals themselves decided to use machine translation when they judged it to involve low levels of risk. A physiotherapy manager explains that machine translation is used for ‘rescheduling appointments if interpreters don’t show up’. This same manager adds, ‘It’s not suitable for complex medical assessment. But it’s good for administrative stuff like rescheduling.’ Similarly, a social services worker used it ‘to arrange visits’. When asked what advice they would give to colleagues who were thinking of using machine translation, this same social services worker said, ‘To use [it] carefully, not [to] use for official work.’
Some professionals are therefore attuned to the risks of machine translation. For these professionals, ancillary communication often represents the types of tasks where machine translation use is acceptable. It is also clear how the impromptu and ephemeral nature of some of these tasks might leave the professionals with few alternatives. When a patient has a query about mealtimes or about leaving the hospital for a short period, it goes without saying that the query is unplanned. It may be difficult to predict when these communication needs will arise, and they are likely to arise often.
The routine or even uneventful nature of these interactions notwithstanding, some of them are crucial for making service users feel supported. The service provided may be particularly valuable because of the attention paid to everyday needs that are not necessarily part of the professional’s core remit. The importance of these ancillary communication events is vividly demonstrated by the account of a public health lead:
As part of a project I was working on with community midwives, I needed to communicate with pregnant women and their families in Polish and Urdu in order to give them some basic information (i.e., what time their taxi was coming, where they needed to be for their next appointment, what time it was and so on). This was because they were migrant families who hadn’t been given any NHS support during the pregnancy to that point, so we were piecing things together for them.
Machine translation is used by this public health lead for something as simple as telling the time. Not unlike previous research on everyday uses of machine translation tools,5 in some of these examples machine translation is used for purposes that would be unlikely to be fulfilled by language professionals. Yet, despite the simplicity of this type of communication, the overall service provided is likely to be more personal if service providers and users can have informal interactions of this nature. Public service professionals may argue that this type of interaction is a key component of the service they provide. A 2022 study conducted in California found that poor communication between front-desk staff and low-English-proficiency individuals required clinicians to perform extra tasks to provide appropriate care.6 In other words, language barriers experienced anywhere in the service are likely to affect the service overall. In a context like the one described involving pregnant women who needed to navigate a new country and new health system, I would argue that the interaction described by the public health lead is essential even if it does not concern their core area of professional activity.
In March 2024, I was at a Bristol healthcare practice waiting to be seen by my primary care doctor. I spent about thirty minutes in the waiting room and did not have a book or my headphones to distract me. I did not witness any uses of machine translation, but I was struck by the range of tasks fulfilled by the receptionists who were on duty. Some patients had the usual queries that most healthcare receptionists can help with, including rescheduling or booking appointments and tests. But I also saw patients come in with queries that put the receptionists in a difficult position. Obtaining test results directly from a clinician at my primary care practice can be a challenge. Booking an appointment just to discuss the results can involve a long wait. Especially if the results are normal, waiting may be unnecessary, so the job of communicating test results to patients usually falls to the practice’s receptionists and admin staff. Just in the thirty minutes I was in the waiting room, I overheard a patient learn that they were diabetic and another one that they were pre-diabetic. The receptionists spoke behind a Perspex screen installed during the Covid-19 pandemic. Sometimes they would raise their voice or try to speak through the rectangular cut-out used for the exchange of documents. Details of the patients’ test results were revealed to the entire waiting room. The patients had follow-up questions, but other than quoting the results and any doctor notes, the receptionists were unable to help. They did, however, do their best to reassure the patients. During those interactions, they fulfilled more than an administrative role.
I was writing this book at the time, so all that I could think about was how someone with low English proficiency would access test results at my primary care practice. There were barriers in place that made it difficult for any patient to access their results and speak to a doctor about them. The experience of those who faced a language barrier in addition to these difficulties was unlikely to be positive. I did not seek contributions from anyone working at my doctor’s practice for this project, but several accounts submitted by the project participants illustrate how ancillary communication can easily become a component of core care where the risks posed by machine translation can be significant.
Some of the accounts submitted by the participating professionals referred to mixed scenarios. A care coordinator at a healthcare setting described using machine translation when ‘confirming appointment dates and times’, and in the same sentence added, ‘[and] understanding medical complaint’. Similarly, an assistant healthcare practice manager used machine translation when ‘trying to register patients’ as well as when ‘trying to communicate to patients about their healthcare needs’. These scenarios show that what may start as an admin task can proceed to questions and assessments that have an impact on the individual’s health. Assistants, receptionists and coordinators are often a first point of contact. Workers in these roles will usually perform ancillary communicative tasks, but the responsibility for identifying care needs may also fall to them. Their qualifications are likely to cover best practices for communicating across language barriers,7 but as I will discuss in Chapter 5, machine translation literacy is unlikely to be part of their workplace training.8
Differentiating ancillary communication and core service provision is therefore not easy. Ancillary communication is a prototypical context in which machine translation is used, and one where its use may involve low levels of risk. Interpreters are also unlikely to be used in these contexts. Even phone interpreting can involve long waits (see Chapter 6), so if patients just wish to know the time or when a meal will be served, using professional interpreters may seem cumbersome or excessive, especially if these brief interactions occur repeatedly throughout the day. Machine translation here may offer timely and often effective assistance, but risk-benefit ratios change fast. Administrative staff may confirm appointment details one moment and carry out a needs assessment the next. Communicative purposes bleed into each other, so drawing clear-cut lines between what is safe and what is not is difficult. Professional roles are not a reliable indicator of risk either. Ancillary communication will often be interspersed with core care and all those who handle information about service users, including clerical and admin staff, will have a great responsibility on their hands.
Combining Language Professionals and Machines
Seeking assistance from a translator or interpreter was often never intended in the contexts discussed in the previous section. This is because the communication was usually judged to be of low risk or too brief or ad hoc to justify the involvement of a linguist. Another type of machine translation use reported by the participants involved situations where language professionals were intended to be involved in some way. Interactions of this nature can be of at least two kinds. The first is where human professionals are expected to assist, but for some reason they are not available or cannot be found. I discuss contexts of this nature in Chapter 4. The second type of context is where both machine translation and linguists are used, often at different points in the process of providing the service. This section is about this second type of context.
Imagine having an emergency in a foreign country. You need to call the country’s emergency phone number, but you do not speak the local language or any language that you could use to communicate. You decide to use your native language in the hope that the call handlers will find a way of communicating with you. In the UK and many other countries, interpreting services are integrated into the working processes of emergency call centres. The call centre will usually have partnered with a company that provides access to a large online pool of interpreters who can be summoned on demand.
Although this process is supposed to work well, finding an interpreter can take time. Guidance about the emergency services available in Wales tries to warn service users that they may need to wait: ‘The interpreters at Language Line [the language services provider] could be anywhere in the world, so it might take time to find someone who speaks your language.’9 The guidance adds, ‘The line will go quiet when the ambulance service is arranging an interpreter.’10 Callers who need language assistance therefore have a different experience to callers who do not. Although language inequalities are easily dismissed as a fact of life, emergencies are particularly effective at bringing home what these inequalities mean in practice. Waiting longer on the line can be life-threatening, and the less widely spoken – and less politically and economically prestigious (see Chapter 6) – the language, the smaller the interpreter pool is likely to be and the harder it will be to find an available interpreter.
Machine translation in these cases may help to reassure the caller while they wait, as described by one of the project participants who used it when ‘having a non-English speaker making a 999 call to us and having to try to communicate with them even enough to let them know we were going to try and connect to a three-way interpreter service’ (Call Handling Supervisor). It is not clear how exactly this call handling supervisor used machine translation on the call. They may have tried to pronounce the translations, or they may have used the speech-to-text and text-to-speech features of the tool. It is always possible for machine translation itself to cause confusion, especially if the caller’s language is not well known to the translation model or if the caller’s accent is poorly recognised. But if the machine translations are reasonably accurate and understandable, they are likely to be more reassuring than the silence which callers in Wales are told to expect.
Some emergency call handling software can be integrated with AI translation tools that are used to automatically identify the caller’s language and to communicate with them.11 The extent to which call handlers rely on this technology will naturally vary, but it is noteworthy that some providers of this type of product do not promote it as a communication method to be used alongside language professionals. The proposed use of the tool may be more ambiguous. The National Telecommunications and Information Administration unit of the United States Department of Commerce says that ‘In a diverse community served by a 9-1-1 center, AI translation and transcription can instantly translate emergency calls into multiple languages, ensuring that all residents receive the help they need promptly.’12 On the one hand, this statement may simply reflect an attempt by the Department of Commerce to promote the inclusivity potential of their new technology. On the other, the claim that ‘all residents in a diverse community’ can receive the help that they need is at best tenuous. Not all languages are supported by AI translation models. Even languages which are supported are not guaranteed to be translated to a high level of accuracy. While human interpreters might not be available to assist all emergency callers either, what is in principle a complementary tool can easily become the default communication method.
In the same way that it can be difficult to draw a neat line between ancillary services and core care, combinations of language professionals and AI tools are not clear-cut. They will be influenced by varying levels of risk awareness and by the organisational factors described in Chapter 1. In contexts marked by funding pressures – and by potentially low levels of AI literacy – combining uses of humans and machines may be the first step towards attempts to eliminate human mediators altogether even when this is unadvisable.
These long-term possibilities are important to keep in sight, although many of the project’s participating professionals saw machine translation tools as essentially complementary. Some of them stressed that machine translation was no more than a tool used, for instance, for ‘very basic translation [of] simple phrases, whilst waiting for an appropriate translator’ (Nurse). It was also used to greet service users and to understand the basics of a situation before seeking professional assistance: ‘helping greet patients before official translators arrived or informing them of what was occurring for their appointment’ (Senior Ophthalmic Technician); ‘[I use it] when I need to gather some basic information to understand what has happened before I get a translator. Also sometimes to just get basic details like name and address’ (Police Officer).
Additionally, machine translation was used as a way of preparing for interactions that were going to be mediated by professional interpreters: ‘There have been occasions [where] I have used these tools to help me prepare for sessions with a physical interpreter (e.g., to get a feel for the wording used within session materials/measures)’ (Trainee Clinical Psychologist). Here machine translation is not a front-line tool but rather a preparatory aid that can help the non-linguist service provider to become familiarised with key vocabulary. While it is the interpreter’s job to be familiar with subject-specific vocabulary in a different language, machine translation may give more agency to non-linguist professionals by allowing them to participate more actively in the interaction. Even in preparatory tasks translation errors could be misleading, but the linguist will ultimately be available to broker understanding, so the complementary value of machine translation here is clear.
Unlike cases where machine translation is used before the involvement of linguists, a consultant paediatrician described a recurrent event where it was only after a professional interpreter had left a call that the need for further assistance tended to arise:
Parents will come to me – after we have completed a consultation using a telephone interpreter – to ask additional follow up questions, or clarify things said earlier. This is exclusively done by parents who have some knowledge of English and are able to understand my simple response (usually yes, no, or a number) but don’t know sufficient English to ask the question without Google Translate.
Very few options are available to this paediatrician. Language support may have been booked in advance, and getting an interpreter back on the line at short notice will in any event involve a wait. The paediatrician is likely to work under significant time pressure.13 Waiting could impinge on the time available for other patients. Allowing the parent to leave the consultation with unanswered questions is not an option either since it would incur health risks for the child. The judgement call to be made here is fraught with difficulties. Especially when parents have some knowledge of English, it is easy to see how the paediatrician would have come to accept the use of machine translation in these cases, even if they would not necessarily endorse the use of the technology more widely. When asked what advice they would give to colleagues who were thinking of using machine translation, this same paediatrician said, ‘Avoid wherever possible as there’s no record of the interaction – but equally, it’s hard to justify the 5 min process of getting a telephone interpreter on the line just for one simple yes/no question!’
While in most contexts discussed in this section machine translation was not used to replace the work of language professionals, its potential to complement professional language assistance varies significantly. Uses of the technology that take place before language professionals get involved are likely to be less risky if machine translation is used either in preparing for professionally interpreted interactions or in interim communication aimed at reassuring service users that language professionals are on the way. When used transiently in this way, machine translation may literally replace a silent wait. When the need for language support arises after a language professional has left the interaction, the risks are likely to be harder to navigate because whatever is communicated through the technology in these cases might not get the chance of being corrected or confirmed by a professional linguist. Moreover, there is always a chance that limited or complementary uses of machine translation tools can give way to wider and riskier uses of the technology – for example, if machine translation is rolled out as the main method of holding multilingual emergency calls or, as discussed in Chapter 1, where it is a government-recommended method for completing immigration forms or used by default to speak to visitors at border crossings.
Multimodality and Performative Interactions
In certain interactions, the understanding of a message will be largely apparent based on actions performed by the other interlocutor. A physiotherapist who completed the project survey used machine translation in tasks that ‘involved giving a patient exercises and respiratory care, so translations of things such as “take a deep breath” or “cough” or “lift your leg” etc.’ If machine translation works well in these cases, the patient will take a deep breath, cough or lift their leg as instructed, and the professional will be immediately reassured that the instructions are being followed. This type of communication highlights the important role of multimodality in machine translation use. As mentioned in Chapter 1, multimodality involves a combination of communicative modes – for example, spoken language as well as gestures and other signals individuals are able to send using their bodies.
The value of non-verbal communication – that is, bodily communication that does not happen through verbal language – has been discussed in several different fields. In the literature on public or customer service, discussions of this nature are usually focused on practical aspects of how to establish rapport with the service user, a type of knowledge that usually goes under the heading of cultural competence. Discussions of cultural competence often refer to the culturally coded nature of gestures and other types of body language. The thumbs-up sign, for instance, is considered vulgar in some cultures.14 Physical touch, eye contact and certain types of hand gestures are all examples of non-verbal signals that may be viewed positively by some cultures and reprehended by others.15 It is important for service providers to be aware of these cultural differences whether machine translation is used or not. But machine translation users are likely to rely even more on these bodily cues given the inherent uncertainty of using a technology that they cannot themselves verify. In other words, users may not know whether the machine translations are correct, so body language is likely to be a welcome complement. In the context reported by the physiotherapist above, it is possible to complement machine translation use by physically guiding the type of movement that the patient needs to perform.
Researchers have listed several functions of non-verbal communication. These functions include complementing, accenting, repeating or replacing the verbal message as well as indicating other aspects of the interaction such as whose turn it is to speak.16 In the translation and interpreting literature, it has been suggested that ‘voluntary non-verbal elements very frequently prove superfluous in practice when compared with the verbal utterance itself … or with the speaker’s prosody (specific intonation for indexical [i.e., context-dependent] words)’.17 This assertion concerns contexts where a verbal message – ‘the verbal utterance itself’ – is used alongside body language. When interactions are mediated by machine translation, any verbal utterances will be less reliable. The original, source-language utterances in these cases are likely to be partially or entirely inaccessible given the language barrier. The translated versions of the utterances are in turn less reliable because they are not directly produced by the utterer, which to some extent applies to messages delivered by human interpreters as well. The language barrier can therefore assign greater significance to multimodality, especially if the interaction is naturally physically performative with requests for the individuals to move or behave in a specific way. For this type of machine translation use, or indeed for any communicative use of machine translation that takes place in a shared physical space, I would argue that voluntary non-verbal elements are anything but superfluous.
Non-verbal communication has received somewhat disparate treatments across fields. It has been covered across psychology, anthropology, linguistics and communication as well as translation and interpreting. In interpreting studies, the value of non-verbal communication in particularly emphasised in multimodal analyses of interpreter-mediated interactions. This type of analysis has questioned the simplicity of the verbal/non-verbal dichotomy.18 It instead seeks to examine the totality of how communication takes place by considering the role of multiple layers of signs used in an interaction. Some of these signs involve individuals’ relationship with their environment. For example, in an analysis of an interpreter-mediated meeting between two teachers and a parent, participants in the communication slid the physical copy of a report across a table to indicate the focus of the conversation and to signal to the interpreter when it was their turn to speak.19 The ways in which the physicality of the environment, and of the participants within it, shaped communication in this interaction has been referred to as an ‘ecology of action’.20 This concept resonates with the framing of human–technology relations presented in Chapter 2. Like digital technologies, physical objects too fit specific purposes. Their shape and design may invite specific human actions, and humans’ use of the objects may also give off signals and play a role in communication.
Relations between humans and machine translation devices too have this type of communicative value. Showing a smartphone screen to someone by turning it in the opposite direction invites the other person to look at the screen. It also indicates the intention to use the technology to communicate. Moreover, the use of written information displayed on a screen may complement spoken language, especially in contexts where individuals may be able to rely on limited levels of language proficiency: ‘If the individual knew a small amount of English sometimes translating the odd sentence or word and showing them made it easier to understand what I was saying’ (Mental Health Recovery Worker); ‘Sometimes having face-to-face conversations with people who had limited English and showing them text on a screen was helpful’ (Triage Worker – Youth Homelessness). Here the text acts as a materialisation of messages that may be more likely to be misunderstood if provided just in spoken form. Understanding therefore comes about through a complex combination of modes including overlaps of written and spoken language as well as individuals’ relations with the objects around them.
The object can be anything that is relevant to the interaction. A cardiac physiologist describes how Google Translate was used to explain to patients how they were supposed to wear a heart monitoring device:
When translators weren’t available or booked and patients arrived, I would use Google Translate to give them instructions regarding a 24-hour heart monitor they were required to wear. This involved explaining what the monitor was for, how to wear it and details on how to return [it]. I always asked the patient if they understood, and allowed them to ask any questions via Google Translate too.
While this cardiac physiologist does not mention how the heart monitor itself is used in these interactions, it would be unusual for the interactions not to involve the monitor in some way. Just the act of handing over any type of object to the patient will indicate that the patient may need to do something with it. Here the interaction is likely to involve fitting the monitor as well as providing instructions regarding what to do with it later.
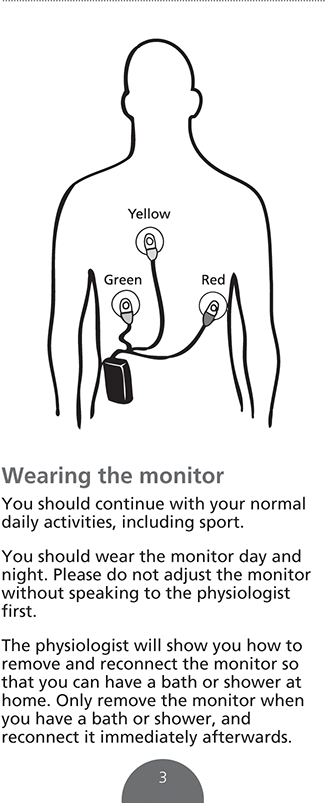
Images can also be useful in these cases. Figure 3.1 shows the third page of an information leaflet provided to cardiac patients at the Guy’s and St Thomas’ NHS Foundation Trust in London.21 Even if translations of the leaflet are not provided, just the illustration displayed on the leaflet will indicate that the electrodes connected to the monitoring device are supposed to be attached to the chest. The heart monitor itself will hold clues about how it is supposed to be worn. The back of the device is likely to have a clip, which will suggest that it is supposed to be clipped into a garment or around the waist. A healthcare provider may also point to the device and use their hands to demonstrate on their own body, or on the patient’s, how to clip the device and attach the electrodes. Machine translation, illustrations, objects from the environment, and the complex, multimodal nature of this interaction can be exploited in compensatory ways where what is missed by one signal might be understood through another.
Extract from a patient information leaflet prepared by the Guy’s and St Thomas’ NHS Foundation Trust.
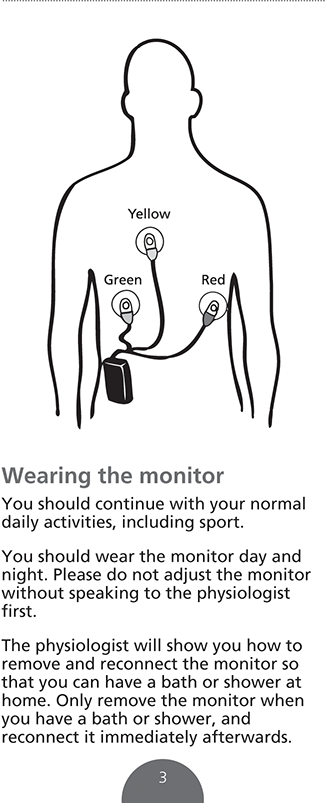
Figure 3.1 Long description
The device is attached to the waist and has three electrodes attached to the chest. The electrodes are in three colours: green, yellow and red. The written instructions read as follows: Wearing the monitor. You should continue with your normal daily activities, including sport. You should wear the monitor day and night. Please do not adjust the monitor without speaking to the physiologist first. The physiologist will show you how to remove and reconnect the monitor so that you can have a bath or shower at home. Only remove the monitor when you have a bath or shower, and reconnect it immediately afterwards.
Body language alone is unlikely to be enough when trying to explain to the patient details of their condition or why they are being asked to perform specific actions. Actions can also be misleading. When the patient does as instructed, the action may imply that they understood the instruction when in fact the patient may just be following along without knowing what they are doing or why they are doing it. Over-reliance on non-verbal communication therefore has the potential to erode service user autonomy, an issue I revisit in Chapter 4 when discussing service user consent. In any case combining communication methods will often be a good idea and may be particularly valuable in interactions where interlocutors need to do something.
Using multiple signals is an intuitive communication strategy that is already widely implemented. When asked about whether machine translation had been used together with other communication methods, most of the project participants said ‘yes’.22 They were provided with multiple-choice options to indicate what other methods they had used. Most of them had relied on other individuals or on Googling/web searching alongside the use of machine translation.23 A speech and language therapy professional who provided their own answer to this question explained: ‘The parents spoke some English and I used gestures, modelling my behaviour, examples and sometimes diagrams.’ Others who chose to type their own answers mentioned ‘body language’, ‘non-verbal’ or, in one case, ‘using objects around me to help’. Objects and our own bodies have communicative value. When using machine translation, it is sensible to draw on all elements of this ecosystem.
* * *
In many examples discussed in this chapter, language professionals would most likely never have been involved. So how would language barriers be dealt with in these scenarios if machine translation did not exist? Many of the communication methods that can be mentioned in response to this question are still in use. These methods are often employed alongside machine translation, and many of them go to the heart of how meaning is conveyed in human communication, such as the use of body language and the physical environment. Machine translation does not necessarily replace other communication methods. It is rather one other method individuals have at their disposal. It is, nonetheless, a powerful additional method. Its use may be transformative in the contexts discussed above, whether it be in making someone feel included, in reassuring them while they wait for an interpreter, or in coming to an appointment more prepared. But in the same way that machine translation helps in these cases, it can introduce risks that were not previously there. Furthermore, these use contexts are not static. What starts as a low-risk interaction can easily become a high-stakes one. Similarly, professional roles are not homogeneous. In the settings discussed in this book, receptionists, secretaries, assistants and other administrative staff all undertake tasks that are often central to the service being provided. Sometimes these tasks are part of the core service, such as explaining test results to patients or assessing their needs before they are seen by a clinician. These tasks come with great responsibility, even if this responsibility does not, arguably, get the public recognition it deserves.

 Open access
Open access