


Impact statement
Violence in intimate relationships is more prevalent in communities affected by war and armed conflict. While this association is well documented, the mechanisms underlying it are less well understood. This review synthesises evidence on the individual, relational and structural drivers linking armed conflict to intimate partner violence (IPV). Key drivers include conflict-related trauma and PTSD, alcohol use, economic stress and insecurity and shifts in gender roles and norms, with evidence highlighting the intersection of gender and economic factors as a particularly significant dynamic. By identifying empirically supported drivers across multiple levels, this review provides evidence to inform prevention and response efforts in conflict-affected settings. The findings highlight the importance of integrating gender-transformative approaches and IPV prevention into humanitarian and post-conflict programming. However, the evidence base is disproportionately drawn from military samples in high-income countries, with comparatively limited research from low- and middle-income settings. Expanding research across diverse geographic and socio-political contexts is essential to developing a more comprehensive and globally relevant understanding of conflict-related IPV.
Introduction
IPV encompasses physical, sexual or psychological violence that takes place between current or former intimate partners (WHO, 2024). This form of violence disproportionately affects women and presents a major threat to health and human rights worldwide. Several studies have documented the association between exposure to armed conflict and higher rates of IPV (e.g., Kelly et al., Reference Kelly, Colantuoni, Robinson and Decker2018; Spangaro et al., Reference Spangaro, Toole-Anstey, MacPhail, Rambaldini-Gooding, Keevers and Garcia-Moreno2021; Bandara et al., Reference Bandara, Knipe, Munasinghe, Rajapakse and Page2022; Le and Nguyen, Reference Le and Nguyen2022). In their study of the intersections between armed conflict and IPV in Liberia, Kelly et al. (Reference Kelly, Colantuoni, Robinson and Decker2018) identified a 50% increased risk of IPV associated with living in conflict-affected districts. This finding was replicated in a study in Sri Lanka (Bandara et al., Reference Bandara, Knipe, Munasinghe, Rajapakse and Page2022), which found that women residing in conflict-affected areas experienced significantly increased odds (OR 2.96) of experiencing IPV. A secondary analysis of Demographic and Health Survey (DHS) data drawn from across Africa (Le and Nguyen, Reference Le and Nguyen2022) further illustrated an association between the intensity of armed conflict and IPV experienced by women. A recent systematic review and meta-analysis (Murphy et al., Reference Murphy, Smith, Chandarana and Ellsberg2025) found a pooled prevalence of 39% lifetime physical or sexual violence among women and girls in conflict-affected settings, and a 24% 12-month rate.
This evidence shows that after the cessation of public violence and the signing of peace agreements, severe violence often continues in the private sphere. Anticolonial theorists have long examined how colonial violence and destruction impact human psychology and relationships. In The Wretched of the Earth, Frantz Fanon (Reference Fanon2001) described how French colonial violence in Algeria produced dehumanisation and aggression within colonised communities, sometimes surfacing in violence against partners and families. These analyses have been extended by feminist decolonial scholars (e.g., Lugones, Reference Lugones2007; Smith, Reference Smith2015; Segato and Monque, Reference Segato and Monque2021), who have further examined the ways in which colonial domination produces rigid gendered power structures that perpetuate gendered violence in post-colonial contexts.
The continuum of violence theory, first articulated by Kelly (Reference Kelly1988), provides a framework for considering how everyday, often normalised acts of gendered harassment and coercion are connected to and reinforce more extreme forms of violence. Extending this analysis to war, peace and security, Cockburn et al. (Reference Cockburn, Giles, Hyndman, Giles and Hyndman2004) argued that gendered power relations normalise violence against women and girls, whereby militarism is directly connected to everyday violence against women and girls. Cockburn et al. (Reference Cockburn, Giles, Hyndman, Giles and Hyndman2004) demonstrated how this violence persists through displacement, economic and social reconstruction, and processes of aid, justice and reconciliation. True (Reference True2010) further showed how these dynamics are also shaped by structural political and economic forces. Violence in the domestic sphere constitutes an ongoing violation of rights in itself, and also threatens longer-term peace and stability. Such violence can perpetuate trauma-related social problems, an effect that can reverberate through generations in post-conflict settings (O’Neill et al., Reference O’Neill, Armour, Bolton, Bunting, Corry, Devine, Ennis, Ferry, McKenna, McLafferty and Murphy2015). Domestic violence also prevents victims from participating in public life, which in turn impacts peace-building processes and reinforces inequality.
Traditionally, peacebuilding and humanitarian response efforts have often neglected to consider gender issues (Cockburn et al., Reference Cockburn, Giles, Hyndman, Giles and Hyndman2004; True, Reference True2010; Mulumba and Namuggala, Reference Mulumba, Namuggala, Asuelime and Francis2014; Swaine, Reference Swaine2018), leading to calls to integrate gender considerations into humanitarian programming, including the Inter-Agency Standing Committee (IASC, 2015) ‘Guidelines for Integrating Gender-Based Violence Interventions in Humanitarian Action’, which sets out priorities for addressing gender-based violence in humanitarian emergencies. Such interventions must be supported by evidence, including an understanding of empirically supported risk factors.
The complex reasons for the greater prevalence of IPV in conflict-affected regions are increasingly being explored in a growing body of evidence (Ringdal, Reference Ringdal2024; Murphy et al., Reference Murphy, Smith, Chandarana and Ellsberg2025). Some drivers of the relationship that have been explored include rigid societal gender norms during times of conflict (Reilly et al., Reference Reilly, Muldoon and Byrne2004; Ellsberg et al., Reference Ellsberg, Ovince, Murphy, Blackwell, Reddy, Stennes, Hess and Contreras2020), conflict-related trauma (Bradley, Reference Bradley2018), stigma associated with conflict-related sexual violence (Annan and Brier, Reference Annan and Brier2010); alcohol use (Kelly et al., Reference Kelly, Colantuoni, Robinson and Decker2018), breakdown of governance and rule of law (Pierson, Reference Pierson2019), disintegration of social systems and networks (Mannell et al., Reference Mannell, Grewal, Ahmad and Ahmad2021a), and greater availability of weapons (Doyle and McWilliams, Reference Doyle and McWilliams2020). As explored by Judith Butler (Reference Butler2009) in Frames of War, social processes and communications that legitimise armed conflict cultivate a perception of war as inevitable or morally just, by defining which lives are grievable and which are not. This legitimisation of public violence in wartime may also translate to greater legitimisation of violence in the domestic sphere, as the ‘frame’ of legitimate violence expands.
However, understanding of the drivers of the relationship between domestic violence and armed conflict is a comparatively underdeveloped area in research. Studies of proposed drivers have tended to focus on the impact of war-related trauma (e.g., Hecker et al., Reference Hecker, Fetz, Ainamani and Elbert2015) and post-traumatic stress disorder (PTSD; e.g., Orcutt et al., Reference Orcutt, King and King2003), with a focus on military samples. A review to broadly examine these and other potential drivers of the association is needed to better understand how to integrate prevention efforts into humanitarian programming and post-conflict peace-building. This review, therefore, aims to systematically synthesise evidence on the factors linking armed conflict and IPV.
Methodology
Search strategy
Five databases (Web of Science, EMBASE, CINAHL, PsycINFO and PubMed) were systematically searched using terms such as humanitarian, war, armed conflict, political violence, post-conflict, militant, refugee, displacement, cross-referenced with terms relating to IPV (e.g., partner violence, domestic violence, spousal abuse). The full search string is provided in Supplementary File 1.
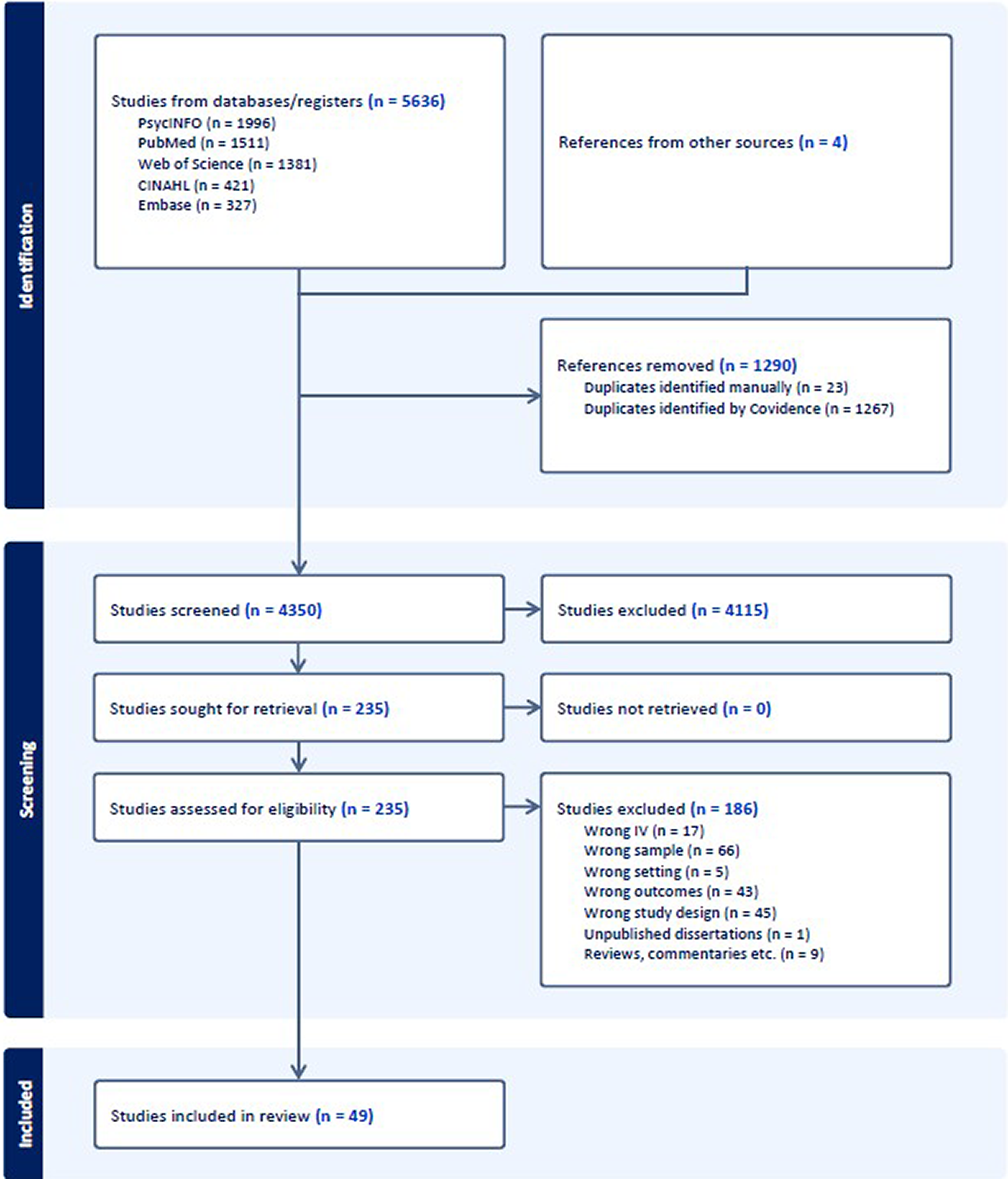
The initial search was conducted on 1 February 2024 and updated on 17 December 2025. There were 5,636 articles identified as potentially meeting the inclusion criteria. All references were exported to the systematic review platform Covidence. After removal of duplicates, 4,350 articles remained for title and abstract screening. All articles were dual-screened independently, first by title and abstract, and then in full text by two reviewers, with any conflicts in ratings settled through discussion with a third reviewer. Bibliographies of included articles were hand-searched for other potentially relevant articles. Four studies were identified through these means. See Figure 1 for further details of the screening procedure.
PRISMA diagram detailing screening process. Adapted from Page et al (Reference Page, McKenzie, Bossuyt, Boutron, Hoffmann, Mulrow and Moher2021).

Figure 1. Long description
The flowchart is divided into three vertical sections: Identification, Screening, and Included.
1. Identification Phase:
* Top-left box: Studies from databases/registers n = 5636. Breakdown: Psyc I N F O n = 1996, PubMed n = 1511, Web of Science n = 1381, C I N A H L n = 421, Embase n = 327.
* Top-right box: References from other sources n = 4.
* These two boxes merge into a central line. A lateral arrow points to a box: References removed n = 1290. Breakdown: Duplicates identified manually n = 23, Duplicates identified by Covidence n = 1267.
2. Screening Phase:
* Central box: Studies screened n = 4350. An arrow points right to: Studies excluded n = 4115.
* Central box: Studies sought for retrieval n = 235. An arrow points right to: Studies not retrieved n = 0.
* Central box: Studies assessed for eligibility n = 235. An arrow points right to a detailed exclusion box: Studies excluded n = 186. Breakdown: Wrong I V n = 17, Wrong sample n = 66, Wrong setting n = 5, Wrong outcomes n = 43, Wrong study design n = 45, Unpublished dissertations n = 1, Reviews, commentaries etc. n = 9.
3. Included Phase:
* Final central box at the bottom: Studies included in review n = 49.
Inclusion and exclusion criteria
Our inclusion criteria specified that studies should be based on adult (18+) samples of all genders, with exposure to armed conflict or political violence. Peer-reviewed quantitative, qualitative or mixed methods studies were included. It was required that studies either explicitly measured (for quantitative studies) or analysed (for qualitative studies) conflict exposure, meaning, for example, that studies with a general sample drawn from a conflict-affected region where it could not be ascertained whether participants had been exposed to armed conflict or violence were excluded. The outcome of interest was IPV, defined as physical, sexual or emotional abuse between current or former intimate partners. Any studies examining the association between armed conflict and other types of violence, such as family violence (e.g., violence against children, siblings or elders) and physical or sexual violence perpetrated by non-partners, were excluded. Studies were required to explore potential drivers of the association between armed conflict and IPV; therefore, studies only documenting the association between armed conflict and IPV without examining the factors linking them were excluded. Included studies were required to be primary research studies written in English; therefore, any reviews or commentary articles, as well as studies written in other languages, were excluded. No time restrictions were applied.
Data extraction and analysis
Data were extracted using two pre-defined data extraction tables, developed collaboratively by the study team. Study information and setting were extracted, as well as sample details, study objectives, main findings and the potential driver identified. See Tables 1 and 2 for a summary of the study characteristics. Due to the methodological heterogeneity of studies included, a narrative synthesis was deemed the most appropriate approach to analysis. Study quality was assessed using the Mixed Methods Appraisal Tool (MMAT; Hong et al., Reference Hong, Pluye, Fàbregues, Bartlett, Boardman, Cargo, Dagenais, Gagnon, Griffiths, Nicolau, O’Cathain, Rousseau and Vedel2018).
Summary of qualitative studies included in the review

Table 1. Long description
The table consists of 25 rows, each detailing a specific research study.
* Al-Natour et al. 2022, Jordan: Studied 16 Syrian refugee women using content analysis. Found war-related financial stress and changed husband behaviors led to increased I P V.
* Azizi et al. 2024, United Kingdom: Studied 15 Afghan women using thematic analysis. Found patriarchal power and lack of rights awareness increased dependence and violence risk.
* Cardoso et al. 2016, Cote d'Ivoire: Focus groups with 91 participants using grounded theory. Found loss of livelihoods and changed gender roles increased I P V risk.
* Daoud 2021, Jordan: Narrative interviews with 23 Syrian women and 13 providers. Found interconnected risks including disruption of cultural codes and conflict-related trauma.
* Doyle and McWilliams 2020, Northern Ireland: Comparative interviews from 1992 and 2016. Found transition to peace improved reporting, but paramilitary influence on control persisted.
* Falb et al. 2014, Cote d'Ivoire: Interviews with 32 men. Found economic empowerment programs for women were accepted but challenged traditional male provider identities.
* Falb et al. 2022, Myanmar and D R C: Interviews and focus groups with over 100 participants. Found power imbalances and exposure to armed conflict exacerbated domestic violence.
* Finley et al. 2010, United States: Interviews with 19 male veterans and 11 spouses. Categorized I P V into anger-based, dissociative, and parasomniac violence related to P T S D.
* Fitzgerald et al. 2021, Palestine: Interviews with 25 women in Gaza. Identified societal expectations and distrust of services as barriers to help-seeking.
* Friedman et al. 2025, United States: Secondary analysis of military partner interviews. Found high firearm ownership and alcohol use as significant risk factors.
* Gerlock et al. 2014, United States: Study of 441 veteran couples. Found P T S D and deployment-related disabilities added relationship stress and increased vulnerability to abuse.
* Guruge et al. 2017, Sri Lanka: Interviews with 15 survivors and 15 providers. Found I P V related to war trauma and men using violence to regain perceived lost masculinity.
* Horn et al. 2014, Sierra Leone and Liberia: Focus groups and interviews with 130 women. Found war normalized violence but sometimes increased women's economic independence.
* Kaul et al. 2024, Afghanistan: Interviews with 60 women and 60 men. Found compounding traumatic experiences of war and lack of mental health services worsened outcomes.
* Kattoura 2022, Israel: Interviews with 36 Arab women. Found structural oppression and political violence projected inward into private intimate relationships.
* Kelly et al. 2012, D R C: Focus groups with 86 participants. Found I P V often resulted from a cycle of blame and anger following conflict-related sexual violence.
* Kiconco and Nthakomwa 2018, Uganda: Interviews with 40 ex-abductees. Found social stigma against women abducted by the L R A reduced reintegration opportunities.
* Kohli et al. 2015, D R C: Interviews with 13 survivors and 5 perpetrators. Linked I P V to alcohol use, economic instability, and gendered power dynamics.
* Lukasiak et al. 2024, Uganda: Interviews with 13 refugee women. Found shifting power dynamics in camps where women became providers increased violence risk.
* Makuch et al. 2021, Brazil: Focus groups with 111 Venezuelan migrant women. Found physical and psychological violence common in shelters, driven by rigid gender roles.
* Mannell et al. 2021a, Afghanistan: Interviews with 20 women. Linked domestic violence to the loss of patriarchal support and the conflict-driven drug trade.
* Restrepo et al. 2024, Colombia: Interviews with 47 women. Found armed conflict amplified patriarchal norms and hypermasculinity.
* Wachter et al. 2018, South Sudan, Kenya, and Iraq: 284 participants. Found displacement destabilized gender roles and increased risk through forced or rapid marriages.
* Wirtz et al. 2014, Colombia: Interviews with 35 survivors and 31 providers. Found G B V perpetrated by both armed actors and intimate partners during displacement.
* Zannettino 2012, Australia: Focus groups with Liberian refugee women. Found migration stressors and changing gender norms made men feel threatened by women's autonomy.
Summary of quantitative studies included in the review

Table 2. Long description
The table consists of 8 columns: Authors, year, country; Sample details; Reported I P V; Study design; Analysis; Study aims/objectives; Main findings; and Proposed driver.
Key entries include:
* Botchkovar et al. 2025, Ukraine: Random sample of 1,185 adults. Findings show daily stressors, negative emotions, and alcohol use predicted I P V, while war exposure had an indirect effect.
* Bourey et al. 2024, Democratic Republic of Congo: 2,080 men. Findings linked interpersonal violence and trauma symptoms to I P V use.
* Cesur and Sabia 2016, United States: 11,474 service men. Combat exposure was associated with domestic violence, mediated by mental health and substance use.
* Creech et al. 2017, United States: 102 women veterans. Alcohol issues and psychological I P V experience were associated with physical I P V use.
* Chiu et al. 2022, United States: 217 veterans. T B I and neurocognitive performance predicted subsequent I P V.
* Gibbs et al. 2021, Palestine: 534 women. Occupation-related events increased I P V experience via depressive symptoms and relationship conflict.
* Gupta et al. 2012, South Africa: 772 men. Significant association between human rights violations and physical I P V perpetration.
* Jewkes et al. 2017, Papua New Guinea: 746 men and 793 women. War trauma related to P T S D and alcohol problems, which affected I P V perpetration.
* Lane et al. 2022, United Kingdom: 4,566 military personnel. Risk factors included childhood adversity, military trauma, and mental health problems.
* Rees et al. 2018, Timor-Leste: 870 individuals. Torture exposure directly and indirectly (via P T S D and drinking) associated with I P V.
* Rojczyk et al. 2024, United States: 49 veterans. Neuroimaging showed psychological aggression associated with right amygdala-hippocampus complex abnormalities.
* Taft et al. 2007, 2015, United States: Multiple studies linking P T S D, hyperarousal, and hostile attribution biases to I P V perpetration.
As this project was funded as part of a funded research collaboration between Ireland and Uganda to develop new research collaboration networks, the findings of the review were presented at a meeting of stakeholders and activists engaged in work relating to refugee and displacement issues, and gender-based violence prevention and support, in Kampala, Uganda, in October 2024. Preliminary findings were discussed at the stakeholder meeting, with a focus on how the findings may apply to the Ugandan context. This process also served to refine and develop the findings through discussion and validation. The findings were grouped and analysed by population, separately considering military samples, refugee and internally displaced samples, and separately considering perpetration and victimisation. Possible drivers at the individual, relational and structural levels are explored.
Results
Study characteristics
The final search returned 49 articles. Quantitative and qualitative studies are presented separately (see Tables 1 and 2). In total, 25 included studies were qualitative and 24 were quantitative. Of the quantitative studies, all but one (Chiu et al., Reference Chiu, Gnall, Pless Kaiser, Taft, Franz, Lee and Vasterling2022) were cross-sectional, and the majority (k = 14) were conducted in the United States (US) on army veterans returning to civilian life, with relatively few studies focused on low- and middle-income countries (LMICs). Study context and sampling procedures differed substantially, including military samples from high-income countries such as the US, as well as community-based studies and household surveys in LMICs.
Quality assessment
The quality of included studies was high overall (see Supplementary Tables 3 and 4 in Supplementary Files 2 and 3 for full details of quality assessment). Among the qualitative studies, sampling and analytic procedures were generally well-outlined and appropriate to the research questions. In a minority of cases, the qualitative methodologies and approaches to sampling were not adequately described to clearly ascertain their appropriateness to the research question. However, in most cases, the findings were well-supported by data and methods were clearly outlined and justified. Similarly, the overall quality of the included quantitative studies was high, with several articles drawing on random samples and meeting all MMAT quality assessment criteria (Jewkes et al., Reference Jewkes, Jama-Shai and Sikweyiya2017; Rees et al., Reference Rees, Mohsin, Tay, Steel, Tam, da Costa, Soares, Tol, Eapen, Dadds and Silove2018; Gibbs et al., Reference Gibbs, Abdelatif, Said and Jewkes2021; Lane et al., Reference Lane, Short, Jones, Hull, Howard, Fear and MacManus2022; Botchkovar et al., Reference Botchkovar, Antonaccio, Timmer, Magin, Johnson and Hughes2025). Studies differed in how they conceptualised and measured conflict exposure, with some using military deployment to conflict zones as a proxy for conflict exposure, and others directly measuring exposure using dichotomous items capturing conflict-related events or standardised scales.
Across quantitative studies, methods of measuring IPV varied significantly, which presents a challenge for the comparison of findings. For example, some studies used dichotomous (yes/no) items (e.g., Gupta et al., Reference Gupta, Reed, Kelly, Stein and Williams2012; Cesur and Sabia, Reference Cesur and Sabia2016), while others used standardised scales, such as the Conflict Tactics Scale-2 (CTS2; Straus et al., Reference Straus, Hamby, Boney-McCoy and Sugarman1996) which ask participants to report on the frequency of a range of abusive behaviours or experiences from a given time period (e.g., 6 or 12 months). A total of 10 included studies used a version of the CTS or its subscales (Orcutt et al., Reference Orcutt, King and King2003; Taft et al., Reference Taft, Pless, Stalans, Koenen, King and King2005; Taft et al., Reference Taft, Street, Marshall, Dowdall and Riggs2007; Kar and O’Leary, Reference Kar and O’Leary2013; Tharp et al., Reference Tharp, Sherman, Bowling and Townsend2016; Creech et al., Reference Creech, Macdonald and Taft2017; Heavey et al., Reference Heavey, Homish, Goodell and Homish2017; Snir et al., Reference Snir, Itzhaky and Solomon2017; Chiu et al., Reference Chiu, Gnall, Pless Kaiser, Taft, Franz, Lee and Vasterling2022; Rojczyk et al., Reference Rojczyk, Heller, Seitz-Holland, Kaufmann, Sydnor, Berger, Pankatz, Rathi, Bouix, Pasternak, Salat, Hinds, Esopenko, Fortier, Milberg, Shenton and Koerte2024). All of the studies using the CTS were based on samples from the US or Israel. Other measures used included the Severity of Violence Against Women Scale (Marshall, Reference Marshall1992; used with a sample of Liberian women by Sileo et al., Reference Sileo, Kershaw, Gilliam, Taylor, Kommajosula and Callands2021); the Composite Abuse Scale (Hegarty et al., Reference Hegarty, Bush and Sheehan2005; used with a sample from Uganda by Saile et al., Reference Saile, Neuner, Ertl and Catani2013). Other studies used and adapted items from large-scale surveys such as the WHO Multi-Country Study on Domestic Violence (Garcia-Moreno et al., Reference Garcia-Moreno, Jansen, Ellsberg, Heise and Watts2006; used by Gibbs et al., Reference Gibbs, Abdelatif, Said and Jewkes2021, in Palestine and by Jewkes et al., Reference Jewkes, Jama-Shai and Sikweyiya2017 in Papua New Guinea).
Studies differed in relation to whether they studied one or both partners, and whether they considered victimisation, perpetration or both. Studies also differed in their operational definitions of IPV and the types of violence included for consideration. For example, some studies (e.g., Snir et al., Reference Snir, Itzhaky and Solomon2017; Rees et al., Reference Rees, Mohsin, Tay, Steel, Tam, da Costa, Soares, Tol, Eapen, Dadds and Silove2018) omitted consideration of sexual IPV. Finally, quantitative studies also considered different time periods when asking participants about abuse. For example, some asked participants to report on the previous 6 months (e.g., Creech et al., Reference Creech, Macdonald and Taft2017; Chiu et al., Reference Chiu, Gnall, Pless Kaiser, Taft, Franz, Lee and Vasterling2022), some considered past-year IPV (e.g., Taft et al., Reference Taft, Pless, Stalans, Koenen, King and King2005; Teten et al., Reference Teten, Schumacher, Taft, Stanley, Kent, Bailey, Dunn and White2010; Saile et al., Reference Saile, Neuner, Ertl and Catani2013; Cesur and Sabia, Reference Cesur and Sabia2016; Jewkes et al., Reference Jewkes, Jama-Shai and Sikweyiya2017) and others considered lifetime rates (e.g., Iverson et al., Reference Iverson, Sayer, Meterko, Stolzmann, Suri, Gormley, Nealon Seibert, Yan and Pogoda2020).
Armed conflict and IPV: Drivers of the association
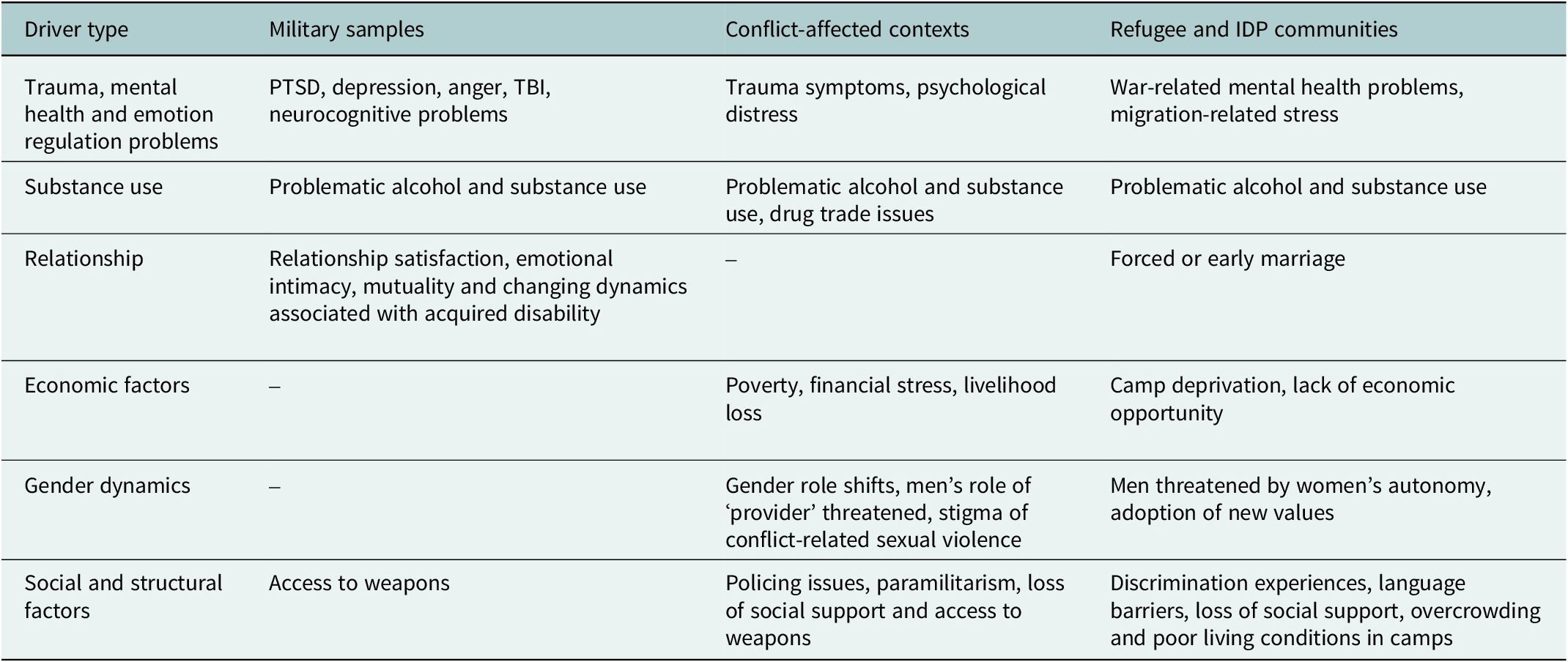
The next sections describe findings on the factors identified by the literature as drivers of the association between armed conflict and IPV. These factors are divided broadly by population, according to the following groupings: (1) military samples, (2) populations in conflict-affected contexts and (3) refugees and displaced persons. A brief summary of drivers separated by group is provided in Table 3.
Summary of drivers separated by population

Table 3. Long description
The table consists of four columns and six rows of data.
1. Trauma, mental health and emotion regulation problems: Military samples list P T S D, depression, anger, T B I, and neurocognitive problems. Conflict-affected contexts list trauma symptoms and psychological distress. Refugee and I D P communities list war-related mental health problems and migration-related stress.
2. Substance use: All three populations list problematic alcohol and substance use, with conflict-affected contexts also noting drug trade issues.
3. Relationship: Military samples list relationship satisfaction, emotional intimacy, mutuality, and changing dynamics with disability. Conflict-affected contexts have no data. Refugee and I D P communities list forced or early marriage.
4. Economic factors: Military samples have no data. Conflict-affected contexts list poverty, financial stress, and livelihood loss. Refugee and I D P communities list camp deprivation and lack of economic opportunity.
5. Gender dynamics: Military samples have no data. Conflict-affected contexts list gender role shifts, threats to the provider role, and stigma of conflict-related sexual violence. Refugee and I D P communities list men threatened by women's autonomy and adoption of new values.
6. Social and structural factors: Military samples list access to weapons. Conflict-affected contexts list policing issues, paramilitarism, loss of social support, and access to weapons. Refugee and I D P communities list discrimination, language barriers, loss of social support, and overcrowding in camps.
Military samples
Studies based on military samples or the partners of military personnel were based primarily in the US (Orcutt et al., Reference Orcutt, King and King2003; Taft et al., Reference Taft, Pless, Stalans, Koenen, King and King2005; Taft et al., Reference Taft, Street, Marshall, Dowdall and Riggs2007; Finley et al., Reference Finley, Baker, Pugh and Peterson2010; Teten et al., Reference Teten, Schumacher, Taft, Stanley, Kent, Bailey, Dunn and White2010; Kar and O’Leary, Reference Kar and O’Leary2013; Gerlock et al., Reference Gerlock, Grimesey and Sayre2014; Taft et al., Reference Taft, Weatherill, Scott, Thomas, Kang and Eckhardt2015; Cesur and Sabia, Reference Cesur and Sabia2016; Gerlock et al., Reference Gerlock, Szarka, Cox and Harel2016; Tharp et al., Reference Tharp, Sherman, Bowling and Townsend2016; Creech et al., Reference Creech, Macdonald and Taft2017; Heavey et al., Reference Heavey, Homish, Goodell and Homish2017; Iverson et al., Reference Iverson, Sayer, Meterko, Stolzmann, Suri, Gormley, Nealon Seibert, Yan and Pogoda2020; Chiu et al., Reference Chiu, Gnall, Pless Kaiser, Taft, Franz, Lee and Vasterling2022; Rojczyk et al., Reference Rojczyk, Heller, Seitz-Holland, Kaufmann, Sydnor, Berger, Pankatz, Rathi, Bouix, Pasternak, Salat, Hinds, Esopenko, Fortier, Milberg, Shenton and Koerte2024; Friedman et al., Reference Friedman, Moceri-Brooks, Meza, Ho, Baker and Bryan2025), with one each from the UK (Lane et al., Reference Lane, Short, Jones, Hull, Howard, Fear and MacManus2022) and Israel (Snir et al., Reference Snir, Itzhaky and Solomon2017). These studies tended to examine individual-level variables that increased the risk of IPV perpetration and victimisation in conflict-exposed military personnel. The most commonly examined driver of the association between armed conflict and IPV perpetration across these studies was PTSD, which was examined by ten of the quantitative studies on military samples. The analysed evidence widely supports PTSD as a significant risk factor for IPV perpetration among conflict-exposed military samples from high-income countries. For example, Orcutt et al. (Reference Orcutt, King and King2003) found that PTSD symptom severity significantly mediated the relationship between warzone stressors and IPV. Similarly, Teten et al. (Reference Teten, Schumacher, Taft, Stanley, Kent, Bailey, Dunn and White2010) found that US Army veterans with PTSD reported a higher level of perpetration compared with veterans without PTSD.
However, there were a few studies that potentially complicate the straightforward conceptualisation of PTSD as a risk factor for IPV. For example, in a study with Israeli military veterans, Snir et al. (Reference Snir, Itzhaky and Solomon2017) found that aggressive impulses were associated with both suicidality and IPV. The authors found that aggressive impulses arising from conflict exposure increased the likelihood of both suicidality and IPV; however, these associations were moderated by PTSD and guilt. Specifically, aggressive impulses were associated with suicidality in the presence of PTSD symptoms and high levels of guilt, whereas aggressive impulses were associated with IPV in the absence of PTSD and under conditions of low guilt. The authors proposed that guilt may represent the internalisation of a moral code, shaping whether aggressive impulses are turned inward on the self or outward towards others. Drawing on Lifton (Reference Lifton1973), they further suggest that wartime produces detachment and depersonalisation in those who participate in it, reducing guilt associated with violent acts, potentially facilitating the persistence of outward aggression in the private sphere post-conflict. Tharp et al. (Reference Tharp, Sherman, Bowling and Townsend2016) also examined patterns of relationship aggression in US Army veterans seeking couple’s therapy and found no difference in mean aggression between those with and without a PTSD diagnosis. However, Tharp et al. (Reference Tharp, Sherman, Bowling and Townsend2016) conceptualised PTSD as a categorical variable, while many of the other studies examining the role of PTSD treated it as a dimensional variable, which may have impacted the results.
Problematic alcohol use was also commonly investigated as a potential contributor to the relationship between conflict exposure and IPV, reported as a significant perpetration-related factor in 12 studies across the review, and five military samples. This evidence supports the significance of alcohol as a driver of the association between armed conflict and IPV. For example, in a longitudinal study of US Army veterans, Chiu et al. (Reference Chiu, Gnall, Pless Kaiser, Taft, Franz, Lee and Vasterling2022) found that problematic alcohol use was associated with partner-corroborated reports of both physical and psychological abuse. Other risk factors investigated in the military samples included mental health problems such as depression, attachment styles, anger and traumatic brain injury (TBI).
Some included studies directly investigated associations between exposure to armed conflict and relationship characteristics. For example, Gerlock et al. (Reference Gerlock, Grimesey and Sayre2014) qualitatively interviewed a sample of US Army veterans and their families, identifying various relationship dynamics that were perceived by respondents as linked to aggression in their relationships. These involved situations, for example, where veterans had acquired a disability during their deployment, placing their partner in a caregiver role, thereby increasing veterans’ vulnerability to abuse. A further study by Gerlock et al. (Reference Gerlock, Szarka, Cox and Harel2016) involved an exploratory analysis of a range of factors (e.g., family of origin violence, PTSD severity and demographic factors) to assess whether they differentiate veterans who were violent to their partners from those who were not. Gerlock et al. (Reference Gerlock, Szarka, Cox and Harel2016) identified only the factor of relationship mutuality to significantly differentiate these two groups, a construct defined as ‘the bi-directional movement of feelings, thoughts and activity between persons in a relationship’ (p. 673, Gerlock et al., Reference Gerlock, Szarka, Cox and Harel2016). Similarly, a study of women army veterans from the US (Creech et al., Reference Creech, Macdonald and Taft2017) reported that relationship satisfaction explained a significant amount of the variance in the women’s recent psychological IPV.
Conflict-affected contexts
Studies from conflict-affected contexts included consideration of a range of geographic locations, including Cote D’Ivoire (Falb et al., Reference Falb, Annan, King, Hopkins, Kpebo and Gupta2014; Cardoso et al., Reference Cardoso, Gupta, Shuman, Cole, Kpebo and Falb2016); Northern Ireland (Doyle and McWilliams, Reference Doyle and McWilliams2020); Myanmar (Falb et al., Reference Falb, Asghar, Pardo, Hategekimana, Kakay, Roth and O’Connor2022), the Democratic Republic of Congo (DRC; Bourey et al., Reference Bourey, Musci, Bass, Glass, Matabaro and Kelly2024; Falb et al., Reference Falb, Asghar, Pardo, Hategekimana, Kakay, Roth and O’Connor2022; Kelly et al., Reference Kelly, Kabanga, Cragin, Alcayna-Stevens, Haider and Vanrooyen2012; Kohli et al., Reference Kohli, Perrin, Mpanano, Banywesize, Mirindi, Banywesize, Mitima, Binkurhorhwa, Bufole and Glass2015); Sri Lanka (Guruge et al., Reference Guruge, Ford-Gilboe, Varcoe, Jayasuriya-Illesinghe, Ganesan, Sivayogan, Kanthasamy, Shanmugalingam and Vithanarachchi2017); Sierra Leone (Horn et al., Reference Horn, Puffer, Roesch and Lehmann2014); Liberia (Horn et al., Reference Horn, Puffer, Roesch and Lehmann2014; Sileo et al., Reference Sileo, Kershaw, Gilliam, Taylor, Kommajosula and Callands2021); Afghanistan (Mannell et al., Reference Mannell, Grewal, Ahmad and Ahmad2021a; Kaul et al., Reference Kaul, Saboor, Ahmad, Mannell, Paphitis and Devakumar2024); Palestine (Fitzgerald et al., Reference Fitzgerald, Chi and Cheyney2021; Gibbs et al., Reference Gibbs, Abdelatif, Said and Jewkes2021); Israel (Kattoura, Reference Kattoura2022); Uganda (Saile et al., Reference Saile, Neuner, Ertl and Catani2013; Kiconco and Nthakomwa, Reference Kiconco and Nthakomwa2018), Columbia (Restrepo et al., Reference Restrepo, Padilla, Ungemack and Schensul2024), Ukraine (Botchkovar et al., Reference Botchkovar, Antonaccio, Timmer, Magin, Johnson and Hughes2025), Papua New Guinea (Jewkes et al., Reference Jewkes, Jama-Shai and Sikweyiya2017) and South Africa (Gupta et al., Reference Gupta, Reed, Kelly, Stein and Williams2012). Similar to the studies with military samples, several of these studies also examined the ways in which the trauma of war and armed conflict can increase the risk of IPV. For example, studies by Gupta et al. (Reference Gupta, Reed, Kelly, Stein and Williams2012), Rees et al. (Reference Rees, Mohsin, Tay, Steel, Tam, da Costa, Soares, Tol, Eapen, Dadds and Silove2018) and Gibbs et al. (Reference Gibbs, Abdelatif, Said and Jewkes2021) found that experiencing human rights violations such as torture and occupation-related violence and loss were associated with increased risk of perpetration. These studies also investigated other mental health problems and the role of alcohol use, indicating a role of these factors in increasing the risk of IPV. For example, Rees et al. (Reference Rees, Mohsin, Tay, Steel, Tam, da Costa, Soares, Tol, Eapen, Dadds and Silove2018) found that mental disturbance (defined as the presence of hazardous drinking, severe psychological distress or PTSD) mediated the relationship between torture exposure and IPV perpetration. Similarly to findings from the military samples, alcohol use was perceived by respondents in studies from several conflict-affected contexts to be a significant factor influencing the severity and frequency of perpetration (Kohli et al., Reference Kohli, Perrin, Mpanano, Banywesize, Mirindi, Banywesize, Mitima, Binkurhorhwa, Bufole and Glass2015; Guruge et al., Reference Guruge, Ford-Gilboe, Varcoe, Jayasuriya-Illesinghe, Ganesan, Sivayogan, Kanthasamy, Shanmugalingam and Vithanarachchi2017; Kiconco and Nthakomwa, Reference Kiconco and Nthakomwa2018).
There is some evidence from the studies included in this review that conflict-related trauma and PTSD can also increase vulnerability to victimisation, as well as increasing the likelihood of perpetration. For example, Saile et al. (Reference Saile, Neuner, Ertl and Catani2013) conducted a cross-sectional quantitative study examining factors affecting IPV risk in conflict-affected communities of Northern Uganda. Saile et al. (Reference Saile, Neuner, Ertl and Catani2013) found that women’s exposure to war trauma and related re-experiencing symptoms were associated with IPV experience. Somewhat similarly, Sileo et al. (Reference Sileo, Kershaw, Gilliam, Taylor, Kommajosula and Callands2021) conducted a quantitative study of pregnant women in post-conflict Liberia and found that women’s trauma (including conflict-related trauma) was associated with the severity of their IPV experiences.
Several included studies from conflict-affected contexts highlighted how the structural and societal consequences of war and armed conflict can affect dynamics relating to IPV perpetration and victimisation. One widely investigated factor, explored in several included studies (e.g., Cardoso et al., Reference Cardoso, Gupta, Shuman, Cole, Kpebo and Falb2016; Wachter et al., Reference Wachter, Horn, Friis, Falb, Ward, Apio, Wanjiku and Puffer2018; Falb et al., Reference Falb, Asghar, Pardo, Hategekimana, Kakay, Roth and O’Connor2022), concerned the economic effects of conflict. For example, in a study from Côte d’Ivoire (Cardoso et al., Reference Cardoso, Gupta, Shuman, Cole, Kpebo and Falb2016), respondents described how the conflict had affected people’s ability to earn livelihoods, resulting in problems such as poverty, lack of social support and financial stress, which were all factors perceived by respondents to affect men’s likelihood of perpetrating IPV. Similarly, Falb et al. (Reference Falb, Asghar, Pardo, Hategekimana, Kakay, Roth and O’Connor2022) found that economic and financial instability in the aftermath of conflict was perceived to be a major source of ongoing stress and emotional problems, which increased the risk of IPV perpetration.
Another social factor highlighted in several studies (e.g., Zannettino, Reference Zannettino2012; Falb et al., Reference Falb, Annan, King, Hopkins, Kpebo and Gupta2014; Kohli et al., Reference Kohli, Perrin, Mpanano, Banywesize, Mirindi, Banywesize, Mitima, Binkurhorhwa, Bufole and Glass2015; Cardoso et al., Reference Cardoso, Gupta, Shuman, Cole, Kpebo and Falb2016; Guruge et al., Reference Guruge, Ford-Gilboe, Varcoe, Jayasuriya-Illesinghe, Ganesan, Sivayogan, Kanthasamy, Shanmugalingam and Vithanarachchi2017; Wachter et al., Reference Wachter, Horn, Friis, Falb, Ward, Apio, Wanjiku and Puffer2018; Daoud, Reference Daoud2021; Al-Natour et al., Reference Al-Natour, Morris and Mohammad Al-Ostaz2022) was gender relations. This was reflected, for example, in the findings of Guruge et al. (Reference Guruge, Ford-Gilboe, Varcoe, Jayasuriya-Illesinghe, Ganesan, Sivayogan, Kanthasamy, Shanmugalingam and Vithanarachchi2017) from Sri Lanka, whereby social changes associated with the conflict were reported as resulting in men’s traditional social roles being threatened, contributing to resentment towards their partners. Falb et al. (Reference Falb, Annan, King, Hopkins, Kpebo and Gupta2014) also found that men’s frustration at not being able to fulfil their perceived gender role of providing financially for their families resulted in feelings of shame, which in turn increased the risk of IPV.
Some studies highlighted the impact of gendered social stigma towards women who survived conflict-related sexual violence (e.g., Kelly et al., Reference Kelly, Kabanga, Cragin, Alcayna-Stevens, Haider and Vanrooyen2012; Kiconco and Nthakomwa, Reference Kiconco and Nthakomwa2018; Daoud, Reference Daoud2021). For example, a qualitative study from the Democratic Republic of Congo (DRC) by Kelly et al. (Reference Kelly, Kabanga, Cragin, Alcayna-Stevens, Haider and Vanrooyen2012) reported a dynamic whereby women who survived conflict-related rape experienced blame from their husbands as well as social ostracisation; respondents described how survivors were sometimes accused of failing to resist the rape, and how rape can result in women being socially devalued due to gendered social norms. A study from Uganda (Kiconco and Nthakomwa, Reference Kiconco and Nthakomwa2018), based on interviews with women who were abducted by the Lord’s Resistance Army (LRA), identified a similar pattern, where women who experienced sexual violence experienced stigma, shame and ostracisation on their reintegration into society.
The intersection between gender role changes and economic factors was noted in multiple studies from conflict-affected and displacement contexts (e.g., Kohli et al., Reference Kohli, Perrin, Mpanano, Banywesize, Mirindi, Banywesize, Mitima, Binkurhorhwa, Bufole and Glass2015; Cardoso et al., Reference Cardoso, Gupta, Shuman, Cole, Kpebo and Falb2016; Daoud, Reference Daoud2021; Al-Natour et al., Reference Al-Natour, Morris and Mohammad Al-Ostaz2022). Respondents from focus groups with conflict-affected communities in Côte d’Ivoire (Cardoso et al., Reference Cardoso, Gupta, Shuman, Cole, Kpebo and Falb2016) described how the conflict created a necessity for some women to be more economically independent. Respondents reported that this change in gender roles, coupled with men’s difficulties in securing employment post-conflict, was a factor that increased IPV. Daoud (Reference Daoud2021), in a study of Syrian refugee women in Jordan, reported that men’s failure to economically provide for their families was a source of stress and shame, which resulted in increased IPV perpetration. Similar dynamics were reported by Kohli et al. (Reference Kohli, Perrin, Mpanano, Banywesize, Mirindi, Banywesize, Mitima, Binkurhorhwa, Bufole and Glass2015) in the Democratic Republic of Congo and Al-Natour et al. (Reference Al-Natour, Morris and Mohammad Al-Ostaz2022) in Jordan. Mannell et al. (Reference Mannell, Grewal, Ahmad and Ahmad2021a), in their study of women seeking refuge from domestic violence in Afghanistan, also found that the ways in which the conflict affected the social fabric and norms of daily life were central to the women’s understanding of how the conflict influenced their experience of IPV. Respondents interviewed by Mannell et al. (Reference Mannell, Grewal, Ahmad and Ahmad2021a) described how the loss of trusted patriarchal support, issues relating to addiction and violence due to the drug trade, and conflict-related poverty, all created increased risks for women of exposure to IPV.
In their qualitative comparative analysis of women’s experience of IPV in Northern Ireland from conflict to post-conflict, Doyle and McWilliams (Reference Doyle and McWilliams2020) identified a significant role of policing and access to justice. The study examined the ways in which the occurrence of violent conflict can affect police responsiveness to IPV and protection of victims. Doyle and McWilliams (Reference Doyle and McWilliams2020) noted that during the conflict in Northern Ireland, Catholic or nationalist communities often viewed the police as a source of harassment or discrimination, rather than protection, which further reduced victims’ likelihood of seeking access to justice by these means. In this context, paramilitarism also impacted women’s experiences of IPV. Respondents interviewed by Doyle and McWilliams (Reference Doyle and McWilliams2020) described how impunity, power and control associated with paramilitary membership continued to influence IPV in Northern Ireland many years after the official cessation of the political conflict, and that paramilitary involvement (whether genuine or fabricated) could provide an additional source of power for perpetrators to leverage over victims.
Availability of firearms was highlighted by Doyle and McWilliams (Reference Doyle and McWilliams2020) as a factor that affected women’s experiences of IPV in Northern Ireland. This was experienced by the women respondents as an additional source of threat that perpetrators exploited. This is similar to findings reported by Gerlock et al. (Reference Gerlock, Grimesey and Sayre2014) and Friedman et al. (Reference Friedman, Moceri-Brooks, Meza, Ho, Baker and Bryan2025) of US Army veterans and their partners, where partners’ knowledge of the veterans’ capacity to access weapons was seen as a factor that instigated significant fear and anxiety among partners.
Refugee and internally displaced communities
Several studies specifically examined drivers of the relationship between armed conflict and IPV in the context of migration and displacement. These samples included Syrian refugee women in Jordan (Daoud, Reference Daoud2021; Al-Natour et al., Reference Al-Natour, Morris and Mohammad Al-Ostaz2022), Afghan women in the UK (Azizi et al., Reference Azizi, Lane and Boyce2024), women refugees from Burundi and the DRC in Uganda (Lukasiak et al., Reference Lukasiak, Palmieri, Svensson, Tumwine and Agardh2024), Venezuelan women in Brazil (Makuch et al., Reference Makuch, Osis, Becerra, Brasil, de Amorim and Bahamondes2021), refugee communities in Kenya, Iraq and South Sudan (Wachter et al., Reference Wachter, Horn, Friis, Falb, Ward, Apio, Wanjiku and Puffer2018), and communities of internally displaced persons in Columbia (Wirtz et al., Reference Wirtz, Pham, Glass, Loochkartt, Kidane, Cuspoca, Rubenstein, Singh and Vu2014) and Côte d’Ivoire (Cardoso et al., Reference Cardoso, Gupta, Shuman, Cole, Kpebo and Falb2016). Similar to studies carried out across other samples and contexts, mental distress associated with war and armed conflict was commonly cited as a driver of IPV. For example, in a qualitative study of Syrian refugee women living in Jordan, Al-Natour et al. (Reference Al-Natour, Morris and Mohammad Al-Ostaz2022) highlighted men’s war-related mental health problems as a factor perceived by women to affect IPV perpetration. Respondents reported how their husbands became violent for the first time during the war. One participant stated: ‘The war emotionally affected my husband a lot. His nervousness increased a lot here in Jordan. He became extreme, now he has a temper, he is so moody and a troublemaker, if something bothered him in his work, he starts fighting with us for no reason’, (Al-Natour et al., Reference Al-Natour, Morris and Mohammad Al-Ostaz2022, p. 28,).
Similar to the studies from conflict-affected contexts, studies with refugee and IDP communities also highlighted the significance of economic factors in increasing IPV risk in conflict-affected settings. For example, in Wachter et al.’s (Reference Wachter, Horn, Friis, Falb, Ward, Apio, Wanjiku and Puffer2018) study of refugee samples in South Sudan, Kenya and Iraq, it was reported that economic deprivation in camp settings in some cases increased the likelihood of women marrying rapidly or being forced into marriage, which was a factor that could also increase the risk of IPV. The same dynamic was reported by Daoud (Reference Daoud2021) in a study of Syrian refugees living in Jordan.
As noted in relation to research from conflict-affected countries, gender dynamics also emerged as significant in relation to IPV in refugee and IDP communities. Included studies described various ways in which conflict and displacement affect gender norms in ways that can, in turn, affect the occurrence of IPV. For example, Wachter et al. (Reference Wachter, Horn, Friis, Falb, Ward, Apio, Wanjiku and Puffer2018) found that women in some refugee camps reported that opportunities to attend training and develop skills resulted in empowerment, which was threatening to men and could precipitate IPV. Some respondents reported that IPV was perpetrated due to men’s perception that women were adopting Western cultural values. Similarly, in a qualitative study with Liberian refugee women living in South Australia, Zannettino (Reference Zannettino2012) reported that cultural differences between Australia and Liberia were perceived as increasing the risk of IPV, whereby men were reported as sometimes perpetrating IPV due to feeling threatened by women’s increased autonomy in the new context. On the other hand, some respondents interviewed by Wachter et al. (Reference Wachter, Horn, Friis, Falb, Ward, Apio, Wanjiku and Puffer2018), who were migrating from more liberal settings, reported finding the camps to be oppressive and highly conservative, feeling their freedoms were limited and their experience of harassment and judgement intensified. The stress of migration was also highlighted in some included studies as affecting the risk of IPV. For example, respondents in Cardoso et al. (Reference Cardoso, Gupta, Shuman, Cole, Kpebo and Falb2016) described how social discrimination against internally displaced people (IDPs) resulted in greater vulnerability to poverty, food insecurity and IPV for women. In a study of Venezuelan refugee women in Brazil (Makuch et al., Reference Makuch, Osis, Becerra, Brasil, de Amorim and Bahamondes2021), xenophobia from the local community was described as compounding other forms of violence they experienced, including violence from their partners.
In a study across three refugee camps Kenya (Dadaab), South Sudan (Ajuong Thok) and Iraq (Domiz) by Wachter et al. (Reference Wachter, Horn, Friis, Falb, Ward, Apio, Wanjiku and Puffer2018), some respondents reported that men using alcohol or other substances to cope with the stress of camp life and unemployment increased the risk of IPV. Wachter et al. (Reference Wachter, Horn, Friis, Falb, Ward, Apio, Wanjiku and Puffer2018) also noted that displacement acted as a risk factor for IPV by removing people from their social support and protective networks. In a study of Afghan women in the UK seeking asylum or family reunification (Azizi et al., Reference Azizi, Lane and Boyce2024), women reported experiences of multiple types of violence, including pre-migration political violence, IPV and other types of family violence. Azizi et al., Reference Azizi, Lane and Boyce2024 noted how migration to flee from conflict and violence can create increased vulnerability to experiencing IPV due to language barriers in the host country, lack of knowledge about criminal justice systems, and financial dependency on the perpetrator. In a study of Syrian refugee women in Jordan (Al-Natour et al., Reference Al-Natour, Morris and Mohammad Al-Ostaz2022), respondents perceived that economic instability and uncertainty were exacerbated by relocation to a country with a higher cost of living, which in turn created a higher risk of IPV perpetration.
Other migration-related stressors highlighted by Liberian refugee women living in Australia (Zannettino, Reference Zannettino2012) included coping with the experience of having lived through conflict, experiencing conflict-related violence, needing to flee, the grief of losing family members to violence or of needing to leave family members behind, as well as the stress associated with living in transient accommodation. Zannettino’s (Reference Zannettino2012) findings highlight how migration-related stressors create emotional dysregulation and gender role stress that may increase the likelihood of IPV.
Discussion
This review examined the state of current evidence on drivers of the relationship between armed conflict and IPV. A range of individual, relational and societal drivers of the relationship were identified. Among the most-studied factors were psychological trauma, PTSD and related social and mental health problems. Several included studies noted the significant role of trauma and PTSD, including exposure to the most extreme forms of conflict-related violence, such as experiencing atrocities (e.g., Taft et al., Reference Taft, Pless, Stalans, Koenen, King and King2005) or torture (Rees et al., Reference Rees, Mohsin, Tay, Steel, Tam, da Costa, Soares, Tol, Eapen, Dadds and Silove2018). This is consistent with existing literature on the impact of trauma (e.g., May and Wisco, Reference May and Wisco2016), which shows that greater severity and proximity are associated with poorer post-trauma outcomes. Included studies explored various ways in which trauma and PTSD could increase the risk of perpetration, including via problematic use of alcohol and other drugs (Creech et al., Reference Creech, Macdonald and Taft2017; Iverson et al., Reference Iverson, Sayer, Meterko, Stolzmann, Suri, Gormley, Nealon Seibert, Yan and Pogoda2020; Mannell et al., Reference Mannell, Grewal, Ahmad and Ahmad2021a). The findings in relation to the impact of substance use, particularly alcohol, are also consistent with the wider research on IPV, supporting a significant association between alcohol and increased risk of perpetration (Foran and O’Leary, Reference Foran and O’Leary2008).
Also similar to the wider literature on IPV risk factors, the review identified significant overlap between the factors that increase the risk of perpetration and those that increase the risk of victimisation. Several included studies examined the impact of conflict-related trauma and its related emotional dysregulation difficulties on both perpetration and victimisation. Two studies (Saile et al., Reference Saile, Neuner, Ertl and Catani2013; Sileo et al., Reference Sileo, Kershaw, Gilliam, Taylor, Kommajosula and Callands2021) found that trauma in women and related re-experiencing (Saile et al., Reference Saile, Neuner, Ertl and Catani2013) and attachment difficulties (Sileo et al., Reference Sileo, Kershaw, Gilliam, Taylor, Kommajosula and Callands2021) may increase vulnerability to experiencing IPV. Although the cross-sectional design of these studies means that the temporal relationship between the variables is not certain, the finding does appear consistent with the wider research on psychological trauma suggesting that experiencing one type of trauma or adverse experience increases the risk of experiencing others, and that those who experience multiple types of adversities are at the highest risk of experiencing more serious and enduring consequences (Felitti et al., Reference Felitti, Anda, Nordenberg, Williamson, Spitz, Edwards and Marks1998; Finkelhor et al., Reference Finkelhor, Ormrod and Turner2007). The included qualitative studies also provide insights into the nuances of how trauma can act as a vulnerability factor for victimisation. For example, several studies (e.g., Kelly et al., Reference Kelly, Kabanga, Cragin, Alcayna-Stevens, Haider and Vanrooyen2012; Kiconco and Nthakomwa, Reference Kiconco and Nthakomwa2018; Daoud, Reference Daoud2021) described how shame and stigma placed on women who had experienced conflict-related sexual violence can be used as a justification for further abuse perpetrated against them by partners, families and the wider community.
However, it should be noted that most of the information on trauma as a risk factor comes from relatively homogenous samples, with a disproportionate number of studies conducted with US Army veterans. This is likely to be partly a product of global research funding inequalities. However, it may also be reflective of cultural and contextual differences in how researchers from different countries tend to perceive the impact of war and armed conflict. Military personnel from high-income countries experience armed conflict differently from people who live daily with the impact of war and violence in their communities over long periods of time. This likely plays a role in the tendency of research with samples based in high-income countries such as the US, UK and Israel to consider the impact of war in terms of more individual-level problems of clinical diagnoses of PTSD (e.g., Orcutt et al., Reference Orcutt, King and King2003; Taft et al., Reference Taft, Pless, Stalans, Koenen, King and King2005; Taft et al., Reference Taft, Street, Marshall, Dowdall and Riggs2007), for example, or of ‘aggressive impulses’ (Snir et al., Reference Snir, Itzhaky and Solomon2017). On the other hand, research conducted in LMICs tended to consider the broader impacts of war and its destruction of the social and economic fabric of communities and societies, as well as its individual mental health impacts (e.g., Falb et al., Reference Falb, Annan, King, Hopkins, Kpebo and Gupta2014; Daoud, Reference Daoud2021; Al-Natour et al., Reference Al-Natour, Morris and Mohammad Al-Ostaz2022). The analysis presented in this review, therefore, highlights some of the ways in which exposure to the ongoing stress, trauma and instability of a post-conflict context, or being forced to flee a conflict-affected setting and experiencing migratory stresses (e.g., Cardoso et al., Reference Cardoso, Gupta, Shuman, Cole, Kpebo and Falb2016), differs from the experience of being exposed to conflict and then returning to high-income countries. Of the 24 quantitative studies included, the majority were based on US Army veterans and their partners. Only four quantitative studies based in Africa (Gupta et al., Reference Gupta, Reed, Kelly, Stein and Williams2012; Saile et al., Reference Saile, Neuner, Ertl and Catani2013; Sileo et al., Reference Sileo, Kershaw, Gilliam, Taylor, Kommajosula and Callands2021; Bourey et al., Reference Bourey, Musci, Bass, Glass, Matabaro and Kelly2024) that met the study inclusion criteria were identified, despite Africa being one of the most conflict-affected regions in the world. This review, therefore, indicates a need for more geographically diverse research to examine how contextual factors interact with individual-level variables.
Some relationship-level factors were identified by included studies as being significantly associated with IPV. For example, Gerlock et al. (Reference Gerlock, Szarka, Cox and Harel2016) identified ‘relationship mutuality’ as a factor that distinguished IPV perpetrators from non-perpetrators. However, it appears that there may be a possibility of some conceptual overlap between the variable of ‘relationship mutuality’ and relationship quality, which may produce a tautological analysis when used as a predictor of IPV. A similar potential problem presents in relation to the interpretation of findings by Creech et al. (Reference Creech, Macdonald and Taft2017), which identified that relationship satisfaction explained significant variance in psychological IPV. It seems that it would stand to reason that dissatisfaction would be more likely in a relationship where psychological abuse is present, and the directionality of the relationship here is unclear. Longitudinal studies are needed to understand which relationship factors may act as early predictors of IPV, and how these factors in turn may be related to conflict exposure.
The findings of this review highlight the importance of an intersectional approach to understanding and preventing violence in conflict-affected settings. Intersectionality brings a focus on the role of power relations in contributing to partner abuse, and on the relationship between structural and interpersonal forms of domination and control (Collins, Reference Collins2024). For example, some included studies (e.g., Gerlock et al., Reference Gerlock, Grimesey and Sayre2014; Jewkes et al., Reference Jewkes, Jama-Shai and Sikweyiya2017) examined how newly acquired disabilities from conflict exposure could negatively impact intimate relationships, through changing the relationship dynamic such that one partner must now act as a carer for the other. This change in power dynamics can create increased vulnerability to partner abuse. In their description of their sampling procedure, which drew on Veteran Health Administration screening centres, Iverson et al. (Reference Iverson, Sayer, Meterko, Stolzmann, Suri, Gormley, Nealon Seibert, Yan and Pogoda2020) noted that US Army personnel are routinely screened for traumatic brain injury (TBI), and that 20% screen positive. Experiences of people with different types of disabilities acquired as a result of war and armed conflict are an area that warrants further consideration in research and humanitarian programming.
The intersection between migration status and gender was also considered in many of the included studies. For example, a study by Azizi et al. (Reference Azizi, Lane and Boyce2024) highlighted how migration-related vulnerabilities, such as language barriers and a lack of knowledge about local services, can be used by perpetrators to exert greater control over victims. However, these intersections between migration and gender issues, including gender-based violence, are often under-considered in law, policy and practice (Tastsoglou and Nourpanah, Reference Tastsoglou and Nourpanah2019). Additionally, despite the broader consideration of the impacts of war and armed conflict presented in studies conducted in conflict-affected and displacement contexts, it was still uncommon for these studies to engage with the legacy of colonialism as a factor shaping the conditions for armed conflict and gendered violence to occur. All of the conflict-affected contexts considered in the studies included in the review had experienced colonial rule or imperial domination at some point in their histories. However, this history was rarely acknowledged; where colonialism was mentioned, it was primarily in a descriptive sense – providing background information to the study – rather than being explicitly theorised as a structural force relevant to understanding ongoing violence and instability. While theory-building in this area does consider structural influences, including the political and economic context (e.g., Cockburn et al., Reference Cockburn, Giles, Hyndman, Giles and Hyndman2004; True, Reference True2010) and broader dynamics such as globalisation (Murphy et al., Reference Murphy, Contreras-Urbina, Spearing and Swaine2023), it often stops short of theorising the impact of colonialism on these structures. Given the close links between colonial violence, instability, armed conflict and gendered violence (e.g., Lugones, Reference Lugones2007; Smith, Reference Smith2015; Segato and Monque, Reference Segato and Monque2021; Mannell et al., Reference Mannell, Amaama, Boodoosingh, Brown, Calderon, Cowley-Malcolm, Lowe, Motta, Shannon, Tanielu and Vergara2021b), closer engagement with these historical and structural dynamics appears important to developing a fuller understanding of how armed conflict perpetuates IPV.
Limitations
This review provides an overview of the current research evidence on the drivers of the association between armed conflict and IPV. However, it is not without limitations. Due to the fact that the majority of the included literature is cross-sectional, the directionality of the relationships explored cannot be assumed. We also acknowledge the limitations inherent in considering ‘armed conflict’ as an exposure, which fails to capture the diversity and complexities of individual experiences, and the socio-political context in which it occurs. Future research and theory-building may identify preferable ways to measure and conceptualise these experiences. Several studies were excluded from consideration from this review due to being based on samples of women of reproductive age (15–49), and not disaggregating analyses between adolescents and adult women. This may have resulted in some potentially relevant findings being overlooked. However, we propose that this also indicates a need for purpose-designed research investigating this topic to better elucidate the causal mechanisms of the relationship. The practice of only considering partner violence against women aged 15–49 obfuscates issues specifically affecting adolescents, as well as violence experienced by middle-aged and older women.
Conclusions and future perspectives
Despite the clear associations between armed conflict and IPV, recognition of this intersection in policy and practice has been relatively slow. More research is needed to explore the ways in which IPV in conflict-affected contexts can best be addressed through intervention. However, the studies included in this review also present some examples of promising practices with potential for scaling to other contexts. For example, Doyle and McWilliams (Reference Doyle and McWilliams2020) have highlighted the use of community-based restorative justice (CBRJ) schemes in Northern Ireland. These schemes involve non-violent resolution of crimes, usually through mediation, as an alternative to paramilitary involvement in communities where trust in police is low. Although these schemes to date have not usually been oriented towards IPV, there may be potential to explore a more significant role for such initiatives in IPV prevention, particularly in post-conflict contexts. As noted by Doyle and McWilliams (Reference Doyle and McWilliams2020), they may present greater opportunities for community identification, ownership, acceptability and sustainability.
In terms of future research and theory-building, studies including mediation analyses will be useful to better understand the processes by which the factors identified in this review act to increase the risk of IPV. Studies gathering data at more than one time point are also needed to clarify the temporality of the associations identified. Additionally, most included quantitative studies tended to focus on individual-level risk factors for IPV, whereas the qualitative studies tended to highlight the role of structural and social factors. However, as outlined already, and consistent with an intersectional perspective (e.g., Bowleg and Bauer, Reference Bowleg and Bauer2016; Collins, Reference Collins2024), researchers should endeavour to integrate risk factors operating at multiple levels to produce a more complete understanding of this association.
Open peer review
To view the open peer review materials for this article, please visit http://doi.org/10.1017/gmh.2026.10248.
Supplementary material
The supplementary material for this article can be found at http://doi.org/10.1017/gmh.2026.10248.
Data availability statement
As this was a systematic review, there is no data, therefore this section is not applicable.
Author contribution
All authors have made substantial contributions to the paper, including its conception, data analysis and drafting and/or revising drafts. All authors have approved the final version of the manuscript and agree to be accountable for its accuracy and the integrity of the work.
Financial support
This research was funded by Taighde Éireann – Research Ireland and the Department of Foreign Affairs under grant number NF/2023/1283.
Competing interests
The authors declare no competing interests.





 Open access
Open access
Comments
Dear Editor,
My colleagues and I submit the manuscript titled 'The mechanisms of the association between armed conflict and intimate partner violence: a systematic scoping review’ for your consideration. Although the association between armed conflict and intimate partner violence is well-established, the mechanisms of this association are less well understood. This review therefore synthesises current evidence on empirically supported drivers of the relationship. Identified mechanisms included trauma and post-traumatic stress disorder (PTSD), substance use and other mental health problems, and socio-economic factors including poverty and changing gender roles in the aftermath of conflict or displacement. Several included studies, particularly the quantitative research, focus on experiences of US army veterans returning home after involvement in conflicts overseas. There are significant concerns about the generalisability of these findings to the majority of conflict-affected regions globally, and so the need for more geographically diverse research is clear.
The manuscript is an original study. It is not under consideration elsewhere, nor has it been published elsewhere in whole, or in part, or in any other language. All authors have made a significant contribution to the preparation of the manuscript. The research holds no financial interest, or other conflicts of interest.
Best wishes,
Áine Travers