

1. Introduction
Laboratories remain foundational to engineering education. Studies document barriers to full participation in laboratory classes for students with disabilities, including lower sense of belonging, challenges with communication and difficulties engaging with practical sessions (Reference Batty and ReillyBatty, Reilly 2023). More inclusive laboratory environments require structured online support, improved laboratory design, and adaptive assessment practices (Reference Batty and ReillyBatty, Reilly 2023).
Virtual and remote laboratories have been advanced to overcome these limitations by enabling full access, removing geographic constraints, and sharing costly equipment across institutions. A recent meta-analysis of 46 studies found that virtual laboratories have a significant positive effect on engineering education outcomes, particularly for learning motivation and engagement (Reference Li and LiangLi, Liang 2024). Despite these advances, accessibility and inclusion remain uneven in current virtual-lab implementations. A recent systematic review of 36 studies concluded that accessibility features are inconsistently planned and evaluated, with gaps spanning assistive-technology integration, multilingual support, interface design, and interaction support (Reference Deriba, Saqr and TukiainenDeriba et al. 2024).
This paper conducted a needs assessment at the faculty of Mechanical Engineering at the host institution. An online survey (n = 43) and semi-structured interviews were used to identify key barriers, needs, and expectations regarding laboratory participation among students. The results empirically defined distinct target groups which will be used for the development of a VR-based framework aimed at supporting students who face limited access to laboratory sessions due to existing barriers.
2. Background and context
2.1. Students with study-impairing conditions
According to the national baseline established in the report from “German Centre for Higher Education and Science Research” (Reference Steinkühler, Beuße, Kroher, Gerdes, Schwabe and KoopmannSteinkühler et al. 2023), the proportion of students in German higher education affected by study-impairing health conditions rose from 11% in 2016/2017 to approximately 16% in 2023. Of those affected, psychological and mental-health disorders comprised about 65%. The definition explicitly spans physical and sensory impairments (e.g mobility impairments and visual or auditory loss), chronic somatic conditions (for example, diabetes or asthma), and psychological conditions, each of which has direct consequences for participation, organization, and academic success in higher education.
2.2. Needs and barriers of impaired students
Students with physical barriers encounter structural, physical, and digital obstacles in daily university life, including inaccessible buildings and non-adjustable lab benches. German Centre for Higher Education Research and Science Studies (DZHW) (Reference Steinkühler, Beuße, Kroher, Gerdes, Schwabe and KoopmannSteinkühler et al. 2023) reported that about 27% of students with impairments state concrete requirements regarding campus buildings and equipment, while roughly 56.4% of universities meet basic accessibility criteria. Specific barriers include missing ramps, unsuitable elevators, and inadequate seating in lecture halls and laboratories, as well as experiment stations and safety-relevant facilities (Reference Qiao, Chen and HouQiao et al. 2024).
Visually impaired students cannot access color-coded information, digital displays, or microscopic details without specialized support. Visual impairment manifests as reduced or absent sight, affecting the ability to perceive written materials, visual demonstrations, and quantitative data presented visually. A lack of high-contrast materials, tactile models, audio descriptions of visual phenomena, or screen-reader-ready formats leads to exclusion from learning activities. The integration of screen readers or magnification tools in digital laboratory systems remains inconsistent (Reference Maasß and RinkMaasß, Rink 2018).
Students with hearing loss require visual equivalents for audio signals, captions for video, and written transcripts for spoken instructions. Hearing loss manifests as reduced or absent auditory perception, limiting access to verbal explanations, safety briefings, and communication in group settings. Therefore, information gaps create both academic and health risks (Reference Maasß and RinkMaasß, Rink 2018).
Students with chronic somatic conditions (e.g. diabetes, asthma and other persistent physical health conditions) experience distinct barriers related to unpredictable symptom variability and fatigue. Unlike mental-health conditions characterized by psychological components, chronic somatic conditions involve physiological manifestations including pain, fatigue, and disease-related complications that fluctuate unpredictably. Studies of disabled students in German higher education reveal that chronic somatic conditions significantly impact academic engagement. Therefore, these students require accommodations such as flexible scheduling, accessible rest spaces, and the ability to manage health requirements (blood glucose monitoring, medication timing) within laboratory timeframes (Reference BartzBartz 2020).
Students with psychological and mental-health conditions (including depression, anxiety, and post-traumatic stress disorder) frequently experience concentration difficulties, reduced motivation, social withdrawal, and fluctuating day-to-day symptom severity. These challenges conflict with rigid lab schedules and high workloads in engineering courses. Such structural features can exacerbate mental health symptoms and reduce participation opportunities for affected students (Reference Solís García, Real Castelao and Barreiro-CollazoSolís García et al. 2024).
Neurodivergent students benefit from predictable, structured procedures, whereas unclear instructions or abrupt process changes can trigger stress and hinder participation (Reference Le Cunff, Glover, Martis, Giampietro and DommettLe Cunff et al. 2024). Autistic students often face sensory overload from bright lighting, noise, simultaneous demands across multiple sensory inputs (visual, auditory, tactile), sometimes accompanied by physical symptoms such as migraines or dizziness.
Students with ADHD may struggle in settings with long, unstructured instructions and distracting environments (Reference Nolan, Doyle, Lewis and TreanorNolan et al. 2023).
Students with neurological conditions such as epilepsy can be adversely affected by flicker and certain visual stimuli in digital or virtual laboratories. Safer delivery methods include flicker-reduced displays with refresh rates of 100 Hz or higher and moderated contrast to minimize seizure risk (Reference Kasteleijn-Nolst Trenité, Acharya, Baumer, Beran, Craiu and FrenchKasteleijn-Nolst Trenité et al. 2025).
Care responsibilities and family duties (caring for ill, elderly or young family members) create time conflicts regarding attendance and studies, leading to extended study duration, transitions to part-time study, or study interruptions (Reference Steinkühler, Beuße, Kroher, Gerdes, Schwabe and KoopmannSteinkühler et al. 2023). Insufficient childcare options and limited family-friendly assessment policies exacerbate scheduling and participation challenges for students with dependent children or regular caregiving duties. The core task is not to adapt individuals to fixed structures but to adjust assessment timing, attendance requirements, and workload distribution so that participation remains feasible when students have other significant commitments (Reference RawlinsonRawlinson 2024).
Consequences across these barriers include disproportionate organizational effort, withdraw from courses or laboratory activities they cannot access under current conditions, and lower study-completion rates (for example, about 49.5% completion within six years for students with recognized disabilities versus about 68% without) (Reference Steinkühler, Beuße, Kroher, Gerdes, Schwabe and KoopmannSteinkühler et al. 2023).
2.3. Applicability of needs and barriers on laboratories
Most barriers reported by students with study-impairing conditions do not arise from laboratories themselves but from general participation requirements at university level. This includes access to buildings, usable elevators, clear campus navigation, rest and quiet rooms, predictable accommodation procedures and family-friendly scheduling (Reference Steinkühler, Beuße, Kroher, Gerdes, Schwabe and KoopmannSteinkühler et al. 2023). Such measures also help students attend laboratories, but they are not designed specifically for labs. The same applies to care and childcare duties. These obligations limit the time windows in which students can be present on campus, but the barrier is organizational, not laboratory-specific (Reference RawlinsonRawlinson 2024).
A smaller group of barriers is directly linked to laboratory formats in engineering and science. These barriers occur when benches, experiment stations or safety equipment cannot be adjusted, when participation is tied to a fixed time slot, when safety instructions are only spoken and not available in writing, or when experimental results are presented only in one sensory channel (Reference Maasß and RinkMaasß, Rink 2018, Reference Maasß and Rink2018). For students with visual or hearing impairments this immediately reduces access. For students with chronic or psychological conditions the main problem is the high and inflexible workload during one laboratory session, not the campus building.
2.4. Current state of the host institution
The host institution provides disability support services through student counseling, including guidance on reasonable accommodations and campus accessibility, alongside awareness-raising initiatives for teaching staff. However, accommodation processes remain individualized through case-by-case negotiations, creating uncertainty and administrative workload, while information is distributed across multiple departments without consolidated procedures. The university does not systematically collect data on accommodations, inclusion measures, or students with disabilities, hindering targeted development of support strategies for laboratory-based education.
The (physics) laboratories feature traditional workstations with real experimental equipment, though only few stations provide assistive functions such as screen magnification. Key constraints include fixed scheduling that prevents flexible repetition or pause-continue functionality, absence of systematic provision of scalable visual elements or stepwise guidance, and complete absence of remotely accessible experiment variants.
2.5. Remote laboratories
Remote laboratories (comprising conceptual simulations, fully virtual laboratories, and remote access to physical equipment via web interfaces) achieve learning outcomes comparable to traditional laboratories when properly designed (Reference Li and LiangLi, Liang 2024) and extend access to practical engineering education for students with disabilities. For general needs, including institutional barriers, remote participation provides an indirect solution. It allows students to work in accessible environments and to align laboratory activities with fluctuating health or caregiving duties, provided that such participation is recognised as equivalent to regular attendance. For laboratory-specific barriers, remote access helps only if the digital laboratory is designed accessibly. Otherwise, the barrier is transferred from the building to the user interface. In digital and remote delivery, web accessibility therefore becomes a necessary condition. Typical problems in current learning and laboratory platforms are missing captions and transcripts for video or audio content, images without alternative text, form fields that cannot be reached by keyboard, and visual elements whose text-to-background contrast is too low for users with low vision (for example light-grey text on a white background that does not meet WCAG 2.1 level AA requirements) (Reference Ifenatuora, Awoyemi and AtobateleIfenatuora et al. 2023). In such cases, remote laboratories do not improve access for the very groups they are intended to support. The accessible implementation of the whole digital chain (Learn Management Systems, remote-lab interface, visualization and assessment) is therefore a prerequisite.
3. Methodology
A mixed-methods design was employed to identify barriers, needs and expectations for inclusive participation in laboratory courses at the Faculty of Mechanical Engineering at the host institution. The paper collected quantitative data through an online survey and qualitative data through guideline-based interviews. This approach enabled cross-validation between quantitative findings (indicative frequencies and patterns) and qualitative insights (contextual understanding and mechanisms), providing complementary evidence.
This paper defines students with study-impairing conditions as students who themselves perceive a health condition as hindering their studies, including undiagnosed or self-identified states. The target group also included significant family responsibilities (dependent children, caregiving). Financial and employment burdens as well as language barriers were not examined. Considering the work situation, the assumption was full-time enrolment with only minor employment. Institutional admission requirements of at least C1 language proficiency excluded basic language difficulties from the analysis.
An online survey was developed in LimeSurvey, a web-based survey platform, and distributed via the faculty-wide email list to all students and staff. The survey employed adaptive display logic, presenting impairment-specific follow-up questions only when respondents indicated relevant conditions or barriers. The survey comprised three item formats, including closed, semi-open, and open-ended questions. It addressed four main content areas, such as demographics, impairments/barriers, support awareness/use, and technical/didactic requirements for remote labs. Data collection occurred over two weeks in Mai 2025, with one reminder email sent after one week to increase response rate. The sampling frame was open to all registered students and staff (approximately 800 individuals). A total of 43 valid responses were received, yielding a response rate of approximately 5%. No incentives were offered. Given the low response rate and self-selection inherent to voluntary online participation, survey results are reported as descriptive frequencies and percentages without claims of representativeness. The respondent sample likely comprises primarily affected students, yet the proportion of study-impairing conditions within the broader student population remains unknown, therefore these findings serve as indicative of participant perspectives rather than representative of the faculty’s student body. Instead, survey findings are interpreted as indicative of participant perspectives and are triangulated with interview data to strengthen evidence and mitigate potential biases from individual sub-groups.
Guideline-based semi-structured interviews were conducted in parallel with the survey to explore barriers, support mechanisms, and perspectives in depth. Two interview guide variants were developed for different participant groups. One was for students with study-impairing conditions while the other was for staff or lecturers without personal impairment but teaching affected students. Interviews were conducted primarily in person on campus, with supplementary data collection via telephone or email when necessary. To protect participant privacy, no audio recordings were made and interviewers maintained structured notes, which were subsequently anonymized and coded.
Survey data were analyzed using descriptive statistics from LimeSurvey’s built-in analytical functions, reporting absolute frequencies and percentage distributions. Interview notes were analyzed through a combined deductive-inductive coding approach. Deductive codes were derived from the research questions and theoretical framework, while inductive subcategories emerged from repeated reading of the interview material.
Recruitment and methodological limitations should be noted. The survey was available in German only and was internally tested for technical functionality, but no formal accessibility audit was conducted. No accessibility-related problems were reported, however accessibility barriers to participation cannot be excluded. Because the survey was anonymous and interviewees were not asked whether they completed the survey, overlap between survey and interview participants cannot be determined. No formal ethics committee or IRB review was obtained for this study.
4. Results
4.1. Survey results
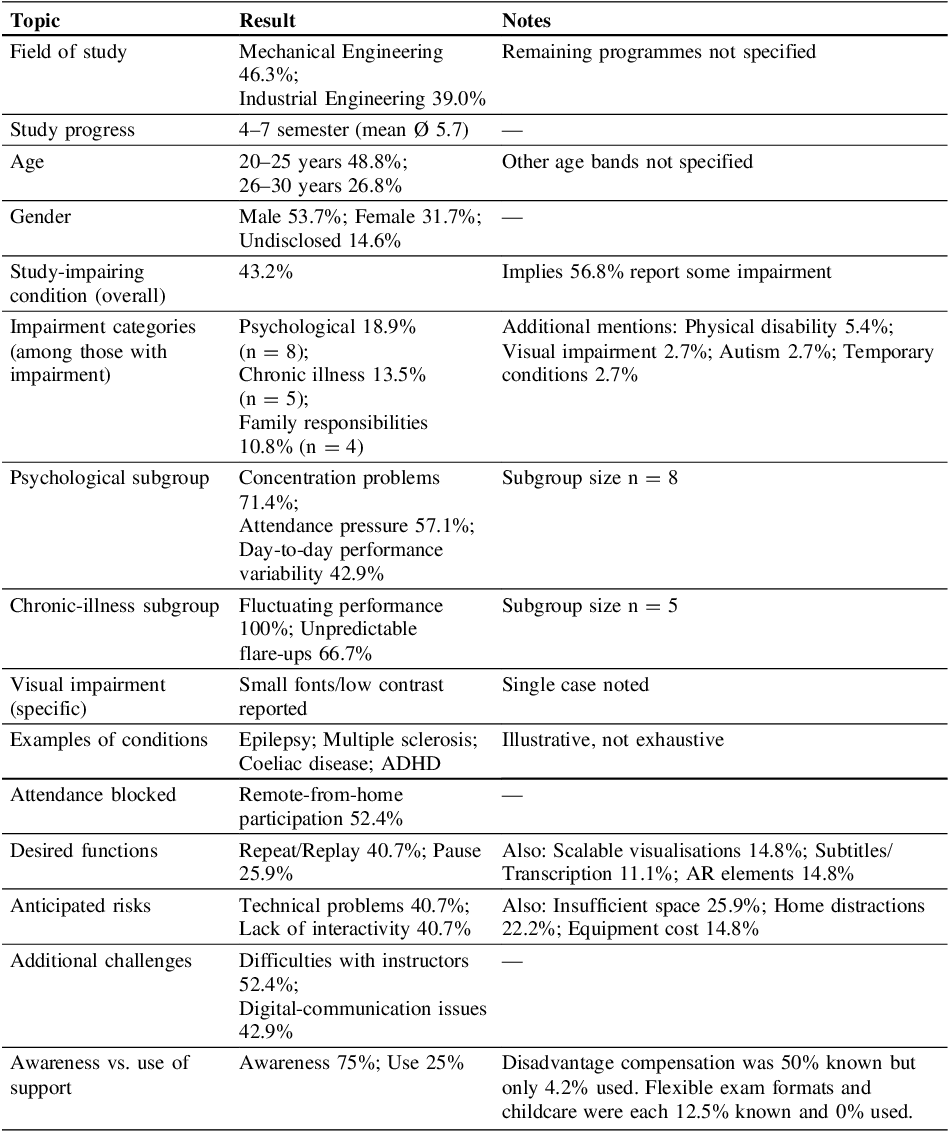
The core findings of this survey are presented in the following (Table 1).
Survey results

Table 1 Long description
The table presents survey results on study impairments and desired functions. It has 15 rows and 3 columns. The columns are labeled Topic, Result, and Notes. The table covers various topics such as field of study, study progress, age, gender, study-impairing conditions, impairment categories, psychological subgroup, chronic-illness subgroup, visual impairment specifics, examples of conditions, attendance blocked, desired functions, anticipated risks, additional challenges, and awareness versus use of support. Each row provides specific results and notes related to these topics. For example, the field of study shows Mechanical Engineering at 46.3 percent and Industrial Engineering at 39.0 percent. Study progress is between 4 and 7 semesters with a mean of 5.7. Age groups are 20 to 25 years at 48.8 percent and 26 to 30 years at 26.8 percent. Gender distribution is Male at 53.7 percent, Female at 31.7 percent, and Undisclosed at 14.6 percent. Study-impairing conditions affect 43.2 percent overall, with psychological impairments at 18.9 percent, chronic illness at 13.5 percent, and family responsibilities at 10.8 percent. The psychological subgroup reports concentration problems at 71.4 percent, attendance pressure at 57.1 percent, and day-to-day performance variability at 42.9 percent. The chronic-illness subgroup reports fluctuating performance at 100 percent and unpredictable flare-ups at 66.7 percent. Visual impairment specifics mention small fonts and low contrast. Examples of conditions include epilepsy, multiple sclerosis, coeliac disease, and ADHD. Attendance is blocked for remote-from-home participation at 52.4 percent. Desired functions include repeat/replay at 40.7 percent and pause at 25.9 percent. Anticipated risks are technical problems and lack of interactivity, each at 40.7 percent. Additional challenges include difficulties with instructors at 52.4 percent and digital-communication issues at 42.9 percent. Awareness of support is at 75 percent, while use is at 25 percent.
4.2. Interview data: presentation and coding
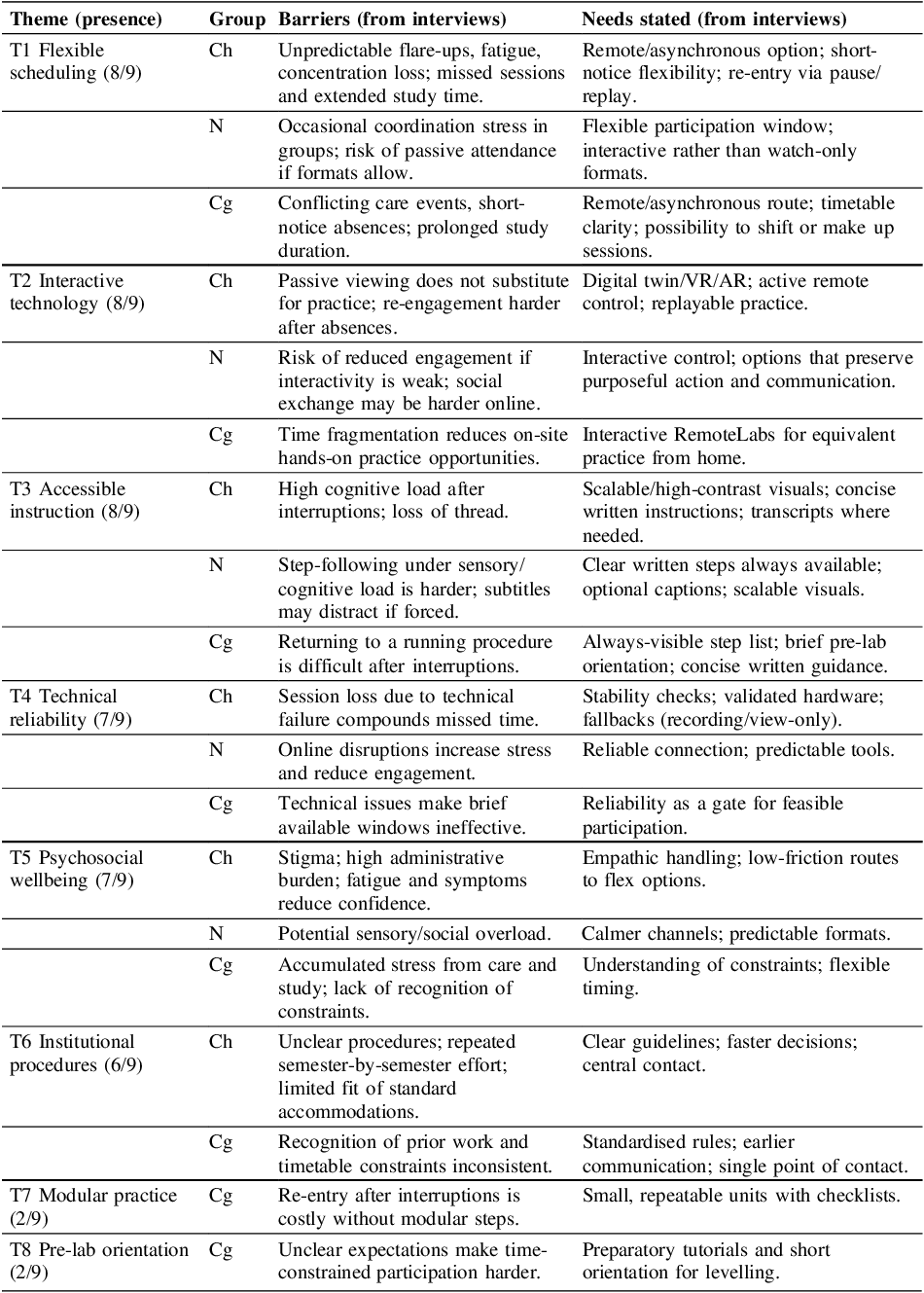
The main themes summarized from the nine interviews are presented in the following (Table 2). The sample comprised five members of teaching or administrative staff and four students with study-impairing conditions, namely two with chronic somatic illness, one with autism, and one with caregiving responsibilities. Each theme is shown with the number of interviews in which it occurred (presence), and a concise core finding. To make group differences explicit, coding participants occurred as follows: St (n=5) = staff/lecturers/administrators, Ch (n=2) = students with chronic or physical impairments, N (n=1) = students with neurodivergence (e.g., autism), and Cg (n=1) = students with caregiving responsibilities. Numbers in parentheses after each core finding indicate how many participants within each code raised the issue over the number of participants in that code.
Interview results

4.3. Derived needs and functions
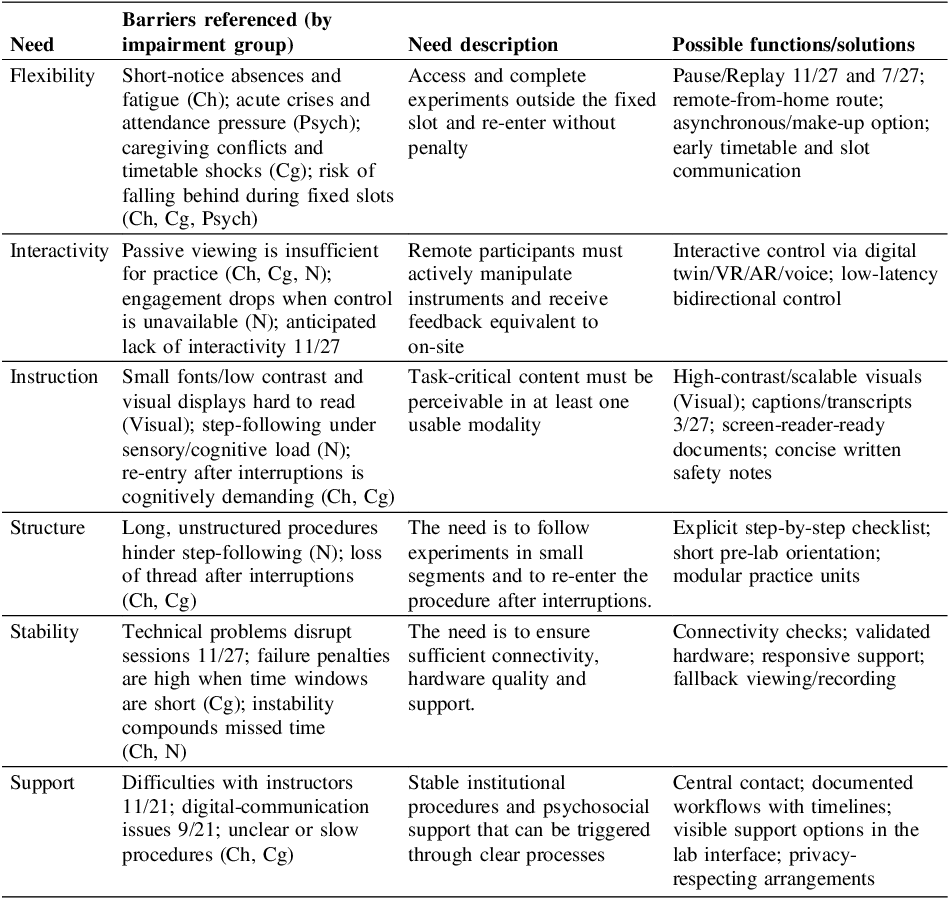
The following (Table 3) summarizes the user-needs identified from the updated survey and interview data. Each need is expressed as a problem that users must overcome. The functions listed are examples of features that could satisfy the need and are annotated with the number of participants who mentioned them in the survey (“XX/43”) or in interviews (“YY/9”).
Barriers, derived needs and related possible functions

4.4. Results analysis
Evidence was drawn from the survey and from non-staff interviews. For each need × impairment group, two counts were formed:
-
• Survey positives: the number of survey respondents in the group who endorsed at least one survey item mapped to that need (i.e., selected “Yes” on any mapped item).
-
• Interview positives (non-staff): the number of interviewees in the group who raised a theme mapped to that need.
The denominator for each cell equals the total group size: all survey respondents in that impairment group plus all non-staff interviewees in the same group. Staff statements were not included in these calculations because they are not tied to specific impairment groups, they are considered qualitatively in the Discussion.
For each cell, the percentage is computed as (survey positives + interview positives) ÷ total group sizeAcknowledgement.
5. Discussion
Two coherent patterns emerged from the data (see Table 4). First, Flexibility and Support appeared at saturation across all groups and were consistently described in interviews as enabling conditions that must precede any further adaptation. Staff interviews emphasized flexible routes, predictable procedures, and rapid centralized responses. Second, the remaining barriers and needs formed two distinct profiles representing target user populations for RemoteLabs development.
The voluntary, self-reported design and the low response rate imply potential selection effects. The data describe participant perspectives rather than population prevalence. In addition, because no formal accessibility audit of the survey was conducted, accessibility-related non participation cannot be ruled out.
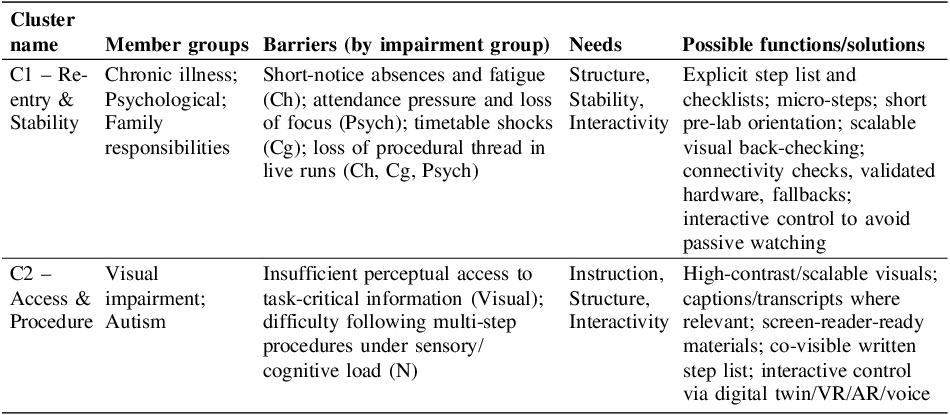
Resulting clusters

Cluster C1 (31.9% of respondents) - Re-entry and continuity under fluctuation aggregates chronic illness, psychological conditions and caregiving. The dominant barriers are short-notice absences, fatigue, and loss of procedural thread in fixed, high-intensity sessions. The corresponding needs are modular procedure architecture, dependable Stability and sufficient Interactivity to maintain equivalence when learning remotely. Possible solutions for the needs of this cluster are to be found in Table 4. Student interviews report these barriers and needs directly for chronic illness and caregiving, with psychological load reflected in free-text survey items and subgroup indicators on concentration problems and attendance pressure. Staff describe the same gate conditions and ask for clearer rules and a central contact, consistent with the Support prerequisite.
Cluster C2 (6.4% of respondents) - Perceptual access and explicit procedure guidance groups visual impairment and autism. The dominant barriers are insufficient perceptual access to task-critical information and the difficulty of following multi-step procedures under sensory or cognitive load. The needs are accessible Instruction, explicit Structure and sufficient interactivity to act rather than watch. Possible solutions for the needs of this cluster are listed in Table 4. Student interviews capture the step-following and sensory load issues; the survey shows visual-access problems and endorsements of scalable visuals. Staff describe the same access features as necessary in practice.
The structure aligns with the theoretical model. Section 2.2 identifies that sensory impairments require perceivable, redundant representations and that neurodivergent students benefit from predictable, step-wise procedures. The same section notes fluctuating symptoms and fatigue in chronic conditions and structural time conflicts in caregiving. Section 2.3 specifies that laboratory barriers become acute when procedures are tied to a single sensory channel or to one fixed timeslot, whereas many obstacles are organizational at the university level. The clusters, prerequisites and solutions therefore reflect the expected access logic for laboratories and the wider institutional context.
Interpretation must account for small-n effects. Visual impairment is represented by one survey respondent, which yields 100 percent cells for any endorsement, restricting generalisability for this subgroup. Auditory and temporary impairments are non-expressive due to routing and case numbers. The physical subgroup shows zero endorsements in the mapped survey items, and interview statements originally labelled “physical” were consolidated under chronic illness by design, which removes interview positives from the physical row. Several mobility-specific on-site barriers (bench adjustability, reachability) are not fully captured by the remote-delivery focus of the instrument and likely align with the access logic of C2 when represented. Staff material indicates that standardizing procedures and improving building access and equipment have already required institutional action, further supporting the prerequisite status of support and the access profile of C2.
For RemoteLabs, flexibility and support should be implemented as enablers. Under these prerequisits, C1 benefits from stability checks, fallback mechanisms, interactive control and modular procedure architecture to permit rapid re-entry, while C2 requires accessible instruction and explicit procedure guidance by default, again with interactive control to maintain equivalence with on-site manipulation. The baseline group without declared impairments shows needs that align with C1 (for example, clear procedures and reliable continuity), which suggests universal-design transfer and supports implementation as standard practice rather than case-by-case accommodation.
These two empirically derived Clusters serve as personas that direct systematic, evidence based development of RemoteLabs functionality toward these specific user populations, while highlighting where further targeted sampling is needed.
Beyond the target groups, the proposed measures also benefit the baseline group by reducing procedural ambiguity, preventing avoidable errors, and improving continuity when students miss steps or sessions. For teaching staff, the cluster-based framing supports a shift from case-by-case negotiations toward standardised participation pathways and clearer communication rules, thereby reducing recurring coordination effort. The operational feasibility of extended flexibility (e.g., whether it necessitates more asynchronous supervision or partial automation of submissions and feedback) is an important topic for future RemoteLabs iterations and evaluation.
6. Conclusion
Inclusive remote laboratories require two non-negotiable enablers: Flexibility to provide equivalent participation and re-entry, and support to activate accommodations through predictable procedures. With these gates in place, two stable profiles emerge. C1 Re-entry & Stability addresses fluctuation and interruption through stepwise structure, reliable delivery, and interactive control. C2 Access & Procedure secures perceptual access and explicit procedural guidance for sensory and neurocognitive needs. This barrier-to-need-to-solution mapping aligns with the theoretical model for laboratory learning and with universal-design principles, and it also benefits the baseline group. Interpretation is constrained by small sample sizes in sensory and mobility subgroups. The results nonetheless provide a reproducible basis for implementation: guarantee the gates, then deploy C1 features to stabilize continuity and C2 features to ensure perceivable, structured instruction. Future work should enlarge the sensory and mobility samples, capture respondent-level joint distributions, and validate the profiles with model-based clustering.
Acknowledgement
The authors express their gratitude to the Volkswagenstiftung, for funding the RemoteLabs-project (Az. 9E481).

 Open access
Open access