


Impact statement
Harmful alcohol use remains a leading determinant of suffering and treatment gaps in mental health within low- and middle-income contexts. This study reports the first validated Tanzanian-Swahili version of the Brief Intervention Adherence Scale (BAS), a culturally adapted instrument rigorously evaluated through exploratory structural equation modeling (ESEM) and confirmatory factor analysis (CFA), demonstrating valid internal consistency. By providing a reliable and accessible tool to assess healthcare providers’ fidelity to brief interventions (BIs), we enable program managers, public health agencies and researchers to identify and address training gaps in harm-reduction practices, promoting uniform standards of care; enhance clinical quality through objective adherence metrics, facilitating evidence-informed decision-making; and strengthen local capacity to evaluate and optimize interventions at clinic, community and policy levels. Given that Swahili serves as an official language across multiple East African countries, this scale holds strong potential for regional implementation, fostering cross-sectoral training networks (health, education and social welfare) and contributing to emerging paradigms in Global Mental Health that prioritize contextual data, equitable access and collaborative partnerships. Widespread adoption of the BAS will strengthen advocacy efforts to expand both coverage and quality of mental health interventions, reduce treatment disparities and reinforce care systems by delivering impact at local, national and international scales.
Introduction
Harmful alcohol use accounts for several adverse health outcomes and is a leading risk factor for mortality and morbidity. Worldwide, it causes over 3.3 million alcohol-related deaths annually, of which ~1.78 million are direct results of alcohol use (GBD 2016 Alcohol Collaborators 2018; GBD 2020 Alcohol Collaborators 2022). Hazardous alcohol use is closely related to various diseases, such as human immunodeficiency virus (Goma et al., Reference Goma, Ng’ambi and Zyambo2024), ophthalmological changes (Spoorthy et al., Reference Spoorthy, Malathesh, Janti, Tekupalli, Donthu, Toomukuntla and Tikka2025) and dementia (Topiwala et al., Reference Topiwala, Levey, Zhou, Deak, Adhikari, Ebmeier, Bell, Burgess, Nichols, Gaziano, Stein and Gelenter2025), and injury, which is considered a grave public health problem. However, there is a lack of effective surveillance systems and evidence-based policy to restrict harmful and hazardous alcohol use (Morojele et al., Reference Morojele, Dumbili, Obot and Parry2021; GBD 2020 Alcohol Collaborators 2022). In Africa, the situation is no better. Injuries are responsible for most of the alcohol-related disability-adjusted life-years on the continent (Lim et al., Reference Lim, Vos, Flaxman, Danaei, Shibuya, Adair-Rohani, Amann, Anderson, Andrews, Aryee, Atkinson, Bacchus, Bahalim, Balakrishnan, Balmes, Barker-Collo, Baxter, Bell, Blore, Blyth, Bonner, Borges, Bourne, Boussinesq, Brauer, Brooks, Bruce, Brunekreef, Bryan-Hancock, Bucello, Buchbinder, Bull, Burnett, Byers, Calabria, Carapetis, Carnahan, Chafe, Charlson, Chen, Chen, Cheng, Child, Cohen, Colson, Cowie, Darby, Darling, Davis, Degenhardt, Dentener, Des Jarlais, Devries, Dherani, Ding, Dorsey, Driscoll, Edmond, Ali, Engell, Erwin, Fahimi, Falder, Farzadfar, Ferrari, Finucane, Flaxman, Fowkes, Freedman, Freeman, Gakidou, Ghosh, Giovannucci, Gmel, Graham, Grainger, Grant, Gunnell, Gutierrez, Hall, Hoek, Hogan, Hosgood, Hoy, Hu, Hubbell, Hutchings, Ibeanusi, Jacklyn, Jasrasaria, Jonas, Kan, Kanis, Kassebaum, Kawakami, Khang, Khatibzadeh, Khoo, Kok, Laden, Lalloo, Lan, Lathlean, Leasher, Leigh, Li, Lin, Lipshultz, London, Lozano, Lu, Mak, Malekzadeh, Mallinger, Marcenes, March, Marks, Martin, McGale, McGrath, Mehta, Mensah, Merriman, Micha, Michaud, Mishra, Mohd Hanafiah, Mokdad, Morawska, Mozaffarian, Murphy, Naghavi, Neal, Nelson, Nolla, Norman, Olives, Omer, Orchard, Osborne, Ostro, Page, Pandey, Parry, Passmore, Patra, Pearce, Pelizzari, Petzold, Phillips, Pope, Pope, Powles, Rao, Razavi, Rehfuess, Rehm, Ritz, Rivara, Roberts, Robinson, Rodriguez-Portales, Romieu, Room, Rosenfeld, Roy, Rushton, Salomon, Sampson, Sanchez-Riera, Sanman, Sapkota, Seedat, Shi, Shield, Shivakoti, Singh, Sleet, Smith, Smith, Stapelberg, Steenland, Stöckl, Stovner, Straif, Straney, Thurston, Tran, Van Dingenen, van Donkelaar, Veerman, Vijayakumar, Weintraub, Weissman, White, Whiteford, Wiersma, Wilkinson, Williams, Williams, Wilson, Woolf, Yip, Zielinski, Lopez, Murray, Ezzati, AlMazroa and Memish2012; GBD 2020 Alcohol Collaborators 2022). There is especially high per capita alcohol use in sub-Saharan Africa (Rehm et al., Reference Rehm, Rehn, Room, Monteiro, Gmel, Jernigan and Frick2003; Morojele et al., Reference Morojele, Dumbili, Obot and Parry2021). At Kilimanjaro Christian Medical Centre (KCMC) at Moshi, Tanzania, around 23% of trauma patients presenting to the Emergency Department (ED) were found to have alcohol-related injuries (Zimmerman et al., Reference Zimmerman, Barcenas, Pesambili, Sakita, Mallya, Vissoci, Park, Mmbaga, Bettger and Staton2022). Age and gender are associated with higher consumption of alcohol in injury patients in Tanzania, as well as with alcohol-related consequences. The early age of first drink raises the risk of consequences and alcohol-related problems (Staton et al., Reference Staton, Zhao, Ginalis, Hirshon, Sakita, Swahn, Mmbaga and Nickenig Vissoci2020).
Brief intervention impact on alcohol use
Studies in high-income countries (HICs) have shown that BI conducted by healthcare providers can reduce the hazardous alcohol use and change drinking patterns of harmful alcohol users seeking care at EDs (D’Onofrio et al., Reference D’Onofrio, Pantalon, Degutis, Fiellin and O’connor2005, Reference D’Onofrio, Fiellin, Pantalon, Chawarski, Owens, Degutis, Busch, Bernstein and O’Connor2012). BI contains four steps: raising the subject of alcohol, providing feedback, enhancing motivation for change and negotiation and advising (D’Onofrio et al., Reference D’Onofrio, Pantalon, Degutis, Fiellin and O’connor2005, Reference D’Onofrio, Fiellin, Pantalon, Chawarski, Owens, Degutis, Busch, Bernstein and O’Connor2012). It is a 15-min conversational process led by healthcare practitioners to discuss safe drinking behavior and negotiation of changes in alcohol use. Numerous meta-analyses have documented this effect for both primary care and ED settings (O’Donnell et al., Reference O’Donnell, Anderson, Newbury-Birch, Schulte, Schmidt, Reimer and Kaner2014; Barata et al., Reference Barata, Shandro, Montgomery, Polansky, Sachs, Duber, Weaver, Heins, Owen, Josephson and Macias-Konstantopoulos2017; Joseph and Basu, Reference Joseph and Basu2017; Staton et al., Reference Staton, Vissoci, El-Gabri, Adewumi, Concepcion, Elliott, Evans, Galson, Pate, Reynolds, Sanchez, Sutton, Yuan, Pauley, Andrade, Von Isenberg, Ye and Gerardo2022a). While a recent pragmatic trial, the Screening and Intervention Programme for Sensible drinking in Emergency Departments (SIPS-ED) trial, showed minimal to no reduction in alcohol use, many suggest this was due to poor intervention fidelity (Drummond et al., Reference Drummond, Deluca, Coulton, Bland, Cassidy, Crawford, Dale, Gilvarry, Godfrey, Heather, McGovern, Myles, Newbury-Birch, Oyefeso, Parrott, Patton, Perryman, Phillips, Shepherd, Touquet and Kaner2014; Heather, Reference Heather2014).
BI protocol adherence by providers
There is a gap in approaches to support the fidelity of BI. One approach is to use a fidelity assessment to evaluate providers’ adherence to the protocol and offer constructive feedback. The BI adherence scale (BAS) was designed to evaluate the degree to which healthcare providers adhere to the BI protocol. The BAS comprises 21 items that are consistent with the components of the BI protocol and has demonstrated reliability and validity in the United States. This scale is useful to provide feedback to healthcare practitioners on their performance in negotiating for the reduction of hazardous alcohol use (Pantalon et al., Reference Pantalon, Martino, Dziura, Li, Owens, Fiellin, O’Connor and D’Onofrio2012). Despite the relevance of BI as an intervention to reduce alcohol-related harms, there are few initiatives to assess the protocol adherence to BI in LMICs (Staton et al., Reference Staton, Vissoci, El-Gabri, Adewumi, Concepcion, Elliott, Evans, Galson, Pate, Reynolds, Sanchez, Sutton, Yuan, Pauley, Andrade, Von Isenberg, Ye and Gerardo2022a). As part of the efforts to adapt and propose a nurse-delivered BI to be applied with ED patients in Tanzania, the Punguza Pombe Kwa Afya Yako (PPKAY, “Reduce Alcohol for Your Health”), we undertook the adaptation and translation of the BAS to Swahili and the Tanzanian culture (Staton et al., Reference Staton, Zadey, O’Leary, Phillips, Minja, Swahn, Hirshon, Boshe, Sakita, Vissoci and Mmbaga2022b). Therefore, our study evaluated the psychometric properties of the Tanzanian-Swahili version of BAS adapted to Tanzanian culture as a part of the PPKAY intervention.
Methods
Study design
The study adopted a mixed-methods approach to evaluate the psychometric properties of an instrument to measure the adherence of healthcare practitioners to the PPKAY protocol, conducted among patients with harmful alcohol use presenting for care at KCMC in Moshi, Tanzania.
Study settings
Tanzania is the most populous country in eastern Africa, with a population of ~57.7 million people. Tanzania’s 945,500 km2 territory is divided into 31 regions, with Kilimanjaro being the largest one, in northern Tanzania. Moshi is the capital of the Kilimanjaro region. Its urban area has a population of over 180,000, while the larger Moshi area is home to ~466,000 people (Tanzania National Bureau of Statistics, 2023). Forty-seven percent of the population identify as lifetime alcohol abstainers, while ~20% of the population admit to heavy periodic drinking (Morojele et al., Reference Morojele, Dumbili, Obot and Parry2021). Overall, the amount of alcohol consumed per capita in Tanzania has increased in recent years (GBD 2020 Alcohol Collaborators 2022).
KCMC is the third-largest hospital in the country, serving as the zonal referral center and regional training center for all types of healthcare workers located in northeastern Tanzania. KCMC is a tertiary referral hospital serving over 15 million people. Annually, KCMC ED sees about 1,500 patients who suffer injuries, of whom ~23% have consumed alcohol before their injury (Zimmerman et al., Reference Zimmerman, Barcenas, Pesambili, Sakita, Mallya, Vissoci, Park, Mmbaga, Bettger and Staton2022). Alcohol use has been associated with a fivefold increase in the odds of injury, and appears to have a dose-dependent effect on the odds of injury and violence at KCMC in Tanzania (Staton et al., Reference Staton, Vissoci, Toomey, Abdelgadir, Chou, Haglund, Mmbaga, Mvungi and Swahn2018a).
Overview of the BAS
The BAS was developed to assess the degree to which health care professionals could practice BI components, which consist of identifying and enhancing motivation for change, negotiating, advising, and providing feedback on alcohol use (Pantalon et al., Reference Pantalon, Martino, Dziura, Li, Owens, Fiellin, O’Connor and D’Onofrio2012). The scale consists of 21 dichotomous questions, with 1 coded for ‘Performed’ and 0 for ‘Not performed’. The overall score ranges from 0 to 21, and a higher score on the BAS is related to a higher degree of adherence. In the development evaluation, the BAS internal structure evaluation suggested a two-factor model with eight items grouped by: (I) patient-centered discussion of alcohol use and (II) identifying motives and plans for change.
Translation and adaptation
The translation and cross-cultural adaptation of BAS was supervised by a committee of five judges (physicians, nurses and research assistants). We used the ADAPT protocol (Staton et al., Reference Staton, Zimmerman, Pesambili, Phillips, Tupetz, de Souza, Boshe, Pantalon, Swahn, Mmbaga and Nickenig Vissoci2025a) to increase rigor and guarantee reproducibility of the cross-cultural adaptation of BAS, as part of a pragmatic randomized adaptive clinical trial (Staton et al., Reference Staton, Minja, de Souza, Gallis, Santos, Buono, Sakita, Ngowi, Boshe, Phillips, Vissoci and Mmbaga2025b).
The instrument was translated through the ‘back-translation’ method (Maneesriwongul and Dixon, Reference Maneesriwongul and Dixon2004). First, a Swahili translator was hired to translate the English version of BAS into a Swahili version. Second, another translator translated the Swahili version back into English. Then, four bilingual research nurses compared the English translated version with the original English version of the instrument to check for inconsistencies. Questions with semantics were discussed, and revisions or additions were made after the evaluation of the health care practitioners in focus groups and the supervision of the judges’ committee.
As core questions, the professionals were asked “What do you think about this intervention; do you think it will be successful?,” “Where do you think patients should follow up after this intervention?” and “Is there any question that you think needs to be changed or adapted to be easier to understand?.” Those questions were asked to gather perceptions about the need for a BI Adherence Scale in the clinical setting, as well as how the scale items reflected the culture of Tanzania, including the healthcare structure and proneness to engage in educational processes.
Participants and data collection procedures
After written informed consent was obtained, we enrolled healthcare professionals trained as counselors at KCMC to receive training on the PPKAY protocol as the participants. Training was led by the principal investigator; each healthcare provider conducted PPKAY sessions and observed and evaluated each other. The healthcare providers then evaluated mock sessions facilitated by healthcare providers with experience in BIs. The mock sessions consisted of a healthcare provider with experience in BIs role-playing as the provider, applying the PPKAY protocol to a research team member role-playing as the patient receiving the intervention. Each participant evaluated up to four mock BI sessions.
Following the training activities, participants completed a self-administered questionnaire capturing sociodemographic information about age, sex, occupation, work experience and alcohol consumption. Questionnaires and BAS were then gathered by research staff; analysts remained blinded to participant identities. All completed forms were entered manually into an internet-based dataset (Research Eletronic Data Capture - REDCap) (Harris et al., Reference Harris, Taylor, Thielke, Payne, Gonzalez and Conde2009).
Data analysis
Sociodemographic data were presented as means and standard deviations or frequencies. In this adaptation to Tanzania and Swahili, we evaluated the adequacy of the proposed two-factor solution, but also explored the underlying latent structure of all the proposed items. Since we are adapting this instrument to a new language and context, we want to evaluate if a different solution would also adequately fit the data. All analyses were conducted with the R Language for Statistical Computing (R Core Team, 2013), using the lavaan package (Rosseel et al., Reference Rosseel, Jorgensen and Wilde2024).
Factor structure
To assess the construct validity of the BAS scale, we used an ESEM on all the adapted BAS items, and an approach based on CFA on the prespecified eight-item, two-factor model. The factor structure of BAS was displayed in graphs.
Initial inspection of the eigenvalues through the scree plot and parallel analysis was conducted, and suggested a three-factor model was the best fit to the data. We then conducted an ESEM approach using the efa function from the Lavaan (Rosseel et al., Reference Rosseel, Jorgensen and Wilde2024) package in the software R Language for Statistical Computing, testing the three-factor solution. This approach used the Geomin Oblique rotation method. In sequence, a CFA was used to test two-factor models spanning from the original BAS development study with the original eight items. The ESEM model, considering three factors, evaluated three theoretically defined dimensions of providing feedback on alcohol use, enhancing motivation for change, as well as negotiating and offering advice. The second model, analyzing two factors, reproduced Pantalon et al.’s study to assess two dimensions of patient-centered discussion of alcohol use and identifying motives and plans for change (Pantalon et al., Reference Pantalon, Martino, Dziura, Li, Owens, Fiellin, O’Connor and D’Onofrio2012).
ESEM and CFA models were fitted using weighted least squares means and variance adjusted. Model fitness was evaluated by fit indices: chi-square (χ 2 and p-value), root mean square error of approximation (RMSEA), Tucker–Lewis index (TLI) and comparative fit index (CFI). These indices aim to assess whether the model is a good fit for the data (Bentler and Bonett, Reference Bentler and Bonett1980; Hu and Bentler, Reference Hu and Bentler1999). Average variance extracted was calculated to assess convergent validity, for which a value over 0.50 is considered acceptable.
Reliability
Reliability refers to the capacity of an instrument to evaluate the same construct regardless of different situations. Internal consistency reliability was measured to ensure the items within each factor assessed the same construct. Kuder–Richardson and factor analysis-derived composite reliability were evaluated to test internal consistency. These metrics are commonly used to evaluate the construct validity of assessment scales.
Ethical statement
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2013. All procedures involving human subjects/patients were approved by the Institutional Review Board of the Duke University Health System (IRB #Pro00062061), the Ethics Committee of the KCMC, Moshi, Tanzania (KCMC Research Ethical Clearance Certificate No.: 497) and the National Health Research Ethics Committee of the Tanzanian National Institute of Medical Research (NIMR/HQ/R.8a/Vol. IX/2121).
Result
Sample characteristics
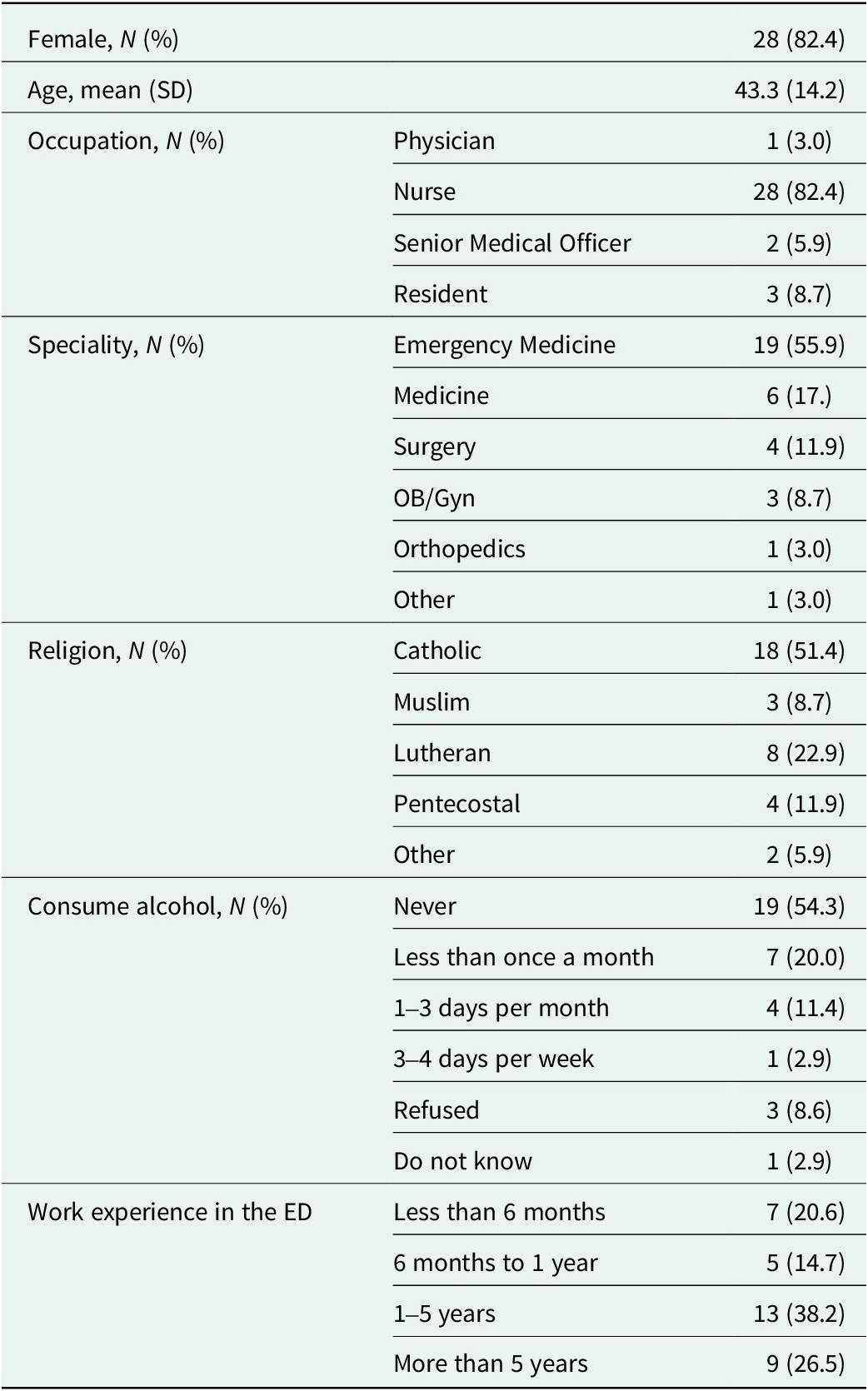
All 34 health care providers who had previously trained as counselors at KCMC participated in the study. Table 1 describes the sociodemographic characteristics of the providers included in the study. Most of the health care professionals (82.4%) were female, and their average age was 43 years. Most health care providers (82.4%) were nurses specialized in emergency medicine (55.9%). Almost all of the healthcare practitioners reported religious affiliation, most of them (51.4%) with Catholicism. More than half of the health care practitioners had more than 1 year’s working experience in ED at KCMC, and over 70% of them never drank alcohol or drank alcohol less than once a month. Health care professionals made a total of 108 assessments for 13 unique mock BI sessions.
Sociodemographic characteristics of health care professionals participating in PPKAY BI adherence scale validation

Translation and adaptation
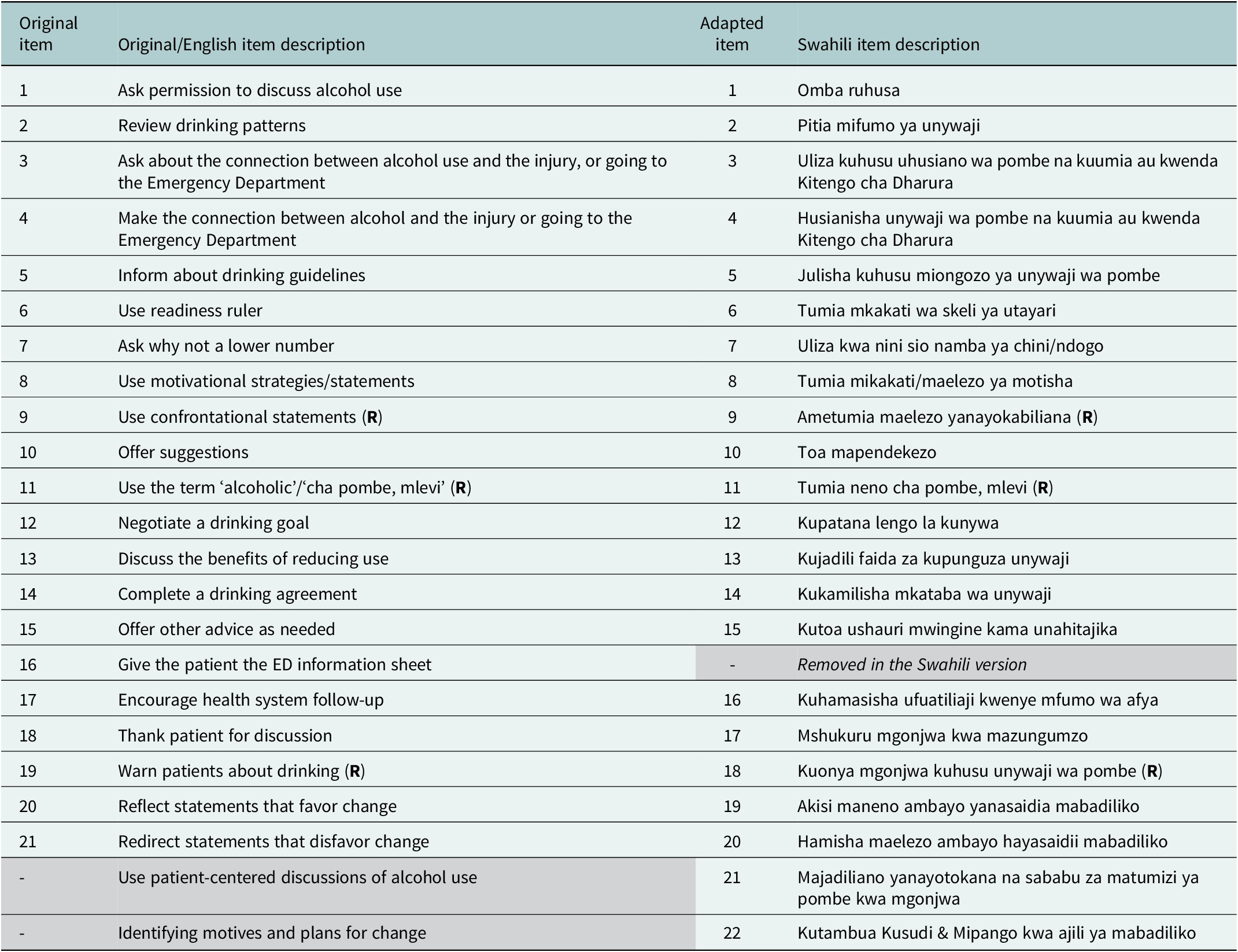
The final version of the Tanzanian-adapted and translated BAS is displayed in Table 2, with English and Swahili versions. Some challenges regarding the cultural adaptation were encountered. We identified some contexts that were not only inappropriate, but also offensive, such as ‘drunk’ (‘mlevi’); the same word is used as ‘under the influence [of alcohol]’, limiting the words that can be used in a more formal context. The health system differences were also evaluated for a better cross-cultural adaptation, guaranteeing the scale reflected the actual structure East Africa has, not comparing it with other countries, especially HICs.
Brief Intervention Adherence Scale characteristics in English and Swahili

Note: (R) = reverse-scored.
The original version of the scale consisted of 21 items. During the adaptation phase, one item of the original scale was removed, one item was modified and two items were added, resulting in a 22-item adapted version to Swahili and the Tanzanian culture. Item 16 (‘Give patient ED information sheet’) of the original scale was removed, given that it was deemed by the experts as not typical for Tanzanian medical culture. The item 17 in the original scale (16 in the Tanzanian BAS, Table 2) was changed from ‘Encourage primary care follow-up’ to ‘Encourage health system follow-up’, considering the adequacy of the Tanzanian health care system structure.
Items 21 and 22 were added to the scale (21 – “Use patient-centered discussions of alcohol use”’ and 22 – “Identifying motives and plans for change”). We included these items during the adaptation because experts, together with the research team, identified these two as essential elements to ensure protocol adherence. These two items were included after the denomination of the domains in the original scale, but were deemed important by the experts to ensure fidelity of the BI process.
Validity related to internal structure
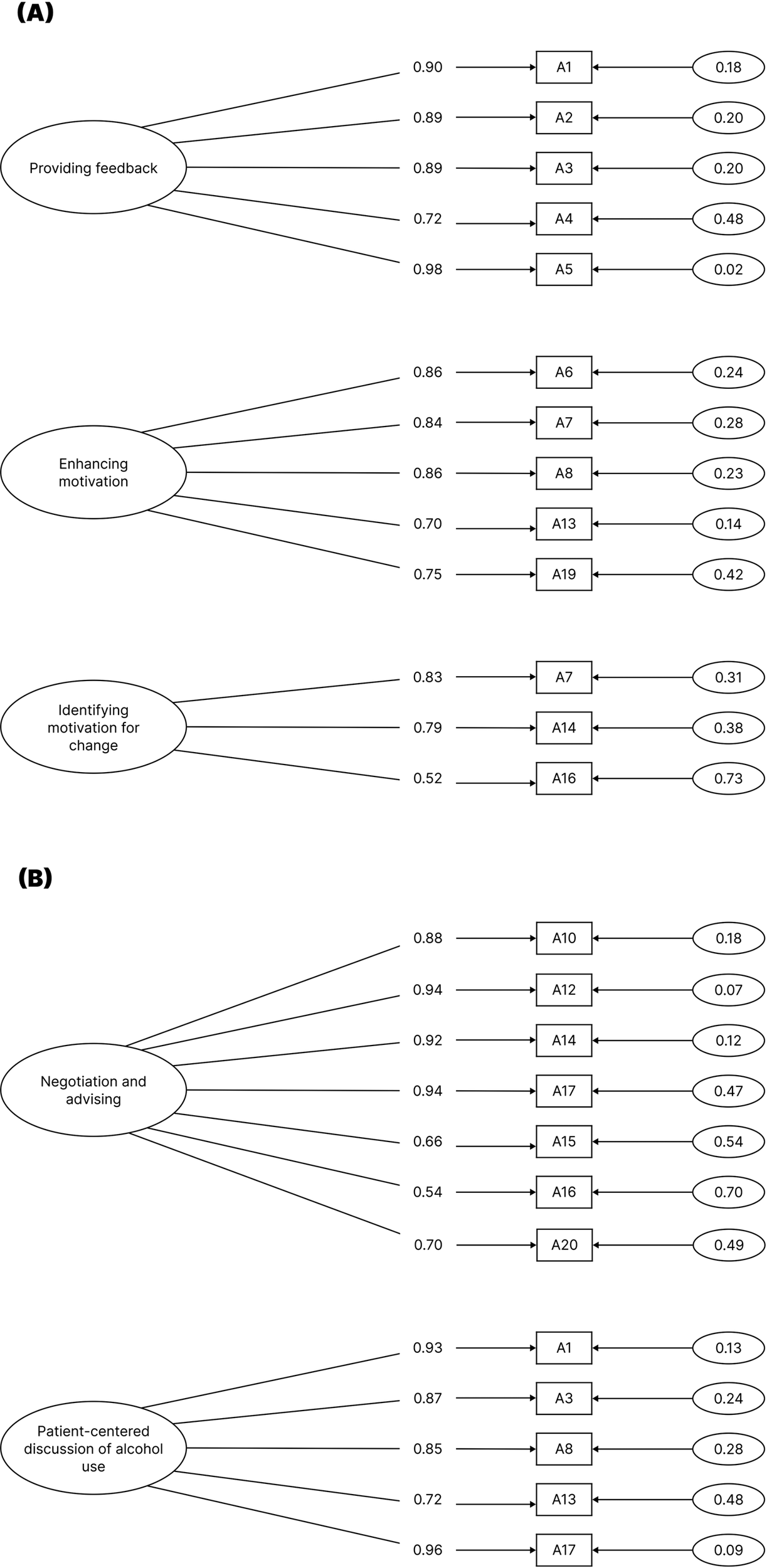
During the evaluation of the internal structure of the 22-item Tanzanian BAS, a three-factor solution was deemed to best fit the data in the factor analysis evaluation. This approach indicated the removal of items 9, 11 and 18 from the 22-item pool, due to low factor loading. Overall factor loadings are depicted in Figure 1 with appropriate latent variable allocation. The factor loadings for the CFA evaluation of the original two-factor model is also depicted in Figure 1b. All items showed high factor loadings to the proposed theoretical solution.
Confirmatory factor analysis diagram, factor loadings for BI Adherence Scale (BAS). (a) Three-factor model excluding items 9, 11, 18, 21 and 22; (b) two-factor model with items 1, 3, 7, 8, 13, 14, 16 and 17.

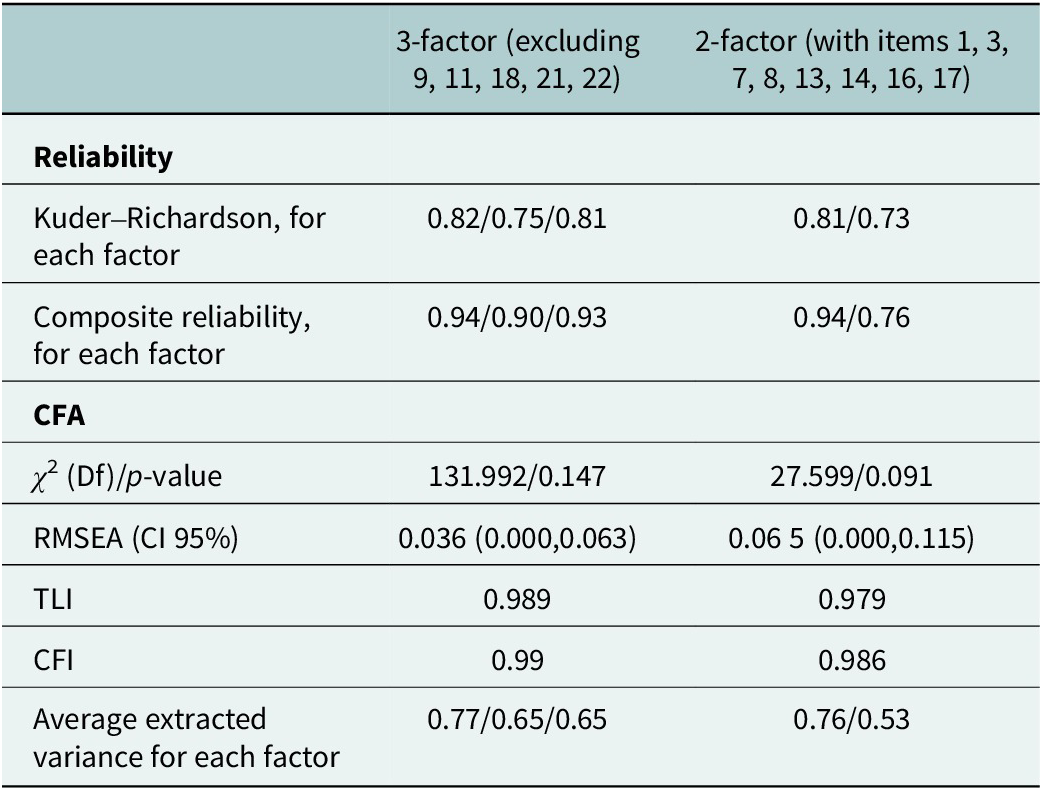
Both models had high values for TLI and CFI, larger than 0.90 (Table 3). The value of RMSEA was lower in the new proposed three-factor model (0.04), with slightly higher values for the original two-factor solution (0.07). For both models, the chi-square test showed p-values below 0.05, suggesting good adequacy of the models to the data. Average extracted variance showed the three-factor model could explain 77%, 65% and 65% variables’ variance of each dimension, while the two-factor model could explain 76% and 53% variables’ variance of each aspect. Both models demonstrated adequate fit, with better evidence for the three-factor model. However, the two-factor model demonstrates the adequacy of the original BAS internal structure in this different context and language.
Reliability and confirmatory factor analysis model fit indicators

Evidences of reliability
Both models tested have shown acceptable Cronbach’s alpha values higher than 0.70 in all dimensions, which indicates strong internal consistency of the questionnaire. However, the three-factor model had a higher Cronbach’s alpha than that of the two-factor model (Table 3).
Discussion
To our knowledge, this is the first study to conduct a cross-cultural validation of BAS for BIs for alcohol use, and the first in Tanzania. Additionally, this is also the first study to assess the psychometric properties of the scale among health care providers in sub-Saharan Africa. We demonstrated the importance of culturally adapting instruments by removing and changing items to reflect the Tanzanian culture and healthcare system, resulting in a 22-item instrument in comparison to the original 21-item instrument. The translated and adapted version of BAS showed additional evidence of the internal structure validity suggested in the original scale (Pantalon et al., Reference Pantalon, Martino, Dziura, Li, Owens, Fiellin, O’Connor and D’Onofrio2012). Our study reproduced the two-factor model with eight items, but also demonstrated the option of a three-factor model retaining further items from the original pool. Both models presented good internal consistency and factor loading.
After discussions with local professionals, some changes were made to the scale in order to align it with the healthcare system structure. The item ‘Encourage primary care follow-up’ was revised to ‘Encourage health system follow-up’, as primary care encompasses various facilities and providers, including dispensaries, traditional healers and informal healthcare providers (Maluka et al., Reference Maluka, Chitama, Dungumaro, Masawe, Rao and Shroff2018). Similarly, the item ‘Give patient ED information sheet’ was removed to reflect the discharge protocol in Tanzania, where it is uncommon to provide patients with sheets. The standard discharge plan emphasizes the information provided by doctors to patients, as literature suggests that patients believe only doctors can discuss the discharge and recovery process, which they adhere to strictly (Joiner et al., Reference Joiner, Tupetz, Peter, Raymond, Macha, Vissoci and Staton2022; Tupetz et al., Reference Tupetz, Barcenas, Isaacson, Nickenig Vissoci, Gerald, Kingazi, Mushi, Peter, Staton, Mmbaga and Bettger2022).
In addition, two new items were included within the scale. The items ‘Use patient-centered discussions of alcohol use’ and ‘Identifying motives and plans for change’ were raised after a broader investigation made by the research center on literature and on-site. Our research confirmed that the Tanzanians find alcohol to bring harm not only to the drinkers, but also to the families and the general society (Pauley et al., Reference Pauley, Metcalf, Buono, West, Rent, Nkenguye, Sawe, Mikindo, Kilasara, Mchome, Mmbaga, Vissoci and Staton2025). They also showed more prone to diminish alcohol use and binge drinking using the BI strategy, compared to the current standard practice, which does not involve testing for alcohol, nor education on alcohol use consequences (Staton et al., Reference Staton, Minja, de Souza, Gallis, Santos, Buono, Sakita, Ngowi, Boshe, Phillips, Vissoci and Mmbaga2025b). The experts confirmed that the culture of Tanzania would present more adherence to the BI if those were added as incentivized behaviors.
The two-factor model converged into two dimensions: patient-centered discussion of alcohol use and identifying motivation for change. This model reflects the main structure of the BI. However, there is a component of BI, negotiation and advice that could not be integrated into either factor. Therefore, our study evaluated the three-factor model that crosses three dimensions: providing feedback, enhancing motivation, as well as negotiation and advice, which is consistent with the composition of BI (Pantalon et al., Reference Pantalon, Martino, Dziura, Li, Owens, Fiellin, O’Connor and D’Onofrio2012). The three-factor model had a slightly better factor structure with satisfactory values of fit indices (CFI, TLI, NFI > 0.98 and RMSEA < 0.05). The p-value is nonsignificant, which indicates that there is no significant difference between the estimated covariance matrix and the actual covariance matrix. Average extracted variance shows that items within each dimension could explain over 60% variance of the corresponding factor.
The use of a three-factor model can challenge the implementation of the scale (Irribarra and Arneson, Reference Irribarra and Arneson2023). The complexity added by an extra dimension changes how providers interpret the results and imposes a higher time demand on the process (Irribarra and Arneson, Reference Irribarra and Arneson2023). However, the added factor increases reliability regarding the cultural context of Tanzania. As a nonconfrontational culture (Erb et al., Reference Erb, Letang, Glass, Natamatungiro, Mnzava, Mapesi, Haschke, Duthaler, Berger, Muri, Bader, Marzolini, Elzi, Klimkait, Langewitz and Battegay2017), but also presenting a high stigma level towards alcohol use (Staton et al., Reference Staton, Vissoci, Wojcik, Hirshon, Mvungi, Mmbaga and Swahn2018b; Pauley et al., Reference Pauley, Metcalf, Buono, West, Rent, Nkenguye, Sawe, Mikindo, Kilasara, Mchome, Mmbaga, Vissoci and Staton2025), the original two-factor model does not comprehend the nuances of the Tanzanian social image of Alcohol Use Disorder (AUD).
During our internal structure evaluation, we removed three items from the item-pool scale due to low factor loading. The items: ‘Using confrontational statements’, ‘using the term “alcoholic”/“cha pombe, mlevi”’ and ‘warning patients about drinking’ were removed. This can be related to these items being reverse-coded, which have demonstrated some problematic psychometric properties in the literature, especially when translating and culturally adapting a scale or questionnaire (DiStefano and Motl, Reference DiStefano and Motl2006; Venta et al., Reference Venta, Bailey, Walker, Mercado, Colunga-Rodriguez, Ángel-González and Dávalos-Picazo2022). Another reason is due to the cultural context, in which two items were deemed superfluous or moot. The ‘using the term “alcoholic”’ item’s exclusion could be explained by the stigma over the term ‘alcoholic’ in Swahili, which is well documented in the literature (El-Gabri et al., Reference El-Gabri, Nickenig Vissoci, Meier, Mvungi, Haglund, Swahn, Mmbaga, Gerardo and Staton2020; Zhao et al., Reference Zhao, Nickenig Vissoci, Mmbaga, Abdullah and Staton2020). The other two exclusions refer to confrontational behavior during the PPKAY session. Tanzanian culture is known to be a welcoming culture, and, thus, confrontational behavior is not well received in the healthcare setting in general, with evidence that providers’ communication can increase adherence to treatment (Erb et al., Reference Erb, Letang, Glass, Natamatungiro, Mnzava, Mapesi, Haschke, Duthaler, Berger, Muri, Bader, Marzolini, Elzi, Klimkait, Langewitz and Battegay2017). The strong stigma in both these contexts might have produced low variance and, therefore, low factor loading, as the providers would not use these behaviors or words seen as offensive.
The BAS was found to have excellent internal consistency, with Kuder Richardson’s alpha > 0.75 for each dimension. The composite reliability was also calculated to evaluate the reliability of the scale. All the parameters are consistent for the items within each dimension, sufficiently explaining the corresponding latent variables. In other words, the Swahili version of the BAS is a reliable psychometric instrument to evaluate healthcare practitioners’ adherence to BI.
The use of the BAS for alcohol-related BIs may contribute to leverage the quality of care provided in Tanzania. By using the instrument developed in the present work, health professionals can gather a quality parameter to assess the BI implementation in ED settings. The potential impact of BI as an effective approach to reduce alcohol-related harms is well documented in the literature (Heather, Reference Heather2014; Cherpitel et al., Reference Cherpitel, Ye, Moskalewicz and Swiatkiewicz2015; Wright et al., Reference Wright, Dietze and Lim2017; Staton et al., Reference Staton, Zadey, O’Leary, Phillips, Minja, Swahn, Hirshon, Boshe, Sakita, Vissoci and Mmbaga2022b).
In this scenario, it is valid to mention that the stakeholders did not have a direct role in the scale development, but their perceptions were included in the protocol for the BAS adaptation (Staton et al., Reference Staton, Minja, de Souza, Gallis, Santos, Buono, Sakita, Ngowi, Boshe, Phillips, Vissoci and Mmbaga2025b). The stakeholders demonstrated a readiness level to address the harm caused by the alcohol use that is high in knowledge and low in attitudes toward alcohol prevention and the lack of material and human resources (Swahn et al., Reference Swahn, Robow, Balenger, Staton, Kasirye, Francis, Komba and Siema2022). Thus, the tool developed here can be used for health managers, policymakers and practitioners to be sure that interventions aiming to reduce alcohol consumption are being implemented in the best way possible.
Nonetheless, the feasibility of the clinical use of the scale is something that needs further research. Although the tool presented valid psychometric properties, the providers show high stigma toward alcohol use, stating that this discussion is not within their expected functions (Staton et al., Reference Staton, Vissoci, Wojcik, Hirshon, Mvungi, Mmbaga and Swahn2018b). In addition, Tanzania has a lack of resources for electronic health records implementation, which can lead to an underuse of the scale (Nuwas et al., Reference Nuwas, Gidabayda, Bellet, Guga and Matu2023; Mwogosi and Kibusi, Reference Mwogosi and Kibusi2024). Training, funding and audit processes are essential to better implement the BAS into the practice.
One limitation of this study is related to the external validity. Our study only contains 34 health care providers working at KCMC, a tertiary academic health center. The results need to be further evaluated to be generalized to other Tanzanian healthcare settings. Another limitation is that the BAS was assessed on a dichotomous scale rather than a Likert-type scale. As a result, the study could not evaluate the degree to which health care practitioners adhere to each BAS item.
As recommendations for the implementations of BIs and the BAS in Tanzania and East Africa, we highlight the need for more research to identify the feasibility in clinical settings and the generalizability among other Tanzanian health facilities, such as rural clinical and community-based health settings. The expansion of screening for alcohol use and advancing the medical training in the country are much-needed policies for a better and faster translational process of evidence-based practices.
In conclusion, this study developed the first validated Swahili version of BAS in Tanzania. The BAS adaptation to Tanzania led to modifications to the original BAS, which made it coherent to assess healthcare providers’ adherence to BI in the context. The Tanzanian BAS had 22 items and showed 3 domains of evaluation. It could be used to study the association between BI and alcohol use among injury patients and drive evidence-based policy to avoid mortality and morbidity caused by harmful alcohol use.
Open peer review
To view the open peer review materials for this article, please visit http://doi.org/10.1017/gmh.2025.10124.
Data availability statement
The data and the analysis code that support the findings of this study are available from the corresponding author, CAS, upon reasonable request.
Acknowledgments
The authors would like to thank the participants for their time and effort in sharing their perspectives and medical experiences. The authors would also like to thank Alice A. Andongolile for her effort in translating the abstracts to Swahili.
Author contribution
All authors were involved in the study’s conception and design. AJP, CAS and JRNV had complete access to the data and assumed responsibility for its integrity and the accuracy of the analysis. All authors contributed to the interpretation of results. AJP, JW, NNO and VMM drafted the first version of the manuscript. TAHR, JVPS, JB and BM critically revised the manuscript. All authors participated in revising and approving the final version of the manuscript, and shared responsibilities for all aspects of the work.
Financial support
This project was conducted with funding from the National Institute of Health Fogarty International Center K01- TW010000 (PI Staton) and the National Institute of Alcohol and Alcoholism PRACT: Pragmatic Randomized Adaptive Clinical Trial to Investigate Controlling Alcohol-related harms in a Low-Income Setting; Emergency Department Brief Interventions in Tanzania R01AA027512 (PI Staton). The funding source had no influence on the study report.
Competing interests
The authors declare none.
Transparency declaration
The authors declare that the results reported here are honest, accurate and transparent. No information has been omitted by the authors. Any discrepancies from the original protocol were explained within the sections of the study.

 Open access
Open access
Comments
To
The Editor-in-Chief
Cambridge Prisms: Global Mental Health
Date: 26th May 2025
Subject: Submission of Research Article manuscript
Dear Editor
We wish to submit the Research Article manuscript for publication in the Cambridge Prisms: Global Mental Health, titled “Translation and Adaptation of the Brief Intervention Adherence Scale for the Tanzanian Culture”. The paper was authored by me and my collaborators listed in the manuscript.
The manuscript presents the psychometric evaluation of the first Tanzanian-Swahili version of the Brief Intervention Adherence Scale (BAS), culturally adapted and rigorously tested within the “Punguza Pombe Kwa Afya Yako” program at Kilimanjaro Christian Medical Centre. Employing exploratory structural equation modeling and confirmatory factor analysis, we identified and confirmed a three-factor structure with strong internal consistency, demonstrating the instrument’s validity and reliability for assessing healthcare providers’ fidelity to brief alcohol interventions in a low-resource, LMIC setting. These results build on global efforts to ensure intervention adherence and fill a critical gap by offering the first validated Swahili BAS in Tanzania, an accessible tool with potential for broad regional implementation across East Africa. Overall, our findings support the BAS’s utility for monitoring and enhancing intervention quality, laying the groundwork for future implementation studies and capacity-building initiatives in harm-reduction services.
Required documents associated with the manuscript have been enclosed as the journal guidelines in the recommended format.
Thank you for your consideration. We look forward to hearing from you.