


1. Introduction
The COVID-19 pandemic was not only a global medical emergency but also a social one. The pandemic response across countries and the varying support it received both within and between societies highlighted the complex interplay between governance and society for successful pandemic management (Bonell et al., Reference Bonell, Michie, Reicher, West, Bear, Yardley, Curtis, Amlôt and Rubin2020; Reicher and Drury, Reference Reicher and Drury2021; Ruggeri et al., Reference Ruggeri, Stock, Haslam, Capraro, Boggio, Ellemers, Cichocka, Douglas, Rand, van der Linden, Cikara, Finkel, Druckman, Wohl, Petty, Tucker, Shariff, Gelfand, Packer and Willer2024; Van Bavel et al., Reference Van Bavel, Pretus, Rathje, Pärnamets, Vlasceanu and Knowles2024; Webster et al., Reference Webster, Brooks, Smith, Woodland, Wessely and Rubin2020). For example, many countries struggled with persuading the public to support policy measures that mandate behaviors aimed at stemming the spread of the disease (Euronews, 2021; Lowen, Reference Lowen2020). Recent research has consistently found socioeconomic factors predict individuals willingness and capacity to adhere to public health recommendations (Atchison et al., Reference Atchison, Bowman, Vrinten, Redd, Pristerà, Eaton and Ward2021; Reicher and Drury, Reference Reicher and Drury2021). Research has uncovered several other predictors of adhering to these recommendations, including risk-taking (Pollak et al., Reference Pollak, Dayan, Shoham and Berger2020), partisan identity (Gollwitzer et al., Reference Gollwitzer, Martel, Brady, Pärnamets, Freedman, Knowles and Van Bavel2020; Van Bavel et al., Reference Van Bavel, Pretus, Rathje, Pärnamets, Vlasceanu and Knowles2024), and perceived threat of the virus (Kachanoff et al., Reference Kachanoff, Bigman, Kapsaskis and Gray2020). Understanding psychological predictors of adopting public health-related behavior is important not only to assess responses in the recent pandemic but also to improve preparedness for future crises. In the current article, we examined the extent to which intellectual humility predicted protective behaviors, support for public health measures, and disbelief in conspiracy theories relating to the COVID-19 pandemic.
During the COVID-19 pandemic, many people adopted mistaken and conspiratorial beliefs about the origin and mechanisms of transmission of the virus (Douglas, Reference Douglas2021; Marchlewska et al., Reference Marchlewska, Hamer, Baran, Górska and Kaniasty2022; Sternisko et al., Reference Sternisko, Cichocka, Cislak and Van Bavel2023; Uscinski et al., Reference Uscinski, Enders, Klofstad, Seelig, Funchion, Everett, Wuchty, Premaratne and Murthi2020; Van Bavel et al., Reference Van Bavel, Baicker, Boggio, Capraro, Cichocka, Cikara, Crockett, Crum, Douglas, Druckman, Drury, Dube, Ellemers, Finkel, Fowler, Gelfand, Han, Haslam, Jetten and Willer2020). Conspiracy beliefs are associated with decreased societal engagement, including a decreased willingness to help high-risk groups and trust government regulations (Pummerer et al., Reference Pummerer, Böhm, Lilleholt, Winter, Zettler and Sassenberg2022) and, as such, may lead people to expose themselves and others to avoidable risks. The adoption of conspiracy beliefs is associated with epistemic motivations to build causal understanding of the world, need for social belonging, and attempts to take narrative control over a complicated and threatening world (Bowes et al., Reference Bowes, Costello and Tasimi2023; Douglas et al., Reference Douglas, Sutton and Cichocka2017; Goertzel, Reference Goertzel1994; Golec de Zavala and Cichocka, Reference Golec de Zavala and Cichocka2012; Sternisko et al., Reference Sternisko, Cichocka and Van Bavel2020). In this article, we investigated whether individuals’ open-mindedness predicted the degree to which they adhered to public health behaviors or held COVID-19-related conspiracy beliefs.
Open-mindedness is sometimes treated as identical to intellectual humility, and sometimes as a facet of a broader notion of intellectual humility (Alfano et al., Reference Alfano, Iurino, Stey, Robinson, Christen, Yu and Lapsley2017; Baehr, Reference Baehr2011; Fantl, Reference Fantl2018; Krumrei-Mancuso and Worthington Jr., Reference Krumrei-Mancuso, Worthington, Ottati and Stern2023; Porter et al., Reference Porter, Elnakouri, Meyers, Shibayama, Jayawickreme and Grossmann2022). Here, we used an open-mindedness sub-scale from a multidimensional, validated scale of intellectual humility (Alfano et al., Reference Alfano, Iurino, Stey, Robinson, Christen, Yu and Lapsley2017). Accordingly, we adopted a conception of open-mindedness as reflecting a disposition to acknowledge the limitations of one’s knowledge, especially relative to others, and one that is contrasted with arrogance about one’s capabilities and knowledge. This conception of open-mindedness should not be confused with other ones, such as ‘reflexive open-mindedness’ (Sternisko et al., Reference Sternisko, Cichocka, Cislak and Van Bavel2023), which correlate with COVID-19 conspiracy beliefs but are based on willingness to accept pseudo-profound bullshit. Hence, people high in open-mindedness, being more willing to consider (and critically evaluate) alternative beliefs, should be more likely to settle on accurate or well-supported beliefs. As such, it is also likely related to the broader concept of actively open-minded thinking (AOT) (Baron et al., Reference Baron, Isler, Yilmaz, Ottati and Stern2023), although this work was not designed to investigate that relationship. Recent work has found that more open-minded people are more likely to report compliance with COVID-19 guidelines (Plohl and Musil, Reference Plohl and Musil2021), and that open-mindedness, together with other measures of analytical thinking, correlates negatively with holding conspiracy beliefs (Bowes and Tasimi, Reference Bowes and Tasimi2022; Maglić et al., Reference Maglić, Pavlović and Franc2021; Stoica and Umbres, Reference Stoica and Umbres2021; Swami et al., Reference Swami, Voracek, Stieger, Tran and Furnham2014).
1.1. Overview
We extend previous research on the relationship between open-mindedness and COVID-19-related beliefs and behaviors by analyzing a large global sample (N = 46,745 from 68 countries). We first report the results of a preregistered analysis investigating whether a six-item self-report measure of open-mindedness correlates positively with support for public health measures and negatively with conspiracy beliefs. We then report exploratory analyses investigating a two-factor structure of open-mindedness and interactions between these 2 factors of open-mindedness and participants’ political beliefs on their public health support and conspiracy beliefs. Past research has implicated left–right political ideology both with adherence or support for public health measures (de la Cerda et al., Reference de la Cerda, Hartlyn and Martinez-Gallardo2024; Gollwitzer et al., Reference Gollwitzer, Martel, Brady, Pärnamets, Freedman, Knowles and Van Bavel2020; Kerr et al., Reference Kerr, Panagopoulos and van der Linden2021; Pavlović et al., Reference Pavlović, Todosijević and Stanojević2021; Van Bavel et al., Reference Van Bavel, Pretus, Rathje, Pärnamets, Vlasceanu and Knowles2024) during the COVID-19 pandemic, as well as with general and COVID-related conspiratorial beliefs (Lamberty et al., Reference Lamberty, Hellmann and Oeberst2018; Stoica and Umbres, Reference Stoica and Umbres2021). Little is known, however, about how political ideology and open-mindedness interact in this context—although AOT tends to correlate with political liberalism (Baron et al., Reference Baron, Isler, Yilmaz, Ottati and Stern2023).
We find that support for public health measures is associated with a learning-oriented factor of open-mindedness while endorsement of conspiratorial beliefs is associated with a threat-oriented factor of open-mindedness. We further find that the effect of threat-oriented open-mindedness is larger for right-wing compared to left-wing participants. These findings suggest that open-mindedness may not be a unified disposition, and that different aspects of it are associated with different attitudes and behaviors.
2. Method
2.1. Dataset
The dataset used in this publication was gathered as part of the International Collaboration on the Social & Moral Psychology of COVID-19 (https://icsmp-covid19.netlify.app/) (Azevedo et al., Reference Azevedo, Pavlović, Rêgo, Ay, Gjoneska, Etienne, Ross, Schönegger, Riaño-Moreno, Cichocka, Capraro, Cian, Longoni, Chan, Van Bavel, Sjåstad, Nezlek, Alfano, Gelfand and Sampaio2023). The original data collection was fully approved by the School of Psychology, University of Kent (UK), review committee panel with an Ethics ID of 202015872211976468. In accordance with the rules developed by the leadership team, in order to access the dataset, we completed a preregistration of our intended primary analyses prior to accessing the raw data (https://osf.io/psbwz).
2.2. Participants
The analyzed dataset consists of responses collected from N = 46,745 participants (mean age = 43.1 (SD = 16.1); 51.9% women, 47.7% men, 0.4% other). The dataset had undergone cleaning, prior to us receiving it, including removing participants who failed attention checks from an original sample size of 50,944. The sample was collected from 68 countries from all continents other than Antarctica. Representative samples were collected in 28 countries while convenience samples were collected in 36 countries, and both types of sampling were used in 3 countries. Full details are provided in Van Bavel et al. (Reference Van Bavel, Cichocka, Capraro, Sjåstad, Nezlek, Pavlović, Alfano, Gelfand, Azevedo, Birtel, Cislak, Lockwood, Ross, Abts, Agadullina, Aruta, Besharati, Bor, Choma and Boggio2022).
2.3. Survey and measures
Questionnaires were administered online. Each participant completed a series of psychological measures and self-reported public health behaviors. Participants completed the scales in random order. For multi-item scales, we average the items to produce the measure.
2.3.1. Primary measures
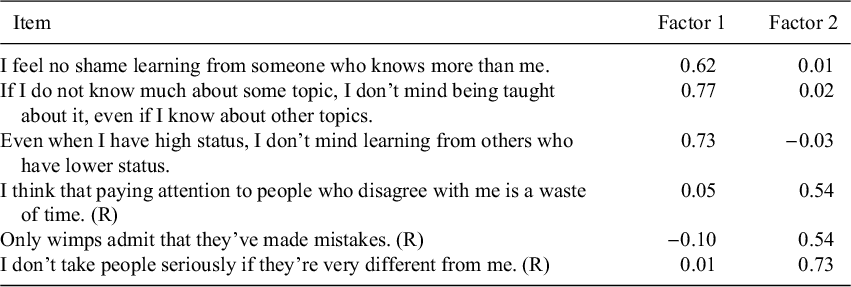
For the current article, the key focus is the extent to which open-mindedness predicts primary outcome variables. Our measure of open-mindedness is part of a recently developed multidimensional self-report measure of intellectual humility (Alfano et al., Reference Alfano, Iurino, Stey, Robinson, Christen, Yu and Lapsley2017). Open-mindedness is conceived in this instrument as a disposition that involves behaviors and attitudes that reflect an acknowledgment of the limitations of one’s knowledge, especially relative to others, and a desire to gain knowledge irrespective of status. See Table 1 for all items. Alpha of the scale was 0.71 in this sample and multilevel reliability (
 $\alpha _{ml}$
) was 0.58 (Nezlek, Reference Nezlek2017).
$\alpha _{ml}$
) was 0.58 (Nezlek, Reference Nezlek2017).
All items on the open-mindedness scale as well as factor loadings from exploratory factor analysis. Factor 1 we call learning orientation and Factor 2 threat orientation. (R) indicates reverse coded item

As our primary outcome variables, we included 1 measure of belief in conspiracy theories and 3 measures of public health support. A conspiracy belief scale consisting of 4 items (
 $\alpha = 0.92$
,
$\alpha = 0.92$
,
 ${\alpha _{ml} = 0.89}$
). A physical distancing scale consisting of 5 items, but following Van Bavel et al. (Reference Van Bavel, Cichocka, Capraro, Sjåstad, Nezlek, Pavlović, Alfano, Gelfand, Azevedo, Birtel, Cislak, Lockwood, Ross, Abts, Agadullina, Aruta, Besharati, Bor, Choma and Boggio2022), 1 item was dropped to improve reliability (
${\alpha _{ml} = 0.89}$
). A physical distancing scale consisting of 5 items, but following Van Bavel et al. (Reference Van Bavel, Cichocka, Capraro, Sjåstad, Nezlek, Pavlović, Alfano, Gelfand, Azevedo, Birtel, Cislak, Lockwood, Ross, Abts, Agadullina, Aruta, Besharati, Bor, Choma and Boggio2022), 1 item was dropped to improve reliability (
 $\alpha = 0.78$
,
$\alpha = 0.78$
,
 $\alpha _{ml} = 0.74$
). A physical hygiene scale (
$\alpha _{ml} = 0.74$
). A physical hygiene scale (
 $\alpha = 0.79$
,
$\alpha = 0.79$
,
 $\alpha _{ml} = 0.72$
) consisting of 5 items. Finally, a policy support scale consisting of 4 items (
$\alpha _{ml} = 0.72$
) consisting of 5 items. Finally, a policy support scale consisting of 4 items (
 $\alpha = 0.87$
,
$\alpha = 0.87$
,
 $\alpha _{ml} = 0.85$
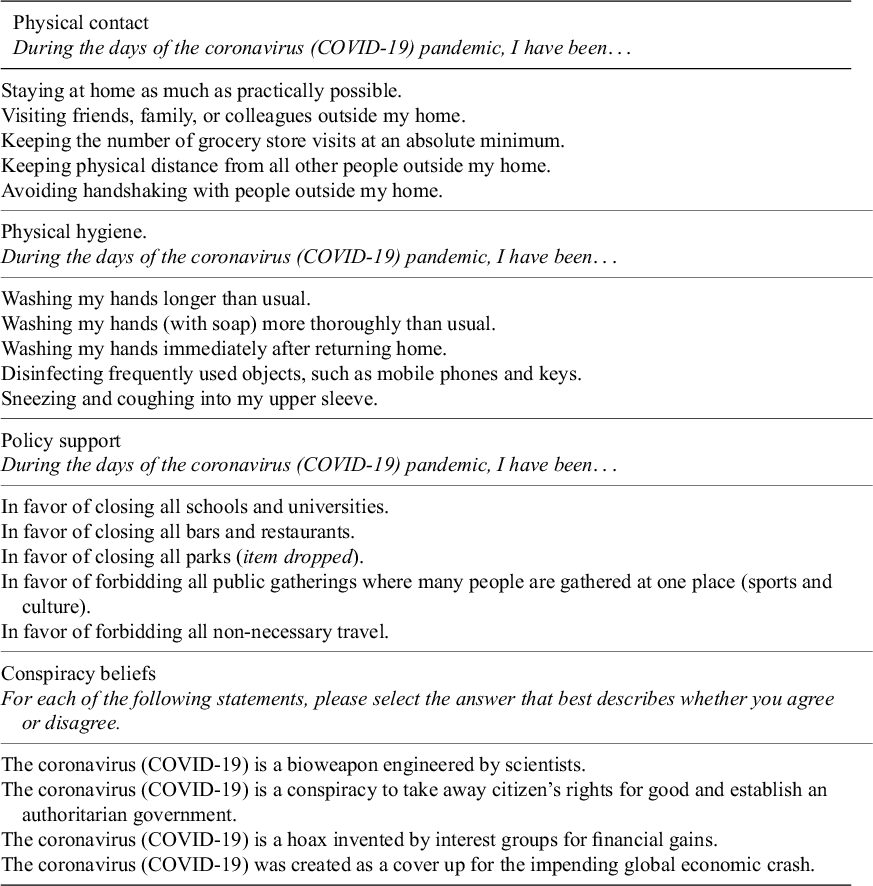
). See Table 2 for all items.
$\alpha _{ml} = 0.85$
). See Table 2 for all items.
Items for the 4 outcome measures

Responses for all primary were recorded using a slider scale with 3 labels: 0 = ‘strongly disagree’, 5 = ‘neither agree nor disagree’, and 10 = ‘strongly agree’.
2.3.2. Demographics and secondary measures
In addition to age and gender, the following demographic variables were collected from participants and used in our analyses. Participants were asked to indicate marital status (single, in a relationship, or married), number of children, current employment status (working, not working, student, retired, or other), whether they resided in a predominately urban or rural area, and socio-economic status (11-rung ladder measure) (Bjørnskov, Reference Bjørnskov2010).
Participants responded to the following social and moral psychological measures:
-
• A four-item social belonging scale (Malone et al., Reference Malone, Pillow and Osman2012) (
 $\alpha = 0.85$
,
$\alpha _{ml} = 0.82$
).
$\alpha = 0.85$
,
$\alpha _{ml} = 0.82$
). -
• A three-item collective narcissism scale (De Zavala et al., Reference De Zavala, Cichocka, Eidelson and Jayawickreme2009) (
$\alpha = 0.87$
,
$\alpha _{ml} = 0.82$
). -
• A six-item narcissism scale (Back et al., Reference Back, Küfner, Dufner, Gerlach, Rauthmann and Denissen2013) (
$\alpha = 0.78$
,
$\alpha _{ml} = 0.69$
). -
• A seven-item morality as cooperation scale (Curry et al., Reference Curry, Chesters and Van Lissa2019) (
$\alpha = 0.73$
,
$\alpha _{ml} = 0.67$
). -
• A ten-item moral identification scale (Aquino and Reed II, Reference Aquino and Reed2002) (
$\alpha = 0.73$
,
$\alpha _{ml} = 0.45$
). -
• A two-item national identification scale, with one item from (Postmes et al., Reference Postmes, Haslam and Jans2013) and one additional item measuring item centrally (
$\alpha = 0.80$
,
$\alpha _{ml} = 0.72$
). -
• A two-item trait optimism scale (Scheier et al., Reference Scheier, Carver and Bridges1994) (
$\alpha = 0.83$
,
$\alpha _{ml} = 0.81$
). -
• A two-item psychological well-being scale (Bjørnskov, Reference Bjørnskov2010) (
$\alpha = 0.77$
,
$\alpha _{ml} = 0.76$
). -
• A two-item COVID-19 risk perception scale, comprised of ‘By April 30, 2021: How likely do you think it is that you will get infected by the Coronavirus (COVID-19)?’ and ‘By April 30, 2021: How likely do you think it is that the average person in [YOUR COUNTRY] will get infected by the Coronavirus (COVID-19)?’. Available answers from 0% to 100%, with 10% increments Risk perception (
$\alpha = 0.95$
,
$\alpha _{ml} = 0.94$
). -
• A four-item trait self control scale (Tangney et al., Reference Tangney, Baumeister and Boone2004) (
$\alpha = 0.63$
,
$\alpha _{ml} = 0.50$
). -
• A one-item self-esteem scale (Robins et al., Reference Robins, Hendin and Trzesniewski2001).
-
• A one-item moral circle measure (Waytz et al., Reference Waytz, Iyer, Young, Haidt and Graham2019).
-
• A one-item subjective physical health measure: ‘In general, how would you rate your physical health as it is today?’
-
• A one-item generosity measure, measuring the proportion of the daily wage in the corresponding country a participant would keep for themselves versus giving to charity (Sjåstad, Reference Sjåstad2019).
-
• A three-item cognitive reflection test (CRT). The test was a reworded version of the test proposed by Frederick (Reference Frederick2005); the items were reworded because the classic CRT is very well known. The proportion of correct responses was distributed as follows: 35% 0, 35% 1, 16% 2, and 14% 3.
-
• A one-item measure of political ideology: ‘Overall, what would be the best description of your political views?’, anchored at 0 = Very left-leaning, 5 = Center, and 10 = Very right leaning. This single-item measure of ideology has been found to account for a significant proportion of the variance in presidential voting intentions in American National Election studies between 1972 and 2004 (Jost, Reference Jost2006) and has been used in cross-cultural research (Caprara et al., Reference Caprara, Vecchione, Schwartz, Schoen, Bain, Silvester, Cieciuch, Pavlopoulos, Bianchi, Kirmanoglu, Baslevent, Mamali, Manzi, Katayama, Posnova, Tabernero, Torres, Verkasalo, Lönnqvist and Caprara2017; Choma et al., Reference Choma, Hodson, Sumantry, Hanoch and Gummerum2021; Imhoff et al., Reference Imhoff, Zimmer, Klein, António, Babinska, Bangerter, Bilewicz, Blanuša, Bovan, Bužarovska, Cichocka, Delouvée, Douglas, Dyrendal, Etienne, Gjoneska, Graf, Gualda, Hirschberger and van Prooijen2022).




















All measures included in the survey and their wording are available at the following page https://tinyurl.com/osfopenmindreview.
2.4. Analysis
We conducted analyses using the R software program version 4.4.3 (R Core Team, 2021) and used the brms package (Bürkner, Reference Bürkner2018) to fit our primary Bayesian regression models and metafor package to fit meta-analytic models (Viechtbauer, Reference Viechtbauer2010).
We report results from 2 types of analyses. First, multilevel correlation analyses that group variation by country. This is fit as a multivariate, multilevel regression in brms on all predictor variables collected in the study (we report a model including demographic variables in the Supplementary Material). The resulting correlations, due to the multilevel fitting, guard against Simpson’s paradox in our inferences. Since the scales we used aren’t perfectly reliable, we disattenuated the full posterior correlation matrix using the scale reliabilities as given by omega total as calculated by the psych package (Revelle, Reference Revelle2020). In the Supplementary Material, we additionally report results from disattentuating using Guttman’s lambda-6 instead.
Second, we report regression analyses on the 4 outcome variables: physical contact, physical hygiene, policy support, and conspiracy beliefs. These analyses are all multilevel and multivariate to account for the structure of the data, with participants nested in countries. For the multilevel regressions, all per-country slopes were modeled in addition to the population-level effects. All variables were z-scored. The following priors were used when fitting the regression models: Normal(0, 0.1) for all predictor variables, Exponential(1) for all standard deviations of the varying intercepts and slopes, and LKJ(5) for the correlation matrix of the per-country varying coefficients. We fit models using 4 chains in parallel with at least 1,000 post warm-up samples each, increasing the number of samples if necessary to reach convergence of the chains. Convergence was assessed using the R-hat statistic (Gelman and Rubin, Reference Gelman and Rubin1992) using a criterion of <1.05.
Exploratory factor analysis was performed using the psych package.
The full analysis code is available at https://osf.io/stx86.
3. Results
3.1. Preregistered analyses
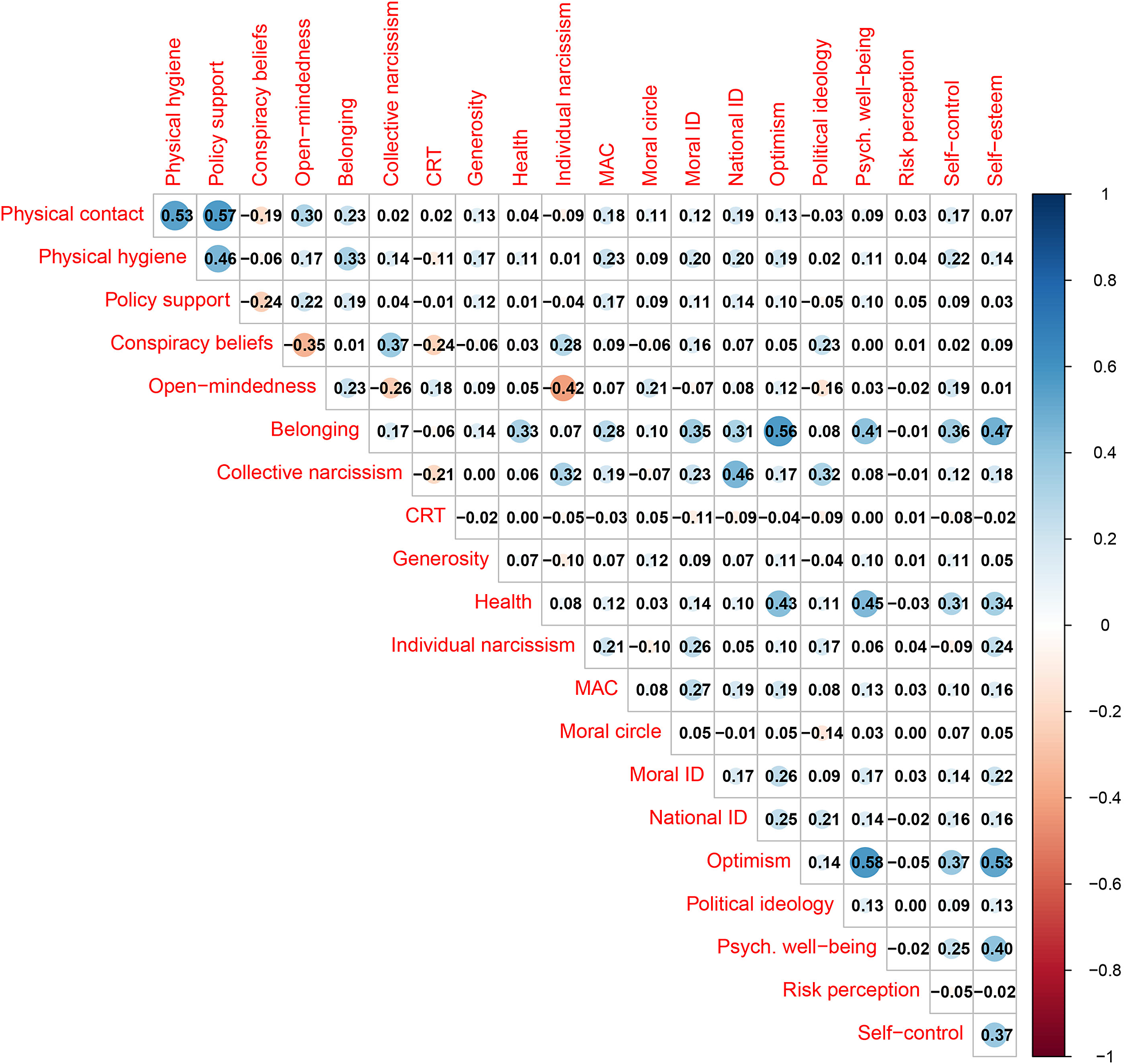
On average, participants reported that they were following guidelines for reduced physical contact (M = 8.5, SD = 1.8) and physical hygiene (M = 7.9, SD = 1.9; all on 0–10 scales), and that they supported policies aiming at reducing movement and activity in society (M = 8.2, SD = 2.2). We estimated correlations among measures using a multilevel regression model and disattenuated the posterior coefficient matrices using scale reliabilities (Kahneman, Reference Kahneman1965) (see Figure 1 in the Supplementary Material for raw correlations and Figure 2 in the Supplementary Material for alternative disattenuation using Guttman’s
 $\lambda _6$
). All 3 measures were moderately correlated with one another (
$\lambda _6$
). All 3 measures were moderately correlated with one another (
 $\mathit {r}$
s = 0.45–0.55, see Figure 1). On average, participants also rejected conspiratorial beliefs about COVID-19 (M = 3.1, SD = 2.9), although variation in conspiracy beliefs was greater than in the preceding measures. Conspiracy beliefs were negatively correlated with physical contact (
$\mathit {r}$
s = 0.45–0.55, see Figure 1). On average, participants also rejected conspiratorial beliefs about COVID-19 (M = 3.1, SD = 2.9), although variation in conspiracy beliefs was greater than in the preceding measures. Conspiracy beliefs were negatively correlated with physical contact (
 $\mathit {r}$
=
$\mathit {r}$
=
 $-$
0.19) and policy support (
$-$
0.19) and policy support (
 $\mathit {r}$
=
$\mathit {r}$
=
 $-$
0.24), and negligibly correlated with physical hygiene (
$-$
0.24), and negligibly correlated with physical hygiene (
 $\mathit {r}$
=
$\mathit {r}$
=
 $-$
0.06). On average, participants’ open-mindedness scores were M = 7.9 (SD = 1.5), and open-mindedness was positively correlated with all public health measures (
$-$
0.06). On average, participants’ open-mindedness scores were M = 7.9 (SD = 1.5), and open-mindedness was positively correlated with all public health measures (
 $\mathit {r}$
s = 0.17–0.33, see Figure 1) and negatively correlated with conspiracy beliefs (
$\mathit {r}$
s = 0.17–0.33, see Figure 1) and negatively correlated with conspiracy beliefs (
 $\mathit {r}$
=
$\mathit {r}$
=
 $-$
0.35).
$-$
0.35).
Pairwise correlations of all variables investigated in the present study. Median posterior estimate is shown from a multilevel correlation model which nests observations in countries. Posterior estimates are disattenuated by scale reliabilities (
 $\omega _t$
). The color gradient indicates the strength of the correlation (blue—positive; red—negative).
$\omega _t$
). The color gradient indicates the strength of the correlation (blue—positive; red—negative).

A key feature of our dataset is that multiple social and moral psychology measures were collected from each participant. This allowed us to investigate the robustness and relative predictive power of open-mindedness in light of multiple potential competing predictors. We fit several multivariate, multilevel regression models, regressing the 3 public health support measures and conspiracy beliefs on open-mindedness (z-scored) with the additional (z-scored) predictors.Footnote
1
All slopes were allowed to vary grouped by country. The correlations between all predictors are shown in Figure 1. For physical contact, the model
 $R^2$
= 0.21, 95% CI = [0.20, 0.22]; for physical hygiene,
$R^2$
= 0.21, 95% CI = [0.20, 0.22]; for physical hygiene,
 $R^2$
= 0.25, 95% CI = [0.25, 0.26]; for policy support,
$R^2$
= 0.25, 95% CI = [0.25, 0.26]; for policy support,
 $R^2$
= 0.23, 95% CI = [0.23, 0.24]; and for conspiracy beliefs,
$R^2$
= 0.23, 95% CI = [0.23, 0.24]; and for conspiracy beliefs,
 $R^2$
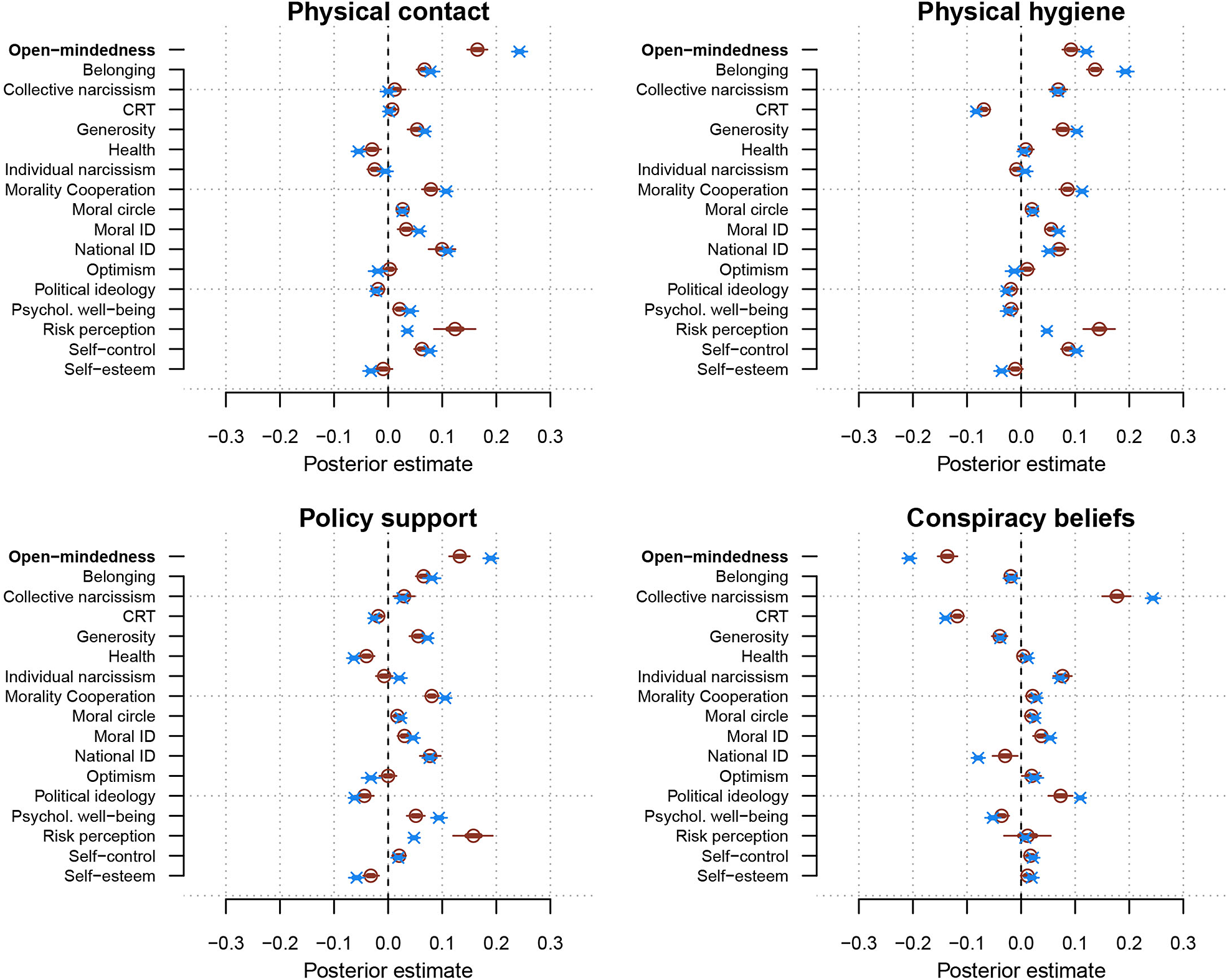
= 0.36, 95% CI = [0.36, 0.37]. All model coefficients are shown in Figure 2.
$R^2$
= 0.36, 95% CI = [0.36, 0.37]. All model coefficients are shown in Figure 2.
Red dots show the posterior mean regression coefficients (population-level estimates) from a multivariate multilevel model that included competing predictors, showing open-mindedness (full scale) together with other social and moral psychological measures predicting health-related outcomes and conspiracy beliefs (all z-scored). Blue dots show the estimated partial correlations computed from the reliability disattenuated correlation matrix. Lines indicate 95% credible intervals in both cases.

Open-mindedness predicted all 4 outcome variables (see Table 2 for scale items). Specifically, open-mindedness positively predicted physical contact (
 $\mathit {b} = 0.17$
, 95% CI = [0.15, 0.18]), physical hygiene (
$\mathit {b} = 0.17$
, 95% CI = [0.15, 0.18]), physical hygiene (
 $\mathit {b}$
= 0.092, 95% CI = [0.076, 0.11]), and policy support (
$\mathit {b}$
= 0.092, 95% CI = [0.076, 0.11]), and policy support (
 $\mathit {b}$
= 0.13, 95% CI = [0.11, 0.15]), and negatively predicted conspiracy beliefs (
$\mathit {b}$
= 0.13, 95% CI = [0.11, 0.15]), and negatively predicted conspiracy beliefs (
 $\mathit {b}$
=
$\mathit {b}$
=
 $-$
0.14, 95% CI = [
$-$
0.14, 95% CI = [
 $-$
0.15,
$-$
0.15,
 $-$
0.12]). Open-mindedness emerged as the strongest predictor of physical contact and tied first with risk perception as the strongest predictor of policy support (
$-$
0.12]). Open-mindedness emerged as the strongest predictor of physical contact and tied first with risk perception as the strongest predictor of policy support (
 $\mathit {b_{diff}}$
= 0.025, 95% CI = [
$\mathit {b_{diff}}$
= 0.025, 95% CI = [
 $-$
0.017, 0.065]). Open-mindedness was second to collective narcissism (Golec de Zavala and Cichocka, Reference Golec de Zavala and Cichocka2012; Stoica and Umbres, Reference Stoica and Umbres2021) as a predictor of rejecting conspiracy beliefs (
$-$
0.017, 0.065]). Open-mindedness was second to collective narcissism (Golec de Zavala and Cichocka, Reference Golec de Zavala and Cichocka2012; Stoica and Umbres, Reference Stoica and Umbres2021) as a predictor of rejecting conspiracy beliefs (
 $\mathit {b_{diff}}$
= 0.041, 95% CI = [0.0068, 0.072]), and was third to risk perception (
$\mathit {b_{diff}}$
= 0.041, 95% CI = [0.0068, 0.072]), and was third to risk perception (
 $\mathit {b_{diff}}$
= 0.053, 95% CI = [0.019, 0.086]) and belonging (
$\mathit {b_{diff}}$
= 0.053, 95% CI = [0.019, 0.086]) and belonging (
 $\mathit {b_{diff}}$
= 0.045, 95% CI = [0.022, 0.068]) in predicting physical hygiene. However, given the imperfect reliability of the scales used, some associations in the multiple regression model may be disproportionately accentuated. To ensure that this did not affect the conclusions drawn, we next estimated partial correlations from the disattenuated correlation matrices computed earlier. Doing so altered several of the associations, especially between predictor variables and conspiracy beliefs, but importantly did not affect the ordinal conclusions drawn (see Figure 2).
$\mathit {b_{diff}}$
= 0.045, 95% CI = [0.022, 0.068]) in predicting physical hygiene. However, given the imperfect reliability of the scales used, some associations in the multiple regression model may be disproportionately accentuated. To ensure that this did not affect the conclusions drawn, we next estimated partial correlations from the disattenuated correlation matrices computed earlier. Doing so altered several of the associations, especially between predictor variables and conspiracy beliefs, but importantly did not affect the ordinal conclusions drawn (see Figure 2).
Previous work with the same dataset has highlighted the predictive power of national identity for public health behaviors (Van Bavel et al., Reference Van Bavel, Cichocka, Capraro, Sjåstad, Nezlek, Pavlović, Alfano, Gelfand, Azevedo, Birtel, Cislak, Lockwood, Ross, Abts, Agadullina, Aruta, Besharati, Bor, Choma and Boggio2022), and our analysis replicates that result. However, we also observe that open-mindedness had a stronger association with the outcome variables compared to national identity (physical contact
 $\mathit {r_{diff}}$
= 0.13, 95%
$\mathit {r_{diff}}$
= 0.13, 95%
 $\mathit {CI_{diff}}$
= [0.11, 0.16]; physical hygiene
$\mathit {CI_{diff}}$
= [0.11, 0.16]; physical hygiene
 $\mathit {r_{diff}}$
= 0.069, 95%
$\mathit {r_{diff}}$
= 0.069, 95%
 $\mathit {CI_{diff}}$
= [0.048, 0.089]; policy support
$\mathit {CI_{diff}}$
= [0.048, 0.089]; policy support
 $\mathit {r_{diff}}$
= 0.11, 95%
$\mathit {r_{diff}}$
= 0.11, 95%
 $\mathit {CI_{diff}}$
= [0.092, 0.13]; conspiracy beliefs
$\mathit {CI_{diff}}$
= [0.092, 0.13]; conspiracy beliefs
 $\mathit {r_{diff}}$
=
$\mathit {r_{diff}}$
=
 $-$
0.13, 95%
$-$
0.13, 95%
 $\mathit {CI_{diff}}$
= [
$\mathit {CI_{diff}}$
= [
 $-$
0.15,
$-$
0.15,
 $-$
0.11]; computed from partial correlation matrix). Thus, these 2 variables seem to be important—but independent—predictors of public health during a pandemic.
$-$
0.11]; computed from partial correlation matrix). Thus, these 2 variables seem to be important—but independent—predictors of public health during a pandemic.
We next investigated the extent to which open-mindedness emerged as a consistent predictor across countries taking 3 different analytical approaches.
First, we examined the variation in per-country coefficients from the multivariate multilevel model just presented. We found similar levels of variation in the effects of open-mindedness across all 4 predictors (physical hygiene:
 $\mathit {b_{sd}}$
= 0.07, 95% CI = [0.05, 0.10]; physical contact:
$\mathit {b_{sd}}$
= 0.07, 95% CI = [0.05, 0.10]; physical contact:
 $\mathit {b_{sd}}$
= 0.08, 95% CI = [0.06, 0.11]; policy support:
$\mathit {b_{sd}}$
= 0.08, 95% CI = [0.06, 0.11]; policy support:
 $\mathit {b_{sd}}$
= 0.09, 95% CI = [0.06, 0.12]; and conspiracy beliefs:
$\mathit {b_{sd}}$
= 0.09, 95% CI = [0.06, 0.12]; and conspiracy beliefs:
 $\mathit {b_{sd}}$
= 0.16, 95% CI = [0.11, 0.22]). The model estimated per-country coefficients from the model are presented in Figure 3 in the Supplementary Material.
$\mathit {b_{sd}}$
= 0.16, 95% CI = [0.11, 0.22]). The model estimated per-country coefficients from the model are presented in Figure 3 in the Supplementary Material.
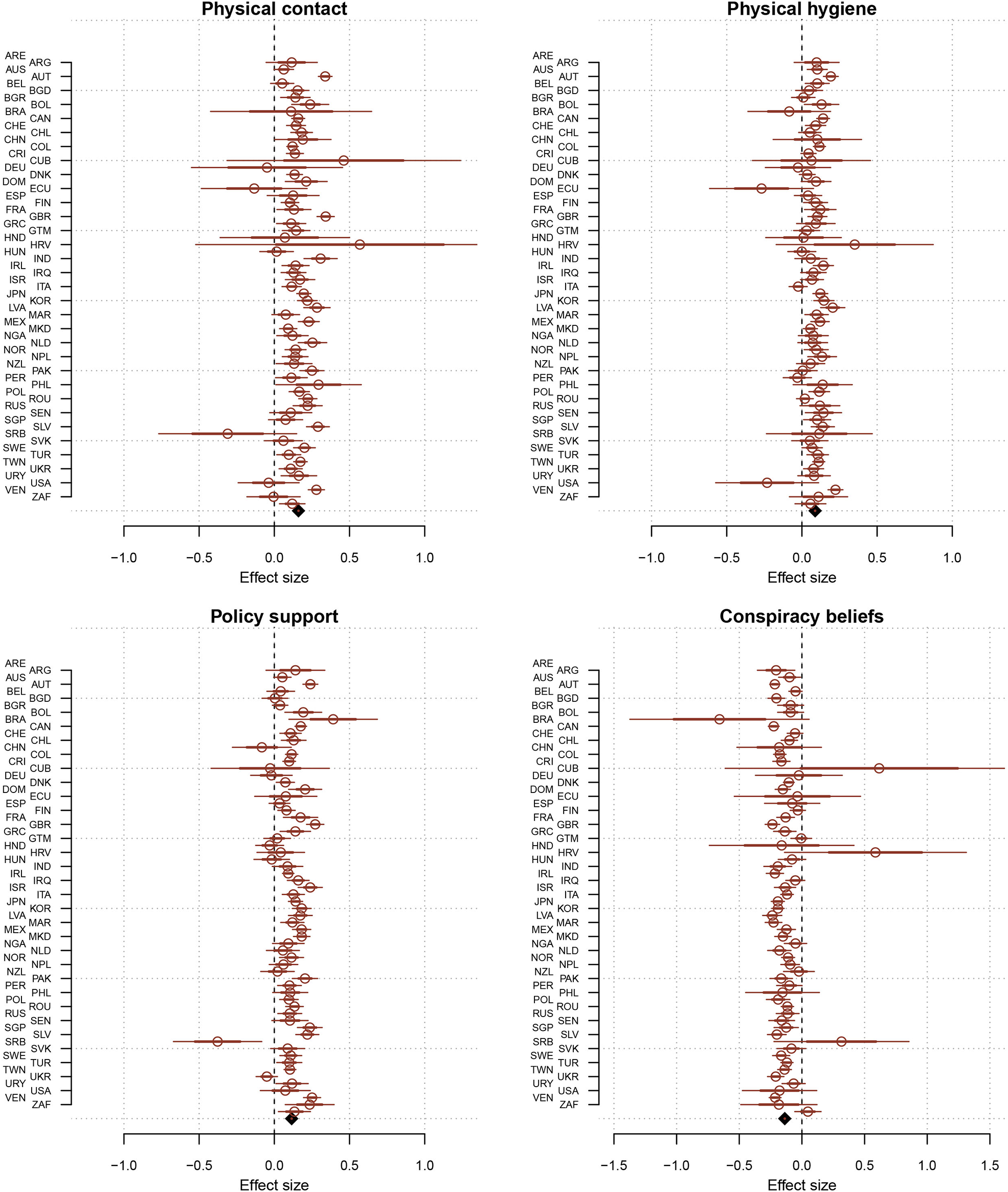
Forest plots showing per-country estimates of the effect of open-mindedness (full scale) from single-level multiple regression models on each of the 4 outcome measures adjusting for all social and moral psychology predictor variables, together with the meta-analytic estimate (rhomboid, bottom of each plot). Thick lines represent the standard error and thin lines the 95% standard normal confidence interval.

Second, we fit an alternative cluster mean-centered model where predictor variables were entered in 2 ways—once where each predictor value was centered around its country mean and once again using each predictor’s country mean centered on the grand mean (Enders and Tofighi, Reference Enders and Tofighi2007). This approach separates participant and country variation and full results are presented in Tables 5–8 in the Supplementary Material. For our purposes, the country mean-centered variables are estimates of the average effect of persons’ open-mindedness on the 4 outcome variables. Our results showed consistent estimates with those presented earlier (physical contact
 $\mathit {b_{cmc}}$
= 0.15, 95% CI = [0.13, 0.17]; physical hygiene
$\mathit {b_{cmc}}$
= 0.15, 95% CI = [0.13, 0.17]; physical hygiene
 $\mathit {b_{cmc}}$
= 0.081, 95% CI = [0.065, 0.096]; policy support
$\mathit {b_{cmc}}$
= 0.081, 95% CI = [0.065, 0.096]; policy support
 $\mathit {b_{cmc}}$
= 0.12, 95% CI = [0.098, 0.14]; and conspiracy beliefs
$\mathit {b_{cmc}}$
= 0.12, 95% CI = [0.098, 0.14]; and conspiracy beliefs
 $\mathit {b_{cmc}}$
=
$\mathit {b_{cmc}}$
=
 $-$
0.12, 95% CI = [
$-$
0.12, 95% CI = [
 $-$
0.14,
$-$
0.14,
 $-$
0.11]).
$-$
0.11]).
Finally, to further address country heterogeneity, we also fit random-effects meta analytical models to regression estimates from single-level multiple regression models using the same predictor variables as above.Footnote
2
The results showing the single-level estimates and the meta analytic estimates are shown in Figure 3. The resulting meta-analytic estimates were again consistent with our previously reported ones (physical contact:
 $\mathit {b_{meta}}$
= 0.16, 95% confidence interval = [0.14, 0.18]; physical hygiene:
$\mathit {b_{meta}}$
= 0.16, 95% confidence interval = [0.14, 0.18]; physical hygiene:
 $\mathit {b_{meta}}$
= 0.088, 95% CI = [0.072, 0.10]; policy support:
$\mathit {b_{meta}}$
= 0.088, 95% CI = [0.072, 0.10]; policy support:
 $\mathit {b_{meta}}$
= 0.12, 95% confidence interval = [0.096, 0.13]; and conspiracy beliefs:
$\mathit {b_{meta}}$
= 0.12, 95% confidence interval = [0.096, 0.13]; and conspiracy beliefs:
 $\mathit {b_{meta}}$
=
$\mathit {b_{meta}}$
=
 $-$
0.14, 95% confidence interval = [
$-$
0.14, 95% confidence interval = [
 $-$
0.16,
$-$
0.16,
 $-$
0.12]). To estimate the impact of heterogeneity of the observed effects, we report prediction intervals (PIs) which capture a likely span of effects for future studies (Borenstein, Reference Borenstein2023; Borenstein et al., Reference Borenstein, Higgins, Hedges and Rothstein2017). Only for policy support was there a slight overlap with 0 for the PIs, indicating some uncertainty in the directional stability of the effect on this analysis. The PIs for all 4 outcome measures were as follows: for physical contact, 95% PI = [0.028, 0.29]; for physical hygiene, 95% PI = [0.0026, 0.17]; for policy support, 95% PI = [
$-$
0.12]). To estimate the impact of heterogeneity of the observed effects, we report prediction intervals (PIs) which capture a likely span of effects for future studies (Borenstein, Reference Borenstein2023; Borenstein et al., Reference Borenstein, Higgins, Hedges and Rothstein2017). Only for policy support was there a slight overlap with 0 for the PIs, indicating some uncertainty in the directional stability of the effect on this analysis. The PIs for all 4 outcome measures were as follows: for physical contact, 95% PI = [0.028, 0.29]; for physical hygiene, 95% PI = [0.0026, 0.17]; for policy support, 95% PI = [
 $-$
0.013, 0.24]; and for conspiracy beliefs: 95% PI = [
$-$
0.013, 0.24]; and for conspiracy beliefs: 95% PI = [
 $-$
0.24,
$-$
0.24,
 $-$
0.032]. In sum, we find the reported associations being remarkably stable across countries and analytical methods in our data.
$-$
0.032]. In sum, we find the reported associations being remarkably stable across countries and analytical methods in our data.
3.2. Exploring sub-scales of open-mindedness
We next explored whether open-mindedness, as measured by our 6 items (Alfano et al., Reference Alfano, Iurino, Stey, Robinson, Christen, Yu and Lapsley2017), could be split into sub-scales. We conducted an exploratory factor analysis that revealed an underlying two-factor solution exhibiting excellent fit (RMSR = 0.0044; RMSEA = 0.0131 (90% confidence interval = [0.0094, 0.017]); TLI = 0.998; and CFI = 0.999). The first factor, which we term learning orientation (M = 8.61, SD = 1.6,
 $\alpha $
= 0.76), captured a generally positive and inquisitive disposition toward gaining information from other people. The second factor, which we term threat orientation (M = 2.77, SD = 2.2,
$\alpha $
= 0.76), captured a generally positive and inquisitive disposition toward gaining information from other people. The second factor, which we term threat orientation (M = 2.77, SD = 2.2,
 $\alpha $
= 0.66), captured overall negative and ego-protective dispositions.
$\alpha $
= 0.66), captured overall negative and ego-protective dispositions.
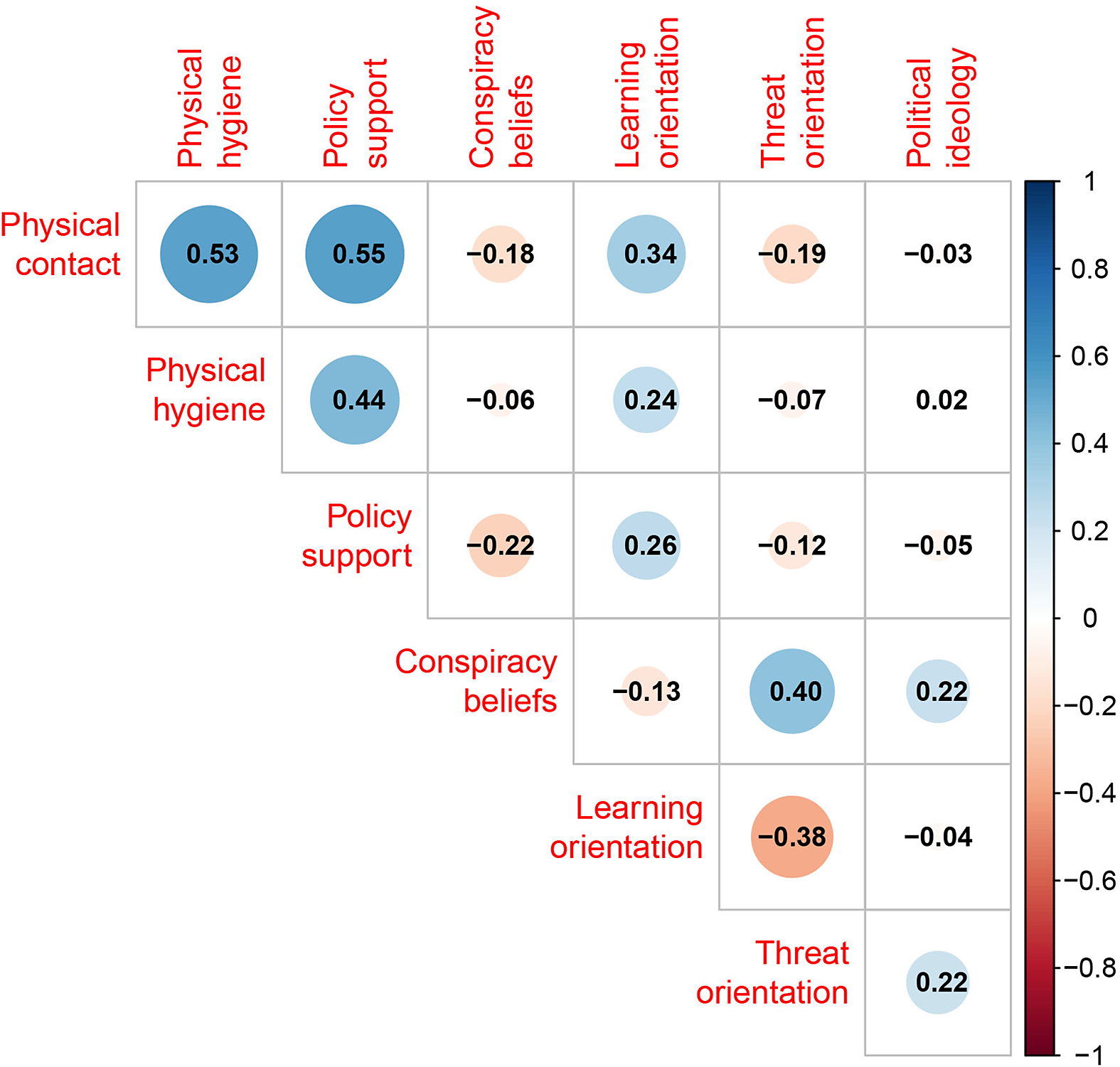
We computed correlations among these exploratory factors of the open-mindedness scale—learning orientation and threat orientation—and the 4 outcome variables in our study. We found that learning orientation was moderately strongly associated with the 3 variables, capturing support for public health measures, while threat orientation exhibited much weaker associations. Specifically, we found that both learning orientation (
 $\mathit {r}$
= 0.34, 95% CI = [0.33, 0.35], see Figure 4) and threat orientation (
$\mathit {r}$
= 0.34, 95% CI = [0.33, 0.35], see Figure 4) and threat orientation (
 $\mathit {r}$
=
$\mathit {r}$
=
 $-$
0.19, 95% CI = [
$-$
0.19, 95% CI = [
 $-$
0.20,
$-$
0.20,
 $-$
0.18]) were associated with physical contact (disattenuated correlation coefficients; for raw correlations, see Figure 3 in the Supplementary Material), as well as physical hygiene (learning orientation:
$-$
0.18]) were associated with physical contact (disattenuated correlation coefficients; for raw correlations, see Figure 3 in the Supplementary Material), as well as physical hygiene (learning orientation:
 $\mathit {r}$
= 0.24, 95% CI = [0.23, 0.25]; threat orientation:
$\mathit {r}$
= 0.24, 95% CI = [0.23, 0.25]; threat orientation:
 $\mathit {r}$
=
$\mathit {r}$
=
 $-$
0.07, 95% CI = [
$-$
0.07, 95% CI = [
 $-$
0.08,
$-$
0.08,
 $-$
0.06]), and policy support (learning orientation:
$-$
0.06]), and policy support (learning orientation:
 $\mathit {r}$
= 0.26, 95% CI = [0.25, 0.27]; threat orientation:
$\mathit {r}$
= 0.26, 95% CI = [0.25, 0.27]; threat orientation:
 $\mathit {r}$
=
$\mathit {r}$
=
 $-$
0.12, 95% CI = [
$-$
0.12, 95% CI = [
 $-$
0.13,
$-$
0.13,
 $-$
0.11]). For conspiracy beliefs, the relationship between the variables was reversed. Threat orientation showed the strongest association (
$-$
0.11]). For conspiracy beliefs, the relationship between the variables was reversed. Threat orientation showed the strongest association (
 $\mathit {r}$
= 0.40, 95% CI = [0.39, 0.41]), while learning orientation showed a much weaker association with conspiracy beliefs (
$\mathit {r}$
= 0.40, 95% CI = [0.39, 0.41]), while learning orientation showed a much weaker association with conspiracy beliefs (
 $\mathit {r}$
=
$\mathit {r}$
=
 $-$
0.13, 95% CI = [
$-$
0.13, 95% CI = [
 $-$
0.14,
$-$
0.14,
 $-$
0.12]). In sum, this suggests that the associations between open-mindedness and public health support versus open-mindedness and conspiracy beliefs may be largely driven by different aspects of the construct.Footnote
3
$-$
0.12]). In sum, this suggests that the associations between open-mindedness and public health support versus open-mindedness and conspiracy beliefs may be largely driven by different aspects of the construct.Footnote
3
Pairwise correlations of the 2 exploratory factors of open-mindedness with the main outcome variables and political ideology. Median posterior estimates are from a multilevel correlation model disattenuated by scale reliabilities.

We also found that self-rated political ideology (higher scores, more right leaning) correlated with both conspiracy beliefs (
 $\mathit {r}$
= 0.22, 95% CI = [0.21, 0.22]) and with the threat orientation factor of open-mindedness (
$\mathit {r}$
= 0.22, 95% CI = [0.21, 0.22]) and with the threat orientation factor of open-mindedness (
 $\mathit {r}$
= 0.21, 95% CI = [0.20, 0.22], see Figure 4).
$\mathit {r}$
= 0.21, 95% CI = [0.20, 0.22], see Figure 4).
4. Discussion
We investigated the relationship between people’s degree of open-mindedness, their support for public health measures, and their degree of belief in COVID-19 conspiracy theories in a large international sample gathered in the early months of the COVID-19 pandemic. We found robust evidence that open-mindedness predicts support for public health measures and disbelief in conspiracy theories.
Our article makes 2 main contributions to understanding the relationship between open-mindedness and socially relevant beliefs and behaviors. First, in line with our preregistered hypotheses, we found that open-mindedness positively correlated with support for 3 different public health measures and negatively correlated with belief in conspiracy theories. Our findings match those from previous studies based on single country samples and significantly bolsters the evidence that these findings replicate cross-culturally across 67 countries. Moreover, these patterns were robust to adding additional predictors to the models to the point where open-mindedness was the largest predictor of all the social and moral variables considered for all dependent variables other than physical hygiene where it remained among the strongest predictors. Additionally, we found highly consistent results of open-mindedness across countries, suggesting a degree of cross-cultural stability in the relationship.
Compared to effect size benchmarks for psychological research, the associations we found are medium to large (Funder and Ozer, Reference Funder and Ozer2019). For conspiracy beliefs, there is a large literature examining its predictors and a recent meta-analysis identified the epistemic variables cognitive reflection (
 $\mathit {r} = -0.17$
) and AOT (
$\mathit {r} = -0.17$
) and AOT (
 $\mathit {r} = -0.25$
) as the strongest negative predictors of conspiracy beliefs, with trust being the largest negative predictor in this meta-analysis at
$\mathit {r} = -0.25$
) as the strongest negative predictors of conspiracy beliefs, with trust being the largest negative predictor in this meta-analysis at
 $\mathit {r} = -0.26$
(Bowes et al., Reference Bowes, Costello and Tasimi2023). In relation to these results, the effect size for open-mindedness reported here stands out as strong (
$\mathit {r} = -0.26$
(Bowes et al., Reference Bowes, Costello and Tasimi2023). In relation to these results, the effect size for open-mindedness reported here stands out as strong (
 $\mathit {r} = -0.28$
;
$\mathit {r} = -0.28$
;
 $\mathit {r_{disattenuated}} = 0.35$
). The effect size for open-mindedness is also comparable in absolute terms to several of the larger positive predictors found in the meta-analysis. Other effect size estimates we find are also similar to those reported in previous meta-analysis, for example, the association we found between collective narcissism (
$\mathit {r_{disattenuated}} = 0.35$
). The effect size for open-mindedness is also comparable in absolute terms to several of the larger positive predictors found in the meta-analysis. Other effect size estimates we find are also similar to those reported in previous meta-analysis, for example, the association we found between collective narcissism (
 $\mathit {r} = 0.30$
;
$\mathit {r} = 0.30$
;
 $\mathit {r_{disattenuated}} = 0.37$
) in this study is close to the meta-analytic estimate reported (
$\mathit {r_{disattenuated}} = 0.37$
) in this study is close to the meta-analytic estimate reported (
 $\mathit {r} = 0.34$
).
$\mathit {r} = 0.34$
).
Nevertheless, there remain questions concerning how open-mindedness, as assessed in this article, relates to, for example, AOT. AOT refers to how individuals process information and how they search information when making decisions. Having appropriately open-minded dispositions will likely be related to the broader process of AOT and both will likely play a part in protecting individuals from holding conspiratorial beliefs.
Second, exploratory analyses identified 2 factors for open-mindedness. One factor loaded on items emphasizing opportunities to learn from other people, which we termed learning orientation. The other factor loaded on items emphasizing negative effects of interacting with or learning from other people, which we termed threat orientation. Learning orientation was positively associated with the 3 public health measures, while threat orientation was positively associated with belief in conspiracy theories. These findings suggest that different epistemic dispositions, one stemming from seeking out and positively valuing interactions with others and the other stemming from avoiding and devaluing interactions with others, differentially predict support for public health interventions and conspiracy beliefs, respectively. The distinction between the factors largely maps to a broader distinction between intellectual virtues and vices. The open-mindedness scale contrasts open-mindedness (virtue) against arrogance (vice), and the learning and threat orientation factors mirror that contrast (Alfano et al., Reference Alfano, Iurino, Stey, Robinson, Christen, Yu and Lapsley2017). Previous work has found that people who score low on open-mindedness are more likely to accept a range of both medical and non-medical conspiracy theories and fake news (Binnendyk and Pennycook, Reference Binnendyk and Pennycook2022; Meyer and Alfano, Reference Meyer, Alfano, Alfano, Klein and Ridder2022; Stanovich and Toplak, Reference Stanovich and Toplak2023). Furthermore, other work investigating epistemic vices, construed in terms of dispositions to be apathetic about evidence and rigid in one’s beliefs, has found them to be powerful predictors of acceptance of COVID-19 myths (Meyer et al., Reference Meyer, Alfano and de Bruin2024, Reference Meyer, Alfano and De Bruin2024). Again, we found relatively little variation between countries in these effects. Nevertheless, we cannot rule out a more mundane explanation that the separation arises from response biases in positive and negative wordings of the items, particularly a yes-saying bias (see also Figures 4 and 5 in the Supplementary Material). Future work should aim to replicate these general findings with a balanced scale. Other explanations are also possible for the separation of items in the scale. The threat orientation items are more strongly worded, and endorsement of them could reflect negative attitudes toward experts or authority figures, attitudes which could plausibly covary with endorsement of conspiratorial beliefs. In sum, these findings are exploratory and further investigation is necessary to understand how learning and threat orientation interact with other facets of intellectual humility broadly and with socially important attitudes and behaviors.
4.1. Limitations
This study has limitations which are important to consider when interpreting its results. First, most of the constructs assessed were short for measures. It is possible that internal consistency was lower leading to greater uncertainty in the results.
Second, and related to the previous point, we assess political ideology using a common one-item measure. A single-item measure of ideology has been found to account for approximately 85% of the statistical variance in presidential voting intentions in American National Election studies between 1972 and 2004 (Jost, Reference Jost2006), and it has been used in cross-cultural research as well (Caprara et al., Reference Caprara, Vecchione, Schwartz, Schoen, Bain, Silvester, Cieciuch, Pavlopoulos, Bianchi, Kirmanoglu, Baslevent, Mamali, Manzi, Katayama, Posnova, Tabernero, Torres, Verkasalo, Lönnqvist and Caprara2017; Choma et al., Reference Choma, Hodson, Sumantry, Hanoch and Gummerum2021; Imhoff et al., Reference Imhoff, Zimmer, Klein, António, Babinska, Bangerter, Bilewicz, Blanuša, Bovan, Bužarovska, Cichocka, Delouvée, Douglas, Dyrendal, Etienne, Gjoneska, Graf, Gualda, Hirschberger and van Prooijen2022). However, this does not allow us to richly assess potential differences in how left- and right-wing ideology are construed globally. Ideological measurement is complicated (Costello et al., Reference Costello, Zmigrod and Tasimi2023), and the findings here should be viewed as tentative pending replication with more sophisticated measures.
Third, one important limitation of the current state of research is that, while we are able to measure open-mindedness, there is currently no consensus on how to inculcate it (Porter and Schumann, Reference Porter and Schumann2018; Porter et al., Reference Porter, Schumann, Selmeczy and Trzesniewski2020). This makes it difficult to answer the causal questions about how open-mindedness affects beliefs and behavior. Importantly, the current results are all correlational and we caution against taking our findings to imply straightforward causal relations.
Finally, we used self-reports to assess behavior, rather than measuring behavior directly. Nonetheless, some research suggests good links between self-reported and actual behavior in the context of the COVID-19 pandemic (Gollwitzer et al., Reference Gollwitzer, McLoughlin, Martel, Marshall, Höhs and Bargh2022).
4.2. Conclusion
Our results add to the growing evidence in favor of viewing open-mindedness and intellectual humility broadly as being central dispositions for understanding which individuals adopt socially valuable attitudes and behaviors. These findings seem to contradict worries that people can be too open-minded or that open-mindedness leads to gullibility (Curzer and Gottlieb, Reference Curzer and Gottlieb2019). How can open-mindedness help promote support for public health measure and disbelief in conspiracy theories? One possibility is that open-mindedness, along with intellectual humility generally, promotes information-seeking intentions and behavior (Jongman-Sereno et al., Reference Jongman-Sereno, Hoyle, Davisson and Park2023; Koetke et al., Reference Koetke, Schumann and Porter2022; Krumrei-Mancuso et al., Reference Krumrei-Mancuso, Haggard, LaBouff and Rowatt2020; Ryu et al., Reference Ryu, Olcaysoy Okten, Gollwitzer and Oettingen2023). This information-seeking behavior then has spillover effects on the likelihood of adopting accurate and socially beneficial beliefs. As such, people who score high on this trait are more closely aligned to scientific consensus in their belief systems. The items that make up the learning orientation factor identified all share a narrow focus on learning attitudes rather than performance or assessments of knowledge. Should future research uncover a causal relationship, the global patterns found here would suggest that investigating the degree to which open-mindedness can be cultivated and the timescales required to reliably shift it will be an important research priority.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/jdm.2026.10033.
Funding statement
This research was made possible through the support of 2 grants from the John Templeton Foundation (Grant Nos. 61378 and 62631). The opinions expressed in this publication are those of the authors and do not necessarily reflect the views of the John Templeton Foundation or the Australian Research Council. P.P. was also supported by Swedish Research Council grant 2020-02584.
Competing interests
The authors declare none.




 Open access
Open access