



Impact statement
The study fills a significant gap in understanding the prevalence of psychological distress among female and male emerging adult students in coastal Karnataka. The study also assessed the various factors associated with psychological distress among both groups, including sociocultural and economic factors. The study setting has its cultural uniqueness, including rural–urban communities, coastal areas and different sociocultural backgrounds.
The study highlights that the prevalence of psychological distress was 32.58% among female participants and was 20.19% among male participants. These results highlight the need for gender-sensitive interventions in association with mental health issues, and they will contribute to promoting overall well-being, as mentioned in Sustainable Development Goal (SDG) 3.4. Female participants studied in the second or third year of college had higher psychological distress, which demands the need for educational institutions to have mental health programs. Adverse childhood experiences and substance use among the participants also acted as a risk factor for developing psychological distress, which is a global issue and needs to be addressed effectively. The research gap in the association between adverse childhood experiences, psychological distress and addiction is an area that requires further exploration.
Introduction
Psychological distress, a broad term that includes symptoms of general stress, depression, posttraumatic stress disorder and anxiety (Zhu et al., Reference Zhu, Jha, Shutta, Huang, Balasubramanian, Clish, Hankinson and Kubzansky2022), has widely been recognized as a significant public health concern among emerging adults in the recent past (Pilar Matud et al., Reference Pilar Matud, Díaz, Bethencourt and Ibáñez2020; Hockey et al., Reference Hockey, Rocks, Ruusunen, Jacka, Huang, Liao, Aune, Wang, Nie and O’Neil2022). Emerging adulthood, spanning 18 to 25 years, is a distinct phase in each individual’s life marked by self-exploration, identity exploration, instability, optimism about the future and the shift from adolescence to adulthood (Arnett, Reference Arnett2000).
Whereas gender in the context of emerging adulthood refers to the socially developed roles, attributes and behaviors that society considers appropriate, generally categorized as male or female, rather than their biological sex. These gender roles and identities are shaped by cultural norms, expectations and socialization processes. These characteristics can increase their vulnerability to psychological distress (Matud et al., Reference Matud, Ibáñez, Hernández-Lorenzo and Bethencourt2023; Conde et al., Reference Conde, Sousa, Silva, Souto, Fernandes and Ferreira2024).
Supporting these factors, global studies found a prevalence of 57% for psychological distress among youth, with 24.6% at mild psychological distress, 18% with moderate psychological distress and 14.4% had severe psychological distress (Anyanwu, Reference Anyanwu2023). While another study reported the prevalence of depression, stress and anxiety was 26.2% (10% mild, 7.4% moderate, 3.9% severe and 4.9% very severe), 29.7% (12.1% mild, 9.7% moderate, 5.8% severe and 2.1% very severe) and 39.9% (10.7% mild, 16% moderate, 4.2% severe and 9% very severe), respectively (Ismail et al., Reference Ismail, Lee, Sutrisno Tanjung, Ahmad Jelani, Abdul Latiff, Abdul Razak and Ahmad Shauki2021).
In India, a study conducted across tier-1 cities in the country (Delhi, Hyderabad, Pune, Chennai, Ahmedabad, Bangalore, Kolkata, Mumbai) found a higher prevalence of psychological distress, with 63.8% reporting moderate distress and 6.8% of emerging adults reporting high distress (Suresh and Dar, Reference Suresh and Dar2025). Another study conducted in southern India reported 34.8% prevalence of psychological distress (TS et al., Reference TS, Rani, Menon, CR, Revamma, Jose, KS, Kishore, Thennarasu and Sivasankaran Nair2017). Mild and moderate psychological distress have important practical effects as they are linked to a greater likelihood of disrupting day-to-day functioning and may lower quality of life. To prevent those symptoms from developing into severe psychological distress, early intervention is needed (McLachlan and Gale, Reference McLachlan and Gale2018).
Many research highlights various sociocultural aspects, such as gender, substance use, type of family and level of education, that were linked to the higher prevalence of psychological distress among emerging adults (Matud et al., Reference Matud, Ibáñez, Hernández-Lorenzo and Bethencourt2023; Mirzaei-Alavijeh et al., Reference Mirzaei-Alavijeh, Najafi, Veis, Moradinazar, Farasati and Jalilian2025). Moreover, adverse childhood experiences (ACEs) and the use of substances were identified as significant risk factors for psychological distress among emerging adults (Tzouvara et al., Reference Tzouvara, Kupdere, Wilson, Matthews, Simpson and Foye2023; Remesan et al., Reference Remesan, Chandra Sekaran, Poojari, Jothikaran, Lakshmi and Ashok2025a).
Additionally, studies also report various gender related pathways to psychological distress. Low decision-making opportunities among women appear as a prominent gendered stressor (Bilodeau et al., Reference Bilodeau, Marchand and Demers2020). Women also report poorer self-esteem than men, which heightens their vulnerability to depression and anxiety, with self-esteem, social support and sleeplessness functioning as significant factors in female pathways (Beauregard et al., Reference Beauregard, Marchand, Bilodeau, Durand, Demers and Haines2018). Men, on the other hand, are more susceptible to the effects of emotional regulation. ACEs have an indirect impact on anxiety and depression in both genders by lowering social support and self-esteem (Zhang et al., Reference Zhang, Xia, Fu, Li, Shi and Yang2025).
In addition, the United Nations Sustainable Development Goals (SDGs) outline global priorities that align with the growing concern of psychological distress (Votruba et al., Reference Votruba and Thornicroft2016). With the specific goal of reducing mental health issues and early mortality from non-communicable diseases by one-third by 2030, mainly focusing on women, SDG 3.4 places a strong emphasis on enhancing mental health and well-being (Bennett et al., Reference Bennett, Kontis, Mathers, Guillot, Rehm, Chalkidou, Kengne, Carrillo-Larco, Bawah, Dain, Varghese, Riley, Bonita, Kruk, Beaglehole and Ezzati2020). Since social determinants such as inequality, access to education, work and poverty highly impact the mental health of women, addressing psychological distress is also linked to other SDGs (Kirkbride et al., Reference Kirkbride, Anglin, Colman, Dykxhoorn, Jones, Patalay, Pitman, Soneson, Steare, Wright and Griffiths2024). Many studies worldwide indicate that women are more susceptible to psychological distress compared to men (Butterworth et al., Reference Butterworth, Watson and Wooden2020; Dessai et al., Reference Dessai, Kankonker, Desai, Vaz, D’Souza, Kulkarni and Vadivel2024). However, scientific enquiries on the psychological distress among the emerging adults through a gender lens in low and middle-income countries, including India has been inadequate.
In accordance with the stress diathesis model, psychological distress is caused by a combination of environmental stressors as well as individual vulnerabilities (Colodro-Conde et al., Reference Colodro-Conde, Couvy-Duchesne, Zhu, Coventry, Byrne, Gordon, Wright, Montgomery, Madden, Ripke, Eaves, Heath, Wray, Medland and Martin2017). The risk of psychological distress among emerging adults in India can be elevated due to an array of external stressors like academic pressure, familial expectations and socioeconomic problems, as well as psychological histories such as ACEs or personality traits (Giano et al., Reference Giano, Ernst, Snider, Davis, O’Neil and Hubach2021; Matud et al., Reference Matud, Ibáñez, Hernández-Lorenzo and Bethencourt2023). This model emphasizes that stressors and vulnerabilities work together in affecting mental health outcomes rather than either one alone causing distress. This interaction underscores the significance of addressing sociocultural issues and provides a valuable framework for examining how various factors contribute to psychological distress among emerging adults (Taylor and Treur, Reference Taylor and Treur2023).
A notable scarcity of research examining psychological distress among emerging adults in India, particularly in the coastal Karnataka’s rural–urban groups within various sociocultural contexts. These include gender roles, parental control fueled by cultural norms and societal expectations, which often heighten distress (Bhat et al., Reference Bhat, Amaresha, Kodancha, John, Kumar, Aiman, Jain and Cherian2018). Additionally, the perspective about mental health concerns in this region is also influenced by cultural beliefs, such as supernatural forces. These beliefs often delay treatment and raise stigma, resulting in social isolation and discrimination (Hegde and Karkal, Reference Hegde and Karkal2022). Furthermore, research exploring the factors such as ACEs and substance use associated with psychological distress are limited. Specifically in the Indian context, comparing these factors between genders leave a significant gap in understanding the underlying risk and protective factors.
Against this background, the current study aimed at understanding the prevalence and determinants of psychological distress among female and male emerging adult college students in Udupi district of Karnataka state in India. The study hypothesized that the prevalence of psychological distress would be higher among female participants in comparison with male participants. In keeping with existing literature, the study also hypothesized that adverse childhood experiences would emerge as a major determinant of psychological distress across both genders.
Methods
Participants and procedure
This cross-sectional study was conducted among undergraduate colleges affiliated with Mangalore University in the Udupi district, Karnataka, India. All procedures involving human participants were approved by the Institutional Ethics Committee of Kasturba Medical College and Kasturba Hospital, Manipal, Karnataka, India (IEC1:378/2022). The Registrar of Mangalore University approved the research, allowing it to be carried out in the associated colleges located in the Udupi district. Permissions were secured from all participating colleges involved in data collection. Data collection occurred between June and October 2023, targeting emerging adults enrolled in undergraduate courses.
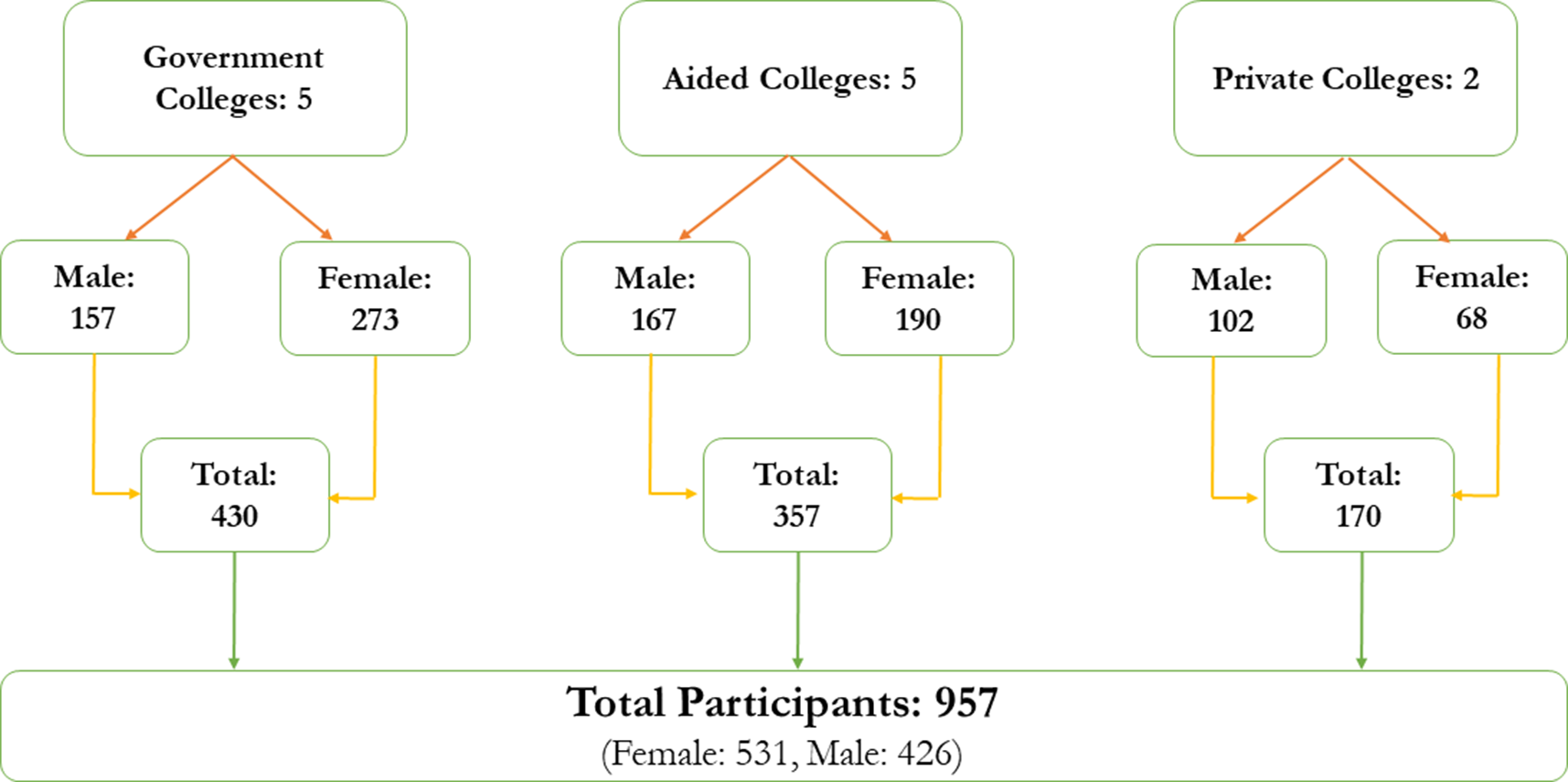
A stratified sampling approach was adopted by classifying colleges into three categories: government (fully funded and managed by the government), aided (private educational institution that receives financial support, such as grants, from the government for operational costs) and private (educational institutions owned and operated by private organizations or individuals). Using the university’s website, a comprehensive list of 12 government colleges, 10 aided colleges and 12 private colleges in the district was prepared. From this pool, five government colleges, five aided colleges and two private colleges were selected through simple random sampling, with consideration given to the variety of academic streams and proportional student representation.
For determining the sample size, an initial calculation yielded 385 participants. However, the finite population correction was applied since the target population was estimated at around 18,000 students. Additionally, the adjusted calculation incorporated a design effect of two and an anticipated 20% non-response rate, leading to a revised sample size of 944. With approval from the selected institutions, data were gathered across various academic streams, including science, arts and commerce, treating each classroom as a sampling cluster. These classrooms were randomly selected based on different academic streams and representation of first year, second year and third year. Every student who was present in the selected classes at the time of data collection participated, and there were no missing values for any of the variables analyzed. Written informed consent was obtained from all the participants prior to data collection. Equal representation of female and male participants was ensured during data collection. On average, each classroom comprised 60–70 emerging adults. Responses were obtained from 957 students, aligning with the cluster sampling strategy employed (Figure 1).
Sample distribution (Remesan et al., Reference Remesan, Sekaran, Jaihind Jothikaran, Goel and Ashok2025b).

Measures
Sociodemographic pro-forma
The data were collected using a sociodemographic pro forma designed to capture the respondents’ key socio-economic and cultural characteristics. The variables included age (categorized as 18–20 years and 21–25 years), year of study (first, second or third year) and type of educational institution (aided, government or private). The stream of study was classified into arts, science and commerce. Information was also gathered on living arrangements (living with parents or others), types of family (nuclear or joint/extended) and family’s economic status (above or below the poverty line). Additional details included religion, number of siblings, birth order and primary caregiver during the first five years of life. The pro forma further captured the current marital status of parents and the participants’ substance use patterns during the COVID-19 pandemic, such as whether use was initiated, increased or decreased, along with substance use among family members and peer groups.
The Kessler Psychological Distress Scale (K10)
The scale was used to assess the psychological distress among the participants (Kessler, Reference Kessler2002). The 10-question survey on psychological distress enquires about symptoms of depression and anxiety faced by participants in the last one month, culminating in an aggregate distress score. The cumulative psychological distress score of the Kessler Scale is calculated by summing the values assigned to each participant’s response. Scores range from 10 to 50. According to this scale, a score below 20 suggests that a participant is likely in a stable psychological state. Scores from 20 to 24 are likely to have a mild disorder, 25 to 29 are likely to have a moderate disorder and 30 to 50 are likely to have a severe disorder.
The World Health Organization Alcohol, Smoking and Substance Involvement Screening Test version three (WHO ASSIST)
According to WHO, “the WHO ASSIST tool focused on substance involvement among emerging adults. The substances included alcohol, tobacco, cannabis, amphetamine-type stimulants, cocaine, inhalants, hallucinogens, sedatives or sleeping pills, opioids and others. These domains helped us to understand the substance use prevalence, and the total score of each domain guided our understanding of the emerging adults at moderate risk and high risk of health and other issues, such as social, legal, financial and relationship issues, due to the participants’ pattern of substance use. Higher scores for each substance indicated a higher risk. For alcohol, scores from 0 to 10 represented a low-risk group, 11–26 represented a moderate-risk group and scores of 27 and more represented a high-risk group. For all the other substances, scores from 0 to 3 were considered low risk, 4–26 were considered moderate risk and 27 and above were considered high-risk groups” (WHO, 2013).
Adverse childhood experiences (ACEs)
“The ACE questionnaire had ten questions, each answered by selecting “yes or no”. The first three questions refer to emotional, physical and sexual abuse, respectively. Questions 4 and 5 assess emotional and physical neglect, and 6–10 refer to household dysfunctions of the participants” (Felitti et al., Reference Felitti, Anda, Nordenberg, Williamson, Spitz, Edwards, Koss and Marks1998). Surveys were administered in both English and Kannada languages, with the Kannada version undergoing reverse translation to ensure instrument reliability and consistency.
Statistical analysis
Descriptive statistics were computed for all variables. Relationships between variables were examined using chi-square and Fisher’s exact tests, with statistical significance as p < 0.05. Subsequently, univariate and multivariate regression analysis were employed using the Jamovi version 2.4.11 to understand the determinants of psychological distress. The variables that showed significance (p < 0.2) during the univariate analysis were adjusted in the multivariate analysis to determine the major factors associated with psychological distress (Chowdhury and Turin, Reference Chowdhury and Turin2020). Multicollinearity was assessed using variance inflation factors (VIF), and all values were below the standard threshold of five (Akinwande et al., Reference Akinwande, Dikko, Samson, Akinwande, Dikko and Samson2015).
Results
Among the 957 participants, 55.49% were female participants. Among the female participants, 89.1% belonged to 18–20 years of age and 54.2% were studying in the first year of college. The majority of them were studying in government colleges (51.4%) and 50.8% were studying the commerce stream. Also, 80.4% were living with both parents and 71.8% were from nuclear families. Additionally, 78.5% belonged to below the poverty line (INR 27000 per year per household). The majority of them reported that they have one or more siblings (90.6%) and most of them had their mother as homemakers (86.3%). In addition, 96% had their parents as primary caregivers, while 92.3% had their parents currently married.
Among the male participants, 81.7% belonged to the 18–20 years of age and 54.2% were studying in the second or third year of college. The majority of them were studying the commerce stream (63.8%), and 81% were living with both parents. Additionally, 77.2% were from nuclear families, and 73.7% belonged to below the poverty line. Also, 88.7% had one or more siblings and 87.1% had mothers who were homemakers. In addition, 97.9% reported that they had parents as primary caregivers and 92% have their parents currently married. Among those who reported ACEs, 53.59% were female participants. Additionally, among those who reported substance use, 62.21% were male participants.
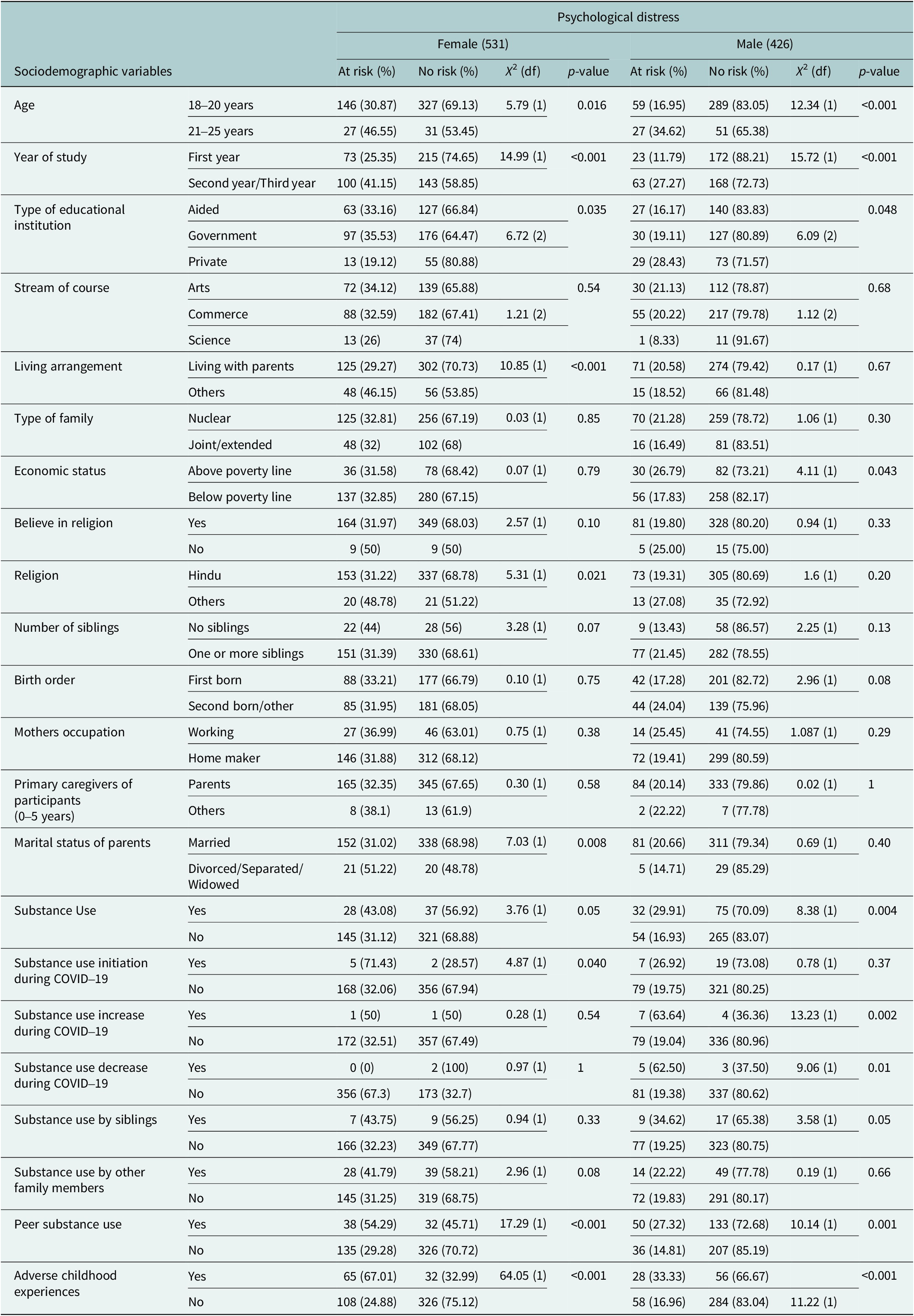
The study found an association between female participants’ psychological distress and the socio-demographic variables. Specifically, age was associated with psychological distress with an effect size of φ = 0.104 and p < 0.05. Also, an association was found between the living arrangement of the female participants and psychological distress, showing an effect size φ = 0.143 and p < 0.001. Additionally, the type of female participants’ educational institution showed an association with psychological distress, with an effect size φ = 0.113 and p < 0.05. In addition, an association was also found between the year in which the female participants were studying and psychological distress (φ = 0.17, p < 0.001).
Further, the religion of the female participants showed an association with psychological distress, with an effect size φ = 0.1 and p < 0.05, while the current marital status of parents also showed an association with psychological distress of female participants (φ = 0.12, p < 0.05). Moreover, substance use initiation among female participants during COVID-19 showed an association with psychological distress, with an effect size φ = 0.1 and p < 0.05. Peer substance use also reflected an association with psychological distress (φ = 0.18, p < 0.001). An association was found between ACEs of female participants with psychological distress, with a moderate effect size (φ = 0.35, p < 0.001).
Among male participants, age was associated with psychological distress, exhibiting an effect size φ = 0.17 and p < 0.001. Additionally, the year of study demonstrated an effect size φ = 0.19 and p < 0.001, showing an association with psychological distress. Moreover, an association was found between economic status and type of educational institute, with an effect size φ = 0.10 and p < 0.05 and Cramér’s V = 0.12, p < 0.05, respectively. Furthermore, substance use was associated with psychological distress (φ = 0.14, p < 0.05), as were increased substance use during COVID-19 (φ = 0.18, p < 0.05) and decreased substance use during this period (φ = 0.15, p < 0.05). In addition, peer substance use (φ = 0.15, p < 0.05) and ACEs (φ = 0.16, p < 0.001) were also shown to be associated with psychological distress (Table 1).
Socio-demographic details of the participants in association with psychological distress (K10) (n = 957)

Notes: At risk: participants having Kessler Psychological Distress Scale (K10) score from 20 and above. No risk: participants having Kessler Psychological Distress Scale (K10) score below 20.
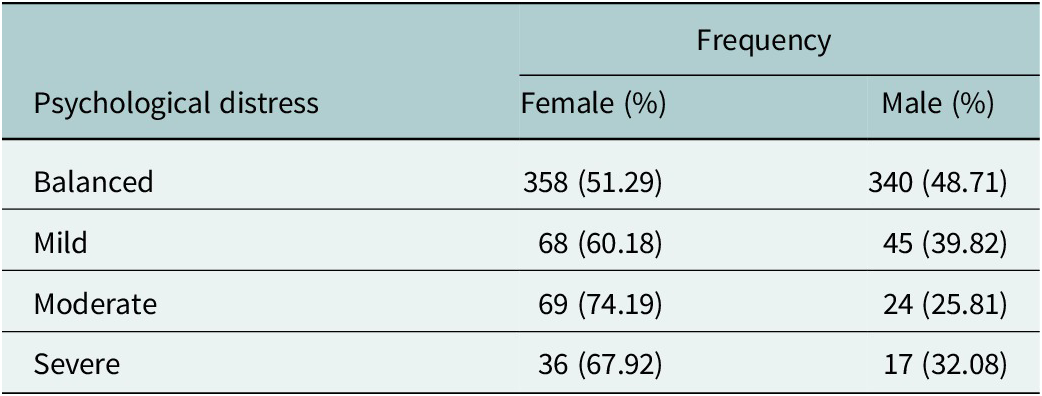
The overall prevalence of psychological distress was 27.06%, with 11.8% likely to have a mild mental disorder, 9.71% likely to have a moderate mental disorder, and 5.53% likely to have a severe mental disorder. Psychological distress was more common among female participants (32.58%) than male participants (20.19%). Among participants with a likelihood of mild mental disorder, 60.18% were female. Among those with a likelihood of moderate mental disorder, 74.19% were female. Similarly, the likelihood of having a severe mental disorder was higher among females, who accounted for 67.92% of this group (Table 2).
Psychological distress (K10) among emerging adults—n = 957 (female = 531, male = 426)

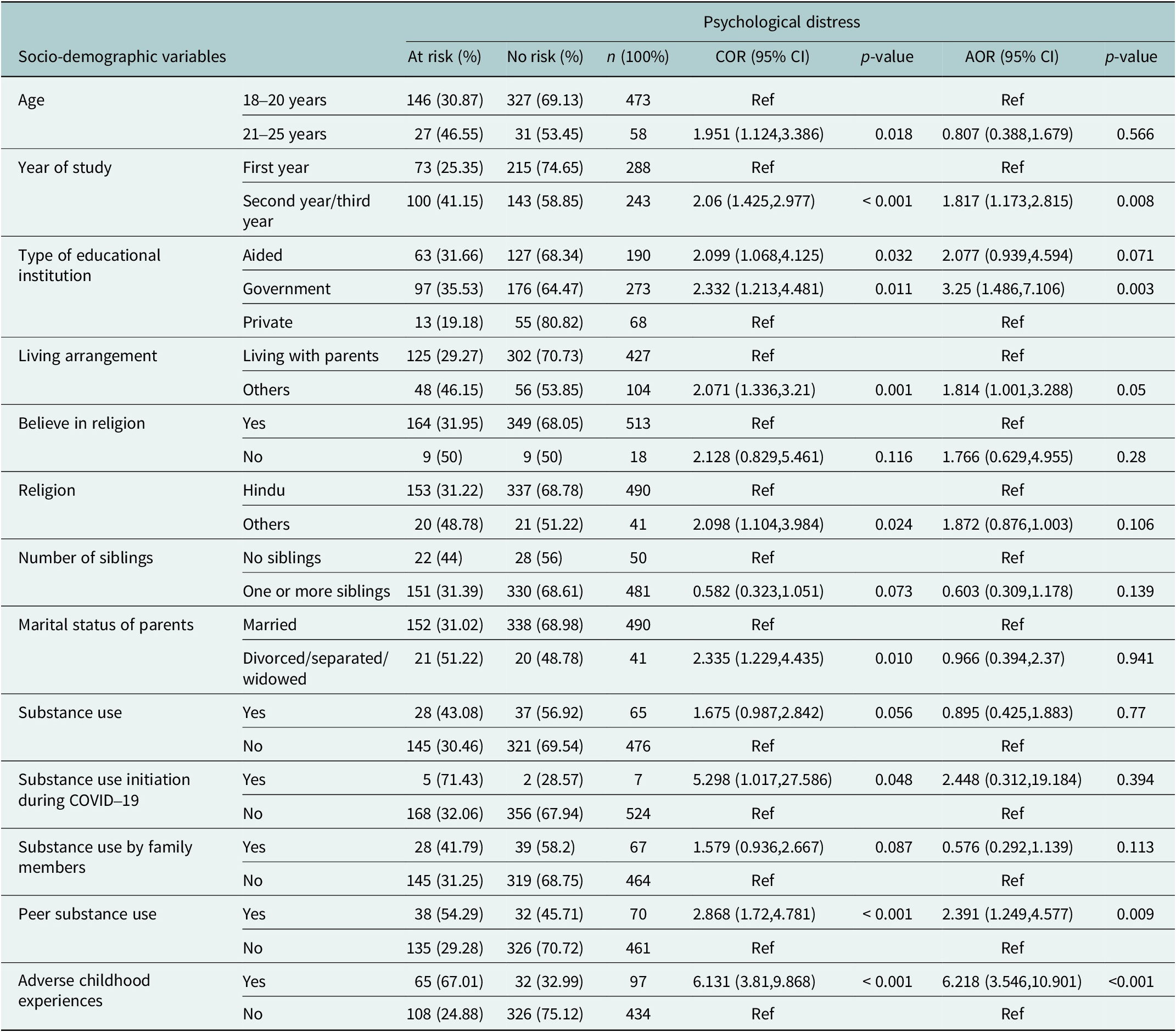
Backward logistic regression was performed to find the predictors of the outcome variable, psychological distress, among female and male participants. Univariate and multivariate analyses for determinants of psychological distress were conducted. For female participants, factors such as age, year in which they are studying, type of their educational institution, their living arrangement, whether they believe in religion, their religion, number of siblings, current marital status of parents, substance use, substance use initiation during COVID-19, substance use by family members, peer substance use and ACEs were adjusted in the multivariate analysis after being shown association in the univariate analysis. Among these, the year in which they are studying, the type of their educational institution, peer substance uses and ACEs showed association in multivariate analysis and crude odds ratio (COR), adjusted odds ratio (AOR) and confidence interval (CI) were reported (Table 3).
Univariate and multivariate analysis for associations of psychological distress (K10) among female participants (n = 531)

Notes: At risk: participants having a Kessler Psychological Distress Scale (K10) score of 20 and above.
No risk: participants having a Kessler Psychological Distress Scale (K10) score below 20.
Abbreviations: AOR: adjusted odds ratio, COR: crude odds ratio, CI: confidence interval.
With reference to female participants studying in the first year of college, those who studied in the second year or third year of college had higher odds of psychological distress (AOR 1.817, 95% CI (1.173, 2.815), p = 0.008). Concerning the type of educational institution the female participants studied, with reference to those who studied in private colleges, those who studied in government colleges had higher odds of psychological distress (AOR 3.25, 95% CI (1.486, 7.106), p = 0.003). Peer substance use was associated with psychological distress among female participants. Participants with peers using substances had higher odds of psychological distress (AOR 2.391, 95% CI (1.249,4.577), p = 0.009) than non-substance-using peers. ACEs were associated with psychological distress as female participants who experienced ACEs had higher odds of psychological distress (AOR 6.218, 95% CI (3.546, 10.901), p < 0.001) with reference to those who never experienced ACEs.
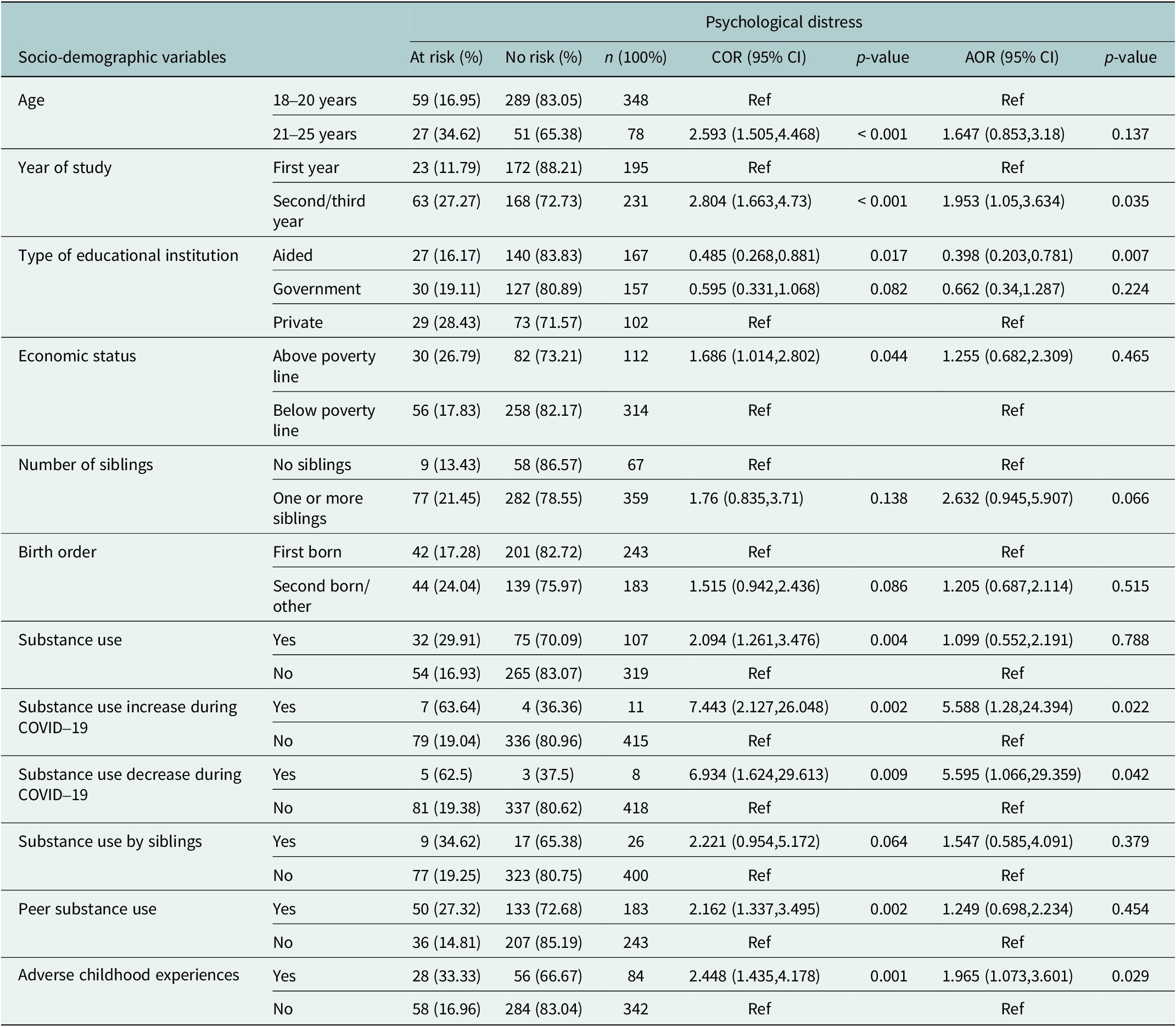
For male participants, factors such as age, year in which they are studying, type of their educational institute, economic status of family, number of siblings, birth order, substance use, increased substance use during COVID-19, reduced use of substances during COVID-19, substance use by siblings, peer substance use and ACEs were adjusted in the multivariate analysis after being shown association in the univariate analysis. Among those, year in which they are studying, type of their educational institute, increased substance use during COVID-19, reduced use of substances during COVID-19 and ACEs showed association in multivariate analysis and crude odds ratio (COR), adjusted odds ratio (AOR) and confidence interval (CI) were reported (Table 4).
Univariate and multivariate analysis for associations of psychological distress (K10) among male participants (n = 426)

Notes: At risk: participants having a Kessler Psychological Distress Scale (K10) score of 20 and above.
No risk: participants having a Kessler Psychological Distress Scale (K10) score below 20.
Abbreviations: AOR: adjusted odds ratio, COR: crude odds ratio, CI: confidence interval.
With reference to male participants studying in the first year of college, those who studied in the second year or third year of college had higher odds of psychological distress (AOR 1.953, 95% CI (1.05, 3.634), p = 0.035). Concerning the type of educational institution the male participants studied, with reference to those who studied in private colleges, those who studied in aided colleges had lower odds of psychological distress (AOR 0.398, 95% CI (0.203, 0.781), p = 0.007). Among male participants, both an increase and a decrease in substance use during the COVID-19 pandemic were associated with a risk of psychological distress compared to those who reported no change or had not initiated substance use prior to the pandemic (AOR 5.588, 95% CI (1.28, 24.394) p = 0.022), (AOR 5.595, 95% CI (1.066, 29.359) p = 0.042), respectively. ACEs were also associated with psychological distress among male participants. Male participants who experienced ACEs had higher odds of psychological distress (AOR 1.965, 95% CI (1.073, 3.601), p = < 0.029) with reference to those who never experienced ACEs.
Discussion
Addressing the gap in data on prevalence and determinants of psychological distress among female and male emerging adult students in coastal Karnataka, the current study found that female participants reported the higher odds of experiencing psychological distress (32.58%) compared to male participants (20.19%), a pattern that is consistently observed in research both globally and within India (Maser et al., Reference Maser, Danilewitz, Guérin, Findlay and Frank2019; Panigrahi et al., Reference Panigrahi, Mohapatra, Shetty, Baby and Singh2021; Viertiö et al., Reference Viertiö, Kiviruusu, Piirtola, Kaprio, Korhonen, Marttunen and Suvisaari2021). Even though multiple studies confirm that women report higher psychological distress (Mommersteeg et al., Reference Mommersteeg, van Valkengoed, Lodder, Juster and Kupper2024; Jamil, Reference Jamil2025), this study advances novelty by focusing on emerging adults.
Particularly in coastal Karnataka, gender roles and parental control based on cultural norms can be a major cause of increased psychological distress (Bhat et al., Reference Bhat, Amaresha, Kodancha, John, Kumar, Aiman, Jain and Cherian2018). Women are expected to uphold family honor, have less autonomy in making decisions and experience stress, including relationship problems and academic challenges, which can also be the reason for heightened psychological distress (Antabe et al., Reference Antabe, Antabe, Sano and Pienaah2025; Shergill and Rathore Hooja, Reference Shergill and Rathore Hooja2025). In addition, studies also reported that females’ ability to understand minute emotional changes than that of males, which may result in underreporting of distress among males (Shi et al., Reference Shi, Yang, Zhao, Chen, Ren and Dai2021). This highlights the need for gender-sensitive approaches in mental health assessment and intervention, which will also help in promoting mental health and well-being, as mentioned in SDG 3.4.
Overall, 27.06% of participants experienced psychological distress, with 9.71% moderate and 5.53% severe mental disorders. This prevalence is similar to a study from coastal Karnataka, India, which reported a rate of 28.5% (Bhat et al., Reference Bhat, Amaresha, Kodancha, John, Kumar, Aiman, Jain and Cherian2018). However, it is notably lower than the 57% prevalence in a global study among 906 students by Anyanwu (Reference Anyanwu2023). These findings suggest that while psychological distress rates may vary across different populations (Nochaiwong et al., Reference Nochaiwong, Ruengorn, Thavorn, Hutton, Awiphan, Phosuya, Ruanta, Wongpakaran and Wongpakaran2021), the results of the current study are consistent with regional data from India.
Compared to participants who had not experienced ACEs, those who experienced ACEs were more at risk of psychological distress, indicating that ACEs function as a major factor associated with psychological distress between both groups. Different studies also report the impact of ACEs on poor mental health outcomes (Tzouvara et al., Reference Tzouvara, Kupdere, Wilson, Matthews, Simpson and Foye2023). The study, by assessing ACEs as a factor associated with psychological distress, fills a critical gap in mental health research in the region, offering targeted insights for tailored interventions.
Moreover, female and male participants studying in their second or third year of college had a higher risk of psychological distress compared to their counterparts in first year of college. This can be associated with existing literature, which reports that academic pressure intensifies as students progress into the final years (Alam et al., Reference Alam, Pratik, Khan, Islam and Hossain2025). Students face higher demands of coursework, specialization, thesis work, career decisions and future uncertainties, which can heighten distress. Additionally, as students get older, increased responsibilities and expectations may further contribute to psychological distress, making upper-year students more vulnerable than their first-year peers (Jaisoorya et al., Reference Jaisoorya, Geetha, Beena, Beena, Ellangovan and Thennarasu2017).
Additionally, with reference to female participants who studied in private colleges, those who studied in government colleges were having higher risk of psychological distress. This finding contrasts with the majority of the existing literature reporting higher psychological distress among students from private colleges (Al-khlaiwi et al., Reference Al-khlaiwi, Habib, Akram, Al-khliwi and Habib2023; Smritikana Mitra Ghosh, Reference Ghosh2016). This could be due to different contextual factors such as the academic environment and the societal background of the participants.
Whereas, with reference to male part,icipants who studied in private colleges, male participants who studied in aided colleges had lesser odds of psychological distress. The results suggest that male participant data aligns with existing literature (Shafiq et al., Reference Shafiq, Nipa, Sultana, Rahman and Rahman2021), exploring social support or academic environments in government colleges in the study area may be valuable, as it contributes to increased distress in female students, countering the pattern reported in other regions.
Among female participants, having peers who used substances was associated with a higher likelihood of experiencing psychological distress, compared to those whose peers did not engage in substance use, but this observation is not reported for male participants. This may reflect differences in socialization and coping strategies and the importance of peer approval and support among females (Yoon et al., Reference Yoon, Yoon, Yoon and Knox2023). The results also suggest that prevention programs should consider these gender differences in addressing the psychological risks associated with substance-using peer groups (Pickering et al., Reference Pickering, Hadwin and Kovshoff2020).
Among male participants, both an increase and a decrease in substance use during the COVID-19 pandemic were associated with a higher risk of psychological distress compared to those who reported no change or had not initiated substance use prior to the pandemic. Substance use among emerging adults was associated with higher levels of psychological distress globally and in India in the literature (TS et al., Reference TS, Rani, Menon, CR, Revamma, Jose, KS, Kishore, Thennarasu and Sivasankaran Nair2017; Connery et al., Reference Connery, McHugh, Reilly, Shin and Greenfield2020). During the pandemic, studies have reported substance use as a maladaptive coping mechanism among emerging adults, which will, in turn, affect their mental health (Romano et al., Reference Romano, Patte, de Groh, Jiang, Wade, Bélanger and Leatherdale2021; Remesan et al., Reference Remesan, Sekaran, Jothikaran and Ashok2023).
The reason for higher psychological distress among those who decreased substance use can be forced or unintentional due to the external constraints, such as lockdown, and loss of access to substances. This may have disrupted routines or coping strategies, resulting in increased distress. Sudden reduction in substance use, especially if not planned or supported, can cause psychological distress due to withdrawal or loss of a familiar coping tool (Layman et al., Reference Layman, Thorisdottir, Halldorsdottir, Sigfusdottir, Allegrante and Kristjansson2022; Korakkottil et al., Reference Korakkottil, Gopal, Sekaran and Ramasamy2025).
In both genders, the associations between sociodemographic variables and psychological distress primarily show small effect sizes, suggesting a moderate but an association with practical implications. Age, year of study, type of educational institution, substance use – including changes during COVID-19, and peer substance use all indicated minor effects, suggesting that these factors marginally but constantly contribute to psychological distress (Roberts et al., Reference Roberts, Rogers, Mason, Siriwardena, Hogue, Whitley and Law2021; Layman et al., Reference Layman, Thorisdottir, Halldorsdottir, Sigfusdottir, Allegrante and Kristjansson2022). The moderate effect size of ACEs in females is associated, indicating a greater practical importance for trauma-informed interventions (Haahr-Pedersen et al., Reference Haahr-Pedersen, Perera, Hyland, Vallières, Murphy, Hansen, Spitz, Hansen and Cloitre2020). These results highlight the need for comprehensive, gender-sensitive approaches among emerging adults, suggesting that although each element alone has a small effect, their combined influence is significant for targeted mental health promotion and intervention.
The study’s results are consistent with the stress-diathesis model, in which ACEs act as a primary diathesis and have a moderate to small effect on psychological distress in emerging adult female and male participants, respectively (Mosley-Johnson et al., Reference Mosley-Johnson, Campbell, Garacci, Walker and Egede2021). These effects are heightened by academic stressors, particularly in the second or third year of study.
Sociodemographic characteristics, including living arrangements, economic condition and type of college, function as intermediate stressors that interact with these vulnerabilities, especially increasing the risk of psychological distress in female participants (Ayad et al., Reference Ayad, Najdi and Senhaji2024). Peer substance use and substance use initiation during COVID-19 are examples of substance use-related variables that served as major environmental triggers that contributed to diathesis (Chacon et al., Reference Chacon, Walia, Allen, Sciancalepore, Tiong, Quick, Mada, Diaz and Rodriguez2021). Gender differences demonstrated that female participants were more vulnerable to social and institutional challenges.
These results highlight the complex ways in which gender, ACEs and substance use interconnect to influence psychological distress in emerging adults. By revealing the adverse effects of these factors on psychological distress among emerging adult female and male participants, the study underscores the need for early, culturally sensitive and multidimensional mental health interventions. Addressing these issues is essential for promoting well-being, reducing inequalities and achieving sustainable development in line with the SDGs.
Conclusion
The study contributed to understanding the necessity for gender-sensitive approaches in youth mental health interventions, which is still not widely recognized in the Indian context. SDG 3.4, which aims to promote mental health and wellbeing, is in line with these findings, which demand gender-responsive and culturally sensitive mental health policies. Gender-sensitive policies should be given importance in mental health initiatives at educational institutions. Normalizing help-seeking behaviors, reducing stigma and boosting access to mental health assistance are vital. The effectiveness of interventions across various populations should be evaluated in future studies. Gender-sensitive programs are also necessary to close the gap between male’s underreporting symptoms and female’s disproportionate burden of psychological distress associated with patriarchal stresses and discrimination (Vigod and Rochon, Reference Vigod and Rochon2020; Shi et al., Reference Shi, Yang, Zhao, Chen, Ren and Dai2021).
Limitation
Even though the current research provides insightful information, it is critical to acknowledge its limits. The sample was restricted to emerging adults who attended undergraduate university programs, which limits the findings’ generalizability and the cross-sectional methodology does not allow for temporality. The scope of future research should be expanded to include emerging adults from different societal sectors, such as those who work or pursue other careers. A further limitation is using self-reported data, where the individuals may underreport psychological distress because of recall biases or social desirability, which could compromise the accuracy of the findings. To overcome these issues, longitudinal research is recommended, which helps to establish a causal relationship between psychological distress and its influencing factors and allows for the assessment of changes over time. By recognizing these shortcomings and implementing the suggestions into practice, future studies can offer a more thorough understanding of psychological distress among emerging adults.
Open peer review
To view the open peer review materials for this article, please visit http://doi.org/10.1017/gmh.2026.10156.
Data availability statement
The authors confirm that the data supporting the findings of this study are available within the article.
Acknowledgements
The authors would like to thank the heads and faculties of the colleges that were part of the study for their valuable time and support in data collection.
Author contribution
Ajith K. Remesan: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Resources, Software, Supervision, Validation, Writing – original draft, Writing – review & editing. Varalakshmi Chandra Sekaran: Conceptualization, Data curation, Formal analysis, Methodology, Resources, Software, Supervision, Validation, Writing – original draft, Writing – review & editing. Teddy Andrews Jaihind Jothikaran: Conceptualization, Methodology, Resources, Software, Supervision, Validation, Writing – review & editing. Anish V Cherian: Conceptualization, Resources, Supervision, Validation, Writing – review & editing. Lena Ashok: Conceptualization, Data curation, Methodology, Resources, Software, Supervision, Validation, Writing – review & editing.
Financial support
I acknowledge the Ministry of Social Justice & Empowerment, Government of India, for providing the fellowship support that enabled me to undertake and complete this research. No. F. 82–44/2020 (SA-III) UGC NFSC JRF funded by Ministry of Social Justice & Empowerment, Government of India.
Competing interests
The authors declare none.
Ethical standard
All procedures involving human participants were approved by the Institutional Ethics Committee of Kasturba Medical College and Kasturba Hospital, Manipal, Karnataka, India (IEC1:378/2022). The Registrar of the Mangalore University approved the research, allowing it to be carried out in the associated colleges located in the Udupi district. Written informed consent was obtained from all the participants prior to the data collection.

 Open access
Open access
Comments
To,
The Editor
Cambridge Prisms: Global Mental Health
Sub: Submission of manuscript for publication
Dear Sir/Madam,
We are pleased to submit our manuscript titled “Gender Differences in Prevalence and Predictors of Psychological Distress among Emerging Adults in Udupi District, Coastal Karnataka: A Cross-Sectional Study” for consideration for publication in the Cambridge Prisms: Global Mental Health journal. In this paper, we explored the prevalence and predictors of psychological distress among emerging adults comparing female and male participants. We believe our findings will resonate well with the journal’s readership and contribute to ongoing discussions in the field. Thank you for considering our manuscript. We look forward to the opportunity to contribute to the journal and are eager to hear your feedback.
On behalf of all the contributors, I will act as guarantor and will correspond with the journal from this point onward.
Prior publication - None
Conflicts of interest -None
• We confirm that neither the manuscript nor any parts of its content are currently under consideration or published in another journal.
• All authors have approved the manuscript and agree with its submission to the Cambridge Prisms: Global Mental Health. We hereby transfer, assign, or otherwise convey all copyright ownership, including any and all rights incidental thereto, exclusively to the journal in the event that such work is published by the journal.
Thanking you,
Yours sincerely,
Corresponding author:
Dr Varalakshmi Chandra Sekaran
Department of Global Public Health Policy and Governance,
Prasanna School of Public Health,
Manipal Academy of Higher Education, Manipal, India.
Email: varalakshmi.cs@manipal.edu | ORCID: http://orcid.org/0000-0003-3319-3075