


Introduction
When a parent is diagnosed with a life-threatening illness, the whole family may be affected and in need of support. However, knowledge about available support for these families remains limited – and in the context of progressive neurological disease almost non-existent – underscoring the importance of comprehensive mapping of existing research to guide future development.
Children of parents with life-threatening illnesses are at increased risk of health problems such as anxiety, depression, stress (Wray et al. Reference Wray, Seymour and Greenley2022; Bergersen et al. Reference Bergersen, Olsson and Larsson2024), and school difficulties (Sieh et al. Reference Sieh, Visser-Meily and Meijer2013), with potential long-term consequences including suicide risk (Ong et al. Reference Ong, Lakoma and Gees Bhosrekar2021). In families affected by fatal progressive neurological diseases, children may struggle with frightening thoughts of loss and change, take on adult responsibilities, and experience social isolation (Malmström et al. Reference Malmström, Öhlén and Jakobsson Larsson2024; Cooper et al. Reference Cooper, Simpson and Dale2025). Their needs may also go unnoticed, as indicated in a study where children of parents with ALS rated their own health as poorer than perceived by their parents (Nilsson et al. Reference Nilsson, Malmström and Nygren2025). Both ill parents and co-parents in these families face a demanding everyday life marked by worry, grief, and uncertainty (Malmström et al. Reference Malmström, Öhlén and Nilsson2025). Parents with a fatal progressive neurological or neuro-oncological disease describe difficulties in balancing their illness and parenting, evoking feelings of guilt and inadequacy due to their reduced emotional or physical presence (Loughan et al. Reference Loughan, Reid and Willis2022; Malmström et al. Reference Malmström, Öhlén and Nilsson2025). Co-parents often carry a dual burden – supporting both the ill parent and the children while grappling with their own difficult emotions (Bergem and Aamotsmo Reference Bergem and Aamotsmo2024; Billaud Feragen et al. Reference Billaud Feragen, Egedal and Kjolaas2025; Malmström et al. Reference Malmström, Öhlén and Nilsson2025). The behavioral, cognitive, and physical changes associated with these diseases – which may occur rapidly – can create complex and multifaceted challenges for the entire family (Masrori and Van Damme Reference Masrori and Van Damme2020; Pender et al. Reference Pender, Pinto-Grau and Hardiman2020; Stoker et al. Reference Stoker, Mason and Greenland2022; Schaff and Mellinghoff Reference Schaff and Mellinghoff2023), including concerns about heredity and disrupted parent–child relationships (Loughan et al. Reference Loughan, Reid and Willis2022; Cooper et al. Reference Cooper, Simpson and Dale2025; Malmström et al. Reference Malmström, Öhlén and Nilsson2025).
Although the need for improved support in families facing a parent’s fatal progressive neurological illness has been acknowledged (Malmström et al. Reference Malmström, Jakobsson Larsson and Nilsson2023, Reference Malmström, Öhlén and Nilsson2025; Billaud Feragen et al. Reference Billaud Feragen, Egedal and Kjolaas2025; Cooper et al. Reference Cooper, Simpson and Dale2025), research on existing interventions in this context remains scarce. Given the limited literature, it is necessary to scope support interventions for families affected by all types of parental life-threatening illness. Here, life-threatening illness refers to conditions with high risk of near-term death, typically involving palliative care needs. This broader approach may allow for a comprehensive mapping of available interventions, providing insight into how support is structured and delivered, as well as into the findings reported across studies. Such mapping is essential for understanding how the needs of children, ill parents, and co-parents have been, and may be, addressed – while also identifying forms of support particularly relevant to families living with progressive neurological disease. With a special interest in informing the development of tailored support for this group, the aim of this scoping review was to systematically map support interventions for families in which a parent has a life-threatening illness.
Methods
Design
This scoping review followed the methodological framework developed by Arksey and O’Malley (Reference Arksey and O’Malley2005), refined by Levac et al. (Reference Levac, Colquhoun and O’Brien2010), and was reported in accordance with the PRISMA-ScR checklist (Tricco et al. Reference Tricco, Lillie and Zarin2018).
Search strategy
The literature search began with a systematic database search – conducted in collaboration with an expert librarian – completed on 12 February 2025, followed by a manual screening of reference lists. The databases searched were PubMed, CINAHL, PsycINFO, and Web of Science. The search was structured into 4 search blocks: type of support intervention, children, family relations, and diagnoses. Filters for publication year (2013–2025) and peer reviewed articles, when applicable, were used (Supplementary File 1).
Eligibility criteria
The review included original peer-reviewed articles on support interventions for families where a parent had a life-threatening illness. While progressive neurological diseases were initially of particular interest, all incurable diseases with fatal outcomes were eligible. No strict diagnostic list or time-based definition was applied (see Supplementary File 1 for full search terms). The term “children” refers to individuals in the role of a child to a parent with a life-threatening illness, including minors, adolescents, and young adults up to the age of 25 years. The decision to include interventions targeting young adults aged 19–25, despite no longer being legally children, was based on evidence and clinical experience showing that many in this age group continue to live at home when a parent becomes life-threateningly ill. In such situations, they often take on caring roles and remain actively involved in family life (Kavanaugh et al. Reference Kavanaugh, Cho and Fee2020b, Reference Kavanaugh, Henning and Mochan2021). Furthermore, research suggesting that brain development is not fully completed until the mid-20s supports the relevance of including this group within the broader definition of “children” used in this study (Sawyer et al. Reference Sawyer, Azzopardi and Wickremarathne2018).
Inclusion criteria were: parents with a life-threatening illness (as defined by the search strategy; Supplementary File 1), co-parents, children aged ≤25 years; randomized controlled trials (RCTs), non-RCTs, interventions evaluated quantitatively or qualitatively; pilot and feasibility studies, brief reports, and study protocols. One study protocol was excluded due to overlap with included publications. The inclusion period covered January 2013 to February 2025 to capture the most recent and relevant research.
Exclusion criteria included non-English publications, reviews, case studies, and gray literature (e.g., reports, dissertations) to ensure scientific quality through peer review.
Selection of sources of evidence
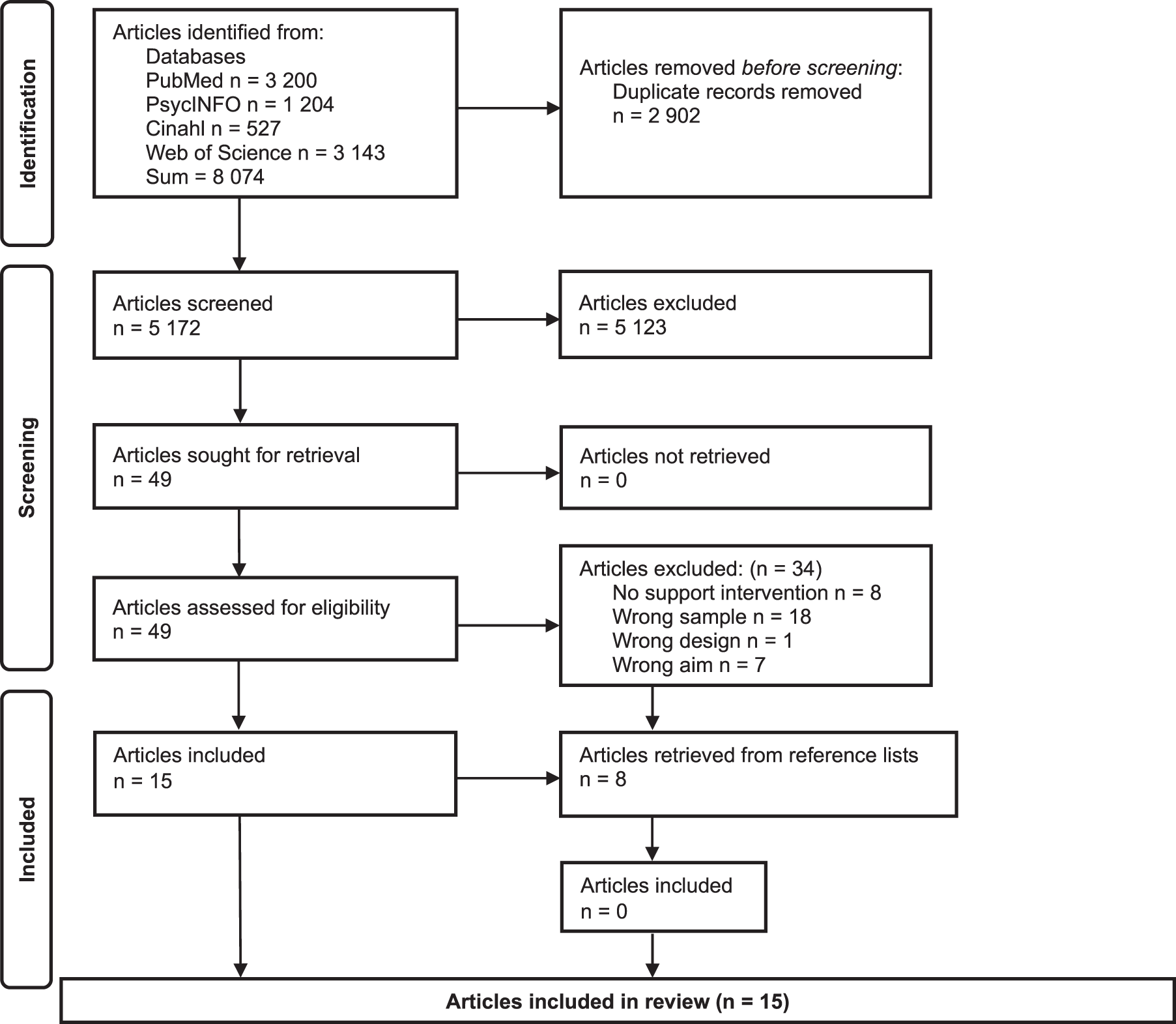
A total of 8074 citations were identified through the database search, of which 5172 remained after deduplication. A blinded screening of titles and abstracts, independently performed by the authors and 2 master’s students in the Rayyan software (Ouzzani et al. Reference Ouzzani, Hammady and Fedorowicz2016) yielded 49 potentially relevant citations. Following full-text reading, 15 articles met the eligibility criteria and were selected for inclusion. Manual screening of reference lists from all 49 full-text articles yielded no additional inclusions (Figure 1).
PRISMA 2020 flow diagram.

Data extraction and descriptive summary
Data relevant for the review aim were extracted in accordance with the stage of charting the data (Arksey and O’Malley Reference Arksey and O’Malley2005; Levac et al. Reference Levac, Colquhoun and O’Brien2010). Using a structured extraction sheet with predefined headings to capture details on the included articles and interventions, 2 authors independently extracted the data, which were reviewed by all authors and compiled into 2 tables (Tables 1 and 2). In line with the stage of collating and summarizing the data, the extracted data were then descriptively and narratively summarized. The articles were categorized based on the primary target group of the interventions, and each intervention was presented individually within its respective category to provide a structured overview of design, content, delivery, and reported findings.
Overview of included articles, grouped by the intervention studied

Overview of studied interventions, grouped by the main target group (children, parents or the entire family)

To map methodological strengths and limitations in the existing literature, all included articles were assessed using the Mixed Methods Appraisal Tool (MMAT), version 2018 (Hong et al. Reference Hong, Pluye and Fàbregues2018). The assessment was conducted by the first author, following discussions with the co-authors to ensure transparency and consistency in interpretation. The overall quality ranking is presented in Table 1 (full appraisal in Supplementary File 2).
Results
Study characteristics
This review includes 15 articles from Sweden (n = 7), the USA (n = 4), Germany (n = 1), and Australia (n = 1). Two articles were multinational: 1 conducted in the USA and Canada, and 1 across Germany, Austria, and the Benelux region. Twelve of the articles were published within the last 5 years. Nine were mixed-method studies, 4 qualitative, and 2 quantitative. Nine of the articles were classified as feasibility or pilot studies, 5 as evaluation studies, and 1 as a brief report. Most studies were small in scale, and only 3 involved more than 40 participants. According to the MMAT appraisal (Hong et al. Reference Hong, Pluye and Fàbregues2018), the methodological quality was generally good, although 2 studies were of medium quality and 1 of low quality (Table 1; Supplementary File 2).
Incurable cancer was the most commonly reported diagnosis among ill parents in the included studies. Progressive neurological diagnoses, such as ALS and Huntington’s disease, were also represented, though to a limited extent. Other diagnoses included were advanced pulmonary disease, chronic liver disease, and gastric bleedings due to Dieulafoy’s lesion. The interventions described in the articles primarily focused on psychosocial (n = 10), psychoeducational (n = 4), or peer support (n = 1), although several combined these approaches or included additional elements such as respite, creative activities, existential content, and practical support (Table 3).
Primary and additional support components in the interventions, as identified in this review

* Primary support component as described in the articles.
A descriptive summary was conducted to map the identified support intervention. Based on the primary target group, the articles were categorized into child-based (n = 4), parent-based (n = 4), and family-based (n = 7) interventions. The parent-based category comprised interventions directed toward either the ill parent, the co-parent, or both. With 4 interventions examined across multiple articles (n = 11), a total of 6 unique interventions are presented in this review. Quantitative findings in the included studies reflected preliminary effects at the group level, while qualitative findings captured participants’ subjective experiences and perceived impacts. An overview of the articles and categorization of interventions are presented in Tables 1 and 2, where the age groups of the children are also specified.
Categorization of interventions
Child-based support interventions
Four articles described 3 interventions directed at children: a caregiving training protocol (Kavanaugh et al. Reference Kavanaugh, Howard and Banker-Horner2018, Reference Kavanaugh, Cho and Howard2020a), a respite camp (Kavanaugh et al. Reference Kavanaugh, Cho and Maeda2017), and the art therapy program My Kite Will Fly (MKWF) (Holland et al. Reference Holland, Hocking and Joubert2018).
YCare Protocol
Two articles focused on an intervention aimed at supporting children providing care for a family member with ALS (Kavanaugh et al. Reference Kavanaugh, Howard and Banker-Horner2018, Reference Kavanaugh, Cho and Howard2020a). It was primarily centered on psychoeducation, designed to empower the children’s supportive roles through structured guidance, increased preparedness, and enhanced understanding. The intervention comprised a 1-day training course divided into 4 modules and was led by a multidisciplinary team. The focus areas of the modules were basic care, speech and feeding, assistive devices, and young caregiver support. By providing participants with information about the disease, care techniques, and practical skills training, the intervention intended to strengthen their ability to cope with their life situation. It sought to increase their knowledge, confidence, and coping skills while supporting them in dealing with the emotional and practical challenges of being a young caregiver. In addition to the educational sessions, the intervention included psychosocial and peer support through age-based small groups.
The intervention was associated with increased caregiving confidence, acquisition of new skills, and correction of previously incorrect techniques (Kavanaugh et al. Reference Kavanaugh, Howard and Banker-Horner2018, Reference Kavanaugh, Cho and Howard2020a). Children valued sharing experiences with peers and supporting each other through various tasks. The hands-on educational sessions were perceived to enhance their understanding of the disease and everyday coping, with practical demonstrations seen as more effective than verbal or written information alone (Kavanaugh et al. Reference Kavanaugh, Howard and Banker-Horner2018). The intervention was also considered feasible by both children and providers.
Youth respite camp
One article focused on a 4-day respite camp aimed to foster a sense of community among children from families living with Huntington’s disease (Kavanaugh et al. Reference Kavanaugh, Cho and Maeda2017). Led by experienced health practitioners, the camp was designed to promote self-esteem, resilience, and life satisfaction through a range of activities and sessions. Children were divided into groups, with siblings placed separately but grouping those from the same geographic regions to encourage ongoing peer support. Sessions addressed topics such as grief and loss, self-image, genetic testing, communication, relationships, caregiving, and research. In addition to peer support, the intervention included psychosocial and psychoeducational components, while also providing respite from everyday challenges.
The camp was associated with improvements in social and informational support, life satisfaction, and disease-related knowledge, particularly among girls and younger children (Kavanaugh et al. Reference Kavanaugh, Cho and Maeda2017). Peer interactions were perceived to promote a sense of belonging and reduce loneliness, while participants described feeling more hopeful, less fearful about the future, and better equipped to cope with everyday challenges. Some also felt better informed when making decisions about genetic testing.
My Kite Will Fly (MKWF)
MKWF was an art therapy program developed to support children in emotional expression and processing when a parent is diagnosed with life-threatening gynecological cancer (Holland et al. Reference Holland, Hocking and Joubert2018). The children participated in structured art therapy workbook activities during 3 phases of the illness: diagnosis, treatment, and palliative care. These included drawing, memory gathering, and exercises in communication and reflection. Although primarily aimed at children, MKWF also sought to support parents indirectly by providing them with tools to facilitate open family dialogue and thereby enhance their children’s understanding of the illness. In addition to its psychosocial focus, MKWF incorporated psychoeducational components, as the workbooks contained informative elements, together with creative activities.
MKWF was positively evaluated by most families at diagnosis and was associated with improved communication during treatment (Holland et al. Reference Holland, Hocking and Joubert2018). Workbook tasks completed during the palliative phase were rated as critical for stabilizing family routines. Children appreciated the creative workbooks, while parents indicated feeling better equipped to share information with their children. Both children and surviving parents described the intervention as helpful in preparing for parental bereavement.
Parent-based support intervention
Four articles presented 2 parent-based interventions: an audiobook intervention (Cuhls et al. Reference Cuhls, Hesse and Ates2021; Ateş et al. Reference Ateş, Hesse and Cuhls2024) and the telephone-delivered program Enhancing Connections-Palliative Care (EC-PC) (Lewis et al. Reference Lewis, Loggers and Phillips2020; Zahlis et al. Reference Zahlis, Shands and Lewis2020).
Family Audiobook
An intervention involving audiobooks was described in 2 of the articles (Cuhls et al. Reference Cuhls, Hesse and Ates2021; Ateş et al. Reference Ateş, Hesse and Cuhls2024). It aimed to help parents at the end of life in processing their emotions related to their illness and limited lifespan by creating personal audiobooks for their children, as part of palliative care. With the support of radio journalists, parents created professional recordings of their life stories, important memories, songs performed by themselves, selected music, readings, or other personally chosen content, intended as a lasting legacy for their children. Each audiobook was accompanied by a small booklet containing a table of contents and photos. The creative act of producing the audiobooks was intended to reduce psychological suffering and strengthen parents’ sense of meaning and closure. Although primarily psychosocial, the intervention also included biographical and existential elements, offering parents a space to reflect on their lives and experiences. Additionally, the audiobooks may serve as a concrete source of emotional support for the children, providing a valuable legacy during the grieving process.
Creating the audiobooks was associated with a sense of ease among the participating parents, who appreciated being able to leave behind a meaningful digital legacy, not only for their children but for the whole family (Cuhls et al. Reference Cuhls, Hesse and Ates2021; Ateş et al. Reference Ateş, Hesse and Cuhls2024). Although some expressed concerns about how their children might react upon hearing the recordings, they hoped the audiobooks would offer comfort during future difficult times (Cuhls et al. Reference Cuhls, Hesse and Ates2021). While the recording process was described as emotionally challenging, parents still valued it as an opportunity to create a lasting bond with their children and would recommend the intervention to others. It was perceived to help them cope with their illness, express thoughts they found difficult to share otherwise, and promote more open dialogue within the family.
Enhancing Connections-Palliative Care (EC-PC)
Two articles reported findings related to the EC-PC program (Lewis et al. Reference Lewis, Loggers and Phillips2020; Zahlis et al. Reference Zahlis, Shands and Lewis2020). This was a telephone-delivered intervention, led by a trained nurse or patient educator, designed to help parents with incurable cancer manage their parental roles. By providing them with education, guidance, and strategies, it aimed to improve parents’ ability to support their children. The intervention included 5 sessions at 2-week interval, focusing on helping parents separate their own experiences from their child’s, manage emotions, enhance self-care, listen actively, and support their child. At-home assignments aimed to improve parents’ communication with their children, as well as strengthening their ability to handle their own with anxiety. While primarily psychoeducational, the intervention also included psychosocial elements encouraging emotional reflection and dialogue.
The EC-PC program was found to be feasible and well-received, with parents reporting increased self-efficacy in supporting their children emotionally, addressing their concerns and helping them cope with the situation (Lewis et al. Reference Lewis, Loggers and Phillips2020). A reduction in parental anxiety was seen, as well as improvements in parenting skills and children’s behavioral and emotional adjustment. Parents described EC-PC as providing tools that supported open communication and enabling deeper conversations with their children (Zahlis et al. Reference Zahlis, Shands and Lewis2020). It helped them become more aware of their children’s emotional needs, manage their own reactions during difficult discussions, and address topics they had previously avoided. EC-PC was also perceived to enhance parents’ awareness of the importance of active listening and creating space for their children to express themselves.
Family-based support intervention
Seven articles focused on the Family Talk Intervention (FTI), designed to support families living with parental life-threatening illness (Eklund et al. Reference Eklund, Alvariza and Kreicbergs2020, Reference Eklund, Jalmsell and Kreicbergs2022a, Reference Eklund, Kreicbergs and Alvariza2022b, Reference Eklund, Lövgren and Alvariza2022c; Alvariza et al. Reference Alvariza, Jalmsell and Eklund2021; Weber Falk et al. Reference Weber Falk, Eklund and Kreicbergs2022; Bergersen et al. Reference Bergersen, Olsson and Larsson2024).
Family Talk Intervention (FTI)
Findings related to the FTI were reported in 7 articles, each offering a different perspective (Eklund et al. Reference Eklund, Alvariza and Kreicbergs2020, Reference Eklund, Jalmsell and Kreicbergs2022a, Reference Eklund, Kreicbergs and Alvariza2022b, Reference Eklund, Lövgren and Alvariza2022c; Alvariza et al. Reference Alvariza, Jalmsell and Eklund2021; Weber Falk et al. Reference Weber Falk, Eklund and Kreicbergs2022; Bergersen et al. Reference Bergersen, Olsson and Larsson2024). The intervention aimed to improve communication within families where a parent is affected by a life-threatening illness, by encouraging open dialogue about the disease and its impact. FTI sought to help family members share experiences and feelings with each other, assisting families in identifying their strengths, and to support parents in recognizing and meeting their children’s needs. It comprised 6 structured meetings held 1–2 weeks apart, led by 2 FTI-trained interventionists, involving parents, children, or the whole family depending on the stage of the intervention. Although primarily psychosocial, FTI also included elements of psychoeducation, peer support, and practical assistance.
Quantitative measurements showed no significant changes in family communication before and after FTI, apart from improved satisfaction with conversations and an increased willingness to talk among ill parents (Weber Falk et al. Reference Weber Falk, Eklund and Kreicbergs2022). However, no negative changes were reported (Eklund et al. Reference Eklund, Alvariza and Kreicbergs2020; Weber Falk et al. Reference Weber Falk, Eklund and Kreicbergs2022). The intervention was positively received by both children and parents, with most indicating that it met their expectations and that they would recommend it to others (Alvariza et al. Reference Alvariza, Jalmsell and Eklund2021; Eklund et al. Reference Eklund, Jalmsell and Kreicbergs2022a). The majority stated that they felt understood by the interventionists and comfortable sharing their thoughts. Some children also reported increased knowledge about their parent’s illness (Eklund et al. Reference Eklund, Alvariza and Kreicbergs2020).
Children and parents described improved family communication and mutual understanding following the intervention (Eklund et al. Reference Eklund, Alvariza and Kreicbergs2020, Reference Eklund, Jalmsell and Kreicbergs2022a, Reference Eklund, Lövgren and Alvariza2022c; Alvariza et al. Reference Alvariza, Jalmsell and Eklund2021; Weber Falk et al. Reference Weber Falk, Eklund and Kreicbergs2022; Bergersen et al. Reference Bergersen, Olsson and Larsson2024). Parents found FTI helpful for initiating sensitive conversations, deepening dialogue, and becoming more attentive listeners (Alvariza et al. Reference Alvariza, Jalmsell and Eklund2021; Eklund et al. Reference Eklund, Lövgren and Alvariza2022c; Weber Falk et al. Reference Weber Falk, Eklund and Kreicbergs2022). Children appreciated feeling heard and experienced family discussions as more open (Eklund et al. Reference Eklund, Alvariza and Kreicbergs2020, Reference Eklund, Jalmsell and Kreicbergs2022a). They valued the individual meeting without their parents (Eklund et al. Reference Eklund, Jalmsell and Kreicbergs2022a), which parents also considered important for giving their child space to express themselves freely (Alvariza et al. Reference Alvariza, Jalmsell and Eklund2021). While some children found participation emotionally challenging or noticed no major change in communication, most valued the supportive and safe environment FTI offered. Still, only a quarter of the children met the minimum level required by Article 12 of the UNCRC, where children’s views are meaningfully taken into account (Eklund et al. Reference Eklund, Kreicbergs and Alvariza2022b). To assess this, the Pathways to Participation model (Shier Reference Shier2001) was applied. The model outlines 5 levels of participation, ranging from being listened to and supported in expressing views (levels 1–2), to having one’s views taken into account (level 3), and progressing toward shared decision-making and shared responsibility (levels 4–5).
The structured yet flexible format of FTI was generally appreciated by families, although several wished for earlier participation, more thorough preparation, additional meetings, or separate sessions to address sensitive topics (Alvariza et al. Reference Alvariza, Jalmsell and Eklund2021; Eklund et al. Reference Eklund, Jalmsell and Kreicbergs2022a). Children described how the intervention enhanced their understanding of the illness and helped them feel more prepared for future challenges, including potential medical emergencies (Eklund et al. Reference Eklund, Alvariza and Kreicbergs2020). Both ill parents and co-parents expressed a sense of security for the future following FTI, reassured that the family was better equipped to cope and support one another (Weber Falk et al. Reference Weber Falk, Eklund and Kreicbergs2022).
The interventionists were described by children and parents as playing a central role in their overall experience, generally perceived as professional and as contributing to a sense of safety (Alvariza et al. Reference Alvariza, Jalmsell and Eklund2021; Eklund et al. Reference Eklund, Jalmsell and Kreicbergs2022a). The practical assistance they provided was also appreciated, for example, facilitating access to external support services for children, helping parents with organizing school meetings, obtaining aids, and navigating application processes (Eklund et al. Reference Eklund, Alvariza and Kreicbergs2020; Weber Falk et al. Reference Weber Falk, Eklund and Kreicbergs2022). In some cases, the interventionists also enabled contact with other families in similar situations, and parents described this peer support as alleviating feelings of loneliness both during and after the intervention (Bergersen et al. Reference Bergersen, Olsson and Larsson2024).
Discussion
This review identified 15 articles describing 6 interventions aimed at supporting children and/or parents in families with a parent who had a life-threatening illness. Of these, 3 targeted children, 2 parents, and 1 the entire family. The interventions were primarily based on psychosocial, psychoeducational, and/or peer support but also incorporated additional supportive elements. Positive findings included improved family communication and mutual understanding, increased illness-related knowledge, enhanced coping, and reduced loneliness among children and parents. Gains in caregiving skills and parenting confidence were reported, and several interventions were considered feasible and acceptable. Although negative findings were few, some participants found their participation emotionally challenging. Overall, the interventions were perceived as helpful in navigating the difficult life situation, with several participants stating they would recommend them to others.
The limited number of included articles in this review – mostly small-scale pilot or feasibility studies covering few interventions – confirms the scarcity of research on support interventions for families facing parental life-threatening illness. It also reflects the previously reported knowledge gap in the context of fatal progressive neurological or neuro-oncological diseases. While the inclusion criteria were broadened to encompass various life-threatening illnesses, this review was primarily motivated by clinical and research interest in the neurological field. Although some interventions targeted a broader range of diseases, most were either designed specifically for cancer or included predominantly cancer-affected participants, with limited representation of other diagnoses. With only 3 articles describing 2 interventions focusing exclusively on fatal progressive neurological diseases (Kavanaugh et al. Reference Kavanaugh, Cho and Maeda2017, Reference Kavanaugh, Howard and Banker-Horner2018, Reference Kavanaugh, Cho and Howard2020a), the urgent need for more tailored support within the neurological care context is clearly highlighted. While all life-threatening illnesses can have a profound impact on families, those facing progressive neurological or neuro-oncological diseases may encounter distinct and complex challenges. Typical symptoms, such as gradually increasing physical impairment and, in some diagnoses, difficulties with breathing, speaking or swallowing (Masrori and Van Damme Reference Masrori and Van Damme2020; Stoker et al. Reference Stoker, Mason and Greenland2022; Schaff and Mellinghoff Reference Schaff and Mellinghoff2023), can complicate parents’ ability to care for their children and express physical affection. The fear of choking and dying from sudden respiratory failure is also a major source of worry among both children and parents (Stoker et al. Reference Stoker, Mason and Greenland2022; Malmström et al. Reference Malmström, Öhlén and Nilsson2025), reflecting a lack of knowledge about the disease. Additionally, cognitive decline and behavioral changes, which may occur (Masrori and Van Damme Reference Masrori and Van Damme2020; Pender et al. Reference Pender, Pinto-Grau and Hardiman2020; Stoker et al. Reference Stoker, Mason and Greenland2022; Schaff and Mellinghoff Reference Schaff and Mellinghoff2023), can impair parents’ capacity to be mentally present and emotionally supportive. These challenges may become even more complicated if speech is impaired and communication limited. Brain tumors have also been associated with increased externalized aggression, adding to families’ emotional strain and instability (Arifin et al. Reference Arifin, Yudoyono and Setiawan2014; Boele et al. Reference Boele, Rooney and Grant2015).
The overall positive experiences across the interventions underline the importance of providing families with support, rather than prioritizing a specific type, as any formal support may be preferable to leaving families to navigate the situation on their own (Malmström et al. Reference Malmström, Öhlén and Jakobsson Larsson2024, Reference Malmström, Öhlén and Nilsson2025; Billaud Feragen et al. Reference Billaud Feragen, Egedal and Kjolaas2025; Cooper et al. Reference Cooper, Simpson and Dale2025). Simultaneously, as needs often vary – both between and within families – different forms of support remain essential. While there may be uncertainty about where to turn for support, families may also have limited time and energy to search for it (Malmström et al. Reference Malmström, Jakobsson Larsson and Nilsson2023, Reference Malmström, Öhlén and Nilsson2025). This further underscores the importance of early and proactive support, to avoid placing the burden on families to initiate help-seeking themselves before the situation may escalate. Given the gradual progression, support from the point of diagnosis with ongoing follow-up is essential throughout the disease trajectory, with palliative care playing a central role – shown to be both feasible and valued by ill parents and their families (Fahrner-Scott et al. Reference Fahrner-Scott, Zapata and O’Riordan2022; Zwicker et al. Reference Zwicker, Smith and Rice2023).
While it is important to tailor support to the neurological context, several components of the interventions identified in this review may still hold value. Support to improve communication has previously been requested, including family therapy to foster dialogue and stronger relationships, as well as individual sessions (Sommers-Spijkerman et al. Reference Sommers-Spijkerman, Rave and Kruitwagen-van Reenen2022; Malmström et al. Reference Malmström, Jakobsson Larsson and Nilsson2023). The structure of FTI was described as flexible to the families’ needs (Alvariza et al. Reference Alvariza, Jalmsell and Eklund2021), which is important given that the ill parent’s condition may deteriorate rapidly and create new everyday challenges. As symptoms may also impair verbal interaction cognitively or physically, families should be supported in identifying alternative strategies for maintaining communication. With the audiobook intervention in mind (Cuhls et al. Reference Cuhls, Hesse and Ates2021; Ateş et al. Reference Ateş, Hesse and Cuhls2024), guidance and tools for recording voice messages before speech becomes severely impaired may be particularly valuable.
Research highlights the need for families facing fatal progressive neurological disease to connect with others in similar situations (Kavanaugh et al. Reference Kavanaugh, Noh and Studer2015, Reference Kavanaugh, Henning and Mochan2021; Malmström et al. Reference Malmström, Jakobsson Larsson and Nilsson2023). As shown in the results, peer camps can help children find a sense of belonging and reduce feelings of isolation (Kavanaugh et al. Reference Kavanaugh, Cho and Maeda2017), while also offering temporary respite from the illness context – an essential need for their well-being (Malmström et al. Reference Malmström, Jakobsson Larsson and Nilsson2023). However, various meeting formats can be valuable, including support groups organized by healthcare, social services, or other organizations. Such support may come not only from professionals but also from civil society and community-based initiatives, reflecting a shared and ideally early responsibility, consistent with a public health palliative care perspective (Sallnow et al. Reference Sallnow, Smith and Ahmedzai2022). In addition to addressing practical and emotional needs, families also require support to process existential dimensions of the situation and the uncertainty it brings, including gaps in information about the disease and its progression.
Families facing a fatal progressive neurological or neuro-oncological illness often express frustration and worry due to a lack of clear information (Loughan et al. Reference Loughan, Reid and Willis2022; Malmström et al. Reference Malmström, Jakobsson Larsson and Nilsson2023, Reference Malmström, Öhlén and Jakobsson Larsson2024, Reference Malmström, Öhlén and Nilsson2025; Cooper et al. Reference Cooper, Simpson and Dale2025). This must be carefully considered when adapting psychoeducational interventions to the neurological context and underscores the importance of specialist expertise among those delivering the support. Involving children and ensuring their access to professionals is essential for promoting understanding (Malmström et al. Reference Malmström, Jakobsson Larsson and Nilsson2023), as illustrated by the expert-led training day intervention, which was considered valuable and helped increase children’s feelings of preparedness (Kavanaugh et al. Reference Kavanaugh, Cho and Howard2020a, Reference Kavanaugh, Howard and Banker-Horner2018). This highlights the need for educational support for caregiving children, as well as adequate practical support for families to prevent children from becoming overburdened. Research shows that children may compensate for gaps in such support by taking on extensive responsibilities (Bergersen et al. Reference Bergersen, Larsson and Olsson2022; Malmström et al. Reference Malmström, Öhlén and Jakobsson Larsson2024, Reference Malmström, Öhlén and Nilsson2025; Cooper et al. Reference Cooper, Simpson and Dale2025). It is therefore crucial to ensure that children are not placed in a position of disproportionate responsibility – especially in contexts with limited home care services.
Digital support has been requested by families affected by fatal progressive neurological illness to improve accessibility when in-person sessions are difficult due to physical limitations or caregiving demands (Malmström et al. Reference Malmström, Jakobsson Larsson and Nilsson2023, Reference Malmström, Öhlén and Jakobsson Larsson2024). Although this review did not identify any digital support, the telephone-based intervention may have helped some of the ill parents to overcome some of these participation barriers (Cuhls et al. Reference Cuhls, Hesse and Ates2021; Ateş et al. Reference Ateş, Hesse and Cuhls2024). Digital support may be particularly relevant for children, as it offers a familiar setting while also improving access for those who may remain at home due to extensive responsibilities and fear of leaving their ill parent (Malmström et al. Reference Malmström, Öhlén and Jakobsson Larsson2024).
Previous research has highlighted the need for a holistic approach from healthcare when encountering a life-threateningly ill patient who is also a parent (Malmström et al. Reference Malmström, Jakobsson Larsson and Nilsson2023, Reference Malmström, Öhlén and Nilsson2025; Billaud Feragen et al. Reference Billaud Feragen, Egedal and Kjolaas2025). Requests from both children and parents for mandatory family meetings at the time of diagnosis reflect the urgency of establishing such meetings as a routine part of care (Malmström et al. Reference Malmström, Jakobsson Larsson and Nilsson2023). While a more proactive approach to supporting the family as a whole may be essential to overall family health, attention should also be given to individual support. Children may require professional help to understand and process their emotions, and to cope with the consequences of the illness (Malmström et al. Reference Malmström, Jakobsson Larsson and Nilsson2023, Reference Malmström, Öhlén and Jakobsson Larsson2024). Given children’s appreciation of the FTI’s individual meetings (Eklund et al. Reference Eklund, Jalmsell and Kreicbergs2022a), along with previous findings indicating that they often refrain from sharing difficult thoughts to avoid burdening their parents (Malmström et al. Reference Malmström, Öhlén and Jakobsson Larsson2024), it is important that they have access to a safe and trusting environment in which to express their emotions. However, as children’s views were not always fully taken into account within FTI (Eklund et al. Reference Eklund, Kreicbergs and Alvariza2022b), it remains essential to ensure that their perspectives are genuinely heard and valued. In some cases, alternative methods of communication may facilitate emotional expression rather than verbal interaction. This highlights the relevance of the art-therapeutic elements included in MKWF, although the structure and implementation of that intervention were unfortunately described in limited detail (Holland et al. Reference Holland, Hocking and Joubert2018). As symptoms progress and increasingly affect parenthood, parental support may also become necessary (Billaud Feragen et al. Reference Billaud Feragen, Egedal and Kjolaas2025; Malmström et al. Reference Malmström, Öhlén and Nilsson2025). Both ill parents and co-parents may need help to cope with the illness and their own emotional reactions, as well as to better understand and support their children. Additionally, ill parents should be provided with guidance on how to maintain a stable and supportive parental presence despite physical and cognitive decline. All in all, it is essential to recognize families in their relational and everyday context, and to draw on both formal and informal support in responding to their shared and individual needs (Sallnow et al. Reference Sallnow, Smith and Ahmedzai2022).
Although most included studies were small-scale feasibility or pilot studies, limiting conclusions about the interventions’ effectiveness, they still provide valuable insights for future support development. Several included components found meaningful by participants, particularly in relation to communication and emotional coping. Study quality and the clarity of intervention descriptions, as assessed by MMAT (Hong et al. Reference Hong, Pluye and Fàbregues2018), varied. While some studies demonstrated strong coherence between data collection, analysis, and interpretation, others lacked transparency or clear methodological rationale. Some interventions were supported by multiple publications using both qualitative and quantitative methods, suggesting a relatively robust evidence base – for instance, FTI, which was examined in several high-quality-rated studies. Others were only described in a single publication, making broader relevance harder to assess. Although studies were not excluded based on quality, the appraisal highlights both methodological strengths and gaps. Future research should use more rigorous designs that combine outcome evaluation with exploration of lived experience to develop interventions that are effective, feasible, acceptable, and adaptable to different contexts.
In conclusion, this review highlights the limited availability of support interventions for families facing parental life-threatening illnesses, as well as in the context of fatal progressive neurological diseases. It underscores the need to develop interventions specifically tailored for these families, while existing approaches may still offer valuable guidance. There is a pressing need for early, proactive, and accessible support that addresses both individual and family needs – support that is holistic, adaptable to disease progression, and includes ongoing follow-up, reflecting core elements of high-quality palliative care.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S1478951526101837.
Acknowledgments
Special thanks are given to Linda Hammarbäck, librarian at the Biomedical Library at the University of Gothenburg, for assistance in conducting the literature search, to Master’s students Anja Lister and Thekla Ekman for their help with the screening of articles, and to Anita Shenoi for language editing.
Funding
This study was funded by the Swedish Neuro Association (Neuro); the ALS Foundation; the Börje Salming ALS Foundation; the Department of Medical Sciences, Neurology, Uppsala University.
Competing interests
The authors declare none.
Declaration of generative AI
During the preparation of this manuscript, the authors used ChatGPT (OpenAI) for assistance with language editing and improving readability. The authors have carefully reviewed and revised the content as necessary and take full responsibility for the final version of the manuscript.






 Open access
Open access