


Introduction
Hospitalised infants are exposed to substantial and recurrent stressors that strain their adaptive capacity and place them at risk for physiological instability, impaired healing, and disrupted neurodevelopment. Emerging evidence from evaluation of stress exposure in preterm infants suggests that exposure to stressful encounters during infancy, including invasive procedures, environmental stressors, and caregiver handling, contributes to altered physiologic stability and long-term developmental outcomes. Reference Brummelte, Glanaghy, Bonnin and Oberlander1–Reference Van Dokkum, De Kroon, Reijneveld and Bos3 Literature in this area, however, is primarily focused on preterm infants and typically excludes infants with congenital anomalies, including heart disease. Infants with CHD undergoing cardiac surgery are particularly vulnerable to perioperative adverse outcomes including haemodynamic instability and cardiac arrest, Reference Alten, Klugman and Raymond4 as well as long-term neurodevelopmental abnormalities. Reference Sood, Newburger and Anixt5 Risk of these negative outcomes may be exacerbated by heightened perioperative stress exposure triggering maladaptive stages of the stress response. Reference Selye6 The significant gap in our understanding of stressful encounters in this unique and particularly vulnerable infant population prevents clinicians from recognising and reducing these stressors and their potential to negatively impact outcomes.
Stress, the physiological, psychological, and behavioural responses to a stimulus or demand, Reference Edes and Crews7,Reference Selye8 is increasingly recognised as not only acutely harmful in infancy but also associated with long-term adverse outcomes. Reference Brummelte, Glanaghy, Bonnin and Oberlander1–Reference Van Dokkum, De Kroon, Reijneveld and Bos3 Stressors or source of stress are any stimulus that disrupts homeostasis, triggering a stress response. Reference Selye8 Hospitalised infants are estimated to encounter 43 to 75 stressors per day of hospitalisation. Reference Carbajal, Rousset and Danan9–Reference van Dokkum, de Kroon, Dijk, Kraft, Reijneveld and Bos12 Stressors have been shown to be concentrated in the first week of admission consisting of frequent handling, light, and noise in addition to painful procedures. Reference van Dokkum, de Kroon, Dijk, Kraft, Reijneveld and Bos12–Reference Smith, Gutovich and Smyser14 Although painful or invasive procedures, such as endotracheal tube suctioning, have been associated with more severe stress response, Reference Li, Zhang, Huang, Ye and Lin15–Reference Slater, Asmerom and Boskovic17 even low-level activities, such as obtaining a weight or diaper changes, have been demonstrated as stressful. Reference Bembich, Trappan and Galimberti18,Reference Mörelius, Hellström-Westas, Carlén, Norman and Nelson19 Previous work investigating the effect of stress exposure on premature infants, has found stressful encounters impact short-term physiological status, may prompt epigenetic changes, and are connected to abnormal cerebral growth impacting neurodevelopment. Reference D’Agata, Walsh, Vittner, Cong, McGrath and Young10,Reference Smith, Gutovich and Smyser14,Reference Fumagalli, Provenzi and Carli20–Reference van Dokkum, Bao and Verkaik-Schakel23 However, the exposure to and impact of stress in infants with CHD remain poorly defined.
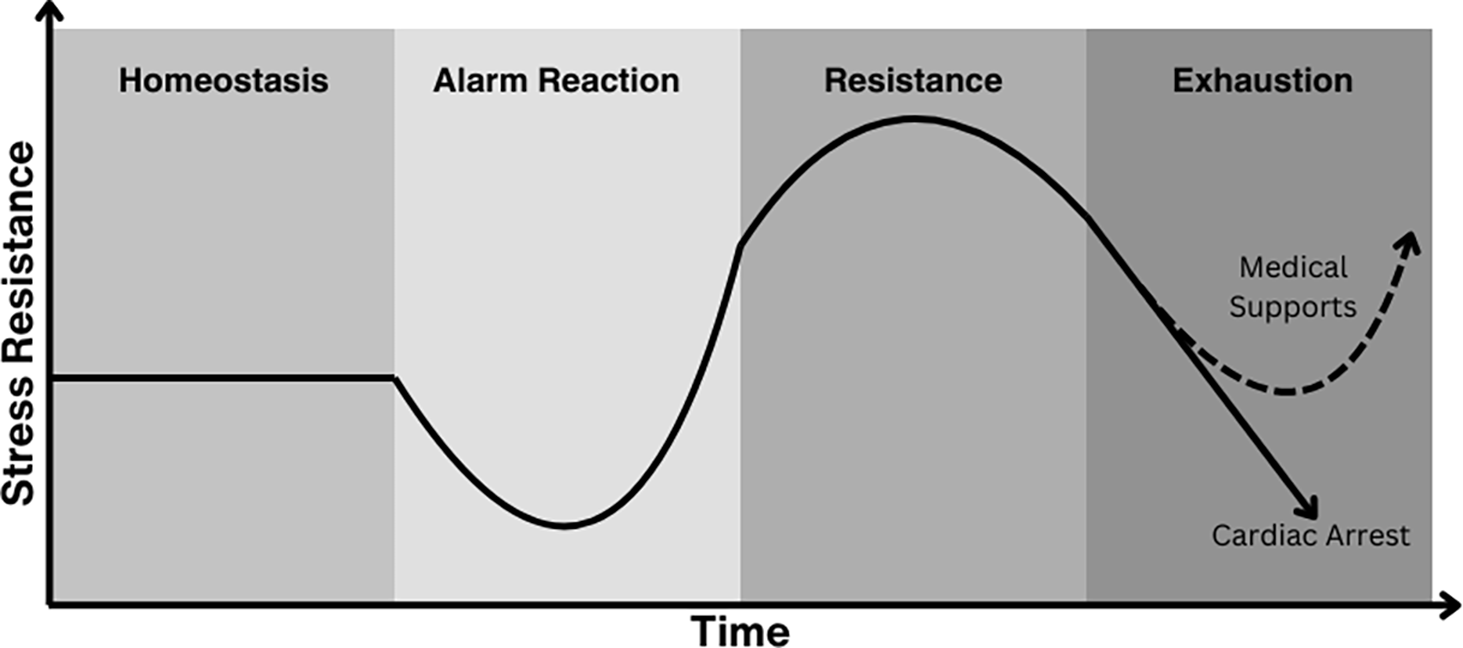
Regarded as the principal stress theory, Selye’s General Adaptation Syndrome describes a stereotypical stress response following a stimulus Reference Selye6,Reference Selye8,Reference Selye24 consisting of three phases: (1) alarm reaction, or initial physiological defence mechanisms to combat the stressor; (2) resistance, the attempts of the body to normalise function with continued exposure to the stressor; and (3) exhaustion, the final stage of the stress response when severe or prolonged exposure to the stressor depletes the body’s reserves. Reference Sood, Newburger and Anixt5,Reference Nist, Harrison and Steward22,Reference van Dokkum, Bao and Verkaik-Schakel23 Based on Selye’s concepts, we identified cumulative stress as a possibly modifiable risk factor for acute haemodynamic instability, including cardiac arrest, and longitudinal neurodevelopmental outcomes in infants following cardiac surgery. Timely recognition of stress prior to this exhaustion phase may allow clinical supports to be utilised to prevent physiological instability and improve clinical outcomes (Figure 1).
General adaptation syndrome modelling of postoperative deterioration. The triphasic response to stress described in Selye’s General Adaptation Syndrome suggests cumulative stress exposure may precipitate postoperative physiological instability as the result of the under-supported or unrecognised exhaustion phase of a stress response. Timely recognition of the exhaustion phase may allow clinical supports to be utilised to prevent deterioration.

Prior studies report correlations between infant stress, acute physiological instability, Reference Li, Zhang, Huang, Ye and Lin15,Reference Bernert, von, Seidl, Vanhole, Devlieger and Casaer25 abnormal cerebral growth, Reference Fumagalli, Provenzi and Carli20 delayed neurodevelopment, Reference Bruce, Compton and Maylott26,Reference Xing, Zhang, Cao and Zhang27 and epigenetic changes, Reference Fumagalli, Provenzi and Carli20,Reference van Dokkum, Bao and Verkaik-Schakel23 though most excluded infants with inherited conditions, including CHD. Differences in pathophysiology, surgical intervention(s), and clinical trajectory undoubtedly expose infants with CHD to sources of stress uncommon to other patient populations. The cardiovascular implications of CHD, including the underlying physiology and subsequent demands of surgical recovery, likely limit adaptation and tolerance of high-stress states. This knowledge gap has hindered the investigation of the relationship between infant stress, impact, and clinical outcomes in neonates and infants with CHD. This study aimed to identify and describe sources of stress, stress cues, stress responses, and clinical implications in infants undergoing cardiac surgery as perceived by expert interdisciplinary clinicians.
Methods
Semantic content analysis, Reference Krippendorff28 a method within the qualitative paradigm, was used to identify and describe sources of stress, stress cues and responses, and clinical implications as perceived by expert clinicians caring for neonates and infants with CHD undergoing cardiac surgery. This study was reviewed by the Children’s National Hospital Institutional Review Board and found to be exempt (STUDY00000572; March 13, 2023). The risks, benefits, and voluntary nature of participation were discussed verbally with eligible participants before the interviews and outlined in a study information sheet provided to each participant.
Study terms
For study purposes, stress was defined as the physiological, psychological, and behavioural responses to a stimulus or demand, which may also be physical or psychological, Reference Edes and Crews7,Reference Selye8 characterised by observable physiological or behavioural reactions that might indicate negative stimulation in a neonate or infant. Reference Selye6,Reference D’Agata, Young, Cong, Grasso and McGrath29 Stressors were defined as actions, inactions, and interactions that might create negative stimulation in a high-risk infant. Stress cues were defined as observable physiological or behavioural signals exhibited by a neonate or infant that indicate exposure to a stressor or emerging difficulty maintaining homeostasis. Stress response was defined as the physiological reaction elicited in a neonate or infant following exposure to a stressor, reflecting the attempt to adapt to or regulate the disruption of homeostasis. High-stress states describe elevated intensity of stress experienced by an individual, characterised by pronounced or sustained stress cues and stress responses suggesting significant negative stimulation or limited regulatory capacity. Cumulative stress exposure describes the total burden of stress experienced by a neonate or infant over time, resulting from repeated, prolonged, or multiple stressors and the associated stress response.
Setting
Four urban tertiary care centres with dedicated cardiac intensive care units (CICUs) from the mid-Atlantic, Midwest, and West Coast regions of the United States. Unit size ranged from 12 to 36 dedicated cardiac ICU beds, performing 165 to 600 paediatric cardiac surgeries per year.
Sample selection
Experienced Clinicians with a minimum of 10 years of post-training experience were purposefully sampled to represent the continuum of clinical specialties across two care areas (operating room and CICU) and three phases of care (preoperative, operative, and postoperative) encountered by neonates and infants undergoing cardiac surgery. Targeted enrolment included the roles of CICU attending physician, CICU clinical nurse, cardiac surgeon, and cardiac anaesthesiologist. These roles were selected for inclusion given their consistent involvement across each phase of care, supporting the examination of patterns both within and across phases. Eligible participants were approached directly by the principal investigator about enrolment.
Data collection
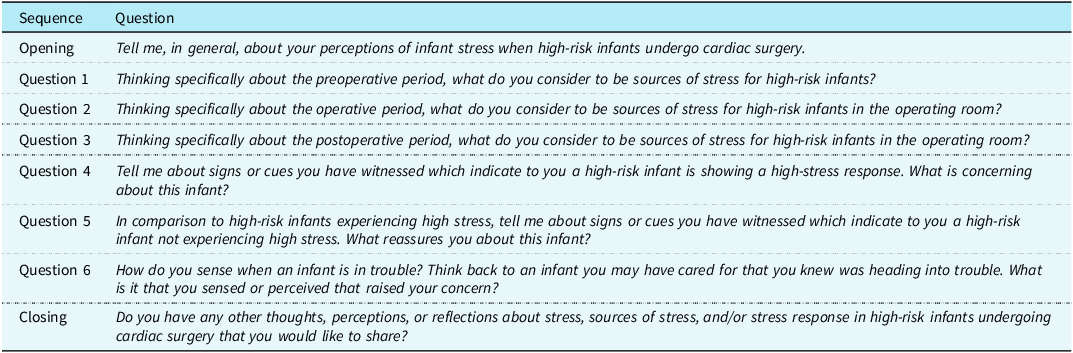
Following the Krippendorff methodology Reference Krippendorff28 for a semantic descriptive content analysis, narrative data were collected through one-on-one semi-structured interviews between March 2022 and April 2023. An interview guide of eight questions derived from infant stress literature Reference Carbajal, Rousset and Danan9,Reference van Dokkum, de Kroon, Dijk, Kraft, Reijneveld and Bos12,Reference D’Agata, Young, Cong, Grasso and McGrath29 and the GAS Reference Selye6 was reviewed by a content expert prior to utilisation (Table 1). In addition to a standardised interview guide, an introduction to the study, including the operational definition of stress, was scripted to maintain consistency across participants. Interviews were conducted either in-person or virtually using Zoom (Zoom Video Communications, Inc.). The initial interview focused on recalled examples of caring for neonates and infants during admission for cardiac surgery. Following data analysis, findings were validated through member checking, a qualitative research technique where researchers share their findings with participants to confirm accuracy, credibility, and resonance with their experiences. Reference McKim30
Interview guide for collection of narrative data

Data analysis
Narrative data were analysed using semantic content analysis, which allows for systematic extraction and definition of intended meaning. Reference Krippendorff28 Resultant codes were described by meaning and frequency. Themes were conceptually defined, and their frequencies and proportions of occurrence were calculated per unit of response, defined as the transcribed response to each interview question.
Three analysts trained in semantic content analysis completed coding (CR, AH, PH). The phrase was the unit of analysis within each transcript. The analysts jointly compiled a coding dictionary with mutually exclusive and exhaustive codes. First-level codes were identified through collective open coding of three initial transcripts. The fourth transcript was individually coded with successive comparison to evaluate intercoder agreement. Subsequently, analysts coded the remaining interviews, resolving discrepancies via consensus. First-level codes were analysed for conceptual overlap and, when indicated, merged with second-level codes and abstracted to explanatory themes. Saturation was determined when no new first-or second-level codes were identified during coding. Reference Guest, Nameyid and Chen31 Qualitative data were managed using Microsoft Office applications.
Results
The sample included 17 participants: CICU attending physicians (n = 4), CICU clinical nurses (n = 6), cardiac surgeons (n = 4), and cardiac anaesthesiologists (n = 3). Participants represented four institutions from the mid-Atlantic, Midwest, and West Coast regions of the United States; 14 of 17 participants were from the primary mid-Atlantic centre. All individuals approached agreed to participate and completed the interview process. Interviews ranged from 20 to 48 minutes. Following the analysis, 1694 distinct phrases were assigned to 76 first-level codes. These were reduced into 20 second-level codes, which were abstracted into 7 explanatory themes. Saturation was achieved following coding of 12 interviews. To ensure saturation of all elements across each participant role, sampling was continued to include a minimum of three participants per role. Member checking did not indicate the need to modify thematic findings.
Description of themes
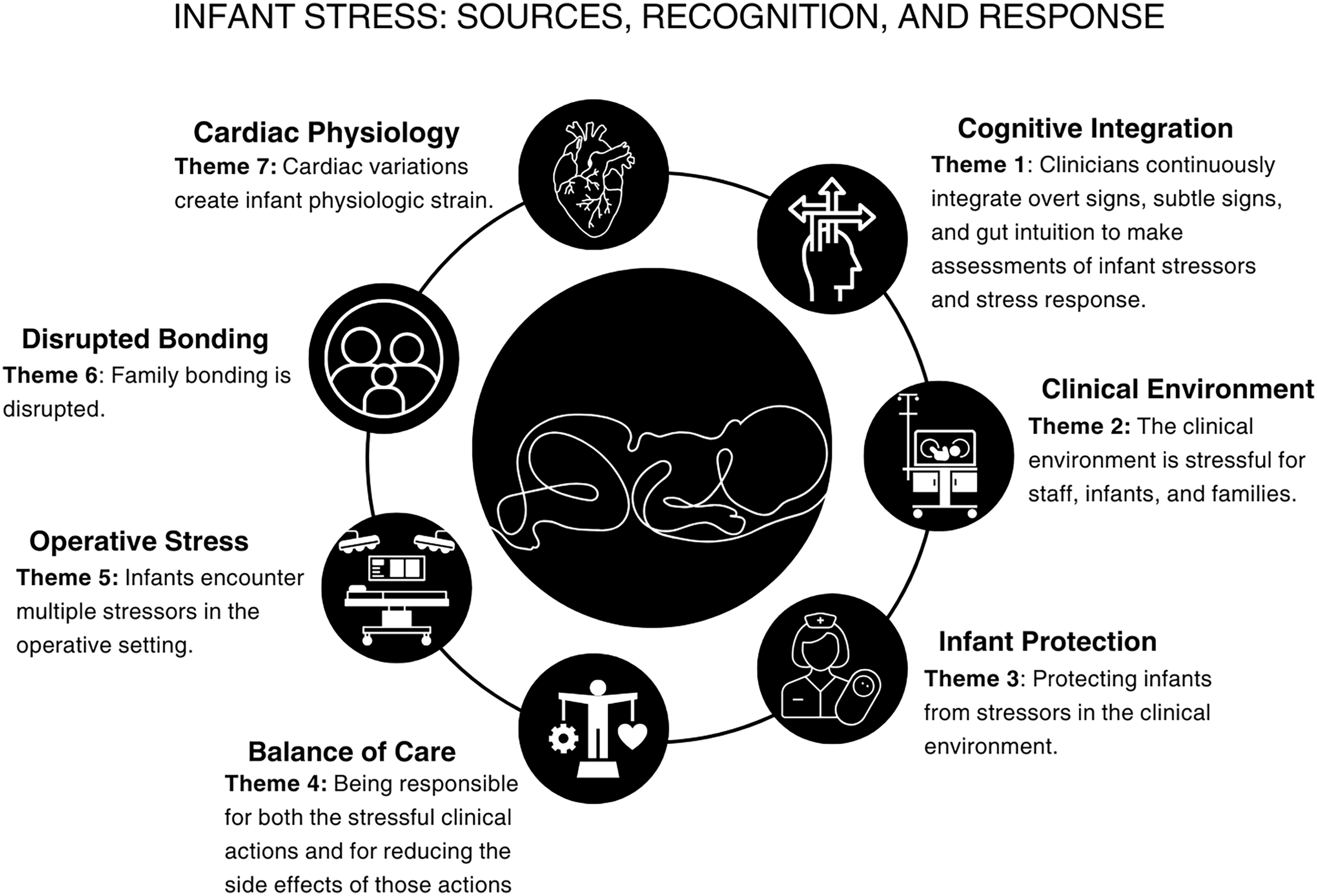
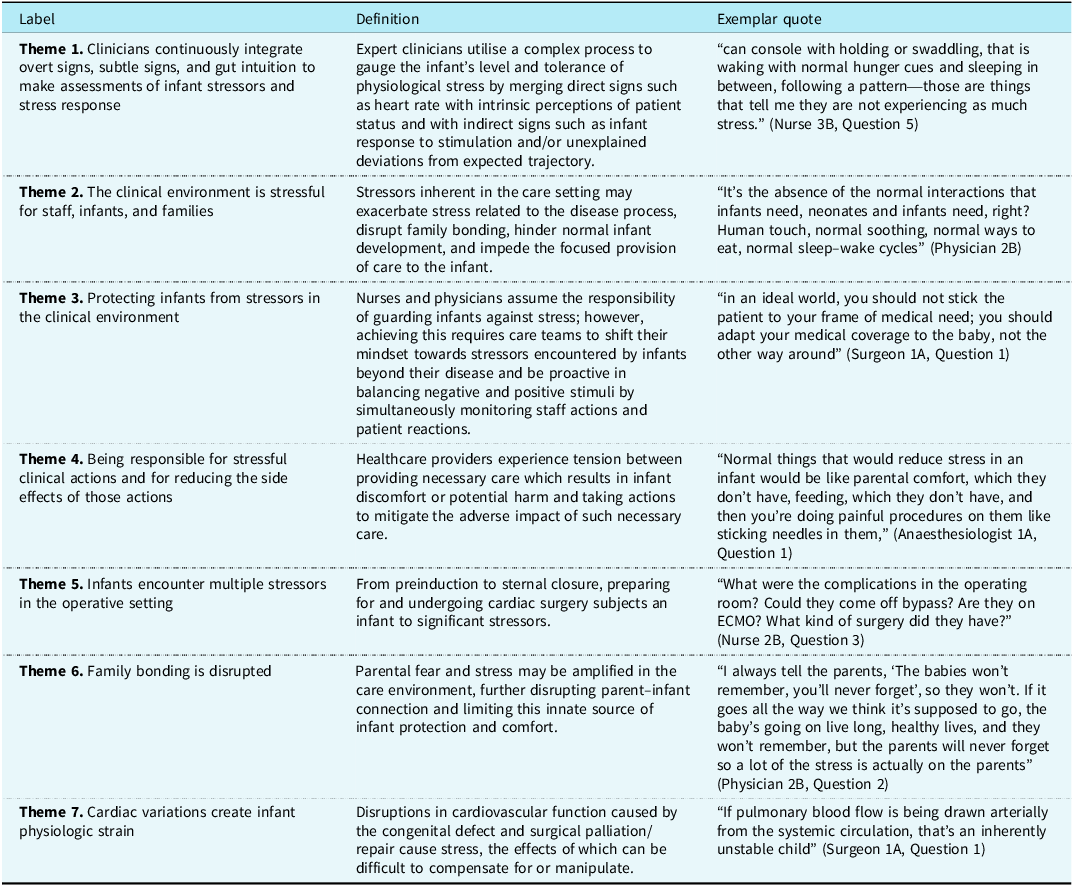
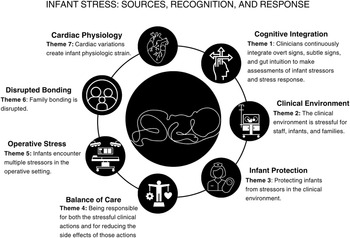
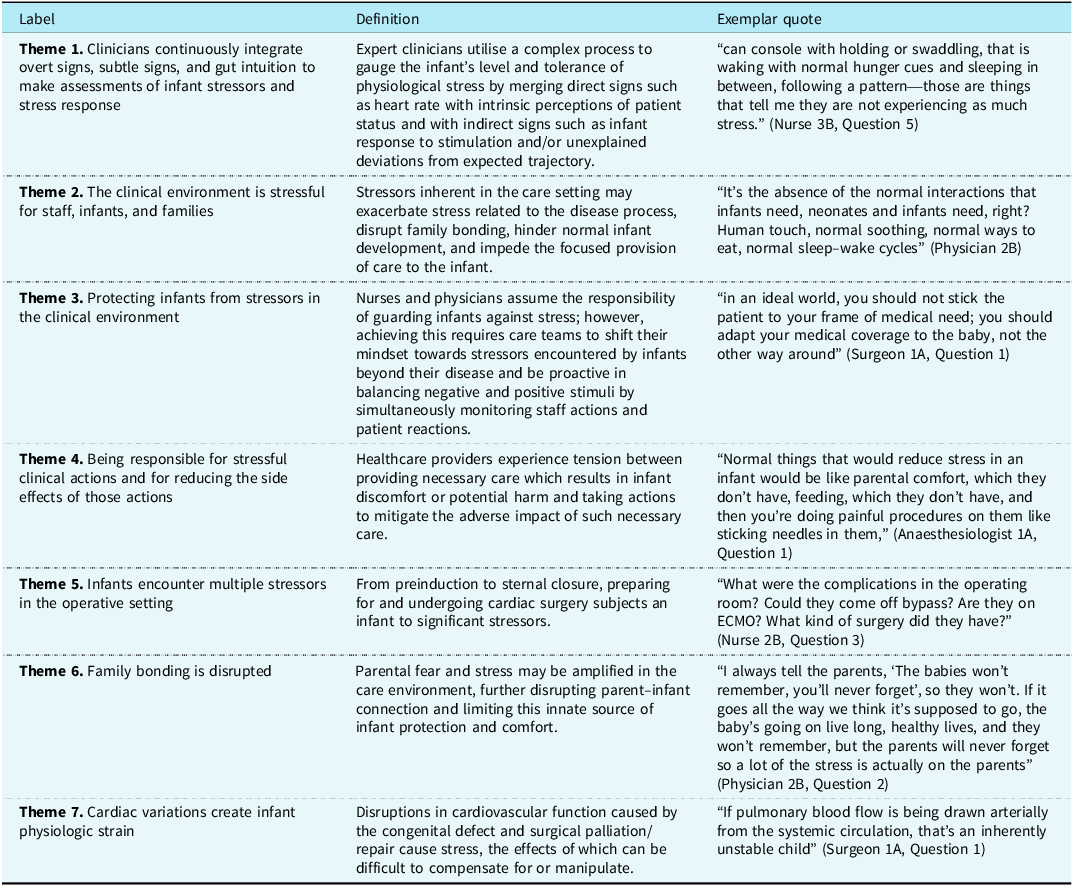
Seven themes were identified (Figure 2). Table 2 presents theme labels, definitions, and exemplar quotes. Supplemental Tables S1 and S2 present exemplar quotes of each theme in descending order of frequency for themes related to identified stressors by phase of care and themes related to clinician recognition of infant stress states.
Themes of infant stress identified by expert clinicians. Seven themes and associated conceptual definitions of stress in infants undergoing cardiac surgery were identified from semantic content analysis of interdisciplinary experts across preoperative, operative, and postoperative phases of care. Theme symbols and abbreviated theme labels are representative of key thematic elements. Themes include sources of infant stress – Clinical Environment (Theme 2), Operative Stress (Theme 5), Disrupted Bonding (Theme 6), Cardiac Physiology (Theme 7), clinician recognition of infant stress exposure – Cognitive Integration (Theme 1), and clinician responses to infant stress – Infant Protection (Theme 3) and Balance of Care (Theme 4).
Identified theme labels, definitions, and exemplar quote
Theme 1. Clinicians continuously integrate overt signs, subtle signs, and intuition to make assessments of infant stressors and stress response
Across roles and care areas, participants described a complex process to evaluate infant stress levels and infant stress response (Physician 3B: “It’s not necessarily one thing but multiple subtle things that are stacking up in the same baby”; Nurse 2A: “every baby has their own rhythm that you can tap into”). Participants described integrating more subtle signs with overt signs, e.g. tachycardia (Nurse 1B: “When patients don’t have calm wake cycles, that’s worrisome when they’re basically either sedated, asleep, or screaming”). Theme 1 was the most commonly occurring theme when participants were asked to identify signs or cues that may indicate overwhelming stress, and when asked which signs or cues may be reassuring.
Theme 2. The clinical environment is stressful for staff, infants, and families
Participants described the clinical environment as highly stressful for infants, staff, and families (Nurse 1B: “The environment in general is stressful. There’s noise, there’s lights, there’s constant overstimulation”; Surgeon 2A: “It’s a very harsh environment. Is there enough comfort in the way we care?”). Participants noted the difference between the clinical environment and a “normal” home environment, citing “the absence of what should be normal” as a source of infant stress (Physician 3B: “As parents, we put them in a quiet room, we have the white noise, we’re coming to them, and every little gurgle is just fantastic. And that can’t happen. It’s loud, it’s bright, there’s no circadian variation. Feeding cues may or may not be paid attention to”). This theme was dominant when participants were asked about general perceptions of infant stress and stress response, offered by 10 participants (59%). Participants frequently offered this theme when describing sources of stress in the preoperative period.
Theme 3. Protecting infants from stressors in the clinical environment
Participants described their actions to mitigate stressors infants encounter in the clinical environment, such as “setting time limits” on stressful clinical activities. Participants emphasised clinicians must have awareness of existing stressors to offer infants protection (Surgeon 2A: “In an ideal world, you should not stick the patient to your frame of medical need; you should adapt your medical coverage to the baby”; Nurse 1B: “Being an infant in this environment is stressful, even if you don’t tack on disease process or anything like that. In our setting, we need to be more mindful of that”). Theme 3 was most common in the final question asking for additional considerations on infant stress, representing 10 (59%) clinicians and 30% of coded phrases.
Theme 4. Being responsible for stressful clinical actions and for reducing the side effects of those actions
Clinicians described negative side effects of necessary care and the need to balance stressful clinical actions with the responsibility to mitigate the negative impact of these actions (Nurse 4B: “In order to save them, I feel like there’s so many things that we’re doing, we are hurting so many other parts of them”; Physician 3B: “The painful stuff, the noisy stuff, the suctioning—you know, all the stuff that we do to have them survive”). Participants acknowledged high-stress exposure and inability to quantify stress; Nurse 1A stated, “it would be helpful to be able to quantitate some aspect of the stress we’re putting them under because it must be just astronomical the amount of stress that these newborns undergo in their first two weeks.” This theme was dominant when participants were asked about sources of infant stress in the postoperative period, present in 50% of coded phrases offered by 13 (77%) clinicians (Supplemental Table S2).
Theme 5. Infants encounter multiple stressors in the operative setting
Participants described “the surgery itself” and multiple additional stressors including separation from parental figures, noise, cold or exposure, pain, and physiological stressors of cardiac surgery which are encountered by an infant in the operating room setting (Anaesthesiologist 2B: “It depends on what kind of surgery they’ve had, but pretty much all kids are going to have some type of pain or discomfort and that can have pretty significant effects on their hemodynamics”). This theme represented 50% of coded responses from 15 participants (88%; Supplemental Table S1) when asked about stressors encountered during the operative period.
Theme 6. Family bonding is disrupted
Across roles and care settings, participants noted the parent–infant connection is adversely impacted, citing physical barriers such as monitoring equipment, emotional barriers such as parental fear and stress, and barriers from staff including nursing staffing ratios and worries about parent interference with care (Anaesthesiologist 1B: “I bet they really need their moms”; Nurse 3B: “They have a role as a mom or a dad and it’s hard to bond with your child when you can’t hold your child”). Theme 6 occurred most frequently in the opening question on general perceptions of infant stress exposure (reported by 6 participants, 35% across 16 coded phrases, 8%) and when participants reflected on stressors encountered in the preoperative phase of care (reported by 7 participants, 41% across 26 coded phrases, 14.5%) and postoperative phases (reported by 4 participants, 23.5% across 13 coded phrases, 5.2%). See Supplemental Table S1.
Theme 7. Cardiac variations create infant physiologic strain
Participants noted that variations in cardiac anatomy and physiology related to tolerance of environmental and care-related stressors. Participants emphasised the need to consider these variations and individualise care accordingly (Nurse 1B: “Thinking about not just what we did that stressed them but like what is their underlying physiology? What is their function like? How well is their ability to compensate with this stress?”). Participants cited patients with single ventricle variants to be most concerning, using descriptors such as “much more fragile” and “inherently unstable”. Participants most frequently referenced this theme in the opening question (reported by 7 participants, 41%; across 25 coded phrases, 12.6%) and when identifying concerning signs in infants (reported by 4 participants, 23.5% across 20 coded phrases, 8%), but mentioned it least when discussing stress within phases of care (Supplemental Table S1).
Discussion
Drawing on decades of collective clinician experience, this work offers insight into sources of stress that have not been previously identified or described in infants undergoing cardiac surgery. Semantic content analysis of narrative data from 17 experienced interprofessional clinicians resulted in the identification of seven themes related to stress in infants undergoing cardiac surgery (Figure 2). Themes described sources of infant stress and clinical implications in preoperative, operative, and postoperative phases of care (Supplemental Table S1) and clinician recognition of potentially harmful high-stress states and subsequent response (Supplemental Tables S2). Findings indicate expert clinicians perceive that infants undergoing cardiac surgery encounter multiple and varied sources of stress. Sources of stress may be intrinsic, such as the disease process; extrinsic, such as environmental stress; or imposed on the infant, such as stress related to standard care. Participants reported multiple sources of stress beyond the physiological stress of abnormal cardiac anatomy and physiology, noting that these overlapping or simultaneous stressors can contribute to a significant cumulative burden.
Expert clinicians across disciplines described extensive and consistent exposure to stress across all phases of care. Participants described the clinical environment as “harsh” and “overstimulating”, noting the contrast between the clinical environment and a home environment. Relatedly, studies of salivary cortisol concentrations in infants cared for in intensive care settings have shown evidence of persistent stress, as levels did not downtrend comparably to those of healthy infants. Reference Lavanga, Bollen and Caicedo32,Reference Cabral, Antonini, Custódio, Martinelli and da Silva33 In a multicentre study evaluation of stressful encounters in neonates admitted to critical care units, an average of 141 stressful procedures were reported during the first 14 days of admission. Reference Carbajal, Rousset and Danan9 D’Agata et al. (2017) reported an average of 46 stressful experiences per day of hospitalisation in preterm infants. Reference D’Agata, Walsh, Vittner, Cong, McGrath and Young10 Given the complexity of care required to stabilise and treat neonates and infants with CHD, this population is likely to experience equivalent or greater stress exposure relative to preterm infants. However, no recent studies were identified reporting the type, frequency, or other descriptions of stressful encounters specific to infants with CHD, Reference Riley, Mastropietro, Darcy-Mahoney, Pintz, Zhou and Hinds34 a gap identified by Lisanti et al. in a recent American Heart Association Scientific Advisory. Reference Lisanti, Uzark and Harrison35
Overwhelmingly, participants reported concern about the negative impact of stressful encounters in infants undergoing cardiac surgery, describing stress as a threat to physiological stability. Stress exposure during this vulnerable period of development has been associated with impaired physiological, functional, and structural development. Reference Van Dokkum, De Kroon, Reijneveld and Bos3,Reference Smith, Gutovich and Smyser14,Reference McPherson, Miller, El-Dib, Massaro and Inder21,Reference Nist, Harrison and Steward22 Stress burden in the neonatal intensive care unit has been positively correlated to epigenetic DNA methylation which was negatively correlated with brain volumes. Reference Fumagalli, Provenzi and Carli20 Studies on stress exposure in infants with cardiac disease are limited, though mitigating infant stress and stress response following cardiac surgery provided the foundation to current analgesic approaches in the operative and post-operatives setting. Reference Anand and Aynsley-Green36,Reference Wessel37 While the direct consequences of stress exposure in infants with CHD are not established, cumulative stress may activate the alarm phase of stress response precipitating physiological instability including cardiac arrest. Based on Selye’s theoretical foundation and the findings presented here, stress exposure may be an unexplored and potentially modifiable risk factor for cardiac arrest in these infants. Negative impacts of stress exposure may help explain variability in physiological stability following cardiac surgery, including increased risk of cardiac arrest, and heterogeneity in neurodevelopmental outcomes. Reference Sood, Newburger and Anixt5
Participants described experiencing tension between delivering stressful clinical interventions and the responsibility to protect infants from that stress, a paradox of simultaneously healing and harming infants. Similar themes, including “and now you have broken them too” and “trauma in the NICU: whose trauma is it?”, have been identified in studies of neonatal intensive care unit clinicians. Reference D’Agata, Young, Cong, Grasso and McGrath29 Comparable to our findings, this study reported that while NICU clinicians find their work meaningful and rewarding, they suffer “vicarious traumatisation” secondary to professional responsibilities and proximity to infant and family suffering. Reference D’Agata, Young, Cong, Grasso and McGrath29 Intensive care providers are at increased risk of burnout Reference Moss, Good, Gozal, Kleinpell and Sessler38 and low levels of well-being. Reference Bor, Moscou-Jackson, Mastropietro and Staveski39 The paradox of harming while helping may contribute to clinician moral distress and burnout.
Across interdisciplinary roles, participants described a complex, evolving cognitive process for determining infant stress states and associated risk. Participants described using assessments of infant stress exposure and responses to individualise patient care by incorporating specific actions and strategies to protect infants from excessive stress, e.g. time-limited diagnostic evaluation, restricting non-essential care, and organising care to allow periods of rest following necessary clinical stressors. The proportion of clinical nurses with less than 2 years’ experience in the paediatric cardiac ICU has been linked to mortality Reference Hickey, Gauvreau, Connor, Sporing and Jenkins40 and survival after cardiac arrest. Reference Lasa, Banerjee and Zhang41 Collectively, these findings suggest clinical nurses are uniquely positioned to impact care and outcomes of infants with CHD, particularly in reducing non-essential stress exposure, identifying high-stress states, and communicating stress exposure and tolerance to the interprofessional team. Future development of a clinical measure to quantify infant stress exposure may allow clinicians across experience levels to recognise and communicate sources of stress and stress responses, promoting timely attention and response to high-stress states.
Clinical implications
Certain sources of stress encountered by infants undergoing cardiac surgery are unavoidable, while others may be modifiable or mitigated. Teams caring for this vulnerable population need the ability to identify and proactively limit non-essential stressors in the clinical environment, alleviate essential stressors with periods of rest, and recognise high-stress states which may necessitate escalation in clinical support. Compared to the diminishing pattern of stress exposure over time described in preterm infants, Reference van Dokkum, de Kroon, Dijk, Kraft, Reijneveld and Bos12–Reference Smith, Gutovich and Smyser14 infants undergoing cardiac surgery likely experience persistently elevated levels of stress in the preoperative, operative, and postoperative phases of care, predisposing them to acute instability and long-term neurodevelopmental vulnerabilities. This study provides a foundation for stress reduction protocols specific to neonates and infants with CHD. These protocols may reduce cumulative stress burden, allowing the exhaustion phase of stress response to be avoided or diminished and promote enhanced clinician recognition of infants experiencing this period of vulnerability.
While surgical and medical advances have improved survival for children with heart disease, less is known about the neurodevelopmental and psychosocial consequences of early life stress in this infant population. The association of longer postoperative CICU length of stay (LOS) and lower cognitive function in early childhood Reference Newburger, Wypij and Bellinger42 informed the rationale for interventions aimed at reducing CICU LOS. Incorporation of developmental care in infants with CHD, a broad category of interventions designed to individualise care and minimise stress, is intended to maximise their neurologic development, Reference Lisanti, Uzark and Harrison35,Reference Sood, Berends and Butcher43 and is increasingly associated with optimised neurodevelopmental outcomes. Reference Sood, Newburger and Anixt5 Developmental care additionally encompasses the deliberate avoidance of practices that needlessly increase stress exposure, which is thought to be neurotoxic. Reference Van Dokkum, De Kroon, Reijneveld and Bos3,Reference Sood, Newburger and Anixt5,Reference Lisanti, Uzark and Harrison35 Recognising stress exposure as a potential treatment toxicity in CHD care is imperative to reducing stress exposure. Developmental care protocols which incorporate measurement of stress exposure and proactive stress reduction in addition to interventions aimed at normalised development and bonding may provide a fully comprehensive approach to optimise outcomes.
Limitations
Although this study was designed to identify and define sources of stress in infants undergoing cardiac surgery and theorise potential relationships between infant stress and outcomes, including physiological instability, it was not designed to test these relationships. While clinicians from multiple centres were included, purposeful sampling did not specify equal representation from alternate centres, resulting in most participants being from the primary centre. Including participants primarily from a single centre may have increased the likelihood of centre bias in participant responses and may limit the transferability of findings. Sampling for this initial exploration focused on the primary clinical roles of nurses and physicians, other clinicians working with this population, e.g. physical and occupational therapists, respiratory therapists, psychologists, have valuable insights on stress exposure and impact, which should be included in subsequent studies. Future work across centres should focus on establishing relationships between stress exposure, cumulative stress burden, acute physiological instability, and long-term neurodevelopment.
Future research
Building on the shared perceptions of expert clinicians that infant stressors are encountered across all three phases of care, some of which may be modifiable, future studies should focus on accurately quantifying infant stress exposure, including the type and frequency of stressful encounters, to identify sources of infant stress that can be eliminated or mitigated. This study is foundational to the exploration of the emerging hypothesis that cumulative stress burden may be a modifiable risk factor for cardiac arrest in infants undergoing cardiac surgery. Investigation of behaviours utilised by experts to protect infants from stress may inform stress-reduction interventions and care models. Evaluation of the relationship between environmental stress and outcomes in infants and infant-parent dyads may guide environmental stress reduction. Closer examination of the processes that expert clinicians utilise to integrate information in the assessment of infant stress burden and associated risks may contribute to the development of technology, making this complex expert-level process readily accessible to more novice clinicians.
Conclusions
Selye’s stress theory guided this exploration of cumulative stress and stress response in infants and neonates undergoing cardiac surgery from the perspective of expert clinicians. Findings indicated that these infants experience numerous, often concurrent stressors in addition to their disease process. Understanding and addressing infant stress burden across preoperative, operative, and postoperative phases of care carries the potential to reduce acute physiological instability and optimise long-term neurodevelopmental outcomes for infants with CHD.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S1047951126111676
Acknowledgements
None.
Financial support
This work was supported by the American Heart Association/Children’s Heart Foundation Predoctoral Fellowship (https://doi.org/10.58275/AHA.23PRECHF1026850.pc.gr.174249) granted to Christine M. Riley.
Competing interests
This work was supported by the American Heart Association as listed in Financial Support.



 Open access
Open access